Charcot Neuroarthropathy: Advanced Classification and Surgical Reconstruction
Key Takeaway
Charcot neuroarthropathy requires a profound understanding of both its temporal evolution and anatomical patterns. The modified Eichenholtz staging dictates the timing of intervention, while the Brodsky classification guides the structural approach to reconstruction. Surgical management aims to create a stable, plantigrade, and braceable foot, mitigating the high risks of ulceration and osteomyelitis through strategic realignment, rigid internal fixation, and meticulous soft tissue balancing.
INTRODUCTION TO CHARCOT NEUROARTHROPATHY
Charcot neuroarthropathy (CN) is a progressive, devastating, and limb-threatening condition characterized by joint dislocation, pathologic fractures, and severe destruction of the pedal architecture in patients with profound peripheral neuropathy. While diabetes mellitus remains the most common etiology in the developed world, any condition resulting in loss of protective sensation (e.g., syringomyelia, tabes dorsalis, chronic alcoholism) can precipitate this cascade.
Successful management of the Charcot foot requires the orthopedic surgeon to synthesize two critical dimensions of the disease: the temporal physiological phase (dictating when to operate) and the spatial anatomical pattern (dictating where and how to reconstruct). These dimensions are codified by the modified Eichenholtz staging system and the Brodsky anatomical classification, respectively.
Clinical Pearl: The primary goal of Charcot reconstruction is not the restoration of normal anatomy, but rather the creation of a stable, plantigrade, and braceable foot to prevent recurrent ulceration, osteomyelitis, and subsequent major lower extremity amputation.
THE TEMPORAL AXIS: MODIFIED EICHENHOLTZ STAGING
The Eichenholtz classification, originally described in 1966 and later modified to include a "Stage 0," categorizes the natural history of Charcot arthropathy based on clinical inflammatory signs and radiographic progression. Understanding these stages is paramount, as surgical intervention during the acute inflammatory phase carries a significantly higher risk of hardware failure and infection.
Stage 0: The Prodromal Phase
- Clinical Presentation: Patients present with marked erythema, warmth, and swelling of the foot and ankle following a minor, often unrecognized, injury. Bounding pulses are typically present due to autonomic neuropathy and resultant autosympathectomy (hyperemia).
- Radiographic Findings: Plain radiographs are entirely normal or show only soft tissue swelling. There is no evidence of fracture or dislocation.
- Advanced Imaging: Magnetic Resonance Imaging (MRI) is diagnostic, revealing diffuse bone marrow edema and microfractures before plain radiographic changes occur.
- Management: Immediate and strict non-weight-bearing in a total contact cast (TCC). Prompt immobilization at this stage can arrest the progression and prevent catastrophic deformity.
Stage 1: Fragmentation (Acute Phase)
- Clinical Presentation: The extremity exhibits profound erythema, warmth, and swelling, often mimicking acute cellulitis or deep space infection. Joint laxity becomes clinically apparent.
- Radiographic Findings: The hallmark of Stage 1 is active bone destruction. Radiographs demonstrate periarticular fragmentation, bony debris, subchondral osteopenia, and frank subluxation or dislocation of the involved joints.
- Management: Continued strict immobilization. Surgical intervention is generally contraindicated in Stage 1 due to the hyperemic, osteopenic state of the bone, which provides poor purchase for internal fixation. Surgery is reserved only for severe instability threatening the soft tissue envelope or acute irreducible dislocations.
Stage 2: Coalescence (Subacute Phase)
- Clinical Presentation: The acute inflammatory signs (erythema, warmth, swelling) begin to subside. The foot remains deformed but feels more stable clinically.
- Radiographic Findings: Radiographs show the absorption of fine bony debris, early new bone formation, sclerosis of bone ends, and the coalescence of larger fracture fragments.
- Management: Transition from TCC to a Charcot Restraint Orthotic Walker (CROW) or continued casting. This stage marks the beginning of the "safe window" for reconstructive surgery if the deformity is unbraceable.
Stage 3: Consolidation (Chronic Phase)
- Clinical Presentation: Complete resolution of swelling and warmth. The foot is stable but often exhibits a fixed, rigid deformity (e.g., rocker-bottom foot).
- Radiographic Findings: Advanced remodeling of bone, rounding of fracture fragments, and solid arthrodesis or pseudoarthrosis of the involved joints.
- Management: Custom orthotic footwear for braceable deformities. For non-braceable deformities or those with recurrent ulcerations, definitive surgical reconstruction (exostectomy or corrective arthrodesis) is indicated.
THE ANATOMICAL AXIS: BRODSKY CLASSIFICATION
The anatomical classification, as described by Brodsky with modifications, categorizes Charcot arthropathy into five distinct types based on the primary joints involved. This system directly informs the biomechanical consequences of the collapse and dictates the surgical approach.
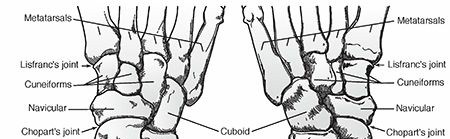
Type 1: Tarsometatarsal (Lisfranc) Joints
- Prevalence: This is the most common type of Charcot arthropathy (affecting approximately 60% of patients).
- Biomechanics & Deformity: Involvement of the Lisfranc complex leads to dorsal subluxation of the midfoot and plantar flexion of the metatarsals. This collapse destroys the longitudinal arch, resulting in the classic "rocker-bottom" deformity.
- Complications: The collapse creates severe bony prominences at the plantar aspect of the midfoot (often the medial cuneiform or cuboid), leading to recalcitrant plantar ulcerations.
Type 2: Chopart and Subtalar Joints
- Prevalence: The second most commonly affected area (approximately 30%).
- Biomechanics & Deformity: Involvement of the transverse tarsal (talonavicular and calcaneocuboid) and subtalar joints. This leads to a more proximal rocker-bottom deformity characterized by severe plantar flexion of the talar head.
- Complications: Marked varus or valgus instability of the hindfoot develops. The talar head often breaches the medial plantar soft tissues, creating a high-risk zone for ulceration and contiguous osteomyelitis.
Type 3A: Ankle Joint
- Prevalence: Less common but highly morbid (approximately 9%).
- Biomechanics & Deformity: Destruction of the tibiotalar joint leads to rapid, marked varus or valgus angulation. The talus may completely dislocate from the ankle mortise.
- Complications: Severe ulceration over the prominent medial or lateral malleoli.
Surgical Warning: Type 3A deformities rarely can be controlled with conservative measures (bracing) because of the massive lever arms acting on the unstable ankle. Early surgical intervention (tibiotalocalcaneal arthrodesis) is almost universally required to salvage the limb.
Type 3B: Calcaneus
- Pathoanatomy: This type encompasses specific fractures of the calcaneus in the neuropathic foot:
- Avulsion of the Posterior Tuberosity: The Achilles tendon avulses the posterior calcaneus, leading to loss of plantarflexion power and posterior heel ulceration.
- Joint Depression: Collapse of the posterior facet results in a varus or valgus deformity and flattening of the talar declination angle.
- Anterior Process Fracture: Leads to instability of the lateral column, which subsequently causes instability and subluxation of the talonavicular joint.
Type 4: Multiple Regions
- Pathoanatomy: Concurrent involvement of two or more of the aforementioned regions (e.g., combined Lisfranc and ankle Charcot). These represent the most challenging reconstructive cases, often requiring staged procedures or massive rigid internal fixation constructs.
Type 5: Forefoot
- Prevalence: A rare form of true Charcot arthropathy, though neuropathic forefoot complications are common.
- Pathoanatomy: Dislocation of the metatarsophalangeal (MTP) joints leads to severe claw toe deformities, retrograde buckling of the metatarsal heads, and subsequent plantar ulcerations.
- Clinical Correlation: Grade 3 ulcers under the metatarsal heads (e.g., the second metatarsal) frequently extend directly into the bone, resulting in contiguous osteomyelitis that requires aggressive debridement or ray resection.
FOREFOOT COMPLICATIONS: ULCERATION AND DRIFT
The neuropathic forefoot is highly susceptible to minor trauma, often exacerbated by ill-fitting footwear or altered biomechanics following minor amputations.


FIGURE 85-11 Cellulitis, abscess, and osteomyelitis arising from an ulcer over the fifth toe caused by a tight shoe. Minor friction in a neuropathic foot rapidly escalates to limb-threatening infection.
When partial foot or toe amputations are performed to manage localized osteomyelitis, the loss of structural support alters the biomechanics of the remaining digits. The remaining toes often drift to fill the void created by the amputation, leading to new areas of friction, pressure, and subsequent ulceration.


FIGURE 85-12 A and B, Drift of toes to fill the defect created by the amputation of a toe. This structural shift necessitates meticulous orthotic management to prevent secondary breakdown.
SURGICAL MANAGEMENT OF CHARCOT ARTHROPATHY
Indications for Surgery
Surgical reconstruction is indicated when conservative management fails to maintain a plantigrade, braceable foot. Specific indications include:
1. Recurrent or recalcitrant ulceration due to fixed bony prominences.
2. Severe instability (especially Brodsky Type 3A ankle Charcot) that cannot be braced.
3. Impending soft tissue compromise from dislocated bony segments.
4. Chronic pain (in patients with retained deep sensation).
Preoperative Optimization
- Infection Control: Any active ulceration must be addressed. If osteomyelitis is present, a staged approach is mandatory: Stage 1 involves aggressive debridement, bone biopsy, and placement of antibiotic-loaded cement spacers. Stage 2 (reconstruction) is performed only after inflammatory markers normalize and cultures are clear.
- Vascular Assessment: Ankle-Brachial Index (ABI), toe pressures, and potentially CT angiography are required. Ischemic limbs must be revascularized prior to any reconstructive effort.
- Glycemic Control: HbA1c should ideally be optimized to < 8.0% to mitigate postoperative infection and wound healing complications.
The Concept of "Superconstructs"
Standard AO principles of internal fixation frequently fail in neuropathic bone. Orthopedic surgeons must employ "Superconstruct" principles (as popularized by Sammarco):
1. Extend the fusion: Arthrodesis must extend beyond the zone of injury to include normal, healthy bone.
2. Resect bone for deformity correction: Do not rely on hardware to pull deformed bone into place; resect wedges of bone to shorten the column and reduce tension on the soft tissue envelope.
3. Use the strongest hardware possible: Utilize locked plates, intramedullary nails, and heavy-duty beaming screws.
4. Maximize hardware footprint: Apply hardware in a manner that maximizes the surface area of fixation.
Step-by-Step Surgical Approach: Midfoot Reconstruction (Brodsky Type 1)
1. Positioning and Preparation:
The patient is positioned supine with a bump under the ipsilateral hip to internally rotate the leg to a neutral position. A thigh tourniquet is applied.
2. Soft Tissue Balancing (Achilles Lengthening):
Almost all Charcot deformities are driven by an underlying equinus contracture. A percutaneous Tendo-Achilles Lengthening (TAL) or open gastrocnemius recession is performed first to eliminate the deforming plantarflexion force and allow dorsiflexion of the foot past neutral.
3. Surgical Approaches:
* Medial Utility Incision: An incision is made along the medial border of the foot, from the navicular tuberosity to the first metatarsal shaft. This exposes the medial column (talonavicular, naviculocuneiform, and first tarsometatarsal joints).
* Lateral Utility Incision: If lateral column correction is required, an incision is made from the distal fibula toward the base of the fourth metatarsal, exposing the calcaneocuboid and lateral tarsometatarsal joints.
4. Joint Preparation and Deformity Correction:
* The periosteum is elevated meticulously to preserve blood supply.
* The involved joints are exposed. In Stage 3 Charcot, the joints are often fused in a deformed position.
* A sagittal saw is used to perform biplanar wedge resections. The apex of the wedge is typically dorsal, allowing the plantar-flexed forefoot to be elevated, thereby correcting the rocker-bottom deformity and restoring the longitudinal arch.
* All cartilage and sclerotic bone must be removed down to bleeding, healthy cancellous bone.
5. Rigid Internal Fixation:
* Medial Column Beaming: A large solid or cannulated screw (e.g., 6.5mm or 7.0mm) is introduced from the first metatarsal head, driven proximally across the medial cuneiform and navicular, and anchored into the body of the talus.
* Lateral Column Beaming: A similar screw is driven from the 4th or 5th metatarsal base into the calcaneus.
* Plating: Plantar or medial locked plates are applied to act as tension band constructs, neutralizing the deforming forces of weight-bearing.
6. Closure:
Meticulous, layered closure is critical. The skin is closed with non-absorbable sutures (e.g., nylon) using a vertical mattress technique to minimize tension on the epidermal edges.
Specific Procedure: 1st MTP Resection Arthroplasty for Hallux Ulceration
Loss of normal joint mobility in the neuropathic foot frequently leads to localized pressure points. Clinical hallux rigidus places immense pressure at the interphalangeal joint during the terminal stance phase of gait, leading to recalcitrant plantar ulcerations.




FIGURE 85-14 A, Hallux laceration related to loss of normal joint mobility; during weight bearing, clinical hallux rigidus places pressure at the interphalangeal joint. B, Planned resection arthroplasty of the first metatarsophalangeal joint. C, Ulcer healed in the immediate postoperative period.
Surgical Steps for Resection Arthroplasty (Keller Procedure):
1. A dorsal longitudinal incision is made over the 1st MTP joint, lateral to the extensor hallucis longus (EHL) tendon.
2. The capsule is incised, and the joint is exposed.
3. A sagittal saw is used to resect the proximal 1/3 to 1/2 of the proximal phalanx.
4. The prominent dorsal osteophytes of the first metatarsal head are resected (cheilectomy).
5. The EHL may be lengthened if severe extension contracture is present.
6. The void created by the resection decompresses the joint, eliminating the rigid lever arm and allowing the plantar ulcer to heal rapidly.
POSTOPERATIVE PROTOCOL AND REHABILITATION
The postoperative management of the reconstructed Charcot foot is as critical as the surgery itself. Neuropathic bone requires twice the normal time to achieve solid arthrodesis.
- Phase I (0-2 Weeks): The patient is placed in a well-padded, short-leg splint and remains strictly non-weight-bearing (NWB). Sutures are left in place longer than usual (typically 3-4 weeks) due to compromised microvascular healing in diabetic patients.
- Phase II (2-12 Weeks): Transition to a Total Contact Cast (TCC) or a rigid fiberglass cast. The patient remains strictly NWB. Serial radiographs are obtained every 4 weeks to monitor alignment and hardware integrity.
- Phase III (12-24 Weeks): Once radiographic consolidation is evident, the patient is transitioned to a Charcot Restraint Orthotic Walker (CROW) boot. Progressive, partial weight-bearing is initiated.
- Phase IV (Long-term): Transition to custom-molded, extra-depth diabetic footwear with rigid rocker-bottom soles. Lifelong surveillance by a multidisciplinary team (orthopedics, podiatry, endocrinology, orthotics) is mandatory.
Pitfall: Premature weight-bearing is the leading cause of hardware failure and recurrent deformity in Charcot reconstruction. Surgeons must explicitly educate patients that the absence of pain (due to neuropathy) does not equate to structural healing. Strict adherence to the NWB protocol is non-negotiable.
📚 Medical References
- Charcot arthropathy of the spine in long-standing paraplegia, Spine 12:480, 1987.
- Kastenbauer S, Winkler F, Fesl G, et al: Acute severe spinal cord dysfunction in bacterial meningitis in adults: MRI fi ndings suggest extensive myelitis, Arch Neurol 58:717, 2001.
- Kattapuram SV, Phillips WC, Boyd R: Computed tomography in pyogenic osteomyelitis of the spine, AJR Am J Roentgenol 140:1199, 1983.
- Konnberg M: Erythrocyte sedimentation rate following lumbar discectomy, Spine 11:766, 1986.
- Krodel A, Kruger A, Lohscheidt K, et al: Anterior débridement, fusion, and extrafocal stabilization in the treatment of osteomyelitis of the spine, J Spinal Disord 12:17, 1999.
- Macnab I, St Louis EL, Grabias SL, et al: Selective ascending lumbosacral venography in the assessment of lumbar-disc herniation, J Bone Joint Surg 58A:1093, 1976.
- Modic T, Masaryk T, Plaushtek D: Magnetic resonance imaging of the spine, Radiol Clin North Am 14:229, 1986.
- Nélaton A: Éléments de pathologie chirurgicale, Paris, 1844, Baillière. Ogata K, Whiteside LA: Nutritional pathways of the intervertebral disc, Spine 6:211, 1981.
- Picada R, Winter RB, Lonstein JE, et al: Postoperative deep wound infection in adults after posterior lumbosacral spine fusion with instrumentation: incidence and management, J Spinal Disord 13:42, 2000.
- Pinner RW, Teutsch SM, Simonsen L, et al: Trends in infectious diseases mortality in the United States, JAMA 275:189, 1996.
- Pott P: Remarks on that kind of palsy of the lower limbs which is frequently found to accompany a curvature of the spine, London, 1779, J Johnson. Puig-Guri J: Pyogenic osteomyelitis of the spine: differential diagnosis through clinical and roentgenographic observations, J Bone Joint Surg 28:29, 1946.
- Razak M, Kamari ZH, Roohi S: Spinal infection—an overview and the results of treatment, Med J Malaysia 55:C18, 2000.
- Richards BR, Emara KM: Delayed infections after posterior TSRH spinal instrumentation for
You Might Also Like