Calcaneotibial Fusion & Talar Fractures: Surgical Guide
Key Takeaway
Calcaneotibial fusion is a powerful salvage procedure for severe talar body fractures, avascular necrosis, and end-stage arthropathy. This comprehensive guide details the anterolateral approach, talar extirpation, and rigid fixation techniques. It also explores the Blair fusion alternative for preserving limb length and midtarsal motion, alongside evidence-based management protocols for lateral process talar fractures, ensuring optimal biomechanical restoration and functional outcomes in complex hindfoot reconstruction.
Introduction to Calcaneotibial Arthrodesis
Calcaneotibial fusion (tibiocalcaneal arthrodesis) is a formidable salvage procedure reserved for the most severe pathologies of the hindfoot and ankle. When the talus is rendered unsalvageable due to highly comminuted fractures, severe avascular necrosis (AVN), chronic infection, or massive bone loss, standard tibiotalar arthrodesis is no longer viable. In these complex scenarios, extirpation of the talar body followed by direct fusion of the tibia to the calcaneus provides a stable, plantigrade, and painless limb, albeit at the cost of hindfoot motion and limb length.
This comprehensive masterclass delineates the surgical indications, biomechanical considerations, step-by-step operative techniques for standard calcaneotibial fusion, the Blair fusion alternative, and the evidence-based management of lateral process talar fractures.
Indications and Preoperative Planning
The primary indication for calcaneotibial fusion is the catastrophic failure or absence of the talar body. Conditions necessitating this approach include:
* Severe Comminuted Talar Body Fractures: Fractures that defy open reduction and internal fixation (ORIF) due to massive articular cartilage destruction or extrusion.
* Avascular Necrosis (AVN) of the Talus: Often a sequela of Hawkins Type III or IV talar neck fractures, leading to talar dome collapse and secondary tibiotalar/subtalar arthritis.
* Chronic Osteomyelitis: Intractable infection of the talus requiring total or partial talectomy.
* Neuropathic (Charcot) Arthropathy: Severe midfoot and hindfoot collapse requiring rigid stabilization.
* Tumor Resection: Primary benign aggressive or malignant lesions of the talus.
Biomechanical Considerations
Direct coaptation of the tibia to the calcaneus inherently shortens the limb by 2 to 3 centimeters, depending on the amount of bone resected and whether structural allografts are utilized. Furthermore, the loss of the talus alters the moment arm of the Achilles tendon, reducing plantarflexion power.
Clinical Pearl: The surgeon must anticipate the "accordion effect." Chronic absence or collapse of the talus leads to severe contracture of the neurovascular bundle, tendons, and skin. Attempting to restore original limb length acutely with massive structural grafts can cause catastrophic neurovascular compromise or wound dehiscence.

FIGURE 88-42 A: Preoperative radiograph demonstrating a severe talar body fracture with an associated fibular fracture, a classic injury pattern that, if unsalvageable, may necessitate tibiocalcaneal arthrodesis.

FIGURE 88-42 B: Attempted fixation of the talar body utilizing headless compression screws.

FIGURE 88-42 C: Concurrent fixation of the fibula with a neutralization plate and screws. Failure of such constructs often leads to the salvage pathways discussed herein.
Surgical Technique: Calcaneotibial Fusion
The goal of this procedure is to achieve rigid osteosynthesis between the distal tibia, the calcaneus, and often the navicular, ensuring a plantigrade foot optimized for weight-bearing.
1. Patient Positioning and Approach
- Place the patient in the lateral decubitus or supine position with a large ipsilateral hip bump to internally rotate the leg, providing excellent access to the lateral hindfoot.
- Utilize a thigh tourniquet for hemostasis.
- Incision: Expose the operative field through an extensile anterolateral incision. This approach utilizes the internervous plane between the superficial peroneal nerve (anterior compartment) and the sural nerve (lateral compartment).
2. Talar Extirpation
- Identify and protect the neurovascular structures. Retract the extensor digitorum longus and peroneus tertius medially.
- Remove the fragmented or necrotic remnants of the body of the talus.
- Handling Intact Bone: In cases of comminuted fractures that are several months old, or when the junction of the talar body and neck remains intact, do not attempt to pry the talus out in one piece. Instead, divide the talus with an osteotome into as many pieces as necessary for easy, atraumatic removal.
- Drive an osteotome through the proximal part of the navicular to resect the proximal articular cartilage and subchondral bone en bloc with the head and neck of the talus.
3. Joint Preparation and Soft Tissue Management
- Meticulously excise the remaining articular surfaces of the distal tibia and the superior aspect of the calcaneus down to bleeding subchondral bone.
- Roughen the medial surface of the lateral malleolus to promote lateral gutter fusion.
- Overcoming the Accordion Effect: Strip the soft tissue attachments around both the medial and lateral malleoli. This release must be sufficient to allow posterior displacement of the foot until the navicular comes into direct contact with the anterior tibia.
- Surgical Warning: It may be necessary to resect a portion of both malleoli. The soft tissues often collapse like an accordion, fiercely resisting efforts to properly appose the calcaneus to the tibia. Forcing this apposition without adequate bony resection or soft tissue release risks skin necrosis.
4. Grafting and Coaptation
- Denude the anterior tibia at the exact point of contact with the navicular to facilitate a secondary fusion mass.
- Structural Allograft: If active infection is definitively ruled out, a femoral head allograft can be utilized to bridge the defect and restore height. The graft, tibia, and calcaneus must be meticulously contoured using spherical reamers or burrs to ensure a perfect, flush fit.
5. Alignment and Rigid Fixation
- Positioning the Foot: Hold the foot strictly at a right angle to the leg (neutral) or in a maximum of 5 degrees of dorsiflexion. Ensure 5 degrees of hindfoot valgus and external rotation matching the contralateral limb.
- Temporary Fixation: Insert two heavy Steinmann pins transversely through the calcaneus and tibia to provisionally hold the reduction.
- Definitive Fixation: Apply robust arthrodesis plates, a retrograde tibiotalocalcaneal (TTC) intramedullary nail, or a multi-planar external fixation device to maintain firm, compressive contact between the tibia and calcaneus.
- Fix the navicular to the anterior tibia using a fully threaded cortical screw or headless compression screw to enhance anterior column stability.
- Bone Grafting: Denude local bone chips obtained during the malleolar resection and pack them densely around the junctions of the calcaneus, navicular, and tibia.
6. Postoperative Care Protocol
- Phase I (0 to 6-8 weeks): The patient is kept strictly non-weight-bearing in a well-padded short-leg cast or rigid splint.
- Phase II (6-8 to 12-16 weeks): Transition to a weight-bearing cast for an additional 6 to 8 weeks, pending radiographic evidence of bridging trabeculae.
- Phase III (Long-term): The limb is protected for the next several months utilizing a custom short-leg double-upright brace with a locked ankle joint to prevent sheer stress on the maturing fusion mass.

FIGURE 88-43 A: Radiographic appearance four years after tibiocalcaneal fusion achieved via compression arthrodesis and autogenous iliac bone grafting. Note the solid consolidation.

FIGURE 88-43 B: Sixteen years post-fusion. While degenerative changes at the midtarsal joints are present, the patient remains highly active with only mild symptoms, demonstrating the long-term durability of the procedure.
The Blair Fusion: A Biomechanical Alternative
Because of the inevitable decrease in limb height and the severe rigidity of the ankle joint following standard calcaneotibial fusion, Blair introduced a highly effective alternative procedure. This technique is particularly useful when the talar body is destroyed, but the talar head and neck remain viable and well-vascularized.
Rationale and Technique
In the Blair fusion, the comminuted or necrotic fragments of the talar body are completely excised. Instead of dropping the tibia down to the calcaneus, a sliding cortical bone graft is harvested from the anterior surface of the distal tibia. This graft is then translated distally and inserted directly into a prepared slot in the remnant of the head and neck of the talus. The goal is to obtain a solid fusion across the anterior tibia and the talar neck.
Biomechanical Advantages of the Blair Fusion
Blair reported several profound advantages to this technique over standard tibiocalcaneal arthrodesis:
1. Preservation of Anatomy: The position of the foot remains unchanged, and backward displacement of the foot is unnecessary.
2. Limb Length: The extremity is not significantly shortened.
3. Joint Kinematics: The relationships of the foot and ankle remain near normal, and the weight-bearing thrust is placed on undisturbed, native joint tissue (the subtalar joint).
4. Retained Motion: Crucially, after this operation, there is still slight flexion and extension of the foot on the leg. The two subtalar facets and the talonavicular joint allow a compensatory "rocking motion." Over time, compensatory movement usually develops in the midtarsal joints, enabling the patient to walk with a fairly elastic gait and only a slight limp.
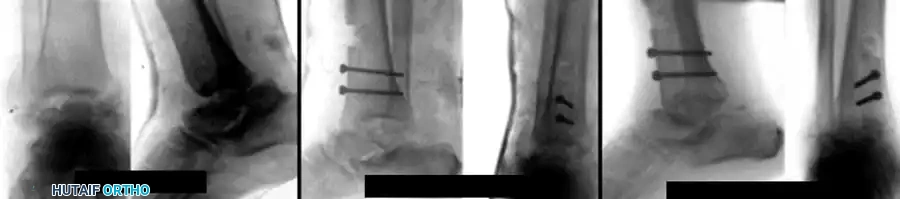
FIGURE 88-44: Results of Blair fusion. (A) Preoperative Type III fracture-dislocation of the talus with severe body comminution. (B) Immediate postoperative radiograph demonstrating the sliding anterior tibial graft slotted into the talar neck. (C) Solid fusion achieved at 3 months, preserving hindfoot height and subtalar kinematics.
Management of Lateral Process Talar Fractures
While massive talar body trauma may necessitate fusion, isolated fractures of the lateral process of the talus require a completely different, joint-preserving algorithm. Often misdiagnosed as severe ankle sprains, these "snowboarder's fractures" demand high clinical suspicion.
Mechanism of Injury and Anatomy
The classic mechanism of injury involves a combination of axial loading, dorsiflexion, external rotation, and eversion. Additionally, a lateral subtalar dislocation may shear off the lateral process of the talus as the calcaneus displaces.
The lateral process is a critical anatomical hub, serving as the site of attachment for three major ligaments:
1. The lateral talofibular ligament (LTFL)
2. The anterior talofibular ligament (ATFL)
3. The posterior talofibular ligament (PTFL)
Surgical Pearl: Despite these dense ligamentous attachments, removing an ununited or severely comminuted lateral process fragment can disrupt these specific attachments but does not cause clinically significant ankle or subtalar instability. The deep deltoid and remaining syndesmotic structures provide adequate stability.
Hawkins Classification of Lateral Process Fractures
Hawkins classified these injuries to guide operative decision-making:
* Type I: A large, single fragment that involves both the talofibular articulation and the subtalar joint.
* Type II: A comminuted fracture that involves these two articulations.
* Type III: A nonarticular, extra-articular avulsion type of fracture.
Treatment Algorithms and Outcomes
Type I Fractures (Large Fragments):
* Nonoperative: Can be treated in a strictly non-weight-bearing cast for 6 weeks if truly undisplaced.
* Operative (ORIF): If the fragment is displaced or involves a significant portion of the talar side of the posterior facet, it should be treated with Open Reduction and Internal Fixation (ORIF) using mini-fragment screws (1.5mm to 2.4mm).
Type II Fractures (Comminuted):
* These fractures rarely heal anatomically and frequently lead to subtalar arthritis if left alone. They highly benefit from primary surgical débridement and excision of the fragments if they are displaced (which is most often the case). Attempting ORIF on severe comminution often fails.
Type III Fractures (Avulsion):
* Usually treated nonoperatively with immobilization and progressive weight-bearing as tolerated.
Outcomes and Salvage:
In a comprehensive review of 109 lateral process fractures, the data heavily favors surgical intervention for displaced injuries: 88% of operatively treated patients had mild or no symptoms, whereas 38% of nonoperatively treated patients suffered from moderate to severe chronic symptoms.
In all fracture types, if a symptomatic nonunion occurs, delayed surgical débridement and excision of the fracture fragment can be performed. Using this excision approach, excellent outcomes can still be obtained, with the vast majority of patients successfully returning to high-impact sporting activities without residual instability.
You Might Also Like
