Peroneus Brevis Tendon Transfer for Neglected Achilles Tendon Ruptures

Key Takeaway
Neglected Achilles tendon ruptures present a complex reconstructive challenge due to tendon retraction and poor tissue quality. When the defect spans less than 6 cm, the peroneus brevis tendon transfer provides an excellent, biomechanically sound autograft solution. This technique bridges the gap, restores plantar flexion power, and utilizes a muscle in phase with the gastrocnemius-soleus complex, ensuring optimal functional recovery for the patient.
Introduction and Rationale
Neglected or chronic ruptures of the Achilles tendon—typically defined as those presenting more than four to six weeks post-injury—pose a formidable challenge to the orthopaedic surgeon. Unlike acute ruptures, which can often be managed with primary end-to-end repair or conservative functional rehabilitation, chronic ruptures are characterized by significant tendon retraction, scar tissue interposition, and fatty infiltration or atrophy of the gastrocnemius-soleus complex (GSC).
When the gap between the debrided, healthy tendon stumps exceeds 3 to 4 cm, primary repair is usually impossible without excessive tension, which would inevitably lead to equinus contracture or catastrophic re-rupture. For defects measuring up to 6 cm, local tendon transfers provide an elegant, autologous solution. The transfer of the peroneus brevis (PB) tendon, popularized by Maffulli et al., is a highly reliable technique that not only bridges the structural defect but also introduces viable, vascularized tissue and supplementary plantar flexion power to the compromised posterior compartment.
Clinical Pearl: The primary goal of tendon transfer in chronic Achilles ruptures is not merely to bridge the gap, but to restore the resting tension of the triceps surae. Failure to adequately tension the transfer will result in a persistent calcaneus gait and profound push-off weakness.
Biomechanics and Graft Selection
The selection of an appropriate tendon for transfer requires a thorough understanding of foot and ankle biomechanics. The ideal transfer should be synergistic (in phase with the GSC during the gait cycle), possess adequate tensile strength, and have a line of pull that closely mimics the native Achilles tendon.
The three most common local autografts utilized for Achilles reconstruction are the Peroneus Brevis, the Flexor Hallucis Longus (FHL), and the Flexor Digitorum Longus (FDL).
Comparison of Tendons for Transfer
Peroneus Brevis (PB)
* Strength Relative to GSC: 18 times weaker.
* Advantages: Strictly in phase with the GSC during normal gait. It shares a role as a secondary plantar flexor of the ankle and is in relatively close proximity to the Achilles tendon, albeit in a separate fascial compartment.
* Concerns: Harvest results in a measurable loss of eversion strength. Furthermore, the lateral-to-medial pull after transfer to the calcaneus or Achilles stump does not perfectly reproduce the natural inversion moment normally created by the native Achilles tendon. There is also a distinct risk of sural nerve damage during harvest and routing.
Flexor Hallucis Longus (FHL)
* Strength Relative to GSC: 13 times weaker (the strongest of the local options).
* Advantages: In phase with the GSC. Shares a role as a plantar flexor. It has the closest anatomical proximity to the Achilles tendon, allowing for a direct line of pull.
* Concerns: Harvest can lead to a loss of push-off strength at the first metatarsophalangeal joint, potential clawed hallux deformity, transfer metatarsalgia, and risk to the neurovascular bundle during deep harvest.
Flexor Digitorum Longus (FDL)
* Strength Relative to GSC: 27 times weaker.
* Advantages: In phase with the GSC and acts as a synergistic plantar flexor.
* Concerns: Weakened flexion of the lesser toes, potential for lesser toe deformities, and risk of neurovascular injury during harvest. It is significantly weaker than both the FHL and PB.
For gaps under 6 cm, the peroneus brevis remains an exceptional choice due to its robust nature, ease of harvest, and excellent excursion profile, provided the surgeon meticulously manages the lateral-to-medial vector.
Preoperative Planning and Patient Positioning
Thorough preoperative clinical evaluation and advanced imaging (typically MRI) are mandatory to assess the extent of the tendon gap, the degree of tendinosis in the remaining stumps, and the severity of fatty atrophy within the GSC.
Positioning:
1. The patient is placed in the prone position on a radiolucent operating table.
2. A thigh tourniquet is applied to provide a bloodless surgical field.
3. The operative leg is prepped and draped free to allow full intraoperative assessment of ankle range of motion and resting equinus tension compared to the contralateral limb.
4. A bump may be placed under the distal tibia to allow the foot to hang freely, facilitating the assessment of the Thompson test and resting tension.
Surgical Anatomy and Neurovascular Considerations
The most critical neurovascular structure at risk during this procedure is the sural nerve. The sural nerve courses distally along the posterolateral aspect of the calf. At approximately 10 cm proximal to the calcaneal insertion of the Achilles tendon, it crosses the lateral border of the tendon, moving from medial/central to lateral.
Surgical Warning: When making the distal lateral incision for the Achilles stump and routing the peroneus brevis, the incision must be made as close as possible to the anterior aspect of the lateral border of the Achilles tendon. This ensures the dissection remains strictly posterior to the sural nerve, preventing painful neuromas or sensory deficits.
Step-by-Step Surgical Technique: The Maffulli Approach
1. Incisions and Exposure
The Maffulli technique utilizes three distinct, minimally invasive longitudinal incisions to preserve the delicate posterior skin envelope and optimize wound healing.
- Proximal Incision: Make a 5-cm longitudinal incision located 2 cm proximal and just medial to the palpable end of the proximal Achilles stump.
- Distal Incision: Make a second longitudinal incision, 3 cm long, located 2 cm distal and just lateral to the lateral margin of the distal stump. Strictly observe the sural nerve precautions mentioned above.
- Harvest Incision: Make a 2-cm longitudinal incision directly over the base of the fifth metatarsal to identify the distal insertion of the peroneus brevis.
2. Tendon Preparation and Gap Measurement
Through the distal Achilles incision, mobilize the distal tendon stump. It is imperative to free it from all peritendinous adhesions, particularly along its lateral aspect. Resect the degenerative, ruptured tendon end back to healthy, organized collagenous tissue. To prevent the separation of the tendon bundles during manipulation, place a locking whipstitch (e.g., No. 1 Vicryl or similar braided absorbable suture) along the free tendon edge.
Next, mobilize the proximal tendon stump through the proximal medial incision. Divide any dense adhesions and meticulously release the soft tissues anterior to the soleus and gastrocnemius muscles. This deep release is critical; it allows for maximal distal excursion of the proximal stump, thereby minimizing the absolute gap between the tendon ends.
With the ankle held in maximal plantar flexion, measure the remaining defect between the two healthy tendon ends. If the gap is less than 6 cm, the peroneus brevis tendon possesses adequate length to bridge the defect effectively.
3. Peroneus Brevis Harvest
Direct attention to the 2-cm incision at the lateral border of the foot. Identify the peroneus brevis tendon at its insertion on the tuberosity of the fifth metatarsal. Expose the tendon circumferentially. Before releasing it from the bone, place a secure locking suture in the distal end of the tendon to maintain control and prevent retraction. Release the tendon sharply from the metatarsal base.
Return to the distal incision over the Achilles tendon. Incise the deep crural fascia overlying the lateral peroneal muscle compartment. Identify the peroneus brevis tendon at the base of this incision. Gently withdraw the peroneus brevis tendon proximally into the distal Achilles incision.
Pitfall: Tendinous interconnections (vincula) between the peroneus brevis and peroneus longus tendons distally are common. Strong, sustained traction may be required to withdraw the tendon, but sharp dissection of these bands through the fascial window is preferred to prevent iatrogenic rupture of the graft.
Once delivered into the distal Achilles wound, mobilize the muscular portion of the peroneus brevis proximally as far as possible to maximize its excursion and functional length.
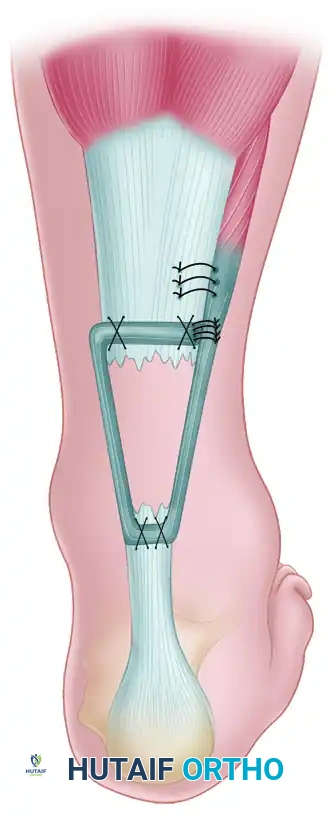
4. Graft Routing and Fixation
The core of the reconstruction involves weaving the harvested peroneus brevis through the native Achilles stumps to create a robust, biologically active bridge.
- Tenotomies: Make a longitudinal tenotomy (parallel to the tendon fibers) in the center of both the proximal and distal Achilles tendon stumps.
- Distal Passage: Use a curved hemostat or right-angle clamp to develop a plane through the distal Achilles tendon stump from lateral to medial. Pass the peroneus brevis graft through this distal tenotomy.
- Distal Fixation: With the ankle held in maximal plantar flexion (equinus), suture the peroneus brevis to both the lateral and medial sides of the distal Achilles stump using heavy non-absorbable or long-lasting absorbable sutures.
- Proximal Routing: Pass the free end of the peroneus brevis tendon subcutaneously beneath the intact skin bridge, directing it from the distal lateral incision into the proximal medial incision.
- Proximal Passage: Pass the graft from medial to lateral through the longitudinal tenotomy previously created in the proximal Achilles stump. Secure it under tension with multiple sutures.
- Final Construct: Finally, reflect the remaining tail of the peroneus brevis tendon back onto itself on the lateral side of the proximal incision and suture it securely, completing the dynamic loop.
Close the paratenon (if viable) and the subcutaneous tissues meticulously. Close the skin incisions in a standard fashion using non-absorbable monofilament sutures to minimize tissue reactivity. Apply a previously prepared, well-padded removable fiberglass cast or rigid splint with the foot locked in maximal equinus.
Alternative Technique: Calcaneal Tuberosity Drill Hole
In cases where the distal Achilles stump is severely degenerated, avulsed, or too short to accept a secure tendon weave, an alternative fixation method must be employed. The peroneus brevis can be anchored directly into the calcaneus.

- Exposure: The Achilles tendon and calcaneal tuberosity are exposed through a slightly more extensile posterolateral incision.
- Bone Tunnel: A transverse drill hole (bone tunnel) is created through the superior aspect of the calcaneal tuberosity.
- Graft Passage: The harvested peroneus brevis tendon is passed through this osseous tunnel from lateral to medial.
- Fixation: The graft is then routed proximally and sutured to the proximal Achilles tendon stump under appropriate resting tension.

If the plantaris tendon is intact and available, it can be harvested and passed in a figure-of-eight or weave pattern through the ruptured ends of the tendon to augment the repair biologically and mechanically, acting as a supplementary scaffold for fibroblastic ingrowth.
Postoperative Rehabilitation Protocol
The rehabilitation following a peroneus brevis transfer for a chronic Achilles rupture must be carefully phased. The construct relies on tendon-to-tendon healing, which requires strict protection in the early phases, followed by progressive mechanical loading to stimulate collagen realignment.
Phase I: Maximum Protection (Weeks 0 - 2)
* The patient is placed in a rigid fiberglass cast or fixed boot in maximal equinus (plantar flexion).
* Weight-bearing to tolerance on the metatarsal heads is permitted with the strict use of elbow crutches.
* Exercises: Active flexion and extension of the hallux and lesser toes are strongly encouraged to prevent tethering. Isometric exercises of the calf muscles and toes are initiated to maintain neuromuscular activation.
Phase II: Early Mobilization (Weeks 2 - 6)
* At the 2-week mark, the surgical wounds are inspected, and sutures are removed.
* The back shell of the cast is removed. Physical therapy commences, focusing heavily on proprioception, active plantar flexion, inversion, and eversion.
* Crucial Restriction: The front shell of the cast (or a dorsiflexion-blocking orthosis) must remain in place to absolutely prevent any passive or active ankle dorsiflexion past neutral, which would stretch and attenuate the transfer.
* Full weight-bearing is theoretically allowed with the front shell in place; however, due to altered biomechanics and balance difficulties, most patients will continue to require the assistance of a single elbow crutch or cane.
Phase III: Progressive Loading (Weeks 6 - 8+)
* At 6 weeks postoperatively, the front shell of the cast is permanently removed.
* Intensive physical therapy is initiated to restore full active range of motion.
* Patients normally regain a plantigrade ankle over the subsequent 2 to 3 weeks as the GSC and the transferred peroneus brevis adapt to the new resting length.
* Progressive resistance exercises, bilateral heel raises, and eventually unilateral heel raises are introduced as strength permits. Return to high-impact activities or sports is typically delayed until 6 to 9 months postoperatively, contingent upon the recovery of at least 80% isokinetic strength compared to the contralateral limb.
Conclusion
The transfer of the peroneus brevis tendon remains a cornerstone technique in the orthopaedic surgeon's armamentarium for addressing neglected Achilles tendon ruptures. By adhering to strict anatomical principles—particularly regarding the sural nerve—and ensuring meticulous tensioning of the graft, surgeons can reliably bridge defects up to 6 cm, restoring functional plantar flexion and significantly improving patient quality of life.
📚 Medical References
- for Achilles tendon rupture in athletes, Orthop Rev 17:822, 1988.
- Us AK, Biglin SS, Aydin T, et al: Repair of neglected Achilles tendon ruptures: procedures and functional results, Arch Orthop Trauma Surg 116:408, 1997.
- Vainionpää S, Böstman O, Pätiälä H, et al: Rupture of the quadriceps tendon, Acta Orthop Scand 56:433, 1985.
- van Reit RP, Morrey BF, Ho E, et al: Surgical treatment of distal triceps rupture, J Bone Joint Surg 85A:1961, 2003.
- Vardakas DG, Musgrave DS, Varitimidis SE, et al: Partial rupture of the distal biceps tendon, J Shoulder Elbow Surg 10:377, 2001.
- Vastamäki M, Brummer H, Solonen KA: Avulsion of the distal biceps brachii tendon, Acta Orthop Scand 52:45, 1981.
- Wapner KL, Pavlock GS, Heckt PJ, et al: Repair of chronic Achilles tendon rupture with fl exor hallucis longus
You Might Also Like


