Neglected Achilles Tendon Rupture Repair: Surgical Guide

Key Takeaway
Neglected Achilles tendon ruptures present significant reconstructive challenges due to tendon retraction and scar interposition. Direct repair often requires advanced tissue mobilization. This guide details the Bosworth gastrocnemius fascial turn-down flap and the Abraham and Pankovich V-Y advancement techniques. Both methods bridge critical defects, restoring the musculotendinous length-tension relationship essential for optimal plantar flexion power and functional recovery in chronic rupture scenarios.
INTRODUCTION TO NEGLECTED ACHILLES TENDON RUPTURES
The management of a neglected or chronic Achilles tendon rupture—typically defined as a rupture presenting more than four to six weeks post-injury—poses a formidable challenge to the orthopaedic surgeon. Unlike acute ruptures, where the tendon ends can often be approximated with minimal tension, neglected ruptures are characterized by significant proximal retraction of the triceps surae, extensive scar tissue interposition, and fatty infiltration or atrophy of the gastrocnemius-soleus complex.
Attempting a primary end-to-end repair in these scenarios is frequently impossible without excessive tension, which invariably leads to equinus contracture, wound breakdown, or catastrophic re-rupture. Consequently, bridging the defect requires advanced reconstructive techniques. The primary goals of surgical intervention are to restore the anatomical length-tension relationship of the musculotendinous unit, bridge the fibrotic gap with viable autogenous tissue, and restore the patient's plantar flexion power for normal gait biomechanics.
Two of the most historically reliable and biomechanically sound techniques for addressing these defects are the Bosworth Technique (utilizing a central gastrocnemius fascial turn-down flap) and the Abraham and Pankovich Technique (utilizing a V-Y tendinous advancement flap).
💡 Clinical Pearl
Preoperative magnetic resonance imaging (MRI) is indispensable in the evaluation of a neglected rupture. It allows the surgeon to accurately quantify the gap length (measured with the ankle in neutral), assess the degree of fatty infiltration in the muscle belly, and determine the viability of the remaining distal stump. A gap of 1 to 3 cm is highly amenable to V-Y advancement, whereas larger gaps may necessitate a Bosworth turn-down flap or flexor hallucis longus (FHL) transfer.
PREOPERATIVE PREPARATION AND POSITIONING
Patient Positioning
The patient is positioned prone on a radiolucent operating table. Chest rolls or a specialized prone frame should be utilized to ensure adequate pulmonary excursion. The knees should be positioned just distal to the break in the table to allow for intraoperative knee flexion, which is critical for assessing tendon tension.
Anesthesia and Hemostasis
General anesthesia or regional neuraxial anesthesia is employed. A well-padded pneumatic tourniquet is applied to the proximal thigh. Exsanguination of the limb is performed using an Esmarch bandage prior to tourniquet inflation to ensure a bloodless surgical field, which is critical for identifying the sural nerve and assessing tissue viability.
Surgical Draping
The entire lower extremity from the mid-thigh to the toes is prepped and draped in a standard sterile fashion. The foot must remain free to allow the surgeon to manipulate the ankle through a full range of motion, facilitating the assessment of resting tension and equinus positioning during the repair.
DIRECT REPAIR OF NEGLECTED RUPTURES: THE BOSWORTH TECHNIQUE
The Bosworth technique is a robust reconstructive option that utilizes a central strip of the gastrocnemius aponeurosis, left attached proximally, which is turned down and woven through the ruptured tendon ends. This technique not only bridges the defect but also provides a biological scaffold that enhances the mechanical strength of the repair.
Indications
- Neglected ruptures with a defect gap greater than 3 cm after debridement.
- Poor quality of the proximal or distal tendon stumps requiring augmentation.
- Revision of a failed primary Achilles tendon repair.
Surgical Approach and Debridement
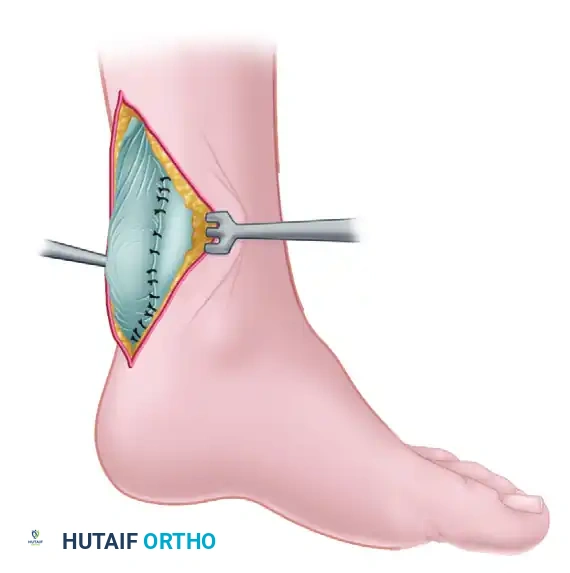
- Incision: Make a posterior longitudinal midline incision, extending from the calcaneal tuberosity to the proximal one-third of the calf. Full-thickness fasciocutaneous flaps must be maintained to preserve the fragile vascular supply to the posterior skin.
- Exposure: Incise the deep fascia and the paratenon longitudinally. Retract the paratenon carefully, as it will be required for closure to provide a gliding surface and vascularity to the healing tendon.
- Debridement: Expose the ruptured tendon ends. Using sharp dissection, meticulously excise the interposed fibrotic scar tissue until healthy, organized tendon fibers are encountered.
⚠️ Surgical Warning
Inadequate resection of the pseudotendon (scar tissue) will result in a repair that is prone to elongation and weakness. You must resect back to normal, glistening tendon tissue, even if this significantly increases the size of the defect.
Flap Harvest and Preparation
- Identify the Median Raphe: Expose the proximal gastrocnemius aponeurosis. Identify the median raphe of the gastrocnemius muscle.
- Harvest the Strip: Free a central strip of tendon from the median raphe. This strip must be precisely 1.5 cm wide and 17.5 to 22.5 cm long.
- Proximal Attachment: Crucially, leave the strip attached just proximal to the site of the rupture. This preserves the vascular tether and provides a strong biomechanical anchor point.
Tendon Weaving and Fixation
- Proximal Pass: Turn the harvested fascial strip distally. Pass it transversely through the center of the proximal tendon stump. Anchor it at this entry point with a heavy absorbable suture (e.g., #1 Vicryl or PDS) to prevent proximal propagation of the split.
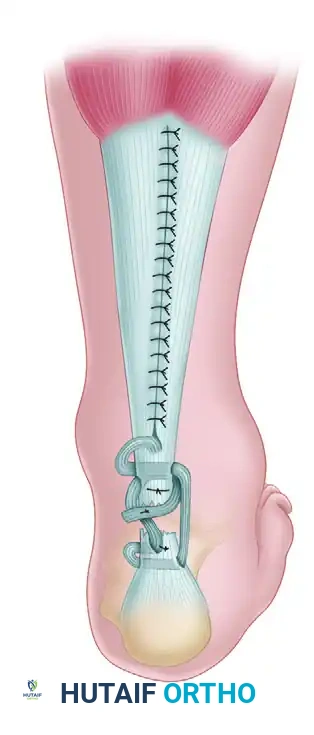
- Distal Weave: Pass the strip distally across the defect and then transversely through the distal end of the tendon (the calcaneal stump).
- Anterior-to-Posterior Pass: Pass the strip again through the distal stump, this time directing it from anterior to posterior to create a locking configuration.
- Tensioning the Construct: While an assistant holds the knee at 90 degrees of flexion and the ankle in 20 degrees of plantar flexion (to mimic resting physiological tension), draw the fascial strip tight. Anchor the strip to the distal stump using heavy nonabsorbable or chromic catgut sutures.
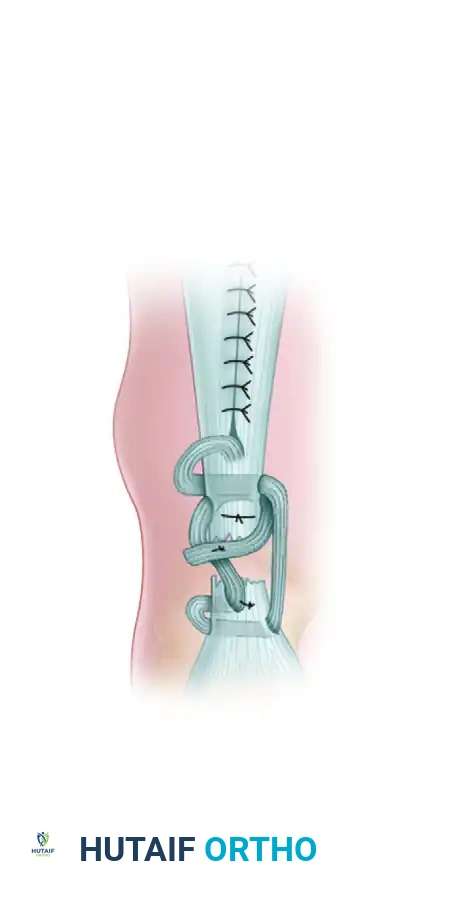
- Final Proximal Pass: Bring the remaining tail of the strip proximally across the defect. Pass it transversely through the proximal end of the tendon again, carry it distally, and suture it securely onto itself. This creates a robust, multi-stranded biological bridge.
- Closure of the Harvest Site: The defect in the proximal gastrocnemius aponeurosis is closed side-to-side with interrupted sutures to restore the integrity of the triceps surae complex.
Closure and Postoperative Care (Bosworth)
- Closure: The paratenon is closed meticulously over the repair with fine absorbable sutures (e.g., 3-0 Vicryl). The deep fascia, subcutaneous tissue, and skin are closed in a routine layered manner.
- Immobilization: Apply a well-padded long-leg cast. The knee must be held in 30 to 45 degrees of flexion, and the foot in gravity equinus (approximately 20 degrees of plantar flexion) to eliminate tension on the repair.
- Rehabilitation: Postoperative care mirrors that of an acute rupture repair. The long-leg cast is typically maintained for 4 weeks, followed by a transition to a short-leg cast or functional walker boot with heel wedges, progressively decreasing the equinus angle over the subsequent 4 to 6 weeks.
DIRECT REPAIR OF NEGLECTED RUPTURES: ABRAHAM AND PANKOVICH (V-Y ADVANCEMENT)
Abraham and Pankovich described an elegant V-Y tendinous advancement flap specifically designed for the repair of chronic ruptures. This technique relies on the proximal mobilization of the gastrocnemius aponeurosis to bridge the defect without sacrificing the structural continuity of the tendon.
Indications and Biomechanics
V-Y advancement is highly indicated when 1 to 3 cm of tendon must be resected after debridement of the scar tissue. It is also the procedure of choice if more than 80% of the tendon width is involved in the degenerative process. The biomechanical advantage of this technique is that it maintains the broad insertion of the gastrocnemius aponeurosis while allowing distal excursion, thereby preserving the muscle's force-generating capacity.
Surgical Approach
- Incision: With the patient prone and under tourniquet control, make a lazy "S" incision. Begin at the lateral aspect of the Achilles tendon insertion on the calcaneus, cross the midline gently, and extend to the midpart of the calf.
- Nerve Protection: Identify and retract the sural nerve. The nerve typically crosses from lateral to medial approximately 10 cm proximal to the calcaneal insertion. It is highly vulnerable during the lateral portion of the lazy "S" incision.
💡 Clinical Pearl
Sural nerve entrapment or transection is a devastating complication that leads to chronic lateral foot pain and numbness. Always dissect bluntly in the subcutaneous tissues laterally, and use a vessel loop to gently retract the nerve out of the surgical field.
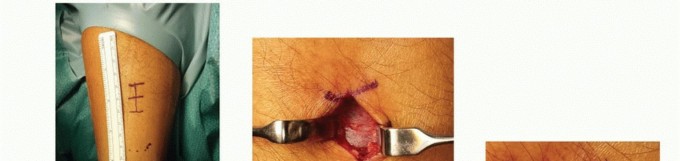
Defect Preparation and Measurement
- Fascial Incision: Incise the deep fascia in line with the skin incision.
- Debridement: Resect the fibrotic scar tissue from the tendon ends until healthy parallel collagen bundles are visible.
- Measurement: Position the knee in 30 degrees of flexion and the ankle in 20 degrees of plantar flexion. In this position, measure the exact length of the tendon defect. This measurement dictates the dimensions of the proximal V-cut.
The V-Y Advancement Technique
- The Inverted-V Incision: Move proximally to the gastrocnemius aponeurosis. Make an inverted-V incision through the aponeurosis, positioning the apex over its central, most proximal part.
- Calculating Arm Length: The arms of the V-incision must be at least one and a half (1.5x) times longer than the measured tendon defect. This geometric ratio is critical; it allows the aponeurosis to slide distally and be approximated in a Y configuration without excessive tension.
- Distal Advancement: Pull the mobilized aponeurotic flap distally.
- Tendon Approximation: Approximate the ends of the ruptured tendon. Secure the repair using a core suture technique (e.g., Krackow or Kessler) with heavy, interrupted nonabsorbable sutures (e.g., #2 FiberWire or Ethibond).
- Proximal Y-Closure: Return to the proximal aponeurosis. Close the proximal part of the inverted-V incision in a Y configuration using interrupted sutures. This secures the lengthened aponeurosis in its new, advanced position.
Closure and Postoperative Care (Abraham and Pankovich)
- Paratenon Closure: Suture the peritenon circumferentially over the repair site with interrupted nonabsorbable or slowly absorbable sutures. This step is vital to prevent skin adherence to the tendon.
- Layered Closure: Close the deep fascia and subcutaneous tissue in a routine manner. Skin closure should be performed with non-absorbable monofilament (e.g., 3-0 Nylon) using a vertical mattress technique to minimize edge ischemia.
- Initial Immobilization: Apply a long-leg cast with the knee in 30 degrees of flexion and the ankle in 20 degrees of plantar flexion.
- Rehabilitation Protocol:
- Weeks 0-6 (or 8): The patient remains non-weight-bearing in the long-leg cast.
- Weeks 6-10: The long-leg cast is removed. A short-leg cast (or rigid CAM boot) is applied, and the patient is allowed to begin protected weight-bearing. This is worn for 1 month.
- Months 2.5 - 3.5: After cast removal, a 3- to 5-cm heel lift is placed in the patient's shoe for 1 month. Progressive, active stretching and strengthening exercises are initiated immediately under the guidance of a physical therapist.
COMPLICATIONS AND PITFALLS IN CHRONIC REPAIRS
Reconstruction of neglected Achilles ruptures carries a higher complication profile than acute repairs. Surgeons must be vigilant regarding the following:
- Wound Breakdown and Infection: The posterior ankle has a tenuous blood supply. Excessive tension on the skin edges, aggressive retraction, or failure to close the paratenon can lead to skin necrosis. If the tendon is exposed, a reverse sural artery flap or free tissue transfer may be required.
- Sural Nerve Injury: As noted, the sural nerve is at risk during both the initial incision and the proximal harvest of the aponeurosis. Meticulous identification is mandatory.
- Over-lengthening (Weakness): If the tendon is repaired with too much slack (failure to adequately tension the Bosworth weave or the V-Y advancement), the patient will suffer from permanent push-off weakness and a calcaneus gait. Intraoperative resting tension must match the contralateral side.
- Re-rupture: While the Bosworth and V-Y techniques provide excellent structural integrity, patient non-compliance during the early postoperative phase (premature weight-bearing or forced dorsiflexion) can lead to catastrophic failure of the repair. Strict adherence to the phased rehabilitation protocol is non-negotiable.
You Might Also Like