Achilles Tendon Augmentation of Superior Peroneal Retinaculum Repair (Jones Technique)

Key Takeaway
The Jones technique for Achilles tendon augmentation of the superior peroneal retinaculum is a robust surgical intervention for chronic peroneal tendon subluxation. By utilizing a distally based slip of the Achilles tendon routed through the lateral malleolus, surgeons can reconstruct an incompetent retinaculum. This guide details the indications, biomechanics, step-by-step surgical approach, and postoperative protocols to optimize patient outcomes and prevent recurrent instability.
ACHILLES TENDON AUGMENTATION OF SUPERIOR PERONEAL RETINACULUM REPAIR (JONES TECHNIQUE)
Peroneal tendon subluxation and dislocation are debilitating conditions that frequently result from sudden, forceful dorsiflexion and inversion of the ankle, leading to the avulsion or attenuation of the superior peroneal retinaculum (SPR). While acute injuries may occasionally be managed conservatively or with direct anatomic repair, chronic instability, recurrent subluxation, or cases involving a severely deficient SPR often require robust tissue augmentation.
The Jones technique provides a highly reliable, autologous reconstruction by utilizing a distally based slip of the Achilles tendon. This slip acts as a biological check-rein, effectively replacing the incompetent SPR and preventing anterior translation of the peroneus longus and brevis tendons over the lateral malleolus.
Pathoanatomy and Biomechanics
The superior peroneal retinaculum is the primary restraint to peroneal tendon subluxation. It originates from the posterolateral margin of the distal fibula and inserts onto the lateral wall of the calcaneus. During ankle dorsiflexion and eversion, the peroneal tendons undergo significant tension, creating an anteriorly directed vector force. If the SPR is compromised, the tendons bowstring anteriorly out of the retromalleolar groove.
The Jones procedure biomechanically neutralizes this bowstringing effect. By routing a robust strip of the Achilles tendon through an osseous tunnel in the lateral malleolus, the surgeon creates an unyielding, dynamic restraint that mimics the native vector of the SPR while preserving the gliding mechanism of the peroneal tendons within their synovial sheaths.
Clinical Pearl: Always evaluate the depth of the retromalleolar groove. In up to 30% of patients with chronic peroneal instability, the fibular groove is convex or flat. The Jones technique may be performed in isolation, but if severe osseous dysplasia is present, it should be combined with a fibular groove-deepening procedure to ensure optimal biomechanical stability.
Preoperative Evaluation
Diagnosis is primarily clinical, characterized by a history of lateral ankle pain, a "snapping" sensation, and visible or palpable subluxation of the tendons over the lateral malleolus during active eversion and dorsiflexion against resistance.
Imaging should include weight-bearing radiographs to rule out avulsion fractures of the lateral malleolus (the "fleck sign") and to assess hindfoot alignment. A varus hindfoot is a known risk factor for failure and must be corrected concomitantly if present. Magnetic Resonance Imaging (MRI) or dynamic ultrasound is highly recommended to evaluate the integrity of the SPR, the presence of longitudinal split tears in the peroneus brevis, and the morphology of the retromalleolar groove.
SURGICAL TECHNIQUE: THE JONES PROCEDURE
Positioning and Preparation
- Anesthesia: General or regional anesthesia is administered.
- Positioning: The patient is placed in the lateral decubitus position with the operative leg up. Alternatively, a prone position can be utilized if bilateral procedures or extensive posterior Achilles work is anticipated.
- Tourniquet: A well-padded thigh or proximal calf tourniquet is applied and inflated after exsanguination to ensure a bloodless surgical field.
Incision and Exposure
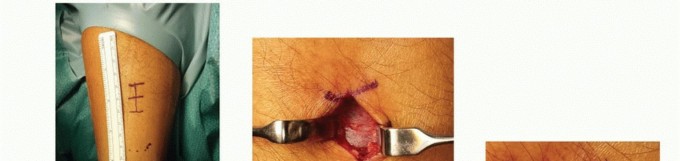
Make a longitudinal incision approximately 5 cm in length, positioned just posterior to the posterior margin of the lateral malleolus. The incision should extend distally toward the calcaneus, following the course of the peroneal tendons.
Surgical Warning: The sural nerve and the short saphenous vein course in close proximity to the surgical field, typically crossing from posterior to anterior near the distal extent of the incision. Meticulous blunt dissection in the subcutaneous tissues is mandatory to prevent iatrogenic neuroma formation or chronic regional pain syndrome (CRPS).
Tendon Inspection and Preparation
Carefully incise the superficial fascia. Identify the peroneal tendon sheath. Without disturbing the integrity of their synovial sheaths more than necessary for inspection, replace the subluxated peroneal tendons into their normal anatomic position behind the lateral malleolus. If longitudinal split tears of the peroneus brevis are identified, they should be tubularized and repaired with 4-0 non-absorbable suture prior to retinacular reconstruction.
Harvesting the Achilles Flap
Identify and expose the lateral border of the Achilles tendon. Using a #15 blade, dissect a longitudinal flap from the lateral aspect of the Achilles tendon.
* Dimensions: The flap should be approximately 5 cm long and 0.6 cm wide.
* Base: It is critical to leave the distal insertion of this flap firmly attached to the calcaneus to maintain its vascularity and biomechanical anchor.
Osseous Tunnel Preparation
Expose the distal lateral malleolus. Using a 3.2 mm or 4.0 mm drill bit (depending on patient size), drill a transverse hole through the lateral malleolus in a strictly anteroposterior direction. The tunnel should be positioned approximately 1.5 to 2.0 cm proximal to the distal tip of the fibula to avoid stress risers and potential iatrogenic fracture.
Figure 1: Preparation of the osseous tunnel through the lateral malleolus in an anteroposterior direction.
Flap Passage and Fixation
Pass a suture loop or a Hewson suture passer through the fibular tunnel from anterior to posterior. Secure the free, proximal end of the harvested Achilles flap and draw it through the osseous hole from posterior to anterior.
Tension the flap with the ankle held in neutral dorsiflexion and slight eversion. The flap should act as a firm check-rein over the peroneal tendons. Once optimal tension is achieved, fold the free end of the flap back onto itself and suture it securely using #0 or 2-0 non-absorbable braided sutures. Additional sutures should be placed anchoring the flap to the robust periosteum of the lateral malleolus to reinforce the construct.
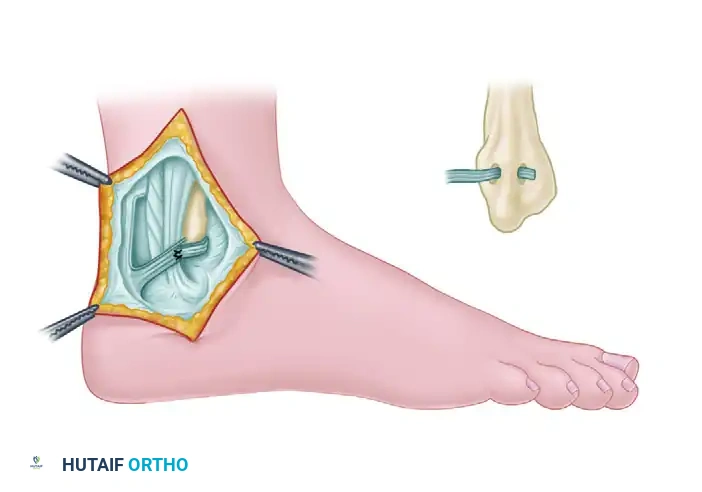
Figure 2: The completed Jones technique. The distally based Achilles flap is routed through the lateral malleolus, acting as a robust check-rein to prevent peroneal tendon displacement.
Closure
Thoroughly irrigate the wound. Ensure that the peroneal tendons glide smoothly beneath the newly constructed retinaculum without impingement. Close the subcutaneous tissue with 2-0 or 3-0 absorbable sutures and the skin with non-absorbable nylon or staples. Apply a sterile dressing and place the limb in a well-padded short-leg splint with the ankle in neutral to slight plantarflexion and slight eversion.
POSTOPERATIVE PROTOCOL
The postoperative rehabilitation following a Jones procedure must balance the protection of the soft-tissue reconstruction with the prevention of peritendinous adhesions.
- Weeks 0-2: The patient is strictly non-weight-bearing in a short-leg splint. Elevation is emphasized to control edema.
- Weeks 2-4: Sutures are removed. The patient is transitioned to a controlled ankle motion (CAM) boot. Non-weight-bearing is maintained. Gentle, active range-of-motion (ROM) exercises in plantarflexion and dorsiflexion are initiated to prevent adhesions. Inversion and eversion are strictly prohibited.
- Weeks 4-6: Progressive partial weight-bearing is initiated in the CAM boot. Early (4 weeks) ROM exercises are critical at this stage to avoid stiffness and limit motion restriction caused by peroneal tendon adhesions.
- Weeks 6-12: Transition to full weight-bearing in a supportive brace. Physical therapy focuses on peroneal strengthening, proprioception, and closed-kinetic-chain exercises.
- Months 3-6: Gradual return to sports and high-impact activities, contingent upon the restoration of symmetric strength and pain-free dynamic stability.
COMPLICATIONS AND MANAGEMENT
Complications of operative treatment for peroneal tendon subluxation require prompt recognition and evidence-based management:
- Nerve Injury: Sural and superficial peroneal nerve injuries are the most common complications. This risk is minimized by meticulous surgical technique, avoiding excessive retraction, and identifying the nerves early in the dissection.
- Peroneal Tendon Adhesions: Postoperative scarring can tether the tendons, limiting hindfoot motion. Early (4 weeks) range-of-motion exercises are the most effective prophylactic measure against this complication.
- Stenosing Flexor Tenosynovitis: Overtightening of the reconstructed peroneal tendon sheath (the Achilles flap) can compress the tendons, leading to pain, swelling, and restricted excursion. Satisfactory tendon excursion with full ankle and hindfoot range of motion must be documented intraoperatively before final closure.
- Persistent Instability: Undertightening the Achilles flap or failing to address an inadequate (shallow or convex) fibular groove depth can lead to recurrent subluxation. Concomitant groove deepening is advised in dysplastic cases.
SECONDARY PATHOLOGY: BICEPS BRACHII TENDON INSTABILITY
Note: While evaluating complex tendinous instabilities, orthopedic surgeons must also be adept at managing upper extremity analogs, such as biceps brachii tendon instability, which shares similar biomechanical principles of retinacular failure.
The precise prevalence of isolated long head of the biceps (LHB) dislocation—often referred to as bicipital syndrome—remains debated. Some authors suggest it is more common than anterior shoulder subluxation and frequently misdiagnosed, whereas others consider isolated lesions extremely rare.
Most often, biceps syndrome is associated with a massive tear of the rotator cuff (specifically the subscapularis) or a fracture of the lesser tuberosity. These pathologies result in the incompetence of the bicipital groove–transverse humeral ligament complex, leading to medial displacement of the tendon.
In a landmark study of 200 patients with rotator cuff tears, biceps tendon instability was identified in 45% of cases. Of these, 80% were subluxations rather than frank dislocations. Posterior instability was the most common directional vector (53%), followed by anteroposterior (27%) and anterior (20%). Notably, subluxations can occur anteriorly or posteriorly, whereas true dislocations are exclusively anterior.
Arthroscopic Classification of Biceps Tendon Instability (Lafosse)
Based on extensive arthroscopic examinations, Lafosse et al. developed a comprehensive classification system for biceps tendon instability according to the direction, extent, and associated rotator cuff pathology (Box 48-7).
Box 48-7: Arthroscopic Classification of Biceps Tendon Instability
Direction of Instability:
* Anterior
* Posterior
* AnteroposteriorExtent of Instability:
* None
* Subluxation
* DislocationLesion Grade:
* 0 (Normal)
* I (Minor lesion)
* II (Major lesion)Rotator Cuff Tear/Lesion:
* A (Intact)
* B (Partial thickness)
* C (Full thickness)
Clinical Evaluation
The diagnosis of biceps instability relies heavily on a detailed history of anterior shoulder pain, often accompanied by a mechanical "popping" sensation when the biceps tendon is stressed.
Provocative Testing:
* Yergason Test: Resisted supination of the forearm with the elbow flexed to 90 degrees.
* Palpation: Tenderness over the bicipital groove with the shoulder abducted to 90 degrees, internally and externally rotated against moderate resistance, is highly suggestive.
* Note on Reliability: The O’Brien and Speed tests are generally not reliable for specifically detecting biceps brachii instability, as they frequently cross-react with SLAP lesions and generalized anterior shoulder pathology.
Imaging:
A specialized bicipital groove radiograph may reveal a shallow groove, a medial wall angle of less than 45 degrees, osteophyte formation, or a healed fracture of the lesser tuberosity. MRI or MR arthrography is the gold standard to confirm the diagnosis. A concomitant rotator cuff tear is frequently identified, and medial displacement of the LHB tendon may be visible on the external rotation axial views.
Surgical Treatment
Surgery is indicated for a persistently symptomatic shoulder that has failed conservative management. Based on the arthroscopic classification of biceps instability, biceps tenodesis is universally recommended for all anterior dislocations if they are not reliably reducible and stable.
Operative Approach:
1. Tenodesis: Tenodesis of the biceps tendon to the proximal humerus (subpectoral or suprapectoral) provides excellent pain relief and functional restoration.
2. Intraarticular Excision: The proximal intraarticular portion of the tendon must be excised through the rotator cuff interval to prevent mechanical catching within the glenohumeral joint.
3. Cuff Repair: Concurrent repair of associated rotator cuff pathology (especially the subscapularis) is mandatory.
4. Trauma Considerations: For acute injuries involving a fracture of the lesser tuberosity, anatomic fixation of the tuberosity and direct repair of the transverse humeral ligament should be performed. Chronic symptoms arising from a malunited fracture of the medial aspect of the intertubercular groove are best treated with primary tenodesis, followed by excision of the intraarticular tendon through a small incision in the rotator interval.
Differential Diagnosis Note: Chronic Exertional Compartment Syndrome
When evaluating patients for chronic lateral ankle and leg pain—particularly athletes presenting with suspected peroneal tendon subluxation—surgeons must maintain a high index of suspicion for Chronic Exertional Compartment Syndrome (CECS) of the lateral or anterior compartments. While peroneal instability presents with mechanical snapping and localized retromalleolar pain, CECS presents with crescendo pain during exertion, often accompanied by transient neurologic deficits (e.g., superficial peroneal nerve paresthesias). If CECS is suspected, dynamic intracompartmental pressure testing is required, and if confirmed, an endoscopically assisted or open minimal-incision fasciotomy may be indicated alongside or instead of retinacular reconstruction.
You Might Also Like