Knee Arthroplasty: Prosthesis Design, Biomechanics & Surgical Technique
Key Takeaway
Total knee arthroplasty (TKA) represents one of the most successful surgical interventions in modern orthopedics. This comprehensive guide details the evolution of prosthesis design, from early total condylar models to modern posterior-stabilized and constrained systems. It provides an in-depth analysis of knee biomechanics, precise surgical techniques, ligamentous balancing, and postoperative protocols, offering orthopedic residents and consultants an evidence-based framework for optimizing patient outcomes and implant survivorship.
Arthroplasty of the Knee: Principles, Biomechanics, and Surgical Masterclass
Total knee arthroplasty (TKA) is a cornerstone of modern orthopedic surgery, providing reliable pain relief and functional restoration for patients with end-stage degenerative joint disease. The success of this procedure relies heavily on a profound understanding of knee biomechanics, the evolution of prosthetic design, meticulous patient selection, and exacting surgical technique.
Modern Prosthesis Evolution and Design
Although many total knee designs predate the total condylar prosthesis designed by Insall and others, its introduction in 1973 marked the beginning of the modern era of TKA. This prosthesis design allowed mechanical considerations to outweigh the desire to reproduce anatomically the kinematics of normal knee motion. Influenced largely by the previous ICLH (Imperial College/London Hospital) design, both cruciate ligaments were sacrificed, with sagittal plane stability maintained by the articular surface geometry.
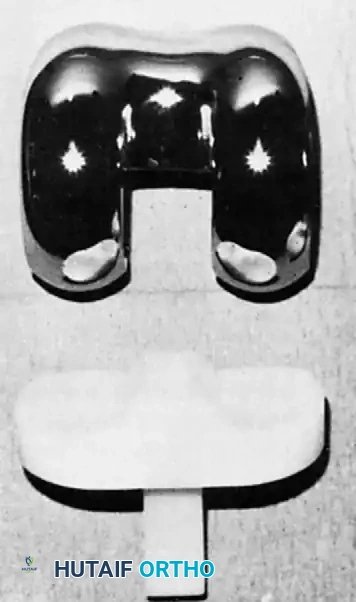
Fig. 6-1: The Total Condylar Prosthesis introduced by Insall in 1973, marking a paradigm shift in TKA survivorship.
The original cemented total condylar prosthesis dramatically reset the standard for survivorship of total knee replacements; Ranawat et al. reported a prosthetic survivorship of 94% at 15-year follow-up. The design included a chrome cobalt femoral component with a symmetrical anterior flange for patellar articulation. The symmetrical femoral condyles had a decreasing sagittal radius of curvature posteriorly and were individually convex in the coronal plane.
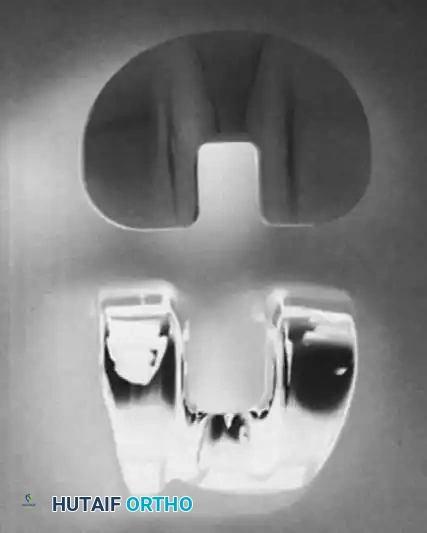
Supplementary View: Early component geometry emphasizing coronal congruency.
The double-dished articular surface of the tibial polyethylene component was perfectly congruent with the femoral component in extension and congruent in the coronal plane in flexion. Translation and dislocation of the components were resisted by the anterior and posterior lips of the tibial component and the median eminence. The tibial component had a metaphyseal stem to resist tilting of the prosthesis during asymmetrical loading. Originally all-polyethylene, metal backing was later added to allow more uniform stress transfer to the underlying cancellous metaphyseal bone and to prevent polyethylene deformation.
Concurrent with the development of the cruciate-sacrificing total condylar prosthesis, the duopatellar prosthesis was developed with the sagittal plane contour of the femoral component being anatomically shaped. This prosthesis included retention of the posterior cruciate ligament (PCL). The duopatellar prosthesis evolved into the kinematic prosthesis, which was widely used in the 1980s.

Fig. 6-2: Kinematic condylar prosthesis, illustrating the evolution toward anatomical shaping and PCL retention.
Two early criticisms of the total condylar prosthesis were its tendency to subluxate posteriorly in flexion if the flexion gap was not balanced perfectly with the extension gap, and a smaller range of flexion compared with prosthetic designs that allowed femoral rollback to occur. By not "rolling back," the posterior femoral metaphysis in a total condylar knee impinged against the tibial articular surface at approximately 95 degrees of flexion.

Fig. 6-3: Total condylar design is limited in flexion by posterior impingement of the femur on the tibial polyethylene component. With PCL retention or substitution, femoral rollback allows greater flexion.
To correct these problems, the Insall-Burstein posterior cruciate–substituting (posterior-stabilized or PS) design was developed in 1978 by adding a central cam mechanism to the articular surface geometry.

Fig. 6-4: Insall-Burstein II posterior-stabilized knee.
The cam on the femoral component engaged a central post on the tibial articular surface at approximately 70 degrees of flexion and caused the contact point of the femoral-tibial articulation to be posteriorly displaced, effecting femoral rollback and allowing further flexion. Most current total knee designs are derivatives of the Insall-Burstein and kinematic designs.
Deep-Dish and Highly Congruent Designs
During the late 1980s and 1990s, patellofemoral complications became the primary cause for reoperation in TKA. Newer designs incorporated greater areas of patellofemoral contact through a larger range of motion and asymmetrical anterior flanges designed to resist patellar subluxation. Some systems incorporated a deep-dish design as a modular tibial polyethylene option.

Fig. 6-5: Deep-dish component, utilizing sagittal plane concavity to control anteroposterior stability.
This design uses sagittal plane concavity or dishing alone to control anteroposterior stability. In comparing deep-dish components with posterior-stabilized devices, Laskin et al. found no difference at follow-up in range of motion or pain scores. They believed this design incorporated the advantages of cruciate sacrifice without the obligatory bone sacrifice in the intercondylar region of the femur required for a PS box, which may predispose to fracture.
Varus-Valgus Constrained Prostheses
The original constrained condylar knee (CCK) was developed by Insall and others from the posterior-substituting design by enlarging the central post of the tibial polyethylene insert, constraining it against the medial and lateral walls of a deepened central box of the femoral component.

Fig. 6-6: Insall-Burstein II constrained condylar knee (CCK).
Varus-valgus stability is controlled by this mechanism with a small amount of varus-valgus toggle allowed. It cannot be used for recurvatum deformity because it does not control hyperextension. The CCK design has been used extensively for revision arthroplasty when instability is present and for difficult primary arthroplasties in patients with extreme valgus deformity and medial collateral ligament insufficiency. Rosenberg, Verner, and Galante reported progressive bone loss and loosening in highly constrained hinged designs, which the CCK mitigates by allowing a controlled degree of toggle, thus reducing stress transfer to the cement-bone interface.
Mobile Bearing Prostheses
Mobile bearing knees, such as the Low Contact Stress (LCS) design, were introduced to reduce polyethylene wear by maximizing congruency while allowing the bearing to move relative to the tibial baseplate.

Supplementary View: Mobile bearing component demonstrating the rotating platform mechanism.
The LCS total knee system includes a rotating platform design with congruent tibiofemoral geometry in extension; however, the tibial polyethylene is additionally free to rotate within the stem of the tibial baseplate. Potential advantages include lower contact stresses at the articulating surfaces, rotational motion of the tibial polyethylene during gait, and self-alignment of the tibial polyethylene compensating for small rotational malalignment of the tibial baseplate during implantation.
Unicompartmental Prostheses
Many surgeons advocate the use of unicompartmental knee arthroplasty (UKA) for arthritis strictly limited to one knee compartment. These prostheses replace the articular surface of either the medial or the lateral femoral condyle and the adjacent tibial plateau surface.
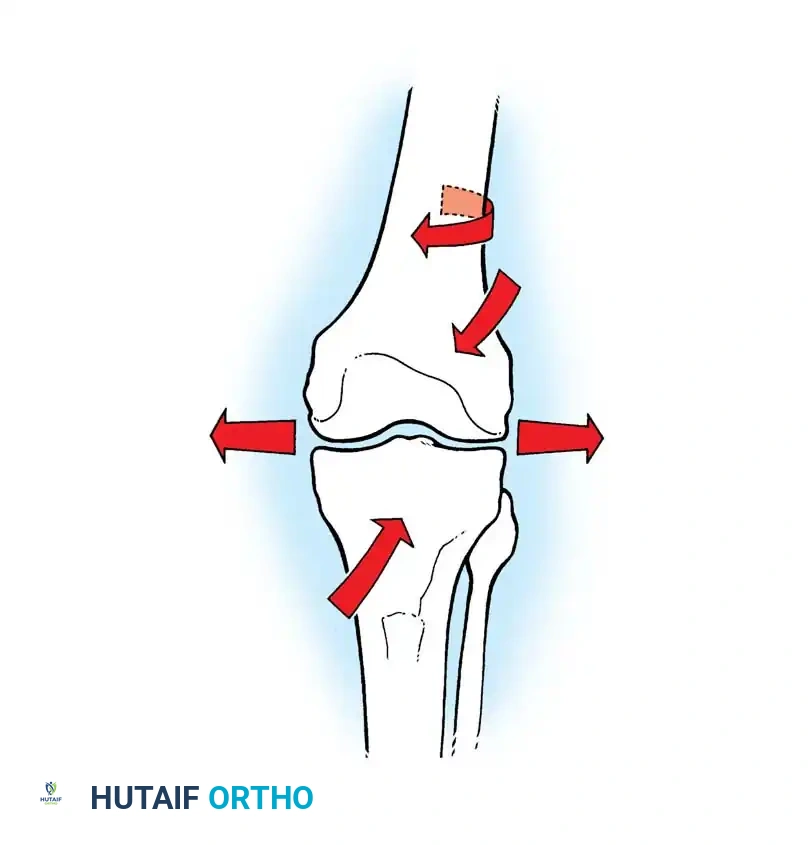
Fig. 6-7: Unicompartmental knee arthroplasty (UKA) components.
Supplementary View: UKA surgical application demonstrating isolated compartmental resurfacing.
The current trend toward minimally invasive surgery has rekindled enthusiasm for these devices. Strict indications include isolated medial or lateral osteoarthritis, an intact anterior cruciate ligament (ACL), a correctable varus or valgus deformity, and an absence of significant patellofemoral symptoms.
Biomechanics of Knee Arthroplasty
Understanding the kinematics of the native knee is essential for executing a successful arthroplasty. The knee is not a simple hinge joint; it exhibits complex polycentric motion involving rolling, gliding, and rotation.

Biomechanical representation of knee kinematics, illustrating the instantaneous center of rotation and polycentric motion.
Kinematics and Femoral Rollback
During early flexion (0 to 20 degrees), the femoral condyles primarily roll posteriorly on the tibial plateau. As flexion increases, the motion transitions to a combination of rolling and gliding, and eventually to pure gliding. This posterior translation of the femur on the tibia is termed femoral rollback. Rollback is critical because it moves the contact point posteriorly, clearing the posterior margin of the tibia and allowing deep flexion without impingement. In TKA, this is achieved either by retaining a functional PCL or by utilizing a cam-and-post mechanism in a PS design.
Axial and Rotational Alignment
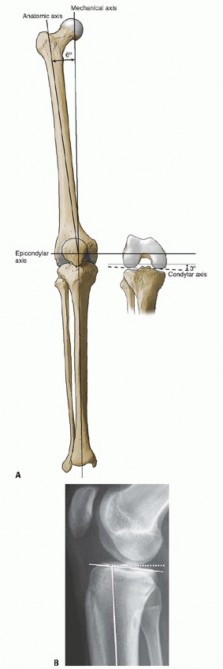
Restoration of the mechanical axis is a fundamental goal of TKA. The mechanical axis of the lower extremity is a line drawn from the center of the femoral head to the center of the ankle joint. In a neutrally aligned knee, this line passes precisely through the center of the knee joint.
* Femoral Cut: Typically made at 5 to 7 degrees of valgus relative to the anatomical axis of the femur to ensure the joint line is perpendicular to the mechanical axis.
* Tibial Cut: Made perpendicular to the mechanical axis of the tibia in the coronal plane, often with a 3 to 5-degree posterior slope in the sagittal plane to aid in flexion and PCL balancing.
Clinical Pearl: Malrotation of the femoral component, particularly internal rotation, is a leading cause of patellofemoral tracking issues, anterior knee pain, and premature polyethylene wear. The femoral component must be aligned parallel to the surgical transepicondylar axis (sTEA) or externally rotated 3 degrees relative to the posterior condylar axis.
Indications and Preoperative Evaluation
Patient Selection
TKA is indicated for patients with severe, radiographically confirmed osteoarthritis, rheumatoid arthritis, or post-traumatic arthritis who have failed exhaustive conservative management (e.g., NSAIDs, physical therapy, intra-articular injections, weight loss).
Contraindications include:
* Absolute: Active local or systemic infection, severe peripheral vascular disease, neuropathic arthropathy (Charcot joint) without specialized constrained implants, and a non-functioning extensor mechanism.
* Relative: Severe osteoporosis, poor soft-tissue coverage, and significant medical comorbidities precluding safe anesthesia.
Preoperative Templating
Standard weight-bearing anteroposterior (AP), lateral, and skyline patellar radiographs are mandatory. Full-length standing hip-to-ankle radiographs are highly recommended to assess the mechanical axis and identify any extra-articular deformities. Templating determines the approximate component sizes, the angle of the distal femoral resection, and the presence of bone defects requiring augments or stems.
Surgical Technique: Step-by-Step Masterclass
1. Positioning and Anesthesia
The procedure is typically performed under regional anesthesia (spinal or epidural) combined with a peripheral nerve block (e.g., adductor canal block) to optimize postoperative pain control and facilitate early mobilization. The patient is positioned supine. A pneumatic tourniquet is applied to the proximal thigh, and the leg is placed in a specialized leg holder allowing for hyperflexion and stable positioning.
2. Surgical Approach
The standard midline longitudinal incision is utilized, extending from the distal third of the quadriceps tendon to the medial border of the tibial tubercle.
* Medial Parapatellar Arthrotomy: The most common deep approach. The incision extends through the medial retinaculum, skirting the medial border of the patella, and extending proximally into the quadriceps tendon.
* Alternative Approaches: The midvastus or subvastus approaches may be used to spare the quadriceps tendon, potentially accelerating early straight-leg raise recovery, though they offer more limited exposure in stiff or obese knees.
3. Bone Preparation and Alignment
The principle of measured resection versus gap balancing dictates bone cuts. Most modern systems utilize a hybrid approach.
* Distal Femoral Resection: An intramedullary alignment rod is inserted into the femoral canal. The distal cutting block is set to the preoperatively templated valgus angle (usually 5-7 degrees). A measured resection (typically 9-10 mm, matching the thickness of the femoral component) is performed.
* Proximal Tibial Resection: An
You Might Also Like