Surgical Anatomy of the Knee: A Comprehensive Operative Guide
Key Takeaway
A profound understanding of knee surgical anatomy is paramount for orthopedic surgeons. This comprehensive guide details the complex interplay of osseous geometry, extraarticular tendinous structures, and ligamentous restraints. By mastering the biomechanics of the patellofemoral joint, the posterolateral corner, and the posteromedial complex, surgeons can optimize operative approaches, enhance joint stability, and ensure superior clinical outcomes in complex knee reconstructions and arthroplasty procedures.
INTRODUCTION TO KNEE BIOMECHANICS AND SURGICAL ANATOMY
The knee is one of the most frequently injured joints in the human body. Its vulnerability stems from its unique anatomical structure, its constant exposure to high-magnitude external forces, and the immense functional demands placed upon it during both activities of daily living and elite athletics. Basic to an understanding of knee injuries—and paramount to executing successful surgical interventions—is a profound mastery of normal knee anatomy.
Although historical emphasis has frequently been placed on the static ligaments of the knee, it is a fundamental biomechanical truth that without the dynamic supporting action of the associated muscles and tendons, the ligaments alone are insufficient to maintain joint stability. The structures surrounding the knee are classically categorized into three broad, interdependent categories: osseous structures, extraarticular structures, and intraarticular structures.
Clinical Pearl: When evaluating the traumatized knee, the surgeon must view the joint as a synergistic organ. An injury to the osseous geometry inevitably alters the tensioning of the extraarticular tendinous structures, which in turn compromises the static ligamentous restraints. Restoration of native kinematics requires addressing all three categories simultaneously.
OSSEOUS STRUCTURES AND ARTICULAR GEOMETRY
The osseous architecture of the knee consists of three primary components: the patella, the distal femoral condyles, and the proximal tibial plateaus (condyles). While traditionally simplified as a hinge joint (ginglymus), the knee's motion is vastly more complex. In addition to flexion and extension, its kinematic profile includes a critical rotary component, often referred to as the "screw-home" mechanism.
The Distal Femur
The femoral condyles are two rounded, eccentrically curved prominences. Anteriorly, the condyles are somewhat flattened, creating a broader surface area designed for optimal contact and weight transmission during extension. The condyles project minimally anterior to the femoral shaft but extend markedly posterior to it.
- Trochlear Groove: The anterior depression between the condyles forms the patellofemoral groove, or trochlea.
- Intercondylar Notch: Posteriorly, the condyles are separated by the intercondylar notch, which houses the cruciate ligaments.
- Condylar Asymmetry: The articular surface of the medial condyle is longer than that of the lateral condyle, yet the lateral condyle is wider. The long axis of the lateral condyle is oriented essentially along the sagittal plane, whereas the medial condyle typically diverges at approximately a 22-degree angle to the sagittal plane.
The Proximal Tibia
The expanded proximal end of the tibia forms two relatively flat surfaces—the medial and lateral plateaus—that articulate with the femoral condyles.
- Intercondylar Eminence: The plateaus are separated in the midline by the intercondylar eminence, featuring medial and lateral intercondylar tubercles.
- Attachment Sites: The areas immediately anterior and posterior to this eminence serve as the critical attachment footprints for the cruciate ligaments and menisci.
- Lateral Plateau Morphology: The posterior lip of the lateral tibial condyle is distinctly rounded off. This anatomical nuance accommodates the lateral meniscus as it slides posteriorly during deep knee flexion.
Surgical Warning: The articular surfaces of the knee are inherently incongruent. On the medial side, the femur meets the tibia like a "wheel on a flat surface," whereas on the lateral side, it resembles a "wheel on a dome." This lateral convexity contributes to the inherent rotary instability seen in anterior cruciate ligament (ACL) deficiencies (the pivot-shift phenomenon).
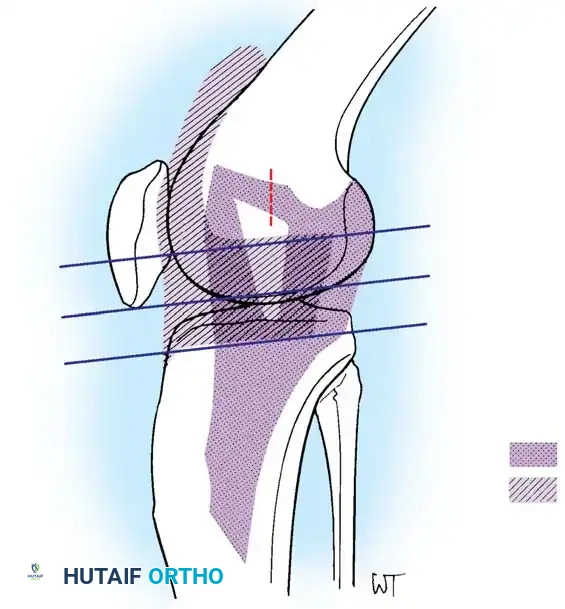
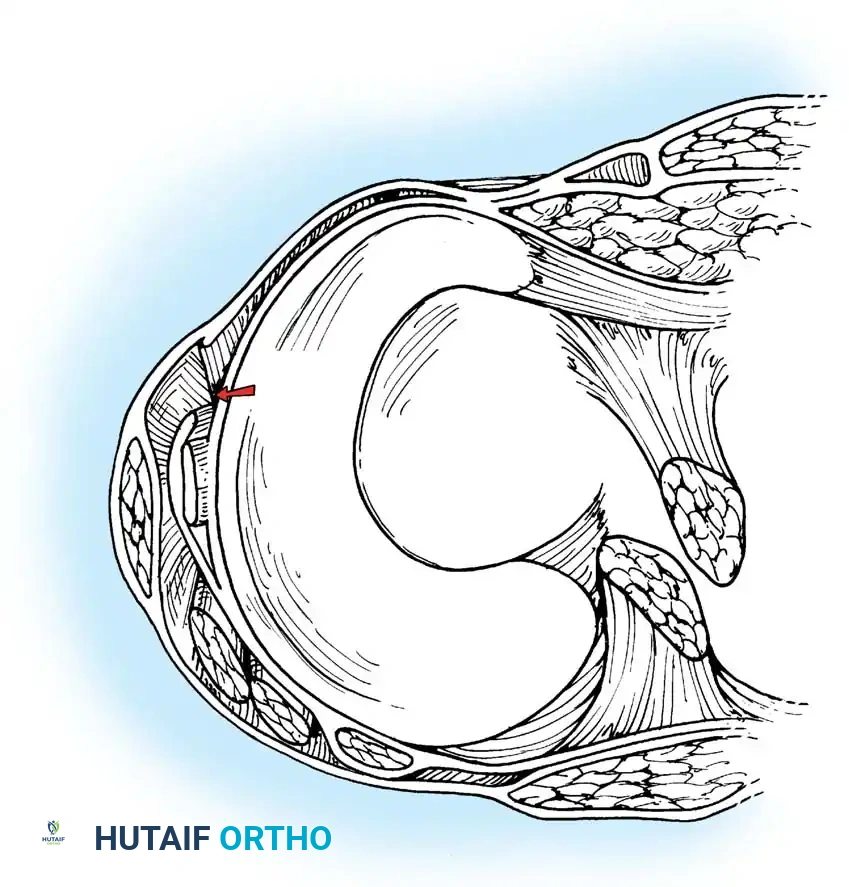
The Patellofemoral Articulation
The patella is a triangular sesamoid bone, wider at its proximal pole than at its distal apex. Its articular surface is divided by a vertical ridge into a smaller medial facet and a larger lateral facet.
- Extension: With the knee in full extension, the patella rides superior to the articular margin of the trochlear groove. The distal portion of the lateral facet articulates with the lateral femoral condyle, while the medial facet barely makes contact.
- Mid-Flexion (45 Degrees): Contact moves proximally to the midportion of the articular surfaces.
- Deep Flexion: In complete flexion, the proximal portions of both facets contact the femur. During the full arc of motion, the patella translates 7 to 8 cm relative to the femoral condyles. In deep flexion, significantly more pressure is applied to the medial facet.
EXTRAARTICULAR TENDINOUS STRUCTURES
The dynamic stability of the knee is governed by the musculotendinous units that span the joint. These include the quadriceps mechanism, the gastrocnemius, the medial and lateral hamstring groups, the popliteus, and the iliotibial band.
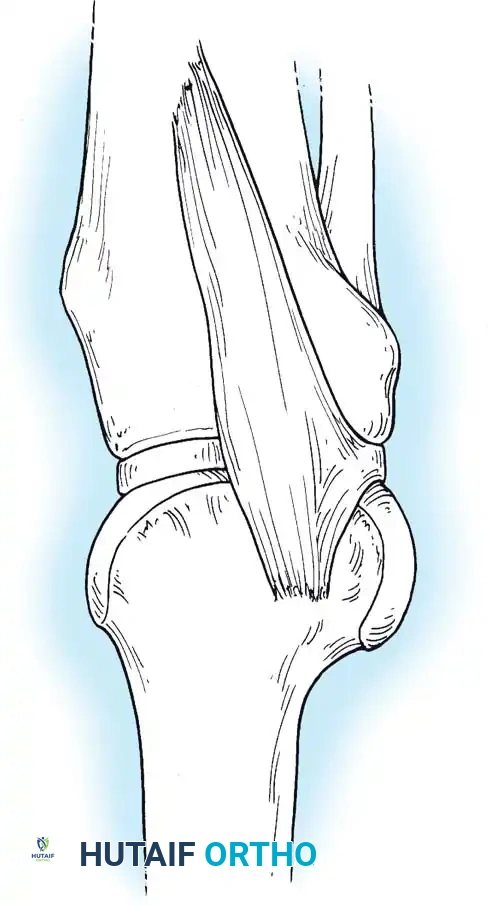
The Extensor Mechanism
The quadriceps mechanism forms a trilaminar tendon that inserts into the superior pole of the patella:
1. Anterior Layer: Formed by the rectus femoris, which flattens immediately above the patella to insert at the anterior edge of the proximal pole.
2. Middle Layer: Formed by the confluent aponeurotic edges of the vastus lateralis and vastus medialis.
3. Deep Layer: Formed by the vastus intermedius, inserting into the posterior edge of the proximal pole.
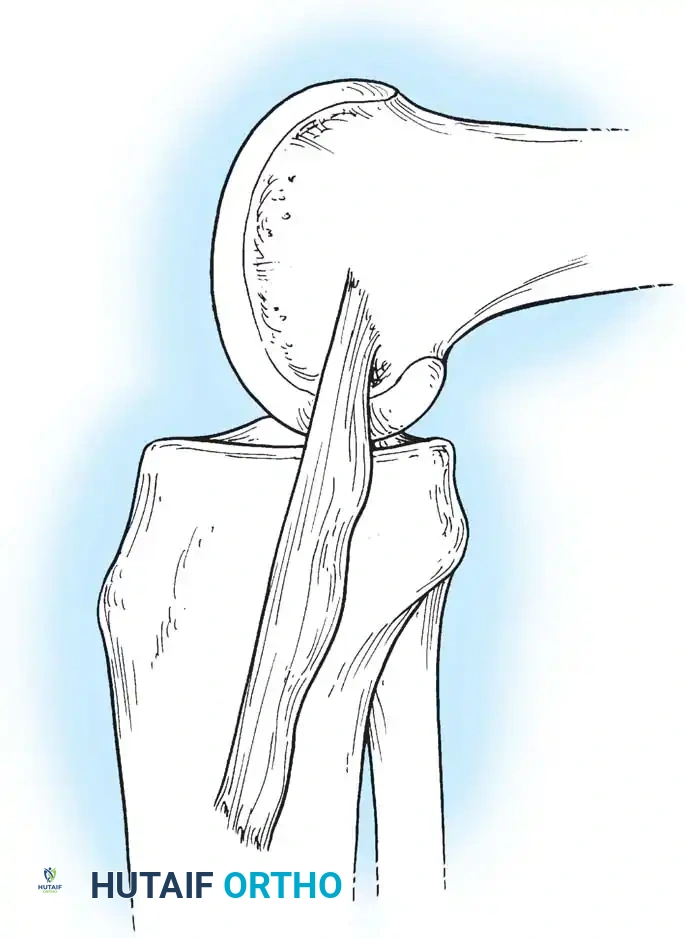
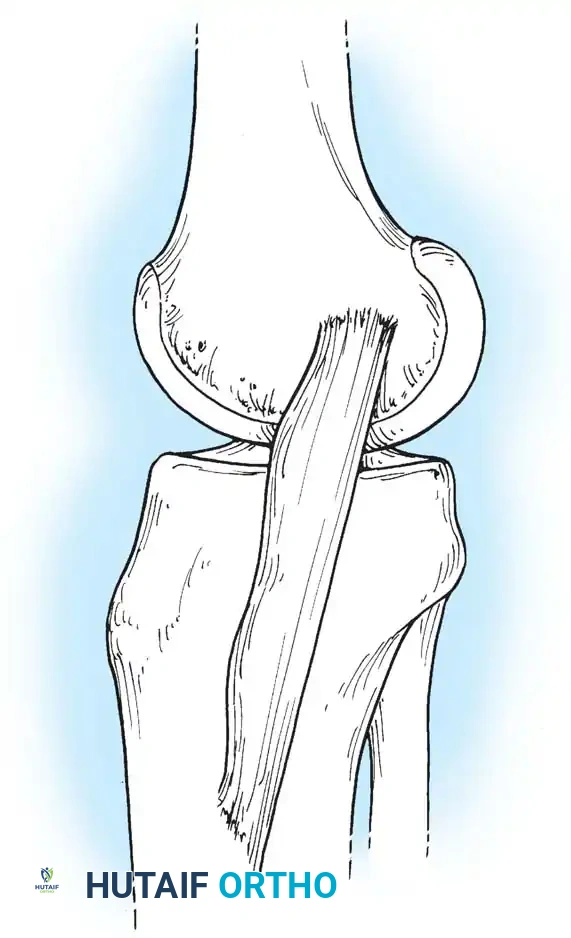
The medial retinaculum, derived from the vastus medialis aponeurosis, inserts directly into the medial border of the patella, acting as the primary dynamic restraint against lateral patellar subluxation. Distally, the patellar tendon originates from the apex of the patella and inserts into the tibial tuberosity.
The Medial and Posterior Flexors
The gastrocnemius spans the posterior aspect of the knee, intimately blending with the posterior capsule before inserting onto the posterior aspects of the medial and lateral femoral condyles.
The Pes Anserinus represents the conjoined insertion of the sartorius, gracilis, and semitendinosus muscles along the proximal anteromedial tibia. These primary knee flexors exert a secondary internal rotational force on the tibia, dynamically protecting the joint against valgus and rotary stresses.
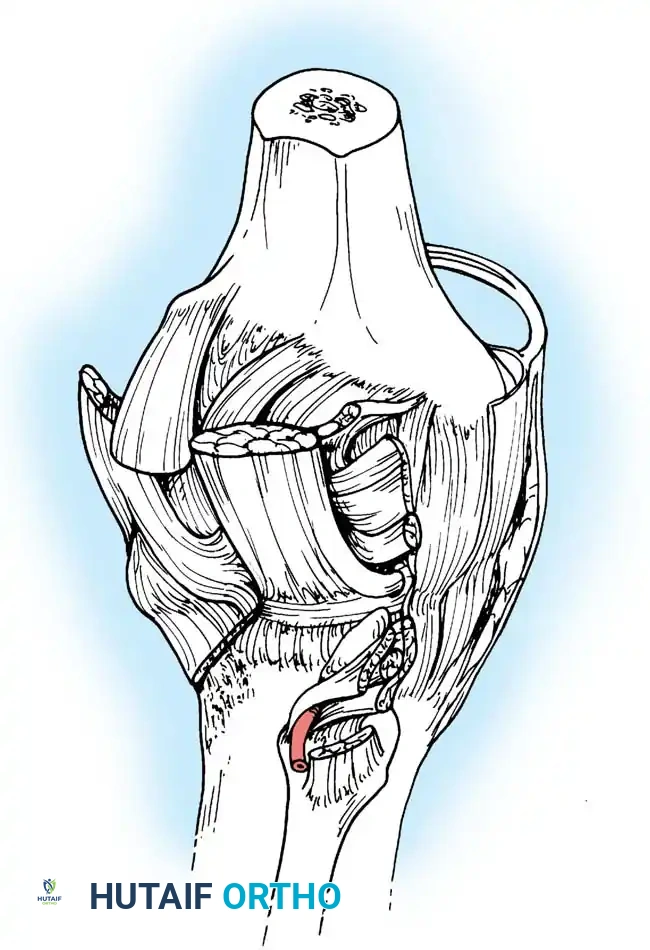
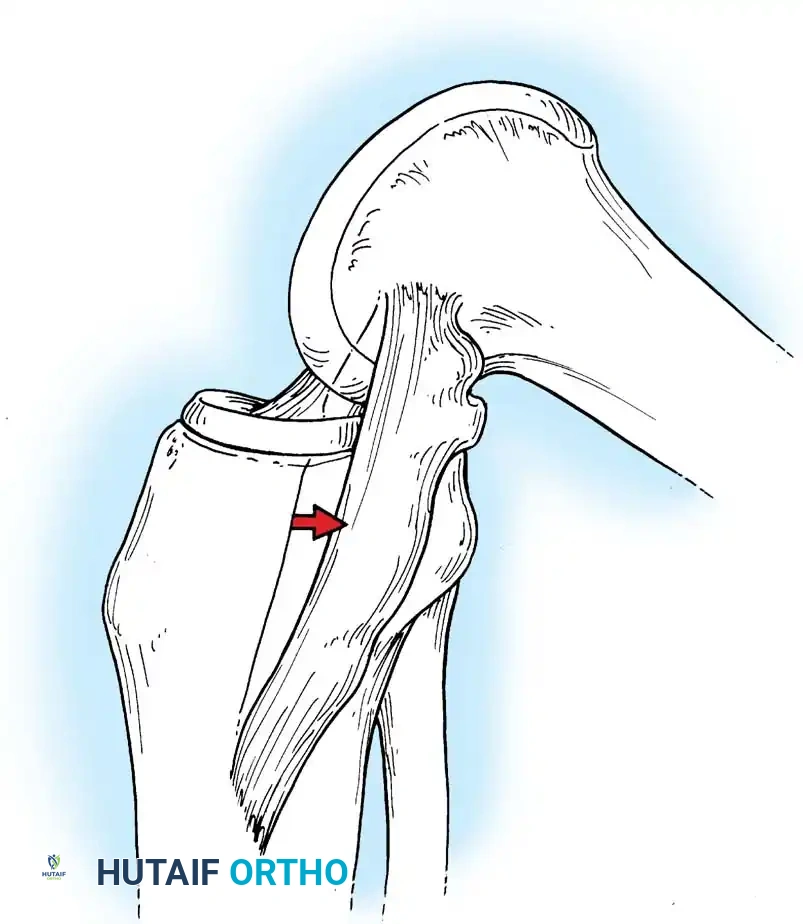
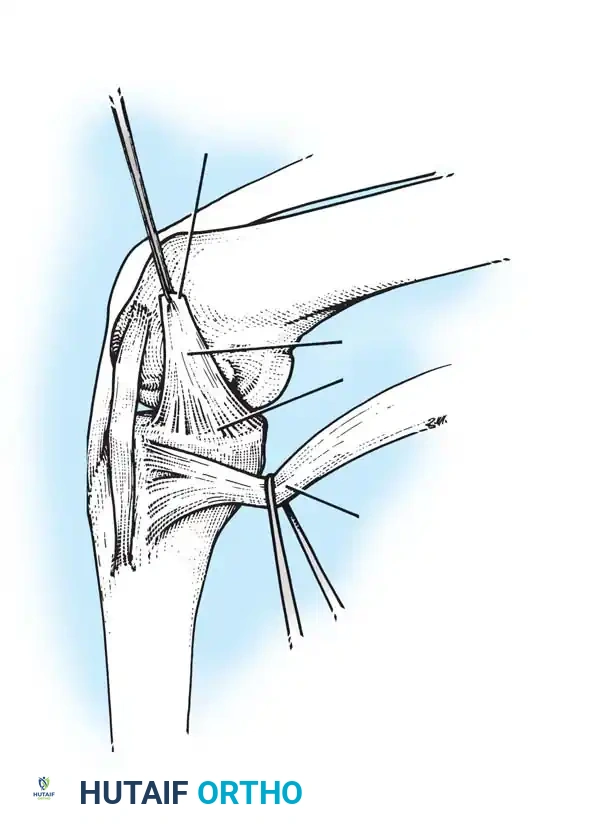
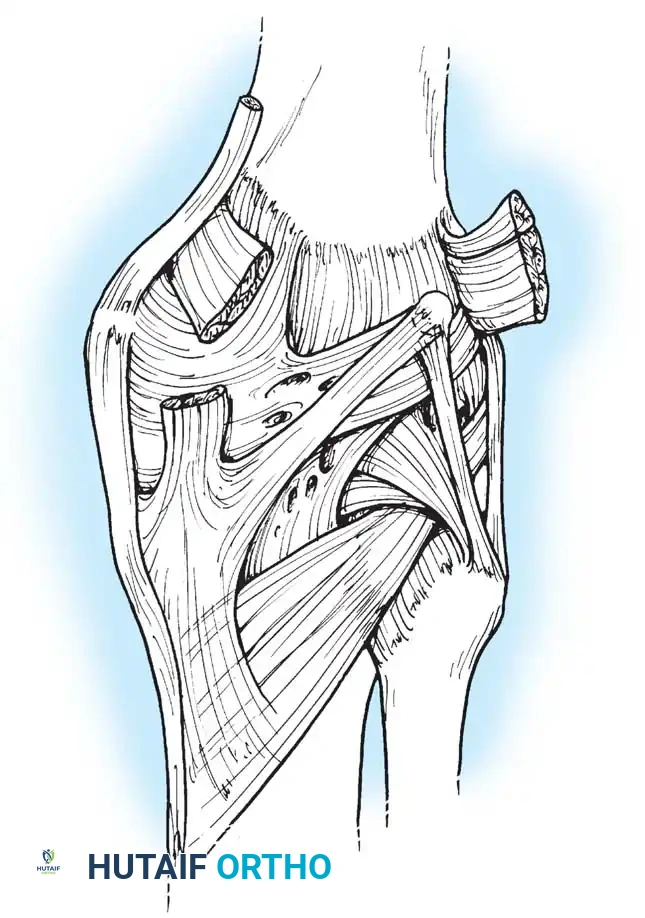
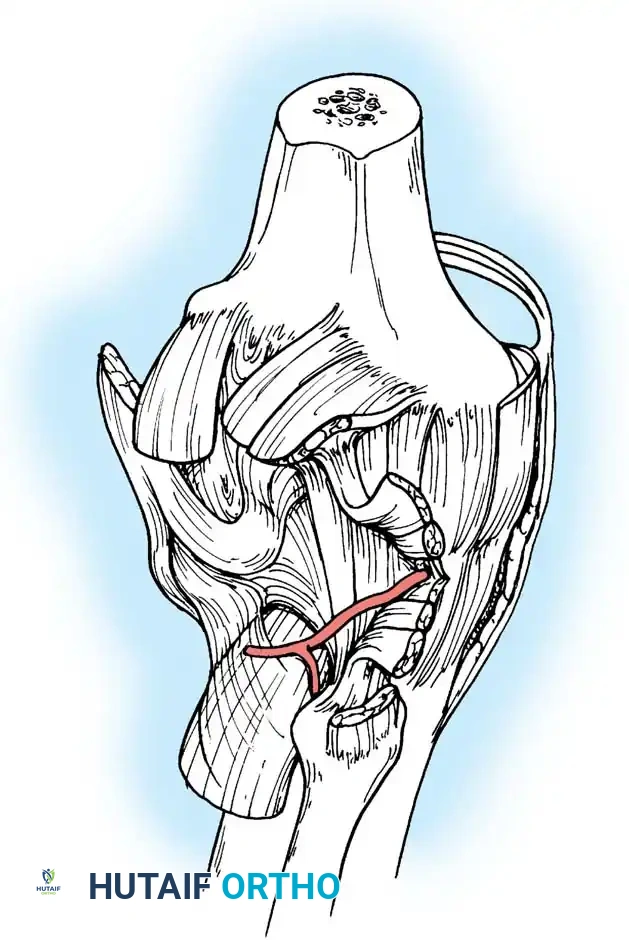
The Semimembranosus Complex
The semimembranosus is a paramount stabilizing structure of the posteromedial corner. It features five distinct distal expansions:
1. Oblique Popliteal Ligament (OPL): Passes obliquely upward and laterally toward the lateral gastrocnemius head. It is a crucial posterior stabilizer; contraction of the semimembranosus dynamically tenses the OPL.
2. Capsulomeniscal Extension: Attaches to the posterior capsule and posterior horn of the medial meniscus, pulling the meniscus posteriorly during flexion to prevent impingement.
3. Anterior (Deep) Head: Continues medially along the tibial flare, inserting beneath the superficial medial collateral ligament (sMCL).
4. Direct Head: Attaches to the posterior tibial tubercle just below the joint line. This provides a robust anchor point for posteromedial capsular surgical repairs.
5. Distal Expansion: Forms a fibrous expansion over the popliteus, fusing with the medial tibial periosteum.
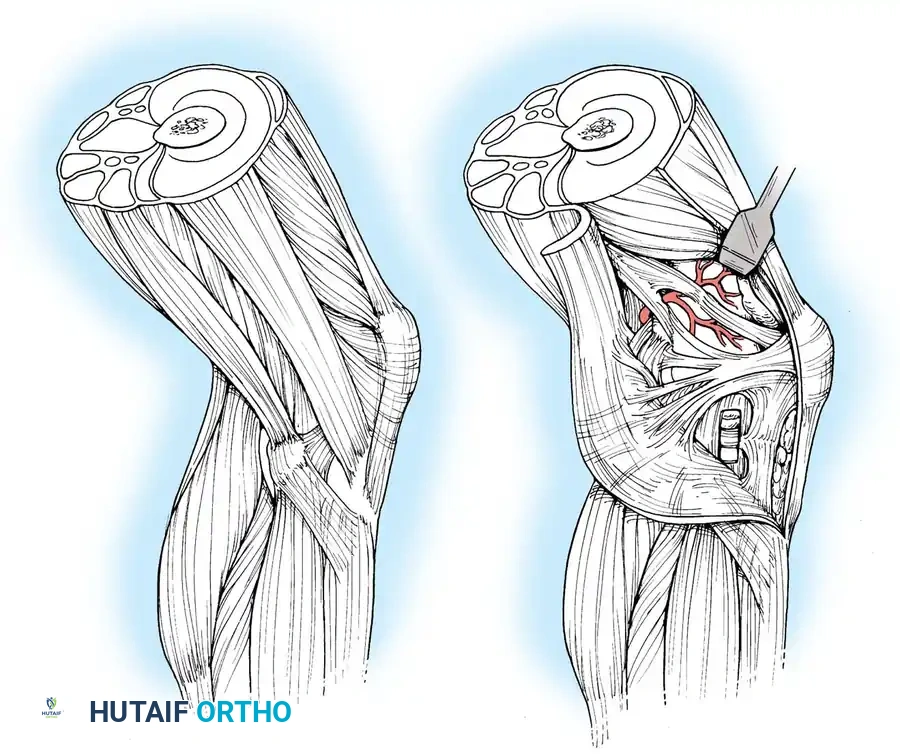
The Lateral and Posterolateral Structures
The lateral counterpart to the pes anserinus is the robust biceps femoris, which inserts into the fibular head, lateral tibia, and posterolateral capsule. It acts as a strong flexor and external rotator of the tibia, providing rotary stability by preventing anterior tibial translation during flexion.
The Iliotibial (IT) Band inserts into Gerdy's tubercle on the anterolateral tibia. It functions as an anterolateral ligamentous restraint. The IT band moves anteriorly in extension and posteriorly in flexion, remaining tense throughout the arc of motion.
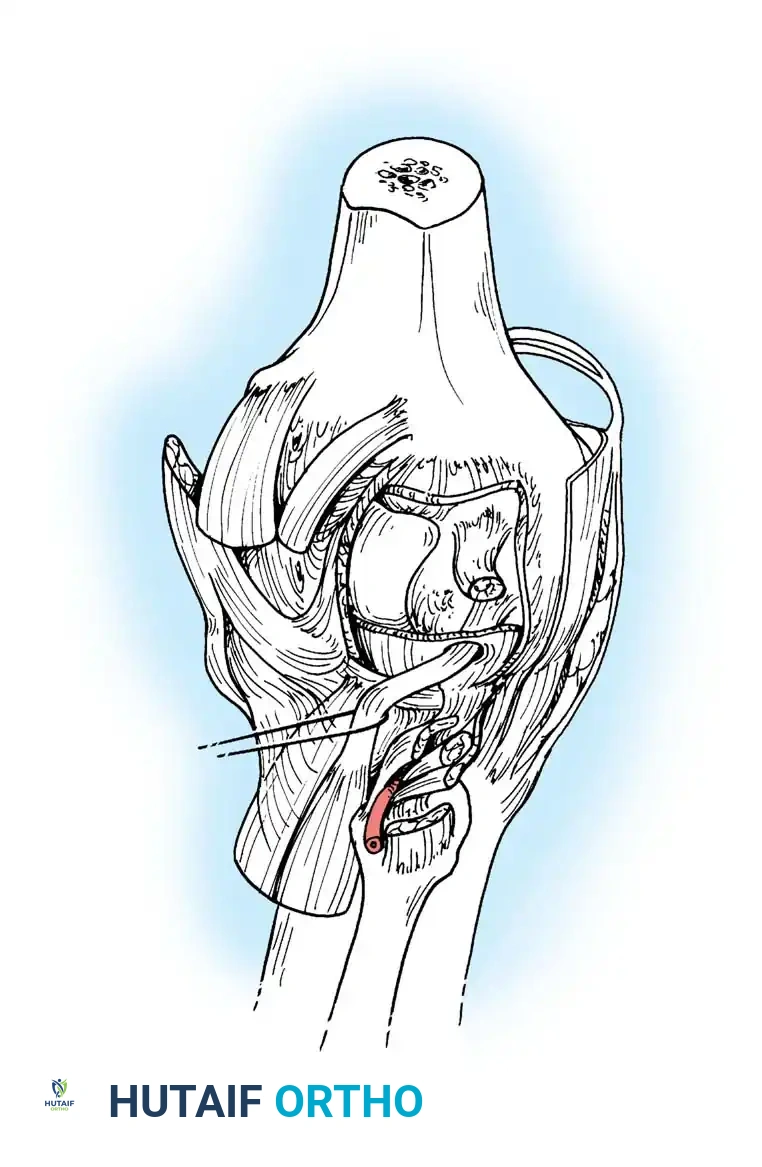
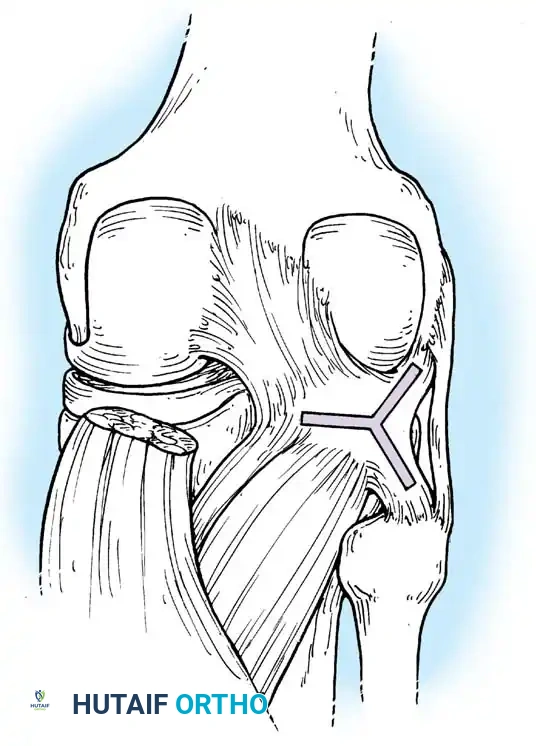
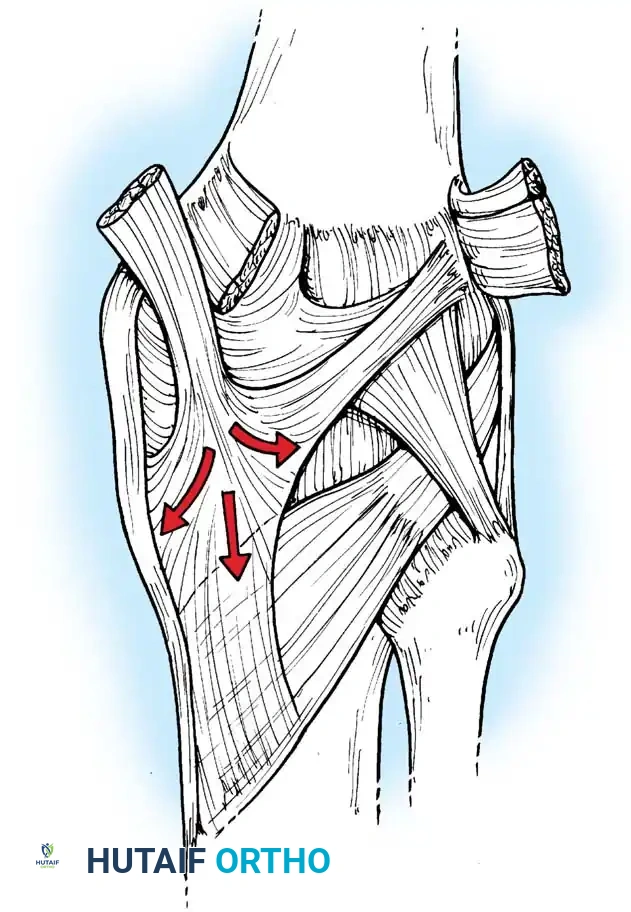
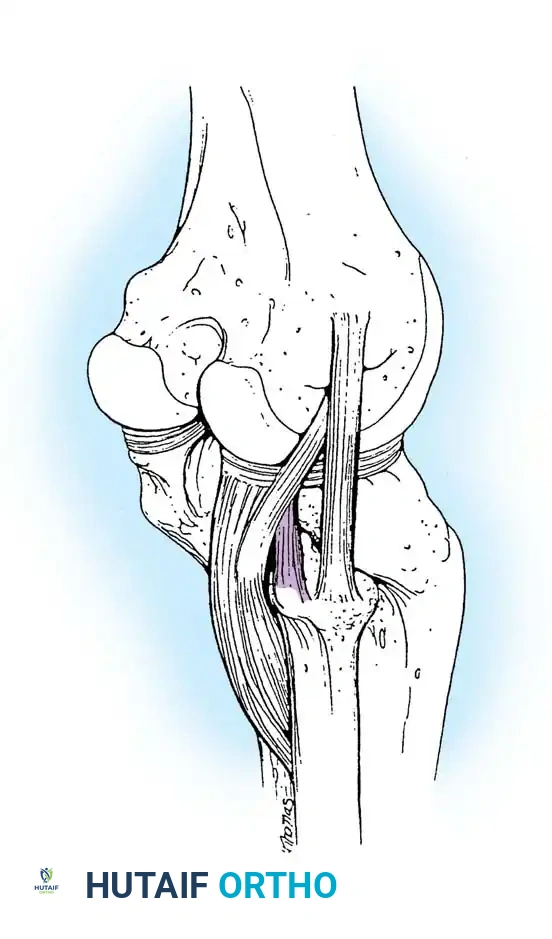
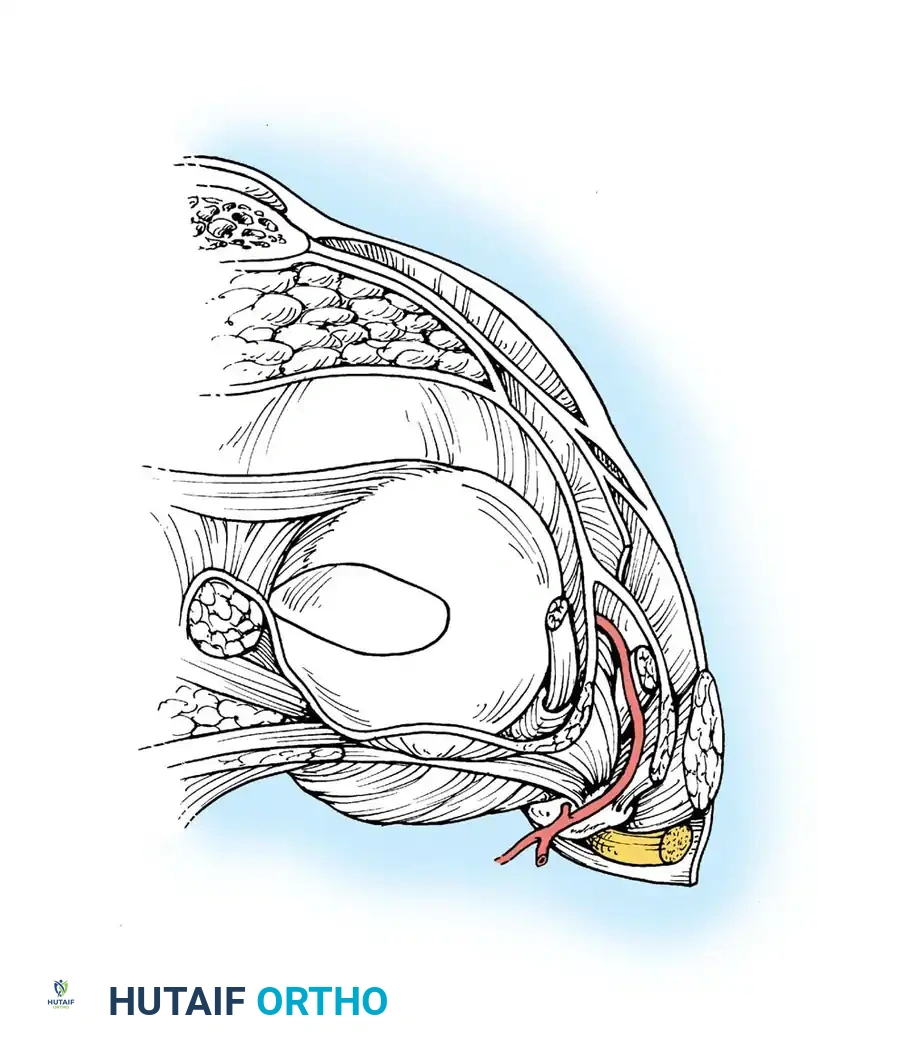
The Popliteus and Arcuate Complex
The popliteus muscle is a critical dynamic stabilizer with a tripartite origin:
1. Femoral Origin: The strongest attachment, originating from the lateral femoral condyle.
2. Fibular Origin: Forms the popliteofibular ligament.
3. Meniscal Origin: Attaches to the posterior horn of the lateral meniscus.
The femoral and fibular origins form the arms of the Y-shaped arcuate ligament. Electromyographic studies demonstrate that the popliteus is the primary internal rotator of the tibia during the initial stages of flexion (unlocking the knee) and actively retracts the lateral meniscus to prevent crushing.
EXTRAARTICULAR LIGAMENTOUS AND CAPSULAR STRUCTURES
The joint capsule and collateral ligaments form the primary static stabilizing framework. The capsule is a fibrous sleeve extending from the patella anteriorly to the posterior expanses of the joint.
- Meniscal Attachments: The menisci are firmly attached to the capsule peripherally. The medial attachment is highly secure (coronary ligaments), whereas the lateral attachment is interrupted by the popliteal hiatus, rendering the lateral meniscus more mobile.
- The Quadruple Complexes: Nicholas and Minkoff described the medial and lateral "quadruple complexes" as the principal stabilizers. The capsular structures, reinforced by the retinacula, collaterals, and hamstring/popliteus expansions, create a highly sophisticated check-rein system against varus, valgus, and rotational forces.
SURGICAL APPROACHES TO THE KNEE
Translating this complex anatomy into operative success requires precise surgical approaches. The choice of approach dictates the exposure of the osseous and ligamentous structures while minimizing iatrogenic soft-tissue morbidity.
1. Medial Parapatellar Approach (Von Langenbeck)
The workhorse approach for Total Knee Arthroplasty (TKA) and complex intraarticular tumor resections.
* Indications: TKA, distal femoral fractures, complex intraarticular visualization.
* Technique: A longitudinal midline skin incision is made. The arthrotomy begins proximal to the patella within the quadriceps tendon, leaving a 3-4 mm cuff of tendon on the vastus medialis for later repair. The incision skirts the medial border of the patella and extends distally along the medial border of the patellar tendon to the tibial tubercle.
* Anatomical Considerations: Care must be taken not to detach the patellar tendon from the tibial tubercle. The infrapatellar branch of the saphenous nerve is frequently sacrificed, leading to predictable lateral skin numbness.
2. Lateral Approach
Utilized for lateral plateau fractures and lateral compartment arthroplasty.
* Indications: Open Reduction Internal Fixation (ORIF) of lateral tibial plateau fractures, lateral unicompartmental knee arthroplasty.
* Technique: An anterolateral incision is made between Gerdy's tubercle and the fibular head. The IT band is incised in line with its fibers. The joint capsule is opened anterior to the lateral collateral ligament (LCL).
* Anatomical Considerations: The common peroneal nerve lies posterior to the biceps femoris and wraps around the fibular neck. Retraction must be meticulous to avoid traction neuropraxia.
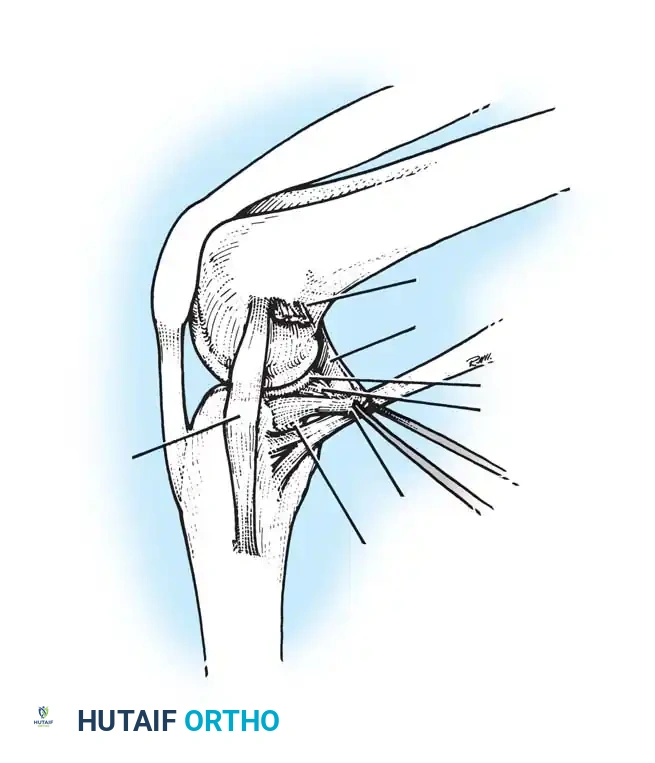
3. Posteromedial Approach
Essential for addressing posterior pathology that cannot be reached anteriorly.
* Indications: Repair of medial meniscus root tears, PCL tibial avulsion fractures, posteromedial corner reconstructions.
* Technique: An incision is made along the posteromedial border of the tibia. The interval is developed between the medial head of the gastrocnemius (retracted posteriorly) and the semimembranosus (retracted anteriorly).
* Anatomical Considerations: The saphenous nerve and great saphenous vein must be protected superficially. Deep dissection exposes the direct head of the semimembranosus and the posterior capsule.
4. Posterolateral Approach
Required for complex posterolateral corner (PLC) injuries.
* Indications: PLC reconstruction, LCL repair, popliteus avulsions.
* Technique: A curvilinear incision is made over the lateral aspect of the knee. The IT band is split, and the biceps femoris is identified.
* Anatomical Considerations: The common peroneal nerve MUST be identified and neurolysed early in the procedure. The surgical intervals allow access to the fibular head, the LCL, and the popliteofibular ligament.
PATIENT POSITIONING AND SETUP
Proper patient positioning is the foundation of a successful knee operation, ensuring optimal visualization and dynamic assessment of joint stability during the procedure.
- Supine Position: The patient is placed supine on a radiolucent operating table.
- Tourniquet Application: A well-padded pneumatic tourniquet is placed high on the proximal thigh. Exsanguination with an Esmarch bandage is performed prior to inflation (typically 250-300 mmHg) to ensure a bloodless field.
- Leg Holders and Positioning Devices: For arthroscopic procedures or ligament reconstructions, a lateral post or a specialized leg holder (e.g., Alvarado) is utilized to allow the knee to be stressed into valgus and held securely at varying degrees of flexion (usually 90 degrees).
- Fluoroscopy: The table must accommodate a C-arm for intraoperative imaging, particularly crucial during fracture fixation or tunnel placement in ligamentous reconstruction.
POSTOPERATIVE PROTOCOLS AND REHABILITATION
Rehabilitation is intrinsically linked to the anatomical structures repaired or reconstructed. Protocols must respect the biological healing phases of osseous, tendinous, and ligamentous tissues.
Soft Tissue and Ligamentous Reconstructions (e.g., ACL, PLC)
- Phase I (0-2 Weeks): Focus on protecting the graft, controlling edema, and restoring full passive extension. The knee is often braced in extension. Weight-bearing status depends on concomitant meniscal or chondral procedures.
- Phase II (2-6 Weeks): Gradual restoration of flexion. Initiation of closed-kinetic-chain quadriceps strengthening.
- Phase III (6-12 Weeks): Progression to full range of motion. Proprioceptive training and advanced strengthening.
- Phase IV (3-6 Months): Sport-specific agility drills, plyometrics, and eventual return to play following functional testing.
Osseous Procedures (e.g., Tibial Plateau ORIF)
- Phase I (0-6 Weeks): Strict non-weight-bearing or touch-down weight-bearing to protect the articular reduction. Early passive range of motion is encouraged to prevent arthrofibrosis and nourish the articular cartilage.
- Phase II (6-12 Weeks): Progressive weight-bearing based on radiographic evidence of callus formation and clinical stability.
- Phase III (3+ Months): Full weight-bearing, advanced strengthening, and normalization of gait mechanics.
Clinical Pearl: In procedures involving the extensor mechanism (e.g., patellar tendon repair or tibial tubercle osteotomy), active knee extension is strictly contraindicated for the first 4-6 weeks to prevent catastrophic failure of the repair.
CONCLUSION
The surgical anatomy of the knee is a masterclass in biomechanical engineering. The delicate interplay between the asymmetrical osseous condyles, the dynamic tendinous expansions of the semimembranosus and popliteus, and the static restraints of the capsuloligamentous complexes dictates the joint's function. For the operative orthopedic surgeon, a three-dimensional understanding of these structures is not merely academic; it is the essential prerequisite for executing precise surgical approaches, restoring native kinematics, and achieving optimal patient outcomes.
You Might Also Like