Introduction and Epidemiology
Proximal phalanx fractures represent a significant portion of hand fractures, accounting for approximately 10 to 15 percent of all upper extremity fractures. These injuries are prevalent across all age groups but demonstrate a bimodal distribution, frequently occurring in younger, active individuals involved in sports or high-energy work-related activities, and older populations susceptible to low-energy falls. The unique anatomy of the proximal phalanx, with its critical role in digital motion, grip strength, and pinch kinematics, dictates that even seemingly minor displacements can lead to substantial functional deficits if not managed with precision.
The primary goal of treatment, whether operative or non-operative, is to achieve stable anatomical reduction, preserve articular congruity, and facilitate early mobilization. Post-traumatic stiffness remains the most debilitating complication following phalangeal trauma. A thorough understanding of fracture morphology, associated soft tissue injuries, and patient-specific factors is paramount for optimizing outcomes. Fracture patterns vary widely based on the mechanism of injury, encompassing transverse, oblique, spiral, and comminuted configurations. High-energy axial loads frequently result in intra-articular base or head fractures, while torsional forces typically produce spiral shaft fractures. Given the tight fascial compartments and intimate relationship between the osseous structures and the flexor and extensor mechanisms, precise management is essential to prevent tendon adhesions and subsequent loss of digit excursion.
Surgical Anatomy and Biomechanics
The proximal phalanx is the longest of the three phalanges in each digit, forming the metacarpophalangeal joint proximally and the proximal interphalangeal joint distally. Its structural integrity is critical to the biomechanical cascade of digital flexion and extension.
Osseous Architecture
The proximal phalanx consists of a base, shaft, and head. The base articulates with the metacarpal head, forming a diarthrodial condyloid joint allowing flexion, extension, abduction, adduction, and limited circumduction. The robust palmar plate and collateral ligaments attach at the base, contributing to the primary static stability of the metacarpophalangeal joint. The shaft is cylindrical proximally but flattens distally on its volar aspect to accommodate the flexor tendons. Fractures through the diaphysis are highly susceptible to angular and rotational deformities due to the lack of stabilizing soft tissue attachments directly on the mid-shaft and the powerful forces exerted by traversing tendons. The head forms two asymmetric condyles that articulate with the base of the middle phalanx, creating a pure hinge joint at the proximal interphalangeal joint.
Soft Tissue and Tendinous Attachments
The extensor mechanism is a highly complex structure traversing the dorsal aspect of the proximal phalanx. The central slip of the extensor digitorum communis inserts into the dorsal base of the middle phalanx. The lateral bands, formed by the tendinous contributions of the lumbricals and interossei, merge dorsally to form the terminal tendon. Fractures of the proximal phalanx can disrupt this intricate mechanism through direct trauma or subsequent scarring, leading to extensor lag or boutonnière deformities.
On the volar aspect, the flexor digitorum superficialis and flexor digitorum profundus tendons run within a rigid fibro-osseous sheath. The A2 pulley, the most critical biomechanical pulley for preventing flexor tendon bowstringing, originates from the proximal and middle thirds of the proximal phalanx shaft. Swelling, fracture hematoma, and surgical dissection around this site can cause restrictive adhesions, severely limiting tendon glide.
Deforming Forces and Fracture Patterns
The intrinsic muscles, including the interossei and lumbricals, insert into the base of the proximal phalanx and the lateral bands of the extensor hood. Depending on the fracture location, these muscles exert predictable deforming forces.
Proximal shaft fractures typically exhibit a volar apex angulation. This occurs because the intrinsic muscles flex the proximal fragment via their insertion on the base, while the central slip of the extensor mechanism exerts an extension force on the distal fragment. Distal shaft fractures, conversely, can exhibit dorsal apex angulation due to the primary pull of the flexor tendons over the fulcrum of the intact A2 pulley.
Rotational deformity is the most critical biomechanical consideration. The natural cascade of the digits requires them to converge toward the scaphoid tubercle during active flexion. A rotational malalignment of even 5 degrees at the proximal phalanx can result in 1.5 centimeters of digital overlap at the fingertips, severely compromising grip mechanics.

Indications and Contraindications
The decision-making process for proximal phalanx fractures involves a careful assessment of fracture stability, displacement, patient demands, and the inherent risks of surgical intervention versus conservative management. The fundamental prerequisite for non-operative management is a stable fracture pattern that maintains acceptable reduction throughout a functional range of motion. Acceptable radiographic parameters generally include less than 10 degrees of angulation in the anteroposterior or lateral planes, less than 2 millimeters of shortening, and absolutely no rotational deformity.
Operative Versus Non Operative Decision Matrix
| Clinical Scenario | Indication Category | Rationale and Considerations |
|---|---|---|
| Non-displaced transverse or oblique fractures | Non-Operative | Inherently stable; amenable to buddy taping or intrinsic-plus splinting with early motion. |
| Stable impacted base fractures | Non-Operative | High union rates; primary risk is stiffness, necessitating early active mobilization. |
| Rotational malalignment (any degree) | Operative | Clinically results in finger scissoring; unacceptable for hand function. |
| Angulation > 10 degrees or Shortening > 2mm | Operative | Alters tendon excursion mechanics; leads to extensor lag or pseudo-clawing. |
| Intra-articular fractures with > 1mm step-off | Operative | High risk of early post-traumatic osteoarthritis and joint incongruity. |
| Multiple digit fractures | Operative | Difficult to control conservatively; fixation allows for early rehabilitation of the entire hand. |
| Open fractures | Operative | Requires formal irrigation, debridement, and rigid stabilization to mitigate infection risk. |
| Fractures with associated tendon/vascular injury | Operative | Requires stable skeletal framework to protect soft tissue repairs. |
Contraindications to Surgical Intervention
Absolute contraindications to surgical fixation are rare but include active, uncontrolled local soft tissue infection (unless the surgery is for debridement and external fixation) or a patient who is medically unstable for anesthesia. Relative contraindications encompass severe soft tissue compromise or crush injuries where extensive surgical dissection would devitalize the bone and skin, leading to necrosis or profound stiffness. Additionally, in severely low-demand or non-ambulatory patients with severe baseline dementia, the risks of operative intervention, hardware complications, and non-compliance with postoperative protocols may outweigh the functional benefits of anatomical reduction.
Pre Operative Planning and Patient Positioning
Thorough preoperative planning is essential for achieving optimal outcomes and minimizing intraoperative complications. The choice of implant, surgical approach, and rehabilitation strategy must be tailored to the specific fracture morphology.
Imaging and Diagnostics
Standard radiographic evaluation includes true posteroanterior, true lateral, and oblique views of the affected digit. It is imperative that the lateral view isolates the injured digit to prevent overlapping osseous shadows from adjacent fingers, which can obscure subtle angulation or articular step-offs.

For complex intra-articular fractures of the phalangeal base or head, a computed tomography scan with fine sagittal and coronal reconstructions is highly recommended. This aids in characterizing fragment size, comminution, and articular depression, directly influencing the choice between percutaneous pinning, mini-fragment screw fixation, or dynamic external fixation.
Operating Room Setup
Surgical management of proximal phalanx fractures is typically performed on a radiolucent hand table. The patient is positioned supine. Depending on the anticipated length of the procedure and patient comorbidities, anesthesia may consist of a regional axillary or supraclavicular block, or a wide-awake local anesthesia no tourniquet approach. The wide-awake approach is increasingly favored for phalangeal fractures as it allows intraoperative assessment of active tendon glide and confirmation of rotational alignment through active patient participation.
If a tourniquet is utilized, a forearm tourniquet is generally preferred over an upper arm tourniquet to improve patient tolerance, inflated to 250 mmHg after exsanguination with an Esmarch bandage. Alternatively, a sterile digital tourniquet can be used for isolated, brief procedures, though care must be taken to remove it promptly to avoid digital ischemia.
The surgical tray should include a comprehensive mini-fragment set featuring 1.2mm, 1.5mm, and 2.0mm screws, low-profile titanium plates, a variety of Kirschner wires ranging from 0.035 to 0.045 inches, and appropriate reduction forceps (e.g., pointed Weber clamps).
Detailed Surgical Approach and Technique
The execution of surgical fixation demands meticulous soft tissue handling. The primary objective is rigid fixation that permits immediate active motion while minimizing iatrogenic trauma to the extensor and flexor mechanisms.
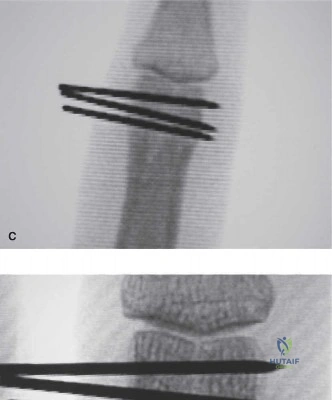
Closed Reduction and Percutaneous Pinning
Closed reduction and percutaneous pinning remains the workhorse for extra-articular transverse or short oblique fractures that are reducible but unstable. Reduction is achieved via longitudinal traction, correction of angular deformity, and strict attention to rotational alignment by assessing the digital cascade.
Kirschner wires (typically 0.035 or 0.045 inch) can be introduced in several configurations. Crossed pinning at the fracture site provides excellent torsional stability but risks tethering the lateral bands if placed too dorsally. Alternatively, intramedullary pinning via a retrograde approach through the collateral ligament recesses of the metacarpophalangeal joint or an antegrade approach through the proximal interphalangeal joint can be utilized. Pins are typically left proud and bent to facilitate removal in the clinic at 3 to 4 weeks, once clinical callus is evident.
Open Reduction Internal Fixation Approaches
When open reduction is mandated, the choice of surgical approach dictates the exposure and subsequent scarring profile.
Dorsal Approach
The dorsal longitudinal approach is the most common. A straight dorsal or slightly curved incision is made over the proximal phalanx. The extensor apparatus is exposed. Two primary internervous/intertendinous planes can be utilized:
1. Tendon-Splitting Approach: A longitudinal incision is made directly through the central slip of the extensor tendon. This provides excellent visualization of the diaphysis but carries a higher risk of postoperative extensor lag and adhesions. Meticulous repair of the tendon with 4-0 non-absorbable suture is required.
2. Tendon-Sparing (Champeau) Approach: The interval between the central slip and the lateral band is developed. The lateral band is retracted volarly, and the central slip is retracted dorsally. This approach provides access to the lateral and dorsal aspects of the phalanx while minimizing direct trauma to the central extensor mechanism, significantly reducing postoperative stiffness.
Midaxial Approach
The midaxial approach is highly advantageous for lateral plating or screw fixation of spiral fractures. The incision is planned along the neutral line of the digit, connecting the apices of the flexion creases. Dissection proceeds between Cleland's ligaments (dorsal) and Grayson's ligaments (volar). This approach completely avoids the extensor and flexor mechanisms, placing the hardware in a functionally silent area. It requires precise identification and dorsal retraction of the neurovascular bundle.
Fixation Strategies
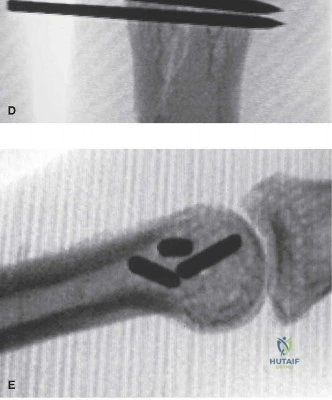
Lag Screw Fixation
For long oblique or spiral fractures where the fracture length is at least twice the diameter of the diaphysis, multiple lag screws offer superior biomechanical stability with minimal soft tissue footprint.

The fracture is anatomically reduced and held with pointed reduction forceps. A glide hole (e.g., 1.5mm) is drilled in the near cortex, followed by a pilot hole (e.g., 1.1mm) in the far cortex. The screw is inserted, compressing the fracture fragments. Typically, two to three screws are required to neutralize torsional forces. Screws must be placed perpendicular to the fracture plane to maximize interfragmentary compression and avoid shear displacement.
Plate Osteosynthesis
Comminuted fractures, short oblique fractures, or fractures with segmental bone loss require plate fixation. Low-profile titanium plates (1.5mm or 2.0mm systems) are utilized.
Dorsal plating provides a strong tension band construct but is notorious for causing extensor tendon irritation and adhesions. If dorsal plating is necessary, the periosteum should be meticulously closed over the plate if possible, or early tenolysis should be anticipated. Lateral plating, accessed via a midaxial approach, is biomechanically robust and significantly reduces tendon interference. Locking plates are specifically indicated in osteoporotic bone or severe comminution where conventional screw purchase is compromised.
Complications and Management
Despite meticulous surgical technique, proximal phalanx fractures carry a high complication rate, primarily related to the delicate soft tissue envelope. Proactive management and timely intervention are critical.
Common Complications and Salvage Strategies
| Complication | Estimated Incidence | Etiology and Risk Factors | Management and Salvage Strategies |
|---|---|---|---|
| Post-traumatic Stiffness | 30% - 50% | Tendon adhesions, joint capsular contracture, prolonged immobilization. | Intensive hand therapy. Surgical tenolysis and capsulotomy if no progress after 3-6 months. |
| Malunion (Rotational) | 5% - 10% | Failure to assess digital cascade intraoperatively, loss of reduction. | Corrective osteotomy (metacarpal or phalangeal base) depending on the degree of deformity. |
| Extensor Lag | 15% - 25% | Central slip injury, dorsal hardware prominence, tendon splitting approach. | Hardware removal, extensor tendon reconstruction, or terminal tendon tenotomy (Fowler procedure). |
| Nonunion | < 5% | Inadequate fixation, severe soft tissue stripping, infection, smoking. | Revision ORIF with autologous bone grafting (e.g., distal radius or iliac crest). |
| Hardware Failure | 2% - 5% | Premature loading, inadequate implant selection, patient non-compliance. | Revision fixation, transition to external fixation, or salvage arthrodesis if joint is destroyed. |
| Infection | 1% - 3% | Open fractures, percutaneous pin tract infections. | Oral or IV antibiotics. Pin removal if tract infection. Formal I&D for deep space infections. |
Management of Stiffness and Adhesions
Stiffness is the most ubiquitous complication. Adhesions between the fracture callus and the extensor mechanism limit flexion, while adhesions to the flexor apparatus limit active extension. If intensive hand therapy fails to yield functional gains by 3 to 6 months post-injury, surgical intervention is indicated.
Tenolysis requires extensive exposure to free the tendons from the osseous bed. It is imperative that the fracture is radiographically healed prior to tenolysis. Concomitant hardware removal is standard. If joint contracture is present, a dorsal capsulotomy of the proximal interphalangeal joint or a volar release of the metacarpophalangeal joint collateral ligaments may be necessary. Postoperative management following tenolysis requires immediate, aggressive active motion, often facilitated by indwelling regional analgesia catheters.
Post Operative Rehabilitation Protocols
The success of proximal phalanx fracture management is inextricably linked to the postoperative rehabilitation protocol. The paradigm has shifted from prolonged immobilization to immediate or early protected motion, facilitated by rigid internal fixation.
Phase One Early Protection
For operatively managed fractures with stable fixation, rehabilitation begins within 3 to 5 days postoperatively. The patient is fitted with a custom thermoplastic splint in the intrinsic-plus position: metacarpophalangeal joints flexed to 70 to 90 degrees, and proximal and distal interphalangeal joints in full extension. This position maintains the collateral ligaments of the metacarpophalangeal joint at their maximum length, preventing contracture, and prevents volar plate contracture at the proximal interphalangeal joint.
Active and active-assisted range of motion exercises for the interphalangeal joints are initiated immediately to promote tendon glide and limit edema. Edema control via compressive wrapping and elevation is strictly enforced.
Phase Two Progressive Motion
At 3 to 4 weeks postoperatively, clinical and radiographic evaluations are performed. If early callus is present and the fracture is clinically stable, the splint is transitioned to a buddy-tape system or a hand-based functional orthosis. Passive range of motion exercises are introduced to address early joint stiffness. Dynamic splinting (e.g., Capener splints for proximal interphalangeal joint extension deficits) may be implemented if specific contractures are identified.
Phase Three Strengthening
By 6 to 8 weeks, assuming radiographic consolidation is progressing, progressive strengthening exercises are initiated. This includes grip and pinch strengthening using putty and hand dynamometers. Full unrestricted activity and return to heavy manual labor or contact sports are typically permitted between 8 and 12 weeks, contingent upon complete radiographic union and functional recovery.
Summary of Key Literature and Guidelines
The evolution of proximal phalanx fracture management is well-documented in orthopedic literature, emphasizing the delicate balance between skeletal stability and soft tissue preservation.
Classic biomechanical studies by the AO Foundation established the principles of interfragmentary compression and rigid plate osteosynthesis, demonstrating that absolute stability reduces fracture gap strain, allowing for primary bone healing and immediate motion. However, subsequent clinical series highlighted the high rates of extensor tendon adhesions associated with dorsal plating.
This led to the popularization of the midaxial approach and lateral plating techniques, which have been shown in comparative studies to significantly improve total active motion outcomes compared to dorsal plating. Furthermore, the literature strongly supports the use of closed reduction and percutaneous pinning for stable or reducible extra-articular fractures, provided that strict rotational alignment is maintained and pins are placed outside the extensor mechanism excursion pathways.
Recent guidelines advocate for the use of wide-awake local anesthesia no tourniquet techniques in phalangeal fracture surgery. This paradigm shift allows surgeons to intraoperatively assess the integrity of the fixation under active physiological loads, directly observe tendon glide, and definitively confirm the absence of rotational malalignment prior to skin closure, thereby substantially reducing the incidence of postoperative malunion and stiffness.
