Scaphoid Nonunion: Advanced Grafting Techniques and Deformity Correction
Key Takeaway
Cancellous bone grafting remains the gold standard for treating scaphoid nonunions without significant deformity. For malpositioned nonunions presenting with a humpback deformity and dorsal intercalated segment instability (DISI), anterior wedge grafting with rigid internal fixation is required to restore carpal kinematics. This guide details the Matti-Russe inlay technique, structural wedge grafting, advanced CT imaging protocols, and evidence-based fixation strategies to optimize union rates and clinical outcomes in complex scaphoid fractures.
INTRODUCTION TO SCAPHOID NONUNION GRAFTING
The management of scaphoid nonunion remains a formidable challenge in operative orthopaedics, demanding a profound understanding of carpal kinematics, precise preoperative imaging, and meticulous surgical execution. Due to the scaphoid’s tenuous retrograde blood supply—predominantly derived from the dorsal carpal branch of the radial artery entering the distal half of the bone—fractures, particularly those in the proximal pole, are highly susceptible to delayed union, nonunion, and osteonecrosis.
Cancellous bone grafting for scaphoid nonunion, initially described by Matti and subsequently modified by Russe to utilize a volar approach, has proven to be a highly reliable procedure. When applied to appropriately selected patients, this technique yields bony union rates ranging from 80% to 97%. The classic Matti-Russe inlay grafting technique is most efficacious for ununited fractures that exhibit minimal to no associated shortening, angulation, or carpal collapse. However, in the presence of a malpositioned nonunion—classically presenting as a "humpback" deformity—structural interposition grafting combined with rigid internal fixation is mandatory to restore carpal alignment and prevent the progression of scaphoid nonunion advanced collapse (SNAC).
PREOPERATIVE EVALUATION AND ADVANCED IMAGING
Accurate preoperative assessment is the cornerstone of successful scaphoid reconstruction. Standard posteroanterior (PA), lateral, scaphoid view (PA with ulnar deviation), and semi-pronated oblique radiographs are mandatory. However, plain radiography often underestimates the degree of comminution, bone loss, and angular deformity.
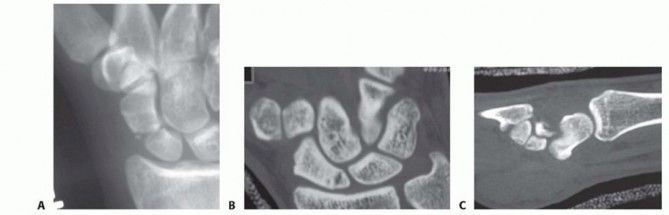
Computed Tomography (CT) is the gold standard for evaluating scaphoid nonunions, assessing the extent of osteolysis, and quantifying the humpback deformity. Because the scaphoid lies obliquely within the carpus (flexed approximately 45 degrees to the longitudinal axis of the radius), standard orthogonal CT planes of the wrist do not provide true anatomical cross-sections of the scaphoid.
Scaphoid-Specific CT Imaging Protocols
To accurately assess the intrascaphoid angle and plan for structural grafting, CT images must be reformatted along the true longitudinal and short axes of the scaphoid.
Sagittal Plane Imaging:
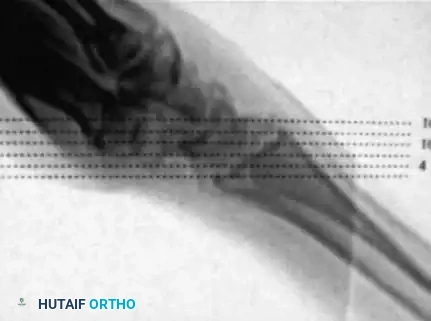
For true sagittal plane images of the scaphoid, the patient's forearm is held pronated, and the hand lies flat on the CT table. The forearm crosses the gantry at an angle of approximately 45 degrees, roughly in line with the abducted thumb metacarpal.

Scout images are obtained to confirm appropriate orientation and to ensure that the entire scaphoid is captured within the imaging field. Sections are obtained at 1-mm intervals to maximize resolution.
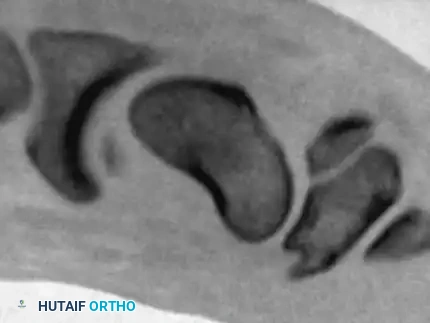
Images obtained in this specialized sagittal plane are optimal for measuring the intrascaphoid angle and quantifying the degree of volar flexion (humpback deformity) of the distal pole relative to the proximal pole.

Coronal Plane Imaging:
For true coronal plane images, the forearm is positioned in neutral rotation.
Scout images demonstrate the alignment of the wrist through the gantry of the scanner, ensuring the imaging plane is parallel to the long axis of the scaphoid.

Interpretation of images obtained in this true coronal plane is straightforward, allowing for precise evaluation of the fracture gap, cyst formation, and the integrity of the proximal pole articular surface.

💡 Clinical Pearl: Assessing Osteonecrosis
While CT is excellent for defining bony architecture, Magnetic Resonance Imaging (MRI) without and with gadolinium contrast remains the most sensitive modality for evaluating the vascularity of the proximal pole. A completely avascular proximal pole significantly alters the surgical algorithm, often necessitating a vascularized bone graft rather than standard non-vascularized techniques.
THE MATTI-RUSSE TECHNIQUE (INLAY GRAFTING)
The Matti-Russe procedure is an inlay cancellous bone grafting technique performed via a volar approach. By utilizing a volar incision, the surgeon preserves the critical dorsal blood supply to the scaphoid. This technique is indicated for established nonunions without significant angular deformity or carpal collapse.
Patient Positioning and Preparation
- Place the patient supine on the operating table with the affected arm extended on a radiolucent hand table.
- Administer general anesthesia or a regional brachial plexus block.
- Prepare and drape the injured upper extremity in a standard sterile fashion.
- Concurrently, prepare and drape the ipsilateral iliac crest to facilitate the harvest of high-quality autologous cancellous bone graft.
- Apply a pneumatic tourniquet to the proximal arm, elevating the limb and exsanguinating it with an Esmarch bandage before inflation (typically to 250 mm Hg).
Surgical Approach
- Make a longitudinal or slightly curvilinear incision, 3 to 4 cm in length, on the volar aspect of the wrist. The incision should be positioned slightly to the radial side of the flexor carpi radialis (FCR) tendon, extending distally to the level of the scaphoid tubercle.
- Carefully dissect through the subcutaneous tissues.
- Nerve Protection: Meticulously identify and protect the palmar cutaneous branch of the median nerve (located ulnar to the FCR) and the terminal branches of the superficial radial nerve (located radially).
- Incise the FCR tendon sheath and retract the FCR tendon ulnarward to expose the deep volar radiocarpal ligaments.
- Incise the wrist capsule longitudinally. Reflect the robust volar radiocarpal ligaments (specifically the radioscaphocapitate and long radiolunate ligaments) as medial and lateral flaps. These must be carefully preserved for robust repair during closure to prevent postoperative carpal instability.
Preparation of the Nonunion Site
- Identify the scaphoid bone and expose the nonunion site. Visualization is significantly enhanced by applying dorsiflexion and ulnar deviation to the wrist, which brings the scaphoid out from under the radial styloid.
- Assess the nonunion. Freshen the sclerotic bone ends using a small gouge or curette.
- Form a central cavity that extends well into both the proximal and distal fragments, removing all fibrous tissue and necrotic bone until punctate bleeding (the "paprika sign") is observed, indicating healthy, vascularized bone.
- Excavation Technique: The cavity can be formed using a high-speed burr; however, continuous saline irrigation is mandatory to prevent thermal necrosis of the surrounding osteocytes. Alternatively, outline a rectangular trough using a fine drill (e.g., 1.5 mm) and connect the holes with a thin osteotome or a powered thin saw blade (as described by Linscheid and Weber).
⚠️ Surgical Warning: Thermal Injury
The use of high-speed burrs without adequate irrigation can cause thermal necrosis of the scaphoid, effectively devascularizing the remaining bone and guaranteeing graft failure. Hand instruments (curettes and fine gouges) are preferred when approaching the subchondral bone of the proximal pole.
Graft Harvest and Insertion
- Direct attention to the prepared iliac crest. Make a small incision over the anterior iliac crest, at least 2 cm posterior to the anterior superior iliac spine (ASIS) to avoid the lateral femoral cutaneous nerve.
- Harvest a block of corticocancellous bone.
- On the back table, shape the cancellous portion of the graft into a large, lozenge-shaped peg designed to fit snugly into the preformed scaphoid cavity. If a rectangular trough was created, shape the graft to match these dimensions precisely.
- Insert the shaped peg into the scaphoid defect, bridging the proximal and distal fragments. The cortical strut of the graft can be used to provide structural support if a volar cortical defect exists, though the classic Matti-Russe utilizes purely cancellous bone.
- Pack multiple small cancellous bone chips tightly around the primary peg to eliminate any dead space and maximize osteoconductive potential.
- Utilize intraoperative C-arm fluoroscopy to verify complete filling of the cavity and restoration of scaphoid contour.
Fixation and Closure
- While the corticocancellous peg provides some intrinsic stability, biomechanical stability is vastly improved with internal fixation. Insert a 0.045-inch or 0.062-inch Kirschner wire (K-wire) from distal to proximal, crossing the fracture site and the graft.
- The K-wire can be cut flush and left just beneath the skin, or left protruding through the palmar skin for easy removal in the clinic.
- Deflate the pneumatic tourniquet and achieve meticulous hemostasis.
- Repair the volar wrist capsule and the radiocarpal ligaments using non-absorbable or slowly absorbable sutures. This step is critical to prevent volar carpal subluxation.
- Close the skin with interrupted sutures.
Postoperative Care (Matti-Russe)
Apply a bulky, sterile dressing followed by a rigid sugar-tong splint with a thumb spica extension. The splint should extend from above the elbow to the palmar crease, immobilizing the wrist in a neutral position and the thumb in slight abduction.
Sutures are removed at 8 to 10 days postoperatively, at which point a long-arm thumb spica cast is applied. If a K-wire was utilized, it is typically removed at 4 to 6 weeks. The patient is monitored clinically and radiographically every 1 to 2 weeks. The cast is converted to a short-arm thumb spica cast at 6 weeks and maintained until radiographic union is confirmed, which typically requires 12 to 16 weeks of total immobilization.
CORRECTION OF MALPOSITIONED NONUNION ("HUMPBACK" DEFORMITY)
Established nonunions of scaphoid fractures frequently undergo volar resorption and comminution. Because the scaphoid spans the proximal and distal carpal rows, loss of volar cortical support leads to a predictable pattern of collapse: the distal pole flexes, and the proximal pole extends alongside the lunate. This results in shortening, radial deviation, and a dorsal convexity known as the "humpback" deformity.
This pathoanatomy drives a dorsal intercalated segment instability (DISI) pattern, visible on lateral plain radiographs as an increased scapholunate angle and an extended lunate posture. Failure to correct this deformity during grafting leads to altered carpal kinematics, restricted range of motion, and inevitable radiocarpal arthrosis.
Principles of Deformity Correction
Fisk originally emphasized that simple inlay grafting is insufficient for these lesions; interposition (structural) bone grafting is required to restore scaphoid length and correct carpal malalignment.
Amadio et al. and Cooney et al. refined this concept, proposing anterior (volar) wedge grafting specifically for nonunions presenting with:
* A scapholunate angle greater than 60 degrees.
* An intrascaphoid angle greater than 45 degrees.
Fernandez further advanced the surgical approach by emphasizing the necessity of careful preoperative planning. This includes obtaining comparison radiographs of the uninjured contralateral wrist to template the exact dimensions of the required wedge graft, ensuring the graft is perfectly fitted to the defect, and utilizing rigid fixation.
Surgical Technique: Volar Wedge Grafting
- Approach: The volar approach is utilized as described in the Matti-Russe technique.
- Deformity Correction: Once the nonunion is exposed and debrided of fibrous tissue, the humpback deformity must be actively corrected. This is achieved by inserting a small lamina spreader into the nonunion site or by placing two joystick K-wires (one in the distal pole, one in the proximal pole) and levering the distal pole into extension.
- Lunate Stabilization: Tomaino et al. highlighted that persistent lunate extension can complicate scaphoid reduction. They recommended temporary radiolunate pinning (inserting a K-wire from the radius into the lunate) to stabilize the lunate in a neutral position before attempting to correct the scaphoid humpback deformity.
- Graft Preparation: Measure the resulting volar defect. Harvest a corticocancellous block from the iliac crest. Shape the graft into a wedge, with the cortical base corresponding to the volar cortex of the scaphoid.
- Insertion: Impact the wedge graft into the defect. The cortical face of the graft restores the volar length of the scaphoid, effectively correcting the intrascaphoid angle and reducing the DISI deformity.
Evidence-Based Fixation Strategies
The choice of internal fixation is critical for maintaining the corrected alignment while the structural graft incorporates.
- Headless Compression Screws: The advent of headless cannulated screws (e.g., the Herbert-Whipple screw) revolutionized scaphoid fixation. These screws provide rigid interfragmentary compression without violating the articular surface. According to Manske, McCarthy, and Strecker, the double-threaded Herbert screw is particularly effective in nonunions with evidence of osteonecrosis, proximal third nonunions, or revision cases following previously failed bone grafts.
- Kirschner Wires: Despite the popularity of screws, Stark et al. strongly recommended K-wire fixation combined with iliac bone grafting for all nonunions. They argued that judging intraoperative stability with bone grafting alone is difficult, and K-wire insertion is technically straightforward, adding minimal operative time. In their series of 151 old ununited scaphoid fractures, they achieved a remarkable 97% union rate.
- Combined Techniques: Combining structural volar wedge grafting with rigid screw fixation yields superior results. Daly et al. reported a 95% union rate using volar wedge grafting combined with Herbert screw fixation in 26 scaphoid nonunions. Similarly, Barton reviewed five different methods and found his best results (a 74% union rate in a highly complex cohort) were achieved using the "wedge" graft and the Herbert screw.
📊 Academic Evidence: Meta-Analysis Outcomes
A landmark meta-analysis of 1,121 articles by Merrell, Wolfe, and Slade (including 36 eligible high-quality reports) provided definitive evidence on fixation superiority:
* Grafting with Screw Fixation: Produced superior healing rates, achieving 94% union.
* Grafting with K-wire Fixation: Resulted in a significantly lower union rate of 74%.
* Proximal Pole Osteonecrosis: In cases complicated by avascular necrosis (AVN) of the proximal pole, vascularized bone grafts provided a vastly superior union rate (88%) compared to standard non-vascularized wedge grafting with screw fixation (47%).
POSTOPERATIVE REHABILITATION FOR WEDGE GRAFTING
When rigid internal fixation (headless compression screw) is achieved alongside structural wedge grafting, the postoperative protocol can be slightly accelerated compared to the un-fixed Matti-Russe technique.
- Initial Phase (0-2 weeks): The wrist is immobilized in a bulky dressing and a volar thumb spica splint. Elevation and digital range of motion are encouraged immediately to prevent stiffness.
- Intermediate Phase (2-6 weeks): Sutures are removed at 10-14 days. The patient is transitioned to a short-arm thumb spica cast or a rigid custom thermoplastic splint, depending on surgeon preference and the rigidity of the intraoperative fixation.
- Advanced Phase (6-12 weeks): Clinical and radiographic evaluation (often utilizing CT to confirm bridging trabeculae) is performed at 6 to 8 weeks. If progressive consolidation is evident, weaning from the splint begins, and active-assisted range of motion exercises for the wrist and thumb are initiated under the guidance of a certified hand therapist.
- Return to Activity: Heavy lifting and contact sports are strictly prohibited until definitive radiographic union is confirmed, which may take up to 16 weeks or longer in complex deformity corrections.
CONCLUSION
The surgical management of scaphoid nonunion requires a tailored approach based on the presence of deformity and the vascular status of the proximal pole. The Matti-Russe inlay technique remains a highly effective, time-tested procedure for non-deformed nonunions. However, the modern orthopaedic surgeon must be adept at recognizing the humpback deformity through advanced CT imaging and executing precise structural volar wedge grafting. By combining meticulous deformity correction with rigid headless compression screw fixation—and reserving vascularized grafts for cases of established osteonecrosis—surgeons can maximize union rates, restore carpal kinematics, and prevent the devastating long-term sequelae of scaphoid nonunion advanced collapse.
You Might Also Like