HY 2026
00:00
Start Quiz
Question 901
High Yield
Decreased activity of which of the following proteins may be predictive of an aggressive soft-tissue sarcoma?
Explanation
It has been proposed that an imbalance in the proteolytic cascade involving matrix metalloproteinases (MMPs) and their inhibitors (TIMPs) may play a role in the development or progression of malignancy. TIMP activity has been shown to be weak or nonexistent and MMP activity to be high in patients with soft-tissue sarcoma. The level of vascular endothelial growth factor is shown to be a negative prognostic indicator because the expression of this factor is associated with angiogenesis and aggressive growth of many tumors including Ewing' s sarcoma and chondrosarcoma. Stromelysin is a type of MMP. The biology of cytokines in malignancy is complex. A low level of interleukin-1 is not known to be associated with high-grade tumors.
Question 902
High Yield
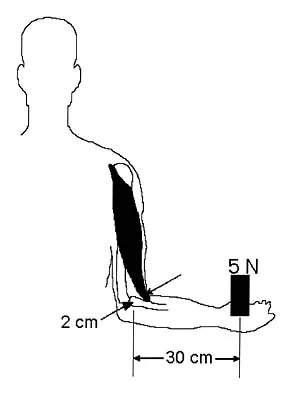
Figure 6 shows an object being held in an outstretched hand. To offset the moment created by the object (ignoring the weight of the forearm), the biceps must generate a force of
Explanation
Answering this question requires understanding of two important biomechanics concepts. First, because neither the object being held in the hand nor the body is moving and, hence, their accelerations are zero, the problem is one of static equilibrium in which the sum of the moments acting on the body is zero. Second, a moment is the action of a force that causes an object to rotate about any point away from its line of action. The magnitude of the moment is the magnitude of the force multiplied by the perpendicular distance between the line of action and the point (often called the moment arm or lever arm). In this problem, two forces are causing moments about the elbow. The magnitude of the moment caused by the object in the hand is 5 N times 30 cm or 150 N-cm. To maintain equilibrium, the moment caused by the biceps force must also have a magnitude of 150 N-cm. Its moment arm is 2 cm, so the magnitude of the biceps force is 150 N-cm divided by 2 cm, which equals 75 N. In general, functional loads such as the object are always at a mechanical advantage (ie, have a longer moment arm) over the muscle. Therefore, muscles must generate large forces to overcome the moments caused by even small functional loads. An KN, Chao ES, Kaufman KR: Analysis of muscle and joint loads, in Mow VC, Hayes WC (eds): Basic Orthopaedic Biomechanics, ed 2. New York, NY, Lippincott-Raven, 1997, pp 1-14.
Question 903
High Yield
Examination of a 5-year-old boy with amyoplasia shows a flexion contracture of 70 degrees of the right knee. The active arc of motion is from 70 degrees to 90 degrees, and the opposite knee has a flexion contracture of 10 degrees. Both hips are dislocated with flexion contractures of 10 degrees, passive hip motion is from 10 degrees to 90 degrees of flexion, and the feet are plantigrade and easily braceable. Despite a daily stretching program, the parents and physical therapists note that it is increasingly difficult for him to walk because of the flexion contracture of the right knee. Management of the knee flexion contracture should now include
Explanation
Most children with amyoplasia are ambulatory and when a decrease in function occurs because of a severe contracture, it must be addressed. A radical posterior soft-tissue release, including the posterior knee capsule and often the collateral ligaments and the posterior cruciate ligament, is needed to obtain extension. After the age of 1 year, aggressive physical therapy will do little to correct a contracture. Botulinum toxin A is indicated for spasticity and is contraindicated with severe contractures. Supracondylar femoral extension osteotomy works well, but will remodel at an average rate of 1 degree per month, which is not considered ideal in a young patient. Gradual correction with a circular ring external fixator is an option, but a soft-tissue release will also most likely be needed for a contracture of this severity. Sarwark JF, MacEwen GD, Scott CI Jr: Amyoplasia (a common form of arthrogryposis). J Bone Joint Surg Am 1990;72:465-469. DelBello DA, Watts HG: Distal femoral extension osteotomy for knee flexion contracture in patients with arthrogryposis. J Pediatr Orthop 1996;16:122-126.
Question 904
High Yield
What is the most common long-term complication of the fracture shown in Figure 32?

Explanation
The fracture pattern shown in the radiograph involves both a talar neck fracture and a talar body fracture. The body fracture propagates into the subtalar joint, with significant risk for the development of arthritis in that surface even with an anatomic reduction. In addition, Canale and Kelly reported a 25% incidence of malunion of talar neck fractures, with varus angulation occurring most frequently. Of these patients, 50% required a secondary surgical procedure because of the development of degenerative joint disease of the subtalar joint. Canale ST, Kelly FB Jr: Fractures of the neck of the talus: Long-term evaluation of seventy-one cases. J Bone Joint Surg Am 1978;60:143-156.
Question 905
High Yield
Spontaneous recovery of upper extremtiy motor function after a cerebrovascular accident occurs in which of the following predictable patterns?
Explanation
Recovery of upper extremity motor function after a cerebrovascular accident follows a predictable pattern. The greatest amount of recovery is seen within the first 6 weeks. Return of function proceeds from proximal to distal. Shoulder flexion occurs first, followed by return of flexion to the elbow, wrist, and fingers. Return of forearm supination follows the return of finger flexion.
Question 906
High Yield
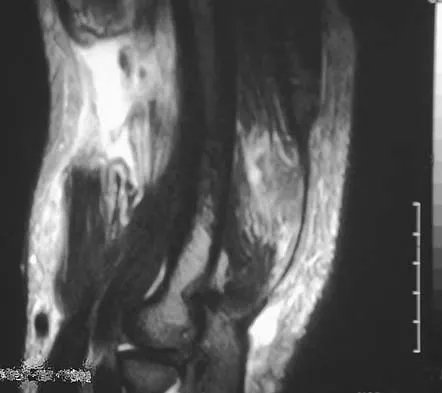
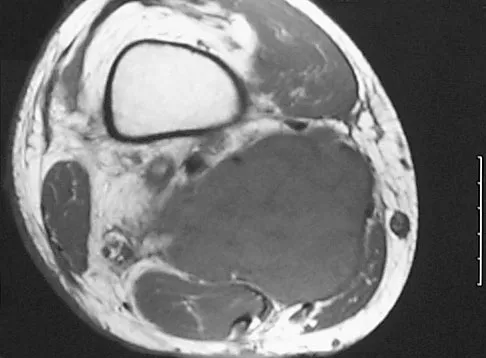
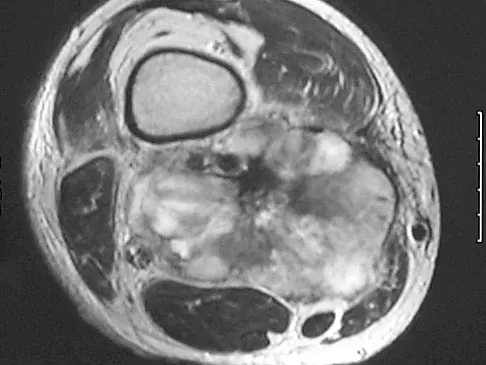
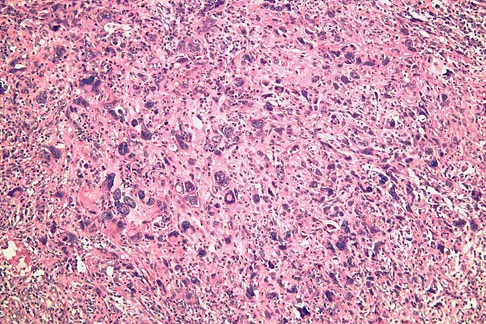
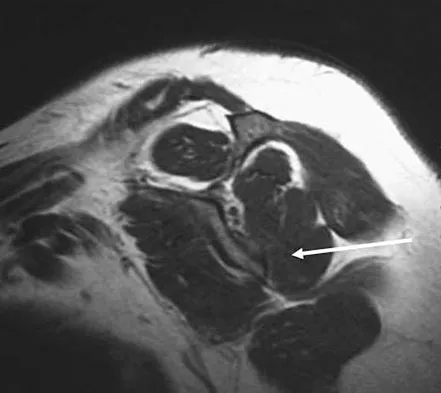
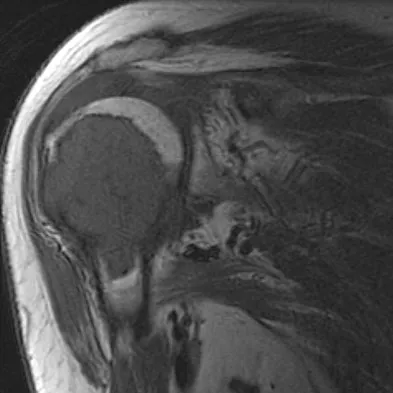
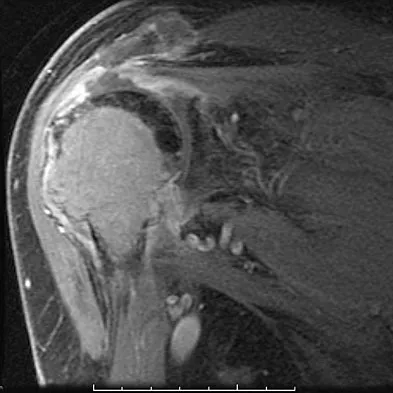
A 37-year-old man pulled his hamstring playing softball 3 weeks ago. The patient had not noted any mass prior to his injury. MRI scans of the posterior thigh are shown in Figures 4a and 4b. Figure 4c shows the biopsy specimen from a needle biopsy. What is the most likely diagnosis?
Explanation
Malignant fibrous histiocytoma (MFH) is the most common soft-tissue sarcoma. MFH typically presents as a large mass, deep to the fascia with heterogeneous signal on MRI. The MRI scans show a heterogeneous lesion in the posterior thigh. There is significant high signal uptake on the T2-weighted image. The histology shows malignant histiocytic cells with marked atypia and pleomorphism. Histology of a hematoma would show only old hemorrhage and some granulation tissue. Lipoma and liposarcoma are both seen as a fat-containing lesion on histology. No significant fat tissue is seen in this histologic specimen. Histology of myositis ossificans would show bone formation. Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 219-276.
Question 907
High Yield
Examination of a hand with compartment syndrome is most likely to reveal which of the following?

Explanation
In a study of 19 patients with compartment syndrome of the hand, all had tense swollen hands with elevated compartment pressures. Most patients were neurologically compromised so pain with passive stretch may be difficult to illicit. Arterial inflow is present in the arch and thus pallor is not present. The typical posture of the hand is not clenched, rather it is an intrinsic minus posture of metacarpophalangeal joint extension and flexion of the proximal and distal interphalangeal joints. Oullette EA, Kelly R: Compartment syndromes of the hand. J Bone Joint Surg Am 1996;78:1515-1522.
Question 908
High Yield
In recurrent posterior shoulder instability, what is the recommended approach to the posterior capsule?
Explanation
Using an infraspinatus-splitting incision allows for excellent exposure of the posterior capsule and minimizes the risk of injury to the axillary nerve which lies inferior to the teres minor in the quadrilateral space. Dreese J, D'Alessandro D: Posterior capsulorrhaphy through infraspinatus split for posterior instability. Tech Shoulder Elbow Surg 2005;6:199-207. Shaffer BS, Conway J, Jobe FW, et al: Infraspinatus muscle-splitting incision in posterior shoulder surgery: An anatomic and electromyographic study. Am J Sports Med 1994;22:113-120.
Question 909
High Yield
The humeral nonunion shown in Figure 27 is most likely to unite when using what method of treatment?

Explanation
The radiograph shows an atrophic nonunion of the humeral shaft. The management of humeral nonunions has been studied with compression plates and bone graft, as well as intramedullary nailing and bone graft. Compression plating with bone graft results in the highest rate of union. Compression plating by itself is not adequate, given the bone loss and lack of callous in this nonunion. Pulsed electromagnetic fields is a viable option for hypertrophic nonunions where there is inherent stability. Intramedullary nailing does not provide as much compression and stability as that achieved with compression plating. Pugh DM, McKee MD: Advances in the management of humeral nonunion. J Am Acad Orthop Surg 2003;11:48-59.
Question 910
High Yield
Figure 42 shows the radiograph of a 12-year-old boy who has a limp and pain in the left hip with athletic activity. Examination reveals decreased abduction and internal rotation of the left hip, with pain at the extremes of motion and a 1-cm limb-length discrepancy. Management should consist of

Explanation
The radiograph shows changes that are most consistent with Legg-Calve Perthes disease. Valgus extension osteotomy is the salvage procedure of choice in patients with late symptomatic Perthes disease with severe joint incongruity. Prerequisites for valgus extension osteotomy include an adequate range of hip adduction and proof of improved congruity in the new position. Total hip arthroplasty is not a good alternative in the young patient. Varus osteotomy would further shorten the extremity and place a flattened portion of the femoral head in the acetabulum. A prerequisite of the innominate osteotomy is a congruent reduction. Skaggs DL, Tolo VT: Legg-Calve-Perthes disease. J Am Acad Orthop Surg 1996;4:9-16.
Question 911
High Yield
Figure 13 shows the radiographs of a 20-year-old intercollegiate basketball player who was injured 6 weeks prior to the start of the season. What is the most appropriate treatment?
Explanation
A Jones fracture occurs at the metaphyseal-diaphyseal junction of the fifth metatarsal. It is often an acute fracture in conjunction with a chronic stress-related injury. It requires either a short leg cast with strict non-weight-bearing or surgical fixation. In the high performance athlete, the need for rapid return to sport activity usually requires surgical intervention, most commonly with an intramedullary screw. Brodsky JW, Krause JO: Stress fractures of the foot and ankle, in Delee JC, Drez D (eds): Orthopaedic Sports Medicine, ed 2. Philadelphia, PA, Saunders, 2003, vol 2, pp 2391-2409.
Question 912
High Yield
Osteolysis after total knee arthroplasty can be minimized through prosthetic design features such as
Explanation
The incidence of osteolysis is minimal in studies reporting the use of all polyethylene or monolithic metal-backed tibial components. Osteolysis has been reported in patients with total knee arthroplasties using cementless implants with modular components. Micromotion between the tibial tray and the polyethylene results in backside wear, leading to osteolysis. Osteolysis also has been reported in cemented posterior cruciate-substituting modular components. O'Rourke and associates reported a 16% incidence of osteolysis in patients with a posterior stabilized implant because of the use of modular polyethylene and the subsequent abrasive wear. Oxidation of the polyethylene that is the result of the method of sterilization and shelf life has also been implicated in the high incidence of osteolysis, along with patient factors such as activity level and weight.
Question 913
High Yield
Which of the following is considered an important factor in improved cemented femoral stem survivorship?
Explanation
Cement technique, relative stem to canal size and position, stem design, surgical technique, and femoral anatomy are important factors in cemented stem survivorship. Varus stem position, a wide diaphyseal to metaphyseal ratio (stovepipe femur), thin cement mantles (1 mm or less), and nonrounded femoral stem designs are negative prognostic factors for stem survivorship. Precoating with methylmethacrylate has not been shown to provide any increased survivorship over nonprecoated stems. Noble PC, Collier MB, Maltry JA, Kamaric E, Tullos HS: Pressurization and centalization enhance the quality and reproducibility of cement mantles. Clin Orthop 1998;355:77-89. Crowninshield RD, Brand RA, Johnston RC, Milroy JC: The effect of femoral stem cross-sectional geometry on cement stresses in total hip reconstruction. Clin Orthop 1980;146:71-77.
Question 914
High Yield
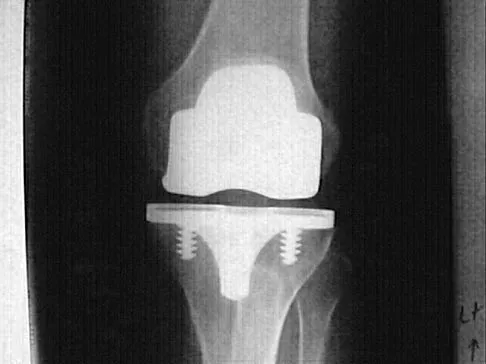
Figure 50 shows the AP radiograph of an asymptomatic 82-year-old woman who underwent total hip arthroplasty 16 years ago. What is the most likely diagnosis?

Explanation
Pelvic osteolysis in the presence of a well-fixed porous-coated socket is a recognized complication in total hip arthroplasty. The radiograph shows large lytic lesions superiorly adjacent to an acetabular screw and inferiorly extending into the ischium. It also reveals eccentricity of the femoral head with respect to the acetabular component, consistent with polyethylene wear. Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 440.
Question 915
High Yield
A 3-year-old patient with L3 myelomeningocele has bilateral dislocated hips. Management should consist of

Explanation
In patients with myelomeningocele, the presence of bilateral hip dislocation does not affect ambulation, bracing requirements, sitting ability, degree of scoliosis, or level of comfort. There is little evidence to support active treatment of bilateral hip dislocations in patients with myelomeningocele proximal to L4. Fraser RK, Hoffman EB, Sparks LT, et al: The unstable hip and mid-lumbar myelomeningocele. J Bone Joint Surg Br 1992;74:143-146.
Question 916
High Yield
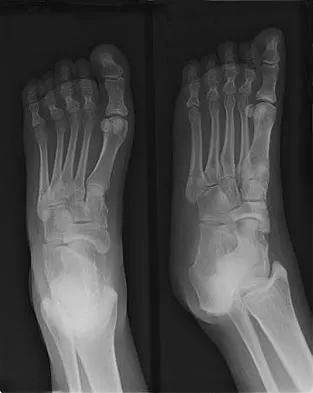
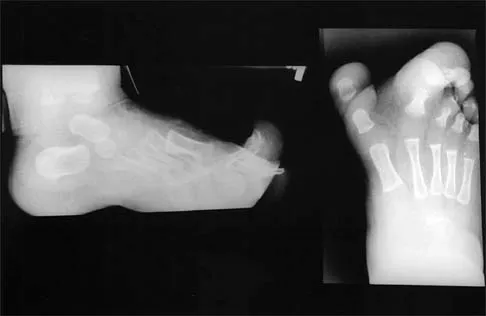
Figures 4a through 4c show the clinical photographs and radiographs of a 12-month-old boy who has progressive difficulty wearing shoes because of the length of the second toe, as well as width of the forefoot. Management should consist of


Explanation
The patient has macrodactyly involving the second ray, with significant enlargement of the width and height of the foot. The radiographs show widening of the interval between the first and second metatarsal and between the second and third metatarsal. With this degree of involvement, amputation of the second ray with excision of the overgrowth of affected soft tissue provides the most consistent desired reduction in foot size. A threaded Steinmann pin should be inserted across the remaining metatarsals until healing has occurred. Patients with macrodactyly should be examined to exclude neurofibromatosis type 1 and Klippel-Trenaunay-Weber syndrome.
Question 917
High Yield
Which of the following is not a reported mode of failure for a constrained acetabular component?
Explanation
There is no evidence of increased polyethylene wear in constrained acetabular components. The rates of wear appear to be the same using standard or constrained liners. Lachiewicz PF, Kelley SS: Constrained components in total hip arthroplasty. J Am Acad Orthop Surg 2002;10:233-238. Anderson MJ, Murray WR, Skinner HB: Constrained acetabular components. J Arthroplasty 1994;9:17-23.
Question 918
High Yield
What is one of the principle concerns when a fracture such as the one seen in Figure 18 is encountered?

Explanation
The injury shown is a fracture-dislocation and it is highly unstable. In addition to this concern, spinal epidural hematomas have a much higher incidence in people with ankylosing spondylitis following knee fracture. It is felt to be due to disrupted epidural veins, with hypervascular epidural soft tissue in the setting of a rigid spinal canal. Patients with ankylosing spondylitis may have other significant comorbidities, especially cardiac and pulmonary, and these should be carefully assessed. Ludwig S, Zarro CM: Complications encountered in the management of patients with ankylosing spondylitis, in Vaccaro AR, Regan JJ, Crawford AH, et al (eds): Complications of Pediatric and Adult Spine Surgery. New York, NY, Marcel Dekker, 2004, pp 279-290.
Question 919
High Yield
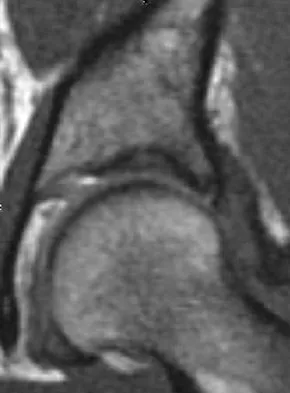
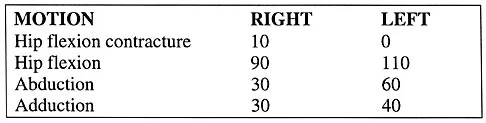
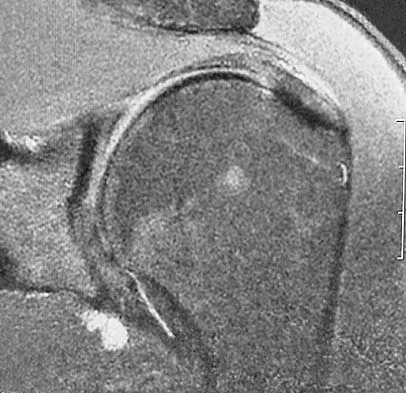
Figure 7 shows a sagittal T1-weighted MRI scan. What muscle/tendon is identified by the arrow?
Explanation
The sagittal T1-weighted MRI scan is useful for interpreting the quality of muscle. The arrow is pointing to the teres minor. Goutallier D, Postel JM, Gleyze P, et al: Influence of cuff muscle fatty degeneration on anatomic and functional outcomes after simple suture of full-thickness tears. J Shoulder Elbow Surg 2003;12:550-554.
Question 920
High Yield
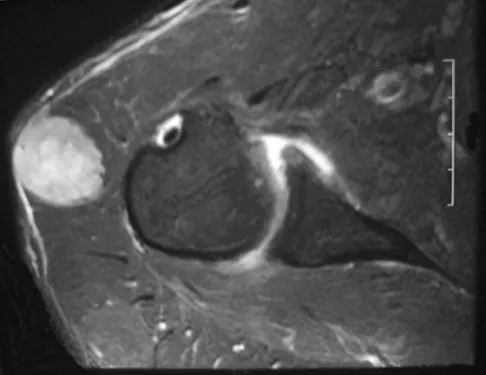
A 28-year-old woman who is an avid runner reports pain about the left hip with activities. Nonsurgical management has failed to provide relief. An MRI arthrogram is shown in Figure 47. What is the most likely diagnosis?
Explanation
The MRI arthrogram reveals dye extravasation into the labrum, consistent with a labral tear. The MRI findings are not typical of osteonecrosis, stress fracture, or transient osteoporosis. There is no increase in bone marrow edema in the neck or femoral head. Guanche CA, Sikka RS: Acetabular labral tears with underlying chondralmalacia: A possible association with high-level running. Arthroscopy 2005;21:580-585.
Question 921
High Yield
Following an episode of transient quadriplegia in contact sports, an athlete's return to play is absolutely contraindicated when
Explanation
Return to play decisions after traumatic spinal or spinal cord injury are not always clear-cut and often must be made on a patient-by-patient basis. The Torg ratio has been found to have low sensitivity in patients with large vertebral bodies. Abnormal electromyographic studies can persist in the face of normal function and do not define spinal injury. Duration of quadriplegia is not related to anatomic pathology. Findings on MRI scans or contrast-enhanced CT scans consistent with stenosis include lack of a significant cerebrospinal fluid signal around the cord, bony or ligament hypertrophy, or disk encroachment. Based on these findings, return to play should be avoided. Cantu RC, Bailes JE, Wilberger JE Jr: Guidelines for return to contact or collision sport after a cervical spine injury. Clin Sports Med 1998;17:137-146. Herzog RJ, Wiens JJ, Dillingham MF, Sontag MJ: Normal cervical spine morphometry and cervical stenosis in asymptomatic professional football players: Plain film radiography, multiplanar computer tomography, and magnetic resonance imaging. Spine 1991;16:178-186.
Question 922
High Yield
What is the most likely cause of recurrent symptoms following excision of a third web space neuroma?
Explanation
When a recurrent neuroma forms at the end of the resected nerve, it does not retract far enough because either the transection was not proximal enough or it is tethered by plantar neural branches. The transverse intermetatarsal ligament may reform, but it is not associated with pathology. Synovial cysts and synovitis are part of the differential diagnosis but are not associated with neuroma excision. Complex regional pain syndrome may result from neuroma excision, but this is rare and the symptoms are different. Beskin JL: Recurrent interdigital neuromas, in Nunley JA, Pfeffer GB, Sanders RW, Trepman E (eds): Advanced Reconstruction: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 481-484.
Question 923
High Yield
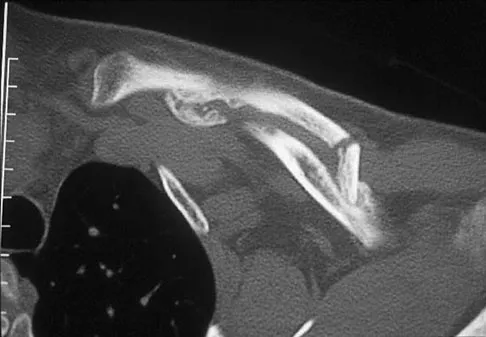
Figures 18a through 18c show the clinical photograph, radiograph, and CT scan of a 21-year-old man who reports persistent pain after injuring his right shoulder 4 months ago. What is the most likely factor associated with this patient's diagnosis?


Explanation
The more severe the trauma, the higher the rate of subsequent clavicular nonunion. Neither duration nor type of immobilization has been clearly demonstrated to be a causative factor in the development of nonunion. Similarly, closed reduction has not been found to alter the healing course in midshaft clavicular fractures. Lazarus MD, Seon C: Fractures of the clavicle, in Bucholz RW, Heckman JD, Court-Brown C (eds): Fractures in Adults. Philadelphia, PA, Lippincott Williams and Wilkins, 2006, vol 2, pp 1241-1242.
Question 924
High Yield
A 60-year-old woman with rheumatoid arthritis has atlanto-axial instability and basilar invagination. What MRI findings would suggest the need for cervical fusion?
Explanation
The cervical medullary junction should be 135 degrees or greater. An angle of 125 degrees suggests compression of the cervical medullary junction. Other findings supporting surgical intervention include a cord diameter in flexion of less than 6 mm or less than 13 mm of space available for the cord. Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 1998, pp 700-701. Monsey RB: Rheumatoid arthritis of the cervical spine. J Am Acad Orthop Surg 1997;5:240-248.
Question 925
High Yield
A 32-year-old man has an open comminuted humeral shaft fracture. Examination reveals absence of sensation in the first web space and he is unable to fully extend the thumb, fingers, and wrist. What is the recommended treatment following irrigation and debridement of the fracture?

Explanation
There is a high incidence of partial or complete laceration of the radial nerve with high-energy open fractures of the humeral shaft. The recommended treatment is irrigation and debridement of the fracture followed by open reduction and internal fixation and exploration of the radial nerve. If the nerve is completely lacerated, primary repair may be performed but poor outcomes have been reported. If a large zone of nerve injury is identified, delayed nerve grafting is advocated. Ring D, Chin K, Jupiter JB: Radial nerve palsy associated with high energy humeral shaft fractures. J Hand Surg 2004;29:144-147. Foster RJ, Swiontkowski MR, Bach AW, et al: Radial nerve palsy caused by open humeral shaft fractures. J Hand Surg Am 1993;18:121-124.
Question 926
High Yield
What is the most common cause for poor outcomes in patients who undergo total shoulder arthroplasty?

Explanation
In an article in the Journal of Shoulder and Elbow, 431 total shoulder arthroplasties were performed with a cemented all-polyethylene glenoid component between 1990 and 2000. Follow-up averaged 4.2 years. In total, 53 surgical complications occurred in 53 patients (12%). Of these, 32 were major complications (7.4%), with 17 of these requiring reoperation. Index complications in order of frequency included rotator cuff tearing, postoperative glenohumeral instability, and periprosthetic humeral fracture. Notably, glenoid and humeral component loosening requiring reoperation occurred in only one shoulder. Data from the contemporary patient group suggest that there are fewer complications of shoulder arthroplasty and less need for reoperation. Especially striking is the near absence of component revision because of loosening or other mechanical factors. Complications involving the brachial plexus have been reported following total shoulder arthroplasty but are not as common of a cause for failure. Chin PY, Sperling JW, Cofield RH, et al: Complications of total shoulder arthroplasty: Are they fewer or different? J Shoulder Elbow Surg 2006;15:19-22.
Question 927
High Yield
A 21-year-old collegiate scholarship football player has an episode of transient quadriplegia. An MRI scan of the cervical spine reveals cord edema and severe congenital spinal stenosis. The athlete has aspirations of playing on a professional level and demands that he be allowed to play. The team physician should give what recommendation to the college?
Explanation
Federal courts have ruled that a student-athlete does not have a constitutional right to participate in athletics against medical advice. As long as the student retains his scholarship, the college is under no legal or ethical obligation to allow the student to participate in sports. A waiver would not hold up in court and would not indemnify the college or the team physician against suit. No equipment has been shown to be effective in preventing transient quadriplegia. Mathias MB: The competing demands of sport and health: An essay on the history of ethics in sports medicine. Clin Sports Med 2004;23:195-214.
Question 928
High Yield
Figure 19 shows an arthroscopic view from the anterior lateral portal of the knee looking into the suprapatella pouch. The use of an electrothermal device during this procedure most commonly causes significant postoperative complications by damaging which of the following structures?
Explanation
While it is possible to damage any of these structures, unrecognized intraoperative laceration without adequate coagulation of the superior lateral geniculate artery is common. This can result in significant postoperative hemarthrosis and a return to surgery when bleeding cannot be controlled. Cash JD, Hughston JC: Treatment of acute patella dislocation. Am J Sports Med 1988;16:244-249.
Question 929
High Yield
A well-developed college football player reports swelling and a heaviness in the arm after lifting weights. Examination reveals that distal pulses are normal and equal in both arms. A venogram is shown in Figure 13. What is the most likely cause of this condition?
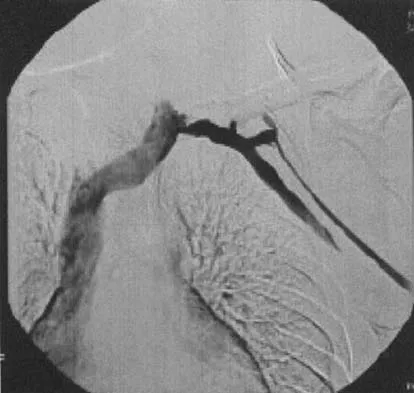
Explanation
The clinical findings indicate venous obstruction without arterial compression, and the venogram reveals occlusion of the subclavian vein, which is most likely the result of thoracic outlet compression. In the developed athlete, scalene muscle hypertrophy (Paget-Schroetter syndrome) causes compression of the subclavian vein. Treatment should consist of thrombolysis followed by decompressive surgery. Angle N, Gelabert HA, Farooq MM, et al: Safety and efficacy of early surgical decompression of the thoracic outlet for Paget-Schroetter syndrome. Ann Vasc Surg 2001;15:37-42.
Question 930
High Yield
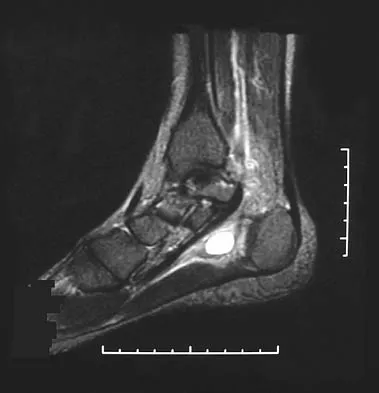
An active 48-year-old woman has had progressive retrocalcaneal pain for the past 2 years. She reports that an injection into the retrocalcaneal bursa 3 weeks ago provided relief, but she now has swelling and weakness after tripping on the stairs 3 days ago. The Thompson test is positive. A radiograph is shown in Figure 36. What is the next most appropriate step in management?

Explanation
The patient's long-standing symptoms and radiograph indicate a chronic insertional Achilles tendinopathy that has progressed to complete rupture. This situation is best treated with tendon debridement and repair, often requiring supplementation graft from the flexor hallucis longus. MRI could provide additional information on the quality of the Achilles tendon, but neither MRI nor ultrasound is necessary to make a diagnosis or determine the surgical indication. Conservative management will be unpredictable with a chronic degenerative tendon injury. Myerson MS, McGarvey W: Disorders of the Achilles tendon: Insertion and Achilles tendinitis. Instr Course Lect 1999;48:211-218. Wilcox DK, Bohay DR, Anderson JG: Treatment of chronic Achilles tendon disorders with flexor hallucis longus tendon transfer/augmentation. Foot Ankle Int 2000;21:1004-1010.
Question 931
High Yield
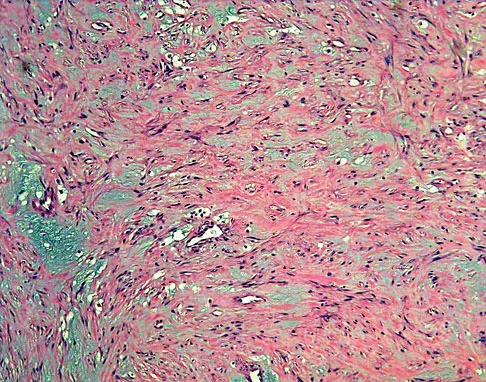
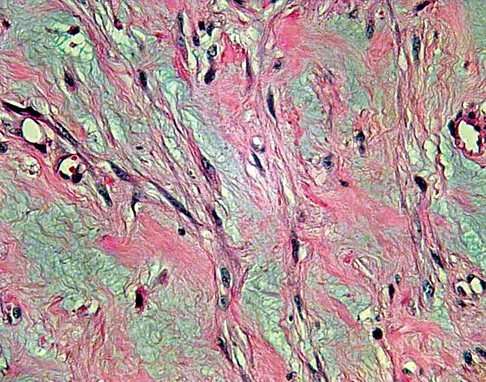
A 35-year-old man reports the development of a painful 2-cm nodule on his dorsal wrist over the past 3 years. A surgeon excised the lesion with a presumptive diagnosis of a ganglion cyst. Histology sections from the excision are shown in Figures 11a and 11b. What is the most likely diagnosis?
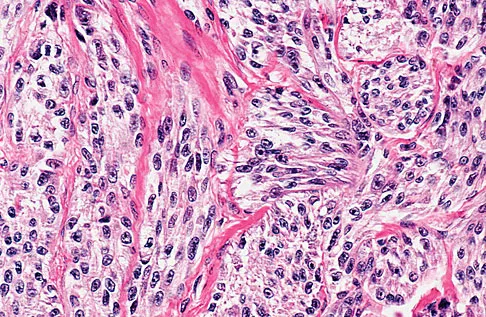
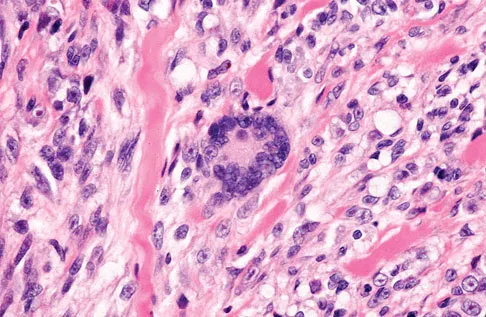
Explanation
The histologic appearance of the soft-tissue lesion reveals compact nests of cells with a clear cytoplasm surrounded by a delicate border of fibrocollagenous tissue. There can be scattered multinucleated giant cells. This is consistent with a clear cell sarcoma, also called malignant melanoma of soft parts. This tumor is usually positive for S-100 and HMB45 (a melanoma-associated antigen). These tumors are frequently found around the foot and ankle. Similar to epithelioid sarcoma, it is usually intimately bound to tendons or tendon sheaths. Often the tumors are present for many years. The classic histologic appearance of this lesion differentiates it from the other choices. Enzinger FM, Weiss SW: Soft Tissue Tumors, ed 3. St Louis, MO, Mosby, 1995, p 913.
Question 932
High Yield
Figures 14a and 14b show the plain radiographs of an 85-year-old woman who has had severe pain in the right knee for the past 4 months. Management should consist of


Explanation
The patient has osteonecrosis of the lateral femoral condyle with collapse of the articular surface. Because there is already collapse of the articular surface, a total knee arthroplasty is the treatment of choice. The results of total knee arthroplasty in these patients are usually excellent. However, knee replacement is only a resurfacing procedure, and some patients with global osteonecrosis of the distal femur may have residual pain after knee replacement. High tibial osteotomy may be indicated in younger patients who have a varus deformity and localized osteonecrosis. Arthroscopic surgery would provide minimal relief for this patient because there is already collapse of the articular surface. A hinged knee brace will not adequately unload the joint. An osteochondral allograft should be considered only for younger patients with localized osteonecrosis. Bergman NR, Rand JA: Total knee arthroplasty in osteonecrosis. Clin Orthop 1991;273:77-82.
Question 933
High Yield
In the anterior forearm approach to the distal radius (Henry approach), the radial artery is located between what two structures?
Explanation
The standard approach to the volar aspect of the distal radius is the Henry approach. Following incision of the skin and subcutaneous tissues, the forearm fascia is incised. The radial artery and venae comitantes lie in the interval between the tendons of the flexor carpi radialis muscle and the brachioradialis muscle. This interval is developed, and the radial artery and veins are retracted in a radial direction. Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics, ed 2. Philadelphia, PA, Lippincott-Raven, 1994, pp 118-131.
Question 934
High Yield
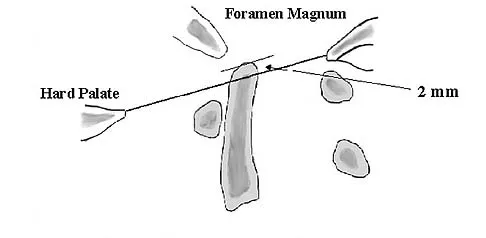
The thickest bone in the occiput is located

Explanation
Anatomic studies have shown that the thickest bone of the occiput is at the level of the external occipital protuberance. It ranges from 11.5 mm to 15.1 mm in men and from 9.7 mm to 12 mm in women. In general, the bone thins as it extends distally from the external occipital protuberance and it also moves laterally from the midline. The structures at risk during screw placement include the venous sinuses. Nadim Y, Lu J, Sabry FF, et al: Occipital screws in occipitocervical fusion and their relation to the venous sinuses: An anatomic and radiographic study. Orthopedics 2000;23:717-719.
Question 935
High Yield
In hybrid arthroplasty, the use of a polymethylmethacrylate (PMMA) precoated femoral component has been shown to result in
Explanation
Precoating of the femoral stem with PMMA results in increased bonding of the stem to the cement mantle. However, this has not been shown to result in superior survivorship compared with nonprecoated stems of similar design. In one series, the rate of revision of precoated stems was greater than that of nonprecoated cohorts. The wear and infection rates have not been shown to differ between precoated and nonprecoated stems. Sporer SM, Callaghan JJ, Olejniczak JP, Goetz DD, Johnston RC: The effects of surface roughness and polymethylmethacrylate precoating on the radiographic and clinical results of the Iowa hip prosthesis: A study of patients less than fifty years old. J Bone Joint Surg Am 1999;81:481-492.
Question 936
High Yield
A 64-year-old man who underwent total shoulder arthroplasty 4 weeks ago is making satisfactory progress in physical therapy, but his therapist notes limitations in external rotation to neutral. A stretching program is started, and the patient suddenly gains 90 degrees of external rotation but now reports increased pain and weakness. What is the best course of action?
Explanation
Nearly all approaches to shoulder arthroplasty require detachment of the subscapularis tendon from the humerus and subsequent repair. Healing of this tenotomy is one of the limiting factors in postoperative recovery. Failure of the tenotomy repair must be recognized and treated early with repeat repair or pectoralis muscle transfer for optimal results. Failure of the subscapularis is diagnosed clinically as excessive external rotation and weakness, especially in the lift-off or belly press position. Muscle testing can be difficult in the postoperative period and may not be possible to assess in those positions. Although MRI might be useful to confirm the diagnosis, studies may be limited by artifact. CT or electromyography would not be diagnostic. Wirth MA, Rockwood CA Jr: Complications of total shoulder-replacement arthroplasty. J Bone Joint Surg Am 1996;78:603-616.
Question 937
High Yield
An excessively large radial styloidectomy poses a risk for wrist instability. What ligament is at greatest risk for injury?
Explanation
The radioscaphocapitate ligament is the most radial of the extrinsic volar ligaments of the wrist. It has a mean attachment to the radius 4 mm from the tip of the radial styloid. Nakamura T, Cooney WP III, Lui WH, et al: Radial styloidectomy: A biomechanical study on the stability of the wrist joint. J Hand Surg Am 2001;26:85-93.
Question 938
High Yield
A 30-year-old man who sustained a tibial fracture with a peroneal nerve palsy 2 years ago now has a drop foot and weak eversion of the foot. He reports success with stretching exercises, but he catches his toes when his foot tires. Examination reveals that the foot is plantigrade and supple. What is the next most appropriate step in management?
Explanation
The patient has a supple plantigrade foot that would benefit from a drop foot brace to prevent catching of the toes. Tendon transfer should not be considered until the patient has undergone bracing. Achilles tendon lengthening is not necessary because the foot is plantigrade and flexible. Nerve grafting is not indicated because of the length of time the peroneal nerve palsy has been present. Dehne R: Congenital and acquired neurologic disorders, in Mann RA, Coughlin MJ (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, vol 1, pp 552-553.
Question 939
High Yield
Which of the following muscles has dual innervation?

Explanation
The brachialis muscle typically receives dual innervation. The major portion is innervated by the musculocutaneous nerve. Its inferolateral portion is innervated by the radial nerve. The others listed have single innervation. The anterior approach to the humerus, which requires splitting of the brachialis, capitalizes on this dual innervation.
Question 940
High Yield
The stiffness of a 16-mm femoral stem is mostly influenced by the
Explanation
The stiffness is most influenced by the geometry, in particular the diameter of the stem. The bending rigidity increases to the fourth power of the radius. The elastic modulus of the material increases as a direct linear relationship. The surface coating does not affect the bending rigidity greatly unless it increases the diameter significantly.
Question 941
High Yield
In Charcot-Marie-Tooth disease a progressive deformity develops in the foot. Which functional muscles predominate in deformity formation?
Explanation
In Charcot-Marie-Tooth disease, the posterior tibialis and peroneus longus tendons remain strong, serving to invert the hindfoot and depress the first metatarsal head thus causing the cavovarus foot associated with this disease. In contrast, the tibialis anterior and peroneus brevis are less functional and therefore cannot dorsiflex the ankle, elevate the first metatarsal, or evert the foot, contributing to the deformity.
Question 942
High Yield
Figure 37 shows the T2-weighted MRI scan of the hip joint. What structure is labeled A?
Explanation
The obturator internus originates on the obturator membrane and adjacent bone, including the quadrilateral plate, and exits the lesser sciatic notch to insert on the posterior medial greater trochanter. The structure labeled C is the pectineus, B is the sartorius, and D is the gluteus medius. Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, pp 145-150, 324.
Question 943
High Yield
What is the primary role of superficial zone protein (SZP) in articular cartilage?
Explanation
Lubricin and SZP share a similar primary structure but may differ in posttranslational modifications with O-linked oligosaccharides. The primary physiologic function of SZP appears to be boundary lubrication. SZP does not influence interleukin-1, collagenase, or TIMP directly because these proteins are associated with articular cartilage turnover. Hlavacek M: The influence of the acetabular labrum seal, intact articular superficial zone and synovial fluid thixotropy on squeeze-film lubrication of a spherical synovial joint. J Biomech 2002;35:1325-1335.
Question 944
High Yield
A 27-year-old woman with Down syndrome has a severe bunion with pain and deformity in the left forefoot. Nonsurgical management has failed to provide relief. She does not use any assistive ambulatory devices. A radiograph is shown in Figure 21. Treatment should now consist of

Explanation
The patient requires an arthrodesis of the first metatarsophalangeal joint because of the abnormal neuromuscular forces. The more traditional bunionectomies such as a distal chevron bunionectomy, a proximal first metatarsal osteotomy, and a double osteotomy have a high failure rate because of the underlying Down syndrome. The Keller procedure is indicated for older, sedentary individuals and has little role in the management of a neuromuscular bunion. Coughlin MJ, Abdo RV: Arthodesis of the first metatarsophalangeal joint with Vitallium plate fixation. Foot Ankle Int 1994;15:18-28.
Question 945
High Yield
An otherwise healthy 65-year-old man reports thigh pain of insidious onset. He states that the pain is increased with weight bearing and also occurs at night. He denies any history of cancer. Radiographs are shown in Figures 22a and 22b. A bone scan shows an isolated lesion. CT scans of the chest and abdominal are negative for any other lesions. Initial management should consist of


Explanation
The patient has a solitary lesion that is at high risk for fracture. While metastatic lesions are most common in this age group, a stabilization procedure is contraindicated until results of a biopsy confirm the presence of a metastasis. Because of the lytic lesion and the associated calcification shown on the radiograph, the most likely diagnosis is a chondrosarcoma. Therefore, any type of stabilization procedure with a rod or plate would compromise a wide surgical excision to remove the entire proximal femur. Radiation therapy and chemotherapy are also contraindicated until biopsy results are obtained. Because of these factors, obtaining a frozen section biopsy specimen is considered the next most appropriate step in management. If a metastatic lesion is confirmed on the frozen section, a stabilization procedure could then be performed under the same anesthetic. Therefore, it is important to have a pathologist available at the time of a biopsy. Frassica FJ, Frassica DA, McCarthy EF, Riley LH III: Metastatic bone disease: Evaluation, clinicopathologic features, biopsy, fracture risk, nonsurgical treatment, and supportive management. Instr Course Lect 2000;49:453-459.
Question 946
High Yield
Hamstring lengthening and posterior transfer of the rectus femoris will be most successful in a patient with cerebral palsy who has which of the following gait abnormalities?
Explanation
Children with cerebral palsy typically ambulate with a crouched gait characterized by excessive flexion of the hips and knees during stance. Many patients exhibit co-contracture of the quadriceps and hamstrings, causing a stiff-knee gait. Normally, the rectus femoris fires at the initiation of swing and in terminal swing through initial contact. Prolonged activity of the rectus femoris throughout the swing phase interferes with normal knee flexion. This contributes to a stiff knee during swing phase and prevents clearance of the foot. Lengthening of the hamstrings alone will not improve foot clearance. Hamstring lengthening is contraindicated when there is hyperextension during stance. Transfer of the rectus femoris to one of the knee flexors has been shown to improve knee flexion during swing by an average of 15 degrees. This allows improved foot clearance. Gage JR, Perry J, Hicks RR, Koop S, Werntz JR: Rectus femoris transfer to improve knee function of children with cerebral palsy. Dev Med Child Neurol 1987;29:159-166.
Question 947
High Yield
A patient who underwent an L5-S1 diskectomy 18 months ago has persistent pain in the left leg. Figures 9a and 9b show postoperative axial T1-weighted MRI scans at the L5-S1 level without and with gadolinium. What is the most likely diagnosis?
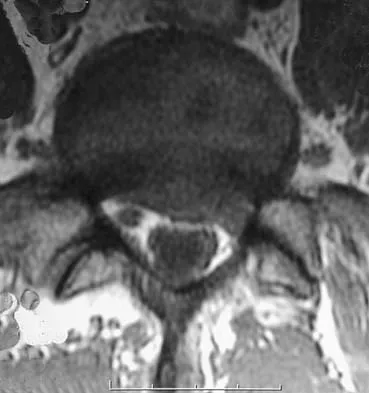

Explanation
Persistent or recurrent symptoms after lumbar diskectomy are troublesome and can be difficult to assess. Gadolinium-enhanced MRI scans may be helpful. The images show enhancement about the left S1 root, a finding that is most consistent with perineural (epidural) fibrosis. The root itself does not enhance. Root enhancement has been associated with compressive radicular symptoms. A disk herniation does not enhance with gadolinium. A neurilemmoma enhances with gadolinium, but the involved root would be enlarged. There is no evidence of a fluid collection which would be consistent with an epidural abscess. Babar S, Saifuddin A: MRI of the post-discectomy lumbar spine. Clin Radiol 2002;57:969-981. Kikkawa I, Sugimoto H, Saita K, et al: The role of Gd-enhanced three-dimensional MRI fast low-angle shot (FLASH) in the evaluation of symptomatic lumbosacral nerve roots. J Orthop Sci 2001;6:101-109.
Question 948
High Yield
A college football player performs bicep curls as part of his weight lifting routine. During the flexion phase of the curl, what term defines the type of muscle contraction?
Explanation
Muscle contractions can be classified by tension, length, and velocity. Isometric contractions involve changing tension in the muscle while the muscle stays at a constant length. An example would be pushing against a wall. Isokinetic contractions occur when the muscle maximally contracts at a constant velocity. Isotonic contractions involve constant tension throughout the range of motion. Eccentric contraction is when the muscle lengthens during contraction. Eccentric contractions have the highest risk of injury. Plyometrics are eccentric contractions at a rapid rate. Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 89-125.
Question 949
High Yield
When comparing the overall outcomes of surgical versus nonsurgical treatment of stable thoracolumbar burst fractures in patients without neurologic injury, 5 years following injury, the principle differences lie in
Explanation
When patients are compared at 5 years follow-up, there are no statistically significant differences between the two groups with respect to kyphosis, the degree of retropulsed bone resorption, pain and function levels, or the ability to return to work. Nonsurgical management of stable neurologically intact burst fractures has a very low incidence of complications. Wood K, Butterman G, Mehbod A, et al: Operative compared with nonoperative treatment of a thoracolumbar burst fracture without neurological deficit: A prospective, randomized study. J Bone Joint Surg Am 2003;85:773-781.
Question 950
High Yield
A 24-year-old man sustained a grade IIIb open tibial fracture and an ipsilateral grade IIIa femoral fracture in a motorcycle accident. He is unresponsive, intubated, and has a Glasgow Coma Scale score of 8. He is resuscitated and taken to the operating room for definitive orthopaedic care. Which of the following intraoperative problems will most likely adversely affect his long-term outcome?
Explanation
Traumatic brain injury is considered to be either primary or secondary. Primary injury is direct or impact damage to the brain, and secondary injury can have intracranial or systemic causes. While treatment has little impact on primary brain injury, secondary brain injury can be avoided. There are also many causes of intracranial secondary brain injury, including intracranial hypertension or cerebral edema. There are many causes of systemic secondary brain injury, but none has a greater impact on outcome than hypotension or hypoxia. In fact, the occurrence of hypotension postinjury causes a 10- to 15-fold increase in mortality. In a series by Pietropaoli and associates, the mortality rate for head-injured patients that were normotensive during surgery was 25%, but if they were hypotensive the mortality rate was 82%. In the same series, the number of patients with a Glasgow Coma Scale score of either 4 or 5 dropped from 58% in those patients that were normotensive during surgery to 6% in those patients that became hypotensive during surgery. Efforts to avoid hypotension postinjury and especially during surgery should be of primary importance. Chesnut RM, Marshall LF, Klauber MR, et al: The role of secondary brain injury in determining outcome from severe head injury. J Trauma 1993;34:216-222. Pietropaoli JA, Rogers FB, Shackford SR, Wald SL, Schmoker JD, Zhuang J: The deleterious effects of intraoperative hypotension on outcome in patients with severe head injury. J Trauma 1992;33:403-407. Schmeling GJ, Schwab JP: Polytrauma care: The effect of head injuries and timing of skeletal fixation. Clin Orthop 1995;318:106-116.
Question 951
High Yield
Figure 19 shows the radiograph of a 6-month-old infant who has limited hip motion. History reveals no complications during pregnancy or delivery. Examination reveals that hip abduction is 45 degrees in flexion bilaterally. The neurologic examination is normal. What is the best course of action?

Explanation
Diminished hip abduction can occur in normal children and is not always associated with hip pathology; therefore, initial management should consist of observation.
Question 952
High Yield
A 69-year-old woman is seen in the emergency department with a bilateral C5-6 facet dislocation and complete quadriplegia after falling down a flight of stairs. After initial evaluation and treatment by the trauma service, she is moved to the intensive care unit. Examination reveals a blood pressure of 90/50 mm/Hg, a pulse rate of 50/min, a respiration rate of 12/min, and urine output of 1 mL/kg/h. Her hemodynamic status should be addressed by
Explanation
The patient's heart rate is not responding to hypotension with tachycardia, as would be expected in the event of hypovolemic shock. Additionally, the adequate urine output suggests proper fluid resuscitation. Instead, she is bradycardic, possibly indicating neurogenic shock and loss of sympathetic tone to the heart. A Swan-Ganz catheter should be used to help differentiate these problems and guide appropriate fluid resuscitation and use of vasopressor agents. Hadley MN: Management of acute spinal cord injuries in an intensive care unit or other monitored setting. Neurosurgery 2002;50:S51-S57.
Question 953
High Yield
Figures 21a and 21b show the radiographs of a 12-year-old patient with an L4-level myelomeningocele who has scoliosis that has been slowly progressing for the past several years. There has been no loss of motor function. An MRI scan shows no syringomyelia or increased hydrocephalus. Management should consist of


Explanation
Scoliosis is a common occurrence in children with myelomeningocele, with the incidence increasing as the neurologic level moves cephalad. The rate of pseudarthrosis for isolated anterior or posterior fusions has been reported as high as 75%. The combination of anterior and posterior fusions with some type of instrumentation has been shown to decrease the rate of pseudarthrosis to 20%. Brace treatment in smaller curves can be used as a temporizing measure to delay surgery, but as with idiopathic scoliosis, the brace is ineffective for larger curves. Observation is not indicated with a curve of this magnitude. Ward WT, Wenger DR, Roach JW: Surgical correction of myelomeningocele scoliosis: A critical appraisal of various spinal instrumentation systems. J Pediatr Orthop 1989;9:262-268.
Question 954
High Yield
What changes in muscle physiology would be expected in an athlete who begins a rigorous aerobic program for an upcoming marathon?
Explanation
Muscle fibers can be categorized grossly into two types. Type I muscle, also known as slow-twitch muscle, is responsible for aerobic, oxidative muscle metabolism. It has a much lower strength and speed of contraction than fast-twitch type II muscle but is significantly more fatigue resistant. With training for endurance sports, the type I muscle undergoes adaptive changes to the increased stress. Increases in capillary density, oxidative capacity, mitochondrial density, and subsequent fatigue resistance are all observed changes. Hypertrophy of type IIb muscle is seen in strength training. Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 89-125.
Question 955
High Yield
What is the most significant prognostic factor in nontraumatic osteonecrosis of the humeral head?

Explanation
Use of systemic steroids has been implicated in the development of nontraumatic osteonecrosis of the humeral head. Staging of the disease is most relevant to prognosis and treatment. Cruess has described a widely accepted staging system. Several authors have shown that patients who have a lower stage of disease (ie, stage I or II) have a much less likely chance of progression compared with those who are in the later stages (IV and V). Cruess RL: Osteonecrosis of bone: Current concepts as to etiology and pathogenesis. Clin Orthop 1986;208:30-39. Cruess RL: Steroid-induced avascular necrosis of the humeral head: Natural history and management. J Bone Joint Surg Br 1976;58:313-317. Rutherford CS, Cofield RH: Osteonecrosis of the shoulder. Orthop Trans 1987;11:239.
Question 956
High Yield
Which of the following is considered the best method for the prevention of wrong-site surgery?
Explanation
The best method of preventing wrong-site surgery is for the surgeon to initial the surgical site in the preoperative holding area after discussion and confirmation of the site with the patient. This should be done before sedating medications are administered. A recent study found that patient noncompliance with specific preoperative instructions to mark the site with a "yes" at home was surprisingly high; only 59% of the patients marked the extremity correctly and 37% made no mark. Noncompliance was higher in those with workers' compensation claims (70%) and those with previous related surgery (51%). DeGiovanni CW, Kang L, Manuel J: Patient compliance in avoiding wrong site surgery. J Bone Joint Surg Am 2003;85:815-819.
Question 957
High Yield
The axis of forearm rotation occurs between what two anatomic points?

Explanation
Forearm rotation results from a complex interaction of osseous articulations and soft tissues including the radiocapitellar articulation, proximal and distal radioulnar joints, the interosseous membrane, and the adjacent forearm muscles. The rotation occurs around a longitudinal forearm axis extending from the center of the radial head proximally through the foveal region of the ulnar head distally. Werner FW, An KN: Biomechanics of the elbow and forearm. Hand Clin 1994;10:357-373.
Question 958
High Yield
In an effort to reduce costs, a limited MRI sequence is planned to detect a possible occult hip fracture. What is the anticipated fracture signal?
Explanation
At present, radiologists perform multiple MRI images to rule out all possible diagnoses. The ability to specify the anticipated changes on MRI should become more important as a means of reducing costs. MRI is sensitive to changes in free water (or hemorrhage) and thus this will appear dark on T1 and bright on T2. Miller MD: Review of Orthopaedics, ed 3. Philadelphia PA, WB Saunders, 2000, p 116.
Question 959
High Yield
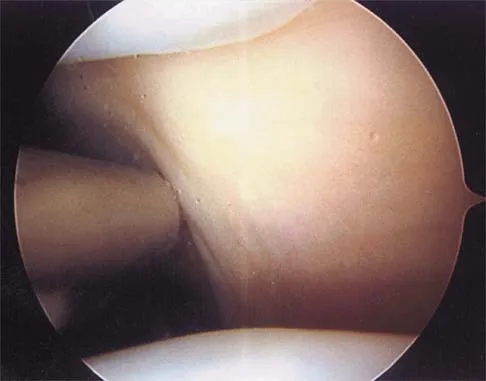
In the arthroscopic photograph shown in Figure 5, the structure labeled "A" functions primarily as a restraint to translation of the humeral head in what direction?
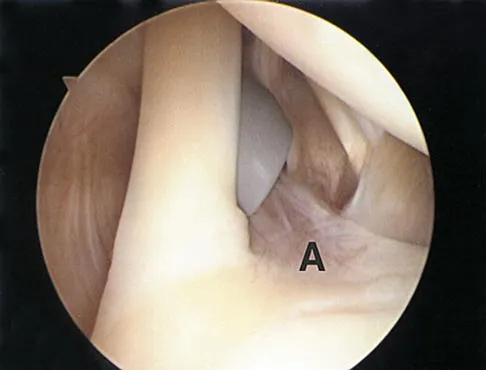
Explanation
The superior glenohumeral ligament identified as "A" in the figure functions primarily as a restraint to inferior glenohumeral translation of the adducted arm. The middle glenohumeral ligament is highly variable and pooly defined in up to 40% of the population and functions to restrain anterior translation of the externally rotated arm in the midrange of abduction. The anterior band of the inferior glenohumeral ligament is the primary restraint to anterior/inferior translation of the head with the shoulder abducted to 90 degrees and in maximum external rotation. Ticker JB, Bigliani LU, Soslowskiy LJ, et al: Inferior glenohumeral ligament: Geometric and strain-rate dependent properties. J Shoulder Elbow Surg 1996;5:269-279.
Question 960
High Yield
A patient with rheumatoid arthritis has a rupture of the extensor digitorum communis to 4 and 5. You are planning to perform an extensor indicis proprius (EIP) tendon transfer. What effect will this have on index finger extension?
Explanation
EIP transfer results in no functional deficit. If the tendon is cut proximal to the sagittal band, there will be no extensor deficit. Browne EX, Teague MA, Snyder CC: Prevention of extensor lag after indicis proprius transfer. J Hand Surg Am 1979;4:168-172.
Question 961
High Yield
Figures 17a and 17b show the radiographs of a 32-year-old professional athlete who sustained an injury to the first metatarsal. A view of the opposite noninjured side is shown in Figure 17c. Management of the fracture should consist of



Explanation
Parameters for first metatarsal fracture management are different than for shaft fractures of the central second, third, and fourth metatarsals. The first metatarsal carries a greater load and if malunited, can create transfer lesions by virtue of uneven weight distribution; therefore, nonsurgical management is not indicated for this patient. Percutaneous pinning is not as likely to result in an anatomic reduction as open reduction and internal fixation. As his livelihood depends on an expeditious return to function, the choice of open reduction and internal fixation allows for earlier motion and rehabilitation. Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 64-65.
Question 962
High Yield
Patients with which of the following primary carcinomas have the shortest overall survival rate after a solitary metastasis to bone?
Explanation
The median survival of patients after discovery of bone metastasis from primary lung carcinoma is shorter compared with other primary sites.
Question 963
High Yield
The parents of a previously healthy 3-year-old child report that she refused to walk on awakening. Examination later in the day reveals that the patient can walk but with a noticeable limp. She has a temperature of 99.5 degrees F (37.5 degrees C). Range of motion measurements are shown in Figure 50. An AP pelvis radiograph is normal. Laboratory studies show a WBC count of 9,000/mm3 and an erythrocyte sedimentation rate of 10 mm/h. Management should consist of
Explanation
The patient has the typical history and presentation of transient synovitis of the hip, a condition that is more common in children age 2 to 5 years but which may affect children up to 12 years. The discomfort typically is noted on awakening, and the child will refuse to walk. Later in the day, the pain commonly improves and the child can walk but will have a limp. Mild to moderate restriction of hip abduction is the most sensitive range-of-motion restriction. The extent of the evaluation for transient synovitis depends on the intensity and duration of symptoms. Because she has been afebrile for the past 24 hours, observation is the management of choice. In the differential diagnosis of suspected transient synovitis, septic arthritis of the hip is the primary disorder to exclude. Osteomyelitis of the proximal femur also should be considered. In most patients, clinical examination will differentiate of these disorders to a reasonable certainty. Plain radiographs are normal in the early stage of an infectious process. Ultrasonography shows increased fluid in the hip joint in both transient synovitis and septic arthritis. MRI can differentiate the two conditions; however, this test would require general anesthesia and is not required in most patients in this age group. If a child with transient synovitis has a concurrent infectious process such as an upper respiratory tract infection or otitis media, the temperature will most likely be elevated. In this situation, a full evaluation for an infectious process and initiation of IV antibiotics should be considered. This would include radiographs, CBC count, erythrocyte sedimentation rate, blood cultures, aspiration of the hip joint, and IV antibiotics. Del Beccaro MA, Champoux AN, Bockers T, Mendelman PM: Septic arthritis versus transient synovitis of the hip: The value of screening laboratory tests. Annals Emerg Med 1992;21:1418-1422.
Question 964
High Yield
A 75-year-old woman has had severe shoulder pain for the past month. Her medical history includes hypertension and a total nephrectomy for renal cell carcinoma 7 years ago. Radiographs and sagittal MRI scans are shown in Figures 36a through 36d. A bone scan reveals this to be an isolated lesion. Biopsy findings are consistent with metastatic renal cell carcinoma. What is the most appropriate treatment for this patient?


Explanation
Resection and reconstruction of this very proximal lesion provides the best chance to avoid hardware complications that may be associated with stabilization procedures. Wide resection of isolated renal cell carcinoma metastasis, which presents distant to the nephrectomy, may improve long-term survival. Fuchs B, Trousdale RT, Rock MG: Solitary bony metastasis from renal cell carcinoma: Significance of surgical treatment. Clin Orthop Relat Res 2005;431:187-192.
Question 965
High Yield
A 32-year-old woman sustained a closed calcaneus fracture 2 years ago and was treated nonsurgically. She now reports a 6-month history of progressively worsening pain over the anterior ankle and lateral hindfoot. Climbing stairs and ascending slopes is particularly difficult for her. Bracing and intra-articular corticosteroid injections have not provided sufficient relief. Figure 36 shows a weight-bearing lateral radiograph. What is the most appropriate surgical option?

Explanation
Intra-articular fractures of the calcaneus often include depression of the posterior facet of the subtalar joint. This can lead to dorsiflexion of the talus because of diminished height posteriorly. In a weight-bearing position, the dorsal surface of the talar neck can impinge against the distal tibia, causing anterior ankle pain. In addition, posttraumatic arthritis of the subtalar joint typically occurs after a calcaneus fracture. The patient's symptoms are consistent with both anterior ankle impingement and subtalar degenerative arthritis. The Bohler angle, approximately 15 degrees, confirms depression of the posterior facet. Distraction subtalar arthrodesis with a corticocancellous bone block autograft will improve talar declination, decrease anterior impingement, and address the subtalar degenerative arthritis simultaneously. Rammelt S, Grass R, Zawadski T, et al: Foot function after subtalar distraction bone-block arthrodesis: A prospective study. J Bone Joint Surg Br 2004;86:659-668.
Question 966
High Yield
Which of the following factors is associated with decreases in active periprosthetic osteolysis in total hip arthroplasty?
Explanation
A 32-mm head design results in less linear wear but more volumetric wear particles. Modular components that allow motion between the polyethylene insert and the shell can result in backside wear. The oxidative degradation of gamma-irradiated polyethylene stored in air leads to increased wear. All of these factors lead to a greater particulate load and more osteolysis. Circumferential porous coating blocks ingrowth of particle-laden fluid and decreases osteolysis. Bartel DL, Bicknell VL, Wright TM: The effect of conformity, thickness, and material on stresses in ultra-high molecular weight components for total joint replacement. J Bone Joint Surg Am 1986;68:1041-1051. Fisher J, Hailey JL, Chan KL, et al: The effect of aging following irradiation on the wear of UHMWPE. Trans Orthop Res Soc 1995;20:12.
Question 967
High Yield
An orthopaedic surgeon frequently uses hip and knee prostheses from a specific manufacturer. The surgeon becomes acquainted with the manufacturer's representative who provides the support for these prostheses in the hospital. They develop a personal relationship outside of work through a common interest in sailing. Together they become interested in buying a sailboat. The manufacture's representative suggests a partnership in a boat costing $200,000. The manufacture's representative would purchase a 90% interest and the surgeon a 10% interest in the boat. There would be no restrictions on use of the boat by the surgeon. What should the orthopaedic surgeon do?
Explanation
Rejecting this proposal is the only appropriate course of action. Accepting it would, in essence, be receiving a huge gift from industry in the form of a sailboat. Physicians frequently assert that they are not influenced by gifts and relationships with industry representatives, but evidence is to the contrary. Such an arrangement constitutes a tremendous incentive to use the manufacturer's products. The fact that the boat partnership seems completely outside of the orthopaedic business relationship does not excuse it. Conflicts of interest should always be resolved and in the best interest of patient care, and in this case the best course clearly is to avoid the conflict of interest totally. An equal interest in the boat does not eliminate the conflict of interest. AAOS Standard of Professionalism -Orthopaedist -Industry Conflict of Interest (Adopted 4/18/07), Mandatory Standard numbers 6-8. www3.aaos.org/member/profcomp/SOPConflictsIndustry.pdf Opinions on Ethics and Professionalism: The Orthopaedic Surgeon's Relationship with Industry (Document 1204), in Guide to the Ethical Practice of Orthopaedic Surgery, ed 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2007, pp 36-40. www.aaos.org/about/papers/ethics/1204eth.asp AdvaMed Code of Ethics on Interactions with Health Care Professionals, Advanced Medical Technology Association, Washington, DC. www.AdvaMed.org
Question 968
High Yield
When performing ankle arthroscopy through the anterolateral portal, what anatomic structure is at greatest risk?
Explanation
The superficial branch of the peroneal nerve travels subcutaneously anterior to the lateral malleolus at the ankle. It can be easily damaged by deep penetration of the knife blade when making this portal or when passing shavers in and out of the portal. Anesthesia or dysesthesia from laceration or neuroma formation can cause significant postoperative morbidity. The anterior tibialis tendon, anterior tibial artery, and the deep peroneal nerve are located much more anterior and central on the ankle. The sural nerve is posterior lateral to the ankle and is not at risk from this portal. Ferkel RD, Heath DD, Guhl JF: Neurological complications of ankle arthroscopy. Arthroscopy 1996;12:200-208.
Question 969
High Yield
A 40-year-old man reports an enlarging soft-tissue mass in his right shoulder. Based on the MRI scan and biopsy specimens shown in Figures 40a through 40c, what is the most likely diagnosis?
Explanation
Nodular fasciitis is a pseudosarcomatous, self-limiting reactive process composed of fibroblasts and myofibroblasts. Most patients give a history of a rapidly growing mass that has been present for only a few weeks. Many have pain associated with the mass and can recall a specific traumatic event predating the presence of the lesion. It can occur at any age but is most commonly seen in adults who are 20 to 40 years of age. Histologically, the lesion is composed of predominantly plump, immature-appearing fibroblasts that bear a close resemblance to the fibroblasts found in granulation tissue. Characteristically, the fibroblasts are arranged in short, irregular bundles and fascicles and are adjacent to collagen and reticulin. The lesions can appear to be more myxoid or more fibrotic in nature and this correlates to the duration of symptoms. The lesions with a short duration of symptoms have a more myxoid appearance in contrast to those of longer duration characterized by hyaline fibrosis. Weiss SW, Goldblum JR, Enzinger FM: Enzinger and Weiss's Soft Tissue Tumors, ed 4. Philadelphia, PA, Elsevier, 2001, pp 250-266.
Question 970
High Yield
A 53-year-old man has a 4- x 5-cm high-grade soft-tissue sarcoma in the midthigh. As part of the staging evaluation, regional nodes should be assessed by

Explanation
In general, soft-tissue metastases to regional nodes are a relatively rare occurrence (less than 5% overall). The incidence of lymphatic metastasis is highest for synovial sarcoma, rhabdomyosarcoma, clear cell sarcoma, and epithelioid sarcoma. Regional nodes should be assessed clinically. CT is not used to routinely assess regional nodes. Evaluation of a sentinal node is not indicated because of the low incidence of regional nodal involvement. Fine needle aspiration may be indicated to assess clinically suspicious nodes. Prophylactic inguinal node dissection is contraindicated because it may lead to unnecessary complications such as lymphedema.
Question 971
High Yield
A 45-year-old man who underwent an open capsulolabral stabilization procedure 15 years ago now reports pain and has no external rotation on the affected side. Nonsurgical management has failed to provide relief. Examination reveals external rotation to -5 degrees compared with 50 degrees of external rotation on the contralateral side. Radiographs show a small inferior osteophyte and minimal posterior glenoid wear. Which of the following procedures will offer the best chance of restoring motion, decreasing pain, and preserving the native joint?
Explanation
Loss of external rotation following stabilization procedures can result in progressive degenerative joint disease. A tight anterior capsule results in posterior humeral translation and progressive posterior glenoid wear. Patients with early degenerative joint disease and pain can be treated with anterior release to restore more normal glenohumeral biomechanics. This procedure not only improves function but also decreases pain in most patients. Closed manipulation at 15 years after surgery is unlikely to be successful and carries the risk of complications. Acromioplasty, posterior release, and removal of osteophytes do not address the pathology. Arthroscopic releases are favored for intra-articular procedures that have addressed the pathology of instability. Open releases are recommended for nonanatomic extra-articular repairs that include subscapularis tightening procedures. MacDonald PB, Hawkins RJ, Fowler PJ, et al: Release of the subscapularis for internal rotation contracture and pain after anterior repair for recurrent anterior dislocation of the shoulder. J Bone Joint Surg Am 1992;74:734-737.
Question 972
High Yield
The vessel seen in the clinical photographs shown in Figures 50a and 50b (1,2 intercompartmental supraretinacular artery) is being dissected to be used as a source of vascularized bone graft for a patient who is scheduled to undergo internal fixation of a scaphoid nonunion. This vessel is a branch of what artery?


Explanation
The 1,2 intercompartmental supraretinacular artery is a branch of the radial artery. The vessel provides a reliable source of vascularized bone graft with an adequate pedicle length for use in scaphoid nonunions. Sheetz KK, Bishop AT, Berger RA: The arterial blood supply of the distal radius and ulna and its potential use in vascularized pedicled bone grafts. J Hand Surg 1995;20:902-914.
Question 973
High Yield
Which of the following findings is a relative contraindication to primary total knee arthroplasty?
Explanation
Contraindications to primary total knee arthroplasty include active infection, an incompetent extensor mechanism, compromised vascularity in the extremity, and local neurologic disruption affecting the competence of the musculature about the knee. Anterior cruciate, posterior cruciate, or lateral ligament incompetence can be managed with primary total knee arthroplasty. Mild flexion contracture and previous high tibial valgus osteotomy are not contraindications to primary total knee arthroplasty.
Question 974
High Yield
Femoral osteotomy for dysplasia of the hip will most likely result in
Explanation
Patients should expect pain relief after femoral osteotomy for hip dysplasia. Patients should not expect improved motion or abduction strength and should be counseled about a postoperative limp and unequal limb lengths. Pellicci PM, Hu S, Garvin KL, Salvati EA, Wilson PD Jr: Varus rotational femoral osteotomies in adults with hip dysplasia. Clin Orthop 1991;272:162-166.
Question 975
High Yield
A 24-year-old dancer sustains the injury shown in Figure 28. Management should consist of

Explanation
The patient has a moderately displaced distal diaphyseal fracture of the fifth metatarsal, and the most appropriate treatment is brief immobilization and symptomatic management. Attempts at closed reduction are unlikely to appreciably alter the position of the fracture. Surgical techniques for either reduction of the fracture or fixation have not been shown to result in improved functional outcomes. O'Malley MJ, Hamilton WG, Munyak J: Fractures of the distal shaft of the fifth metatarsal: "Dancer's Fracture." Am J Sports Med 1996;24:240-243. DeLee JC: Fractures and dislocations of the foot, in Mann RA, Coughlin MJ (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, CV Mosby, 1993, pp 1465-1703.
Question 976
High Yield
A 22-year-old man sustained a stable pelvic fracture, bilateral femur fractures, and a left closed humeral shaft fracture in a motor vehicle accident. Examination 24 hours after injury reveals that the patient is confused and has shortness of breath. A clinical photograph of his conjunctiva is shown in Figure 44. He has a temperature of 101 degrees F (38.3 degrees C) and a pulse rate of 120/min. Laboratory studies show a hemoglobin level of 8 g/dL, a platelet count of 50,000/mm3, and a PaO2 of 57 mm Hg on 2L of oxygen. What is the most likely diagnosis?

Explanation
The major criteria for the diagnosis of fat embolism syndrome include hypoxemia (PaO2 of less than 60 mm Hg), central nervous system depression, and a petechial rash that is most often located in the axillae, conjunctivae, and palate. The rash is often transient. Tachycardia, pyrexia, anemia, thrombocytopenia, and the presence of fat in the urine are all considered minor criteria. To establish the diagnosis of fat embolism syndrome, one major and four minor signs should be present. Pulmonary embolism, which is the major differential diagnosis, usually is not associated with conjunctival petechia or thrombocytopenia.
Question 977
High Yield
Using methylmethacrylate to fill a biopsy hole in the diaphysis of a femur theoretically achieves what purpose?

Explanation
Placing cement over a bone biopsy site prevents tumor contamination by controlling hematoma. Even though the use of cement may impart some strength, the femur is still at significant risk for fracture. The use of bone cement in this manner has not been cleared by the FDA, but many physicians feel that it is appropriate when the patient's health status has been given careful consideration, and the physician has the necessary knowledge and training. The other options are not important reasons to use methylmethacrylate in biopsies. Simon MA, Springfield DS, et al: Biopsy: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 55-65.
Question 978
High Yield
An 82-year-old woman fell on her right shoulder 2 days ago. She is alert, oriented, and in mild discomfort. Prior to falling, she lived alone and functioned independently. Examination reveals extensive ecchymosis extending to the midhumeral region. Her neurovascular examination is normal. Radiographs are shown in Figures 41a and 41b. What is the most appropriate management?


Explanation
The patient has a displaced four-part proximal humerus fracture. Given her age and the presence of osteopenia, a cemented hemiarthroplasty is the treatment of choice. The glenoid is uninjured so a total shoulder arthroplasty is not indicated. Percutaneous pinning in younger individuals with good bone quality may be indicated but not in an 82-year-old woman with osteopenia. Sling immobilization and immediate pendulum exercises will lead to a nonunion. Sling immobilization for 6 weeks followed by active range of motion will result in a nonunion or malunion with unacceptable functional results. Neer CS II: Displaced proximal humeral fractures: I. Classification and evaluation. J Bone Joint Surg Am 1970;52:1077-1089.
Question 979
High Yield
An active 49-year-old woman who sustained a diaphyseal fracture of the clavicle 8 months ago now reports persistent shoulder pain with daily activities. An AP radiograph is shown in Figure 8. Management should consist of

Explanation
The radiograph reveals an atrophic nonunion of the diaphysis of the clavicle. Electrical or ultrasound stimulation may be an option in diaphyseal nonunions that have shown some healing response with callus formation, but these techniques are not successful in an atrophic nonunion. The preferred technique for achieving union is open reduction and internal fixation with bone graft. Percutaneous fixation has no role in treatment of nonunions of the clavicle. Boyer MI, Axelrod TS: Atrophic nonunion of the clavicle: Treatment by compression plating, lag-screw fixation and bone graft. J Bone Joint Surg Br 1997;79:301-303.
Question 980
High Yield
A 62-year-old man has a severe pes planus and pain in the hindfoot. Radiographs show advanced degenerative changes at the talonavicular and subtalar joints with good preservation of the ankle joint. What is the most appropriate surgical procedure to alleviate his pain?
Explanation
Once degenerative changes have occurred, soft-tissue procedures are not indicated. Triple arthrodesis is the treatment of choice for adult-acquired flatfoot. Isolated fusion of the subtalar or talonavicular joint will not be sufficient to correct the problem. Lutter LD, Mizel MS, Pfeffer GB (eds): Orthopaedic Knowledge Update: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 269-282.
Question 981
High Yield
Figures 48a and 48b show the radiographs of a 26-year-old woman who fell down two steps and twisted her foot and ankle. What is the most appropriate treatment for this injury?


Explanation
The patient has a zone 1 base of the fifth metatarsal fracture (Pseudojones) that represents a less serious injury compared to zone 2 and 3 fractures with regard to healing potential. Treatment is symptomatic and casting is not necessary. These fractures are well treated with a hard-soled shoe for comfort and weight bearing as tolerated. Surgical intervention is not warranted. Vorlat P, Achtergael W, Haentjens P: Predictors of outcome of non-displaced fractures of the base of the fifth metatarsal. Int Orthop 2007;31:5-10. Wiener BD, Linder JF, Giattini JF: Treatment of fractures of the fifth metatarsal: A prospective study. Foot Ankle Int 1997;18:267-269.
Question 982
High Yield
A 52-year-old woman slipped on ice in her driveway. Radiographs are shown in Figures 19a and 19b. The patient was treated in a short leg cast with weight bearing as tolerated for 6 weeks. Due to persistent tenderness at the fracture site, a CAM walker was used for an additional 8 weeks. Nine months after the injury, the patient still walks with a limp and reports pain with deep palpation at the fracture site. What is the next most appropriate step in management?


Explanation
Persistent pain at the fracture site in the absence of infection is most likely due to a nonunion, best detected by CT. Walsh and DiGiovanni reported on a series of closed rotational fibular fractures in which nonunions were detected by CT in the absence of standard ankle radiographic findings. Repeat immobilization would not be appropriate at this late date. Pain management/sympathetic blocks would be considered if the patient displayed pain with light touch and disproportionate pain consistent with a complex mediated pain syndrome. Acupuncture would be expected to be of limited benefit. Walsh EF, DiGiovanni C: Fibular nonunion after closed rotational ankle fracture. Foot Ankle Int 2004;25:488-495.
Question 983
High Yield
What is the most commonly reported complication following elbow arthroscopy?

Explanation
The complication rate following elbow arthroscopy is reported at 5%. The most commonly reported complication is transient neurapraxia, with nerve transection remaining an unfortunate and rare event. While infection remains the most common serious complication, it is uncommon (0.8%). Synovial cutaneous fistula and compartment syndrome, while reported, are the least frequent complications of elbow arthroscopy. Kelly EW, Morrey BF, O'Driscoll SW: Complications of elbow arthroscopy. J Bone Joint Surg Am 2001;83:25-34.
Question 984
High Yield
A 55-year-old man has had a mass in his right thigh for the past 2 months. An MRI scan and biopsy specimens are shown in Figures 55a through 55c. What is the most likely diagnosis?
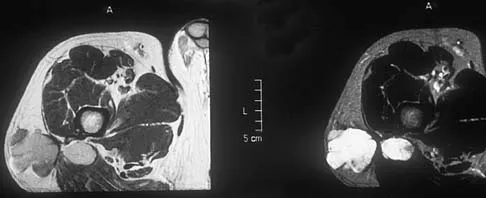
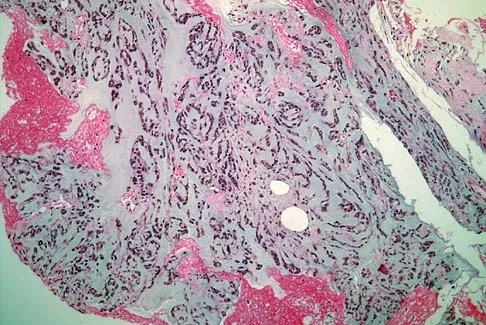
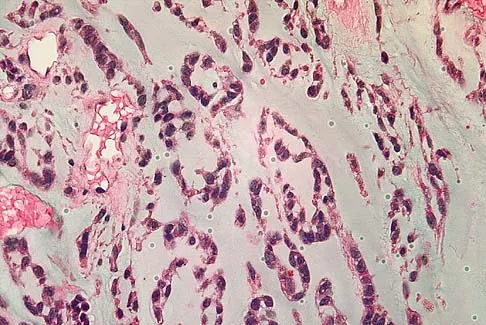
Explanation
The histology shows extraskeletal myxoid chondrosarcoma, characterized by abundant blue myxoid matrix with cords and nests of small tumor cells. Treatment consists of wide resection. Despite the name, hyaline cartilage is not a common component of these tumors. Adult rhabdomyosarcoma and malignant fibrous histiocytoma are highly pleomorphic sarcomas often containing multinucleated giant cells. Myxoid liposarcoma contains a prominent capillary network and lipoblasts. Myxoma is less cellular than extraskeletal myxoid chondrosarcoma and does not have a cord-like arrangement of tumor cells.
Question 985
High Yield
A 20-year-old collegiate football player sustains an injury to his left foot 3 weeks before the start of the fall season. Examination reveals localized tenderness over the lateral midfoot and normal foot alignment. Radiographs are shown in Figures 28a through 28c. What is the treatment of choice?



Explanation
Due to the relatively high incidence of delayed union and nonunion associated with this mildly displaced Jones-type fracture, and the temporal proximity to his playing season, intramedullary screw fixation is the treatment of choice in this collegiate athlete to best ensure healing and expedite his return to football. If nonsurgical management were elected, application of a non-weight-bearing short leg cast would be appropriate since a higher likelihood of healing is expected with it versus a short leg walking cast. The risk of recurrent fracture of fractures that heal with nonsurgical management has reportedly been high (approximately 30%). Quill GE: Fractures of the proximal fifth metatarsal. Orthop Clin North Am 1995;26:353-361. Torg JS, Balduini FC, Zelko RR, et al: Fractures of the base of the fifth metatarsal distal to the tuberosity: Classification and guidelines for nonsurgical and surgical management. J Bone Joint Surg Am 1984;66:209-214.
Question 986
High Yield
Figures 54a and 54b show the radiograph and MRI scan of a 7-year-old boy who has a painful right thoracic scoliosis that measures 35 degrees. Neurologic examination is normal. Management should consist of


Explanation
Because hydrosyringomyelia, with or without an Arnold-Chiari malformation, is now being recognized as the etiology of many infantile and juvenile idiopathic scolioses, management should consist of a neurosurgical consultation. Observation with follow-up radiographs is not an option in curves of this magnitude. A technitium Tc 99m bone scan is unnecessary because the etiology of the curve has been identified. Although spinal fusion may be needed in the future, it should not be undertaken before the neurosurgical problem has been addressed. Zadeh HG, Sakka SA, Powell MP, Mehta MH: Absent superficial abdominal reflexes in children with scoliosis: An early indicator of syringomyelia. J Bone Joint Surg Br 1995;77:762-767. Schwend RM, Hennrikus W, Hall JE, Emans JB: Childhood scoliosis: Clinical indications for magnetic resonance imaging. J Bone Joint Surg Am 1995;77:46-53.
Question 987
High Yield
In the treatment of thoracic disk herniations, what approach is associated with the highest risk of iatrogenic paraplegia?
Explanation
Laminectomy is associated with the highest risk of iatrogenic paraplegia because retraction on the cord is necessary for visualization, but retraction is difficult because of tethering of the intradural dentate ligaments. All of the other approaches allow for access to the disk herniation through an angle that avoids the cord itself, although other limitations may exist. Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 87-96.
Question 988
High Yield
Figures 8a and 8b show the current radiographs of a 10-year-old boy with a hip disorder who was treated with an abduction orthosis 3 years ago. If no further remodeling occurs, what is the most likely prognosis?


Explanation
The radiographs show a child with Legg-Calve-Perthes disease (LCPD) that has healed. Deformity (asphericity) of the femoral head is evident, but the femoral head and acetabulum are congruous. Stulberg and associates found that hips with aspherical congruity at skeletal maturity functioned well until the fifth or sixth decade of life. Similarly, another study found that degenerative arthritis caused deteriorating hip function after age 40 years in patients with this degree of residual deformity. Repeated episodes of ischemic necrosis are unlikely. Although some studies suggested coagulation abnormalities such as protein C and S deficiencies in children with LCPD, other studies failed to show any evidence of inherited thrombophila in most children with this disorder. There are no studies to suggest growth acceleration occurs following LCPD. Stulberg SD, Cooperman DR, Wallenstein R: The natural history of Legg-Calve-Perthes disease. J Bone Joint Surg Am 1984;66:479-489.
Question 989
High Yield
The bone avulsion shown in Figure 32 has a high correlation with tearing of the

Explanation
As described by Segond in 1987, an avulsion fracture of the lateral tibial plateau is commonly referred to as a Segond fracture. Subsequent to 1987, several authors have also found that the lateral capsular sign represents, but is not limited to, a disruption of the middle third of the lateral capsule and a tear of the anterior cruciate ligament. Bach BR, Warren RF: Radiographic indicators of anterior cruciate ligament injury, in Feagin JA (ed): The Crucial Ligaments. New York, NY, Churchill Livingston, 1988, pp 301-327. Segond P: Recherches cliniques et experimentales sur les epanchements sanguins du genou par entorse. Prog Med (Paris) 1987;7:297.
Question 990
High Yield
Which of the following knee ligament injury patterns is most associated with an increase in external tibial rotation with the knee at 90 degrees of flexion?
Explanation
Cadaveric studies have shown that external rotation of the tibia is most pronounced following transection of the posterior cruciate and lateral collateral ligaments with the knee at 90 degrees of flexion. Isolated release of the lateral collateral ligament results in increased external tibial rotation at 30 degrees. Gollehon DL, Torzilli PA, Warren RF: The role of the posterolateral and cruciate ligaments in the stability of the human knee: A biomechanical study. J Bone Joint Surg Am 1987;69:233-242. Cooper DE: Tests for posterolateral instability of the knee in normal subjects: Results of examination under anesthesia. J Bone Joint Surg Am 1991;73:30-36.
Question 991
High Yield
Which of the following tendons is found in the same dorsal compartment of the wrist as the posterior interosseous nerve?
Explanation
The terminal branch of the posterior interosseous nerve is contained in the fourth dorsal compartment. The contents of the various dorsal wrist compartments are as follows: 1st Compartment: Abductor pollicis longus, extensor pollis brevis; 2nd Compartment: Extensor carpi radialis brevis, extensor carpi radialis longus; 3rd Compartment: Extensor pollicis longus; 4th Compartment: Extensor digitorum comminus, extensor indicus proprius, posterior interosseous nerve; 5th Compartment: Extensor digiti minimi; 6th Compartment: Extensor carpi ulnaris. The extensor indicis proprius is also contained in the fourth dorsal compartment. The extensor digiti minimi is located in the fifth dorsal compartment. The extensor carpi radialis brevis is located in the second dorsal compartment. The extensor pollicis longus is located in the third dorsal compartment, and the abductor pollicis longus is located in the first dorsal compartment. Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics, ed 2. Philadelphia, PA, Lippincott-Raven, 1994, pp 150-151.
Question 992
High Yield
A 12-year-old child with spina bifida paraplegia requires brace management for ankle stability. Which of the following principles applies to brace management in this individual?
Explanation
Bracing for spina bifida paraplegia provides both support and improved function of the movable limb. An orthosis has value in controlling unstable joints. The three-point pressure effect applies a force above and below the joint to prevent it from buckling. A four-point pressure effect is only required for a two-joint system (this patient has problems only at the ankle). A longer lever arm brace and a brace with a greater area of support provide better stability. Finally, a straighter limb, without contracture, applies less pressure to the brace and lessens overload to the skin. Gage JR: An overview of normal walking. Instr Course Lect 1990;39:291-303. Bleck EE: Current concepts review: Management of the lower extremities in children who have cerebral palsy. J Bone Joint Surg Am 1990;72:140-144.
Question 993
High Yield
A 59-year-old man reports moderate shoulder pain and very restricted range of motion after undergoing humeral arthroplasty for osteoarthritis 1 year ago. An AP radiograph is shown in Figure 32. Management should now consist of

Explanation
The radiograph reveals that an insufficient amount of the proximal humerus was excised in the index procedure, resulting in malalignment of the humeral component, overstuffing of the glenohumeral joint, and glenoid arthritis. It is unlikely that physical therapy or soft-tissue releases alone will be adequate. Revision of the humeral component, recutting of the proximal humerus to allow a more anatomic alignment of the humeral component, appropriate soft-tissue releases, and glenoid arthroplasty will offer the best chance of improvement in this difficult situation. Neer CS II, Kirby RM: Revision of humeral head and total shoulder arthroplasties. Clin Orthop 1982;170:189-195.
Question 994
High Yield
What radiographic view will best reveal degeneration of the pisotriquetral joint in a patient who is being evaluated for pisotriquetral arthrosis?
Explanation
The pisotriquetral joint is best seen on a lateral view in 30 degrees of supination. The carpal tunnel view provides visualization of the joint but to a lesser extent. The other views do not provide clear and accurate visualization. Paley D, McMurty RY, Cruickshank B: Pathologic conditions of the pisiform and pisotriquetral joint. J Hand Surg Am 1987;12:110-119.
Question 995
High Yield
When performing knee arthroplasty, which of the following procedures provides the most consistent fixation for the tibial component?

Explanation
All of the options, except cementing the metaphyseal portion and press fitting the keel of the tibial component, have been shown to create strong and long-lasting constructs; however, cementing of both the platform and the keel offers the most predictable solution. Cementing the platform and not the keel has been shown to have a higher loosening rate than the more traditional methods of fully cementing or using screws to augment fixation.
Question 996
High Yield
A 21-year-old basketball player inverts his foot during practice. Examination reveals obvious deformity of the hindfoot with a prominence of the talar head dorsolaterally and medial displacement of the forefoot. A radiograph is shown in Figure 17. What is the most likely obstacle to closed reduction?

Explanation
The patient has a medial subtalar dislocation. These injuries should be reduced as soon as possible to minimize risk to the skin. Most often, this can be done easily, and further radiographic evaluation then can be performed as necessary. On rare occasions, closed reduction is not possible because of fractures of the articular surface of the talus, navicular, interposed extensor digitorum brevis, or transverse fibers of the cruciate crural ligament. The posterior tibial tendon is the most common obstruction to closed reduction in lateral subtalar dislocations, which are less common than medial dislocations. The majority of both injuries can be managed by closed reduction and immobilization. Mulroy RD: The tibialis posterior tendon as an obstacle to reduction of a lateral anterior subtalar dislocation. J Bone Joint Surg Am 1953;37:859-863. Heckman JD: Fractures and dislocations of the foot, in Rockwood CA, Green DP, Bucholz RW (eds): Fractures in Adults. Philadelphia, PA, JB Lippincott, 1991, pp 2093-2100.
Question 997
High Yield
A 70-year-old man has worn through his metal-backed patellar component and sustained damage to the femoral component. Following removal of the components and debridement of the metal-stained synovium, the surgeon finds that the thickness of the remaining patella is 10 mm. Treatment should now include
Explanation
Revision of a failed patellar component can be difficult because of bone loss and damage to the extensor mechanism. Several authors have advised against reinsertion of a patellar component if the residual patellar thickness is 10 mm or less. Leaving an unresurfaced bony remnant in place at the time of revision or reimplantation surgery has been shown to be a reasonable option; however, the results are of a lower quality when compared with revision surgery where the patellar component can be retained or revised. The other treatment options have not been shown to be effective approaches to this problem. Rand JA: The patellofemoral joint in total knee arthroplasty. J Bone Joint Surg Am 1994;76:612-620. Pagnano MW, Scuderi GR, Insall JN: Patellar component resection in revision and reimplantation total knee arthroplasty. Clin Orthop 1998;356:134-138.
Question 998
High Yield
A patient undergoes a proximal tibial resection that is reconstructed with a fresh frozen osteoarticular allograft. Eleven months later, the graft is retrieved. Histologically, the articular cartilage and subchondral bone retrieved would be expected to show evidence of
Explanation
Osteoarticular allografts are devoid of host chondrocytes but do contain "mummified" cellular debris left over from donor processing. The cartilage architecture is preserved in the first 2 to 3 years after transplantation. The articular surface is covered with a pannus of fibrocartilage maintaining the joint space radiographically; this pannus later contains islands of fibrocartilage containing host mesenchymal stem cells. Degenerative changes to the joint surface occur earlier and are more severe in joints that are unstable. Only with degenerative changes at the surface is there histologic evidence of subchondral revascularization. Often degenerative changes involving the articular cartilage reach the tidemark, but the tidemark itself remains structurally intact. Enneking WF, Campanacci DA: Retrieved human allografts: A clinicopathological study. J Bone Joint Surg Am 2001;83:971-986.
Question 999
High Yield
Figure 29 shows the AP radiograph of a 14-year-old boy. The radiographic findings are most consistent with what pathologic process?

Explanation
The severe depression of the proximal medial tibial epiphysis is most consistent with the diagnosis of neglected infantile Blount's disease. Blount's disease in adolescents produces a deformity in the metaphyseal region. Septic arthritis and JRA affect both sides of the joint. Hemophilia produces a characteristic widening of the intercondylar notch. Thompson GH, Carter JR: Late-onset tibia vara (Blount's Disease). Clin Orthop 1990;255:24-35.
Question 1000
High Yield
Late surgical treatment of posttraumatic cubitus varus (gunstock deformity) is usually necessitated by the patient reporting problems related to
Explanation
Cubitus varus, elbow hyperextension, and internal rotation are all typical components of the gunstock deformity. This deformity results from malunion of a supracondylar fracture of the humerus. All of the problems listed above have been reported as sequelae of a gunstock deformity, although the malunion usually causes no functional limitations. Unacceptable appearance is the most common reason why patients or parents request corrective osteotomy. O'Driscoll SW, Spinner RJ, McKee MD, et al: Tardy posterolateral rotatory instability of the elbow due to cubitus varus. J Bone Joint Surg Am 2001;83:1358-1369. Gurkan I, Bayrakci K, Tasbas B, et al: Posterior instability of the shoulder after supracondylar fractures recovered with cubitus varus deformity. J Pediatr Orthop 2002;22:198-202.
