HY 2026
00:00
Start Quiz
Question 801
High Yield
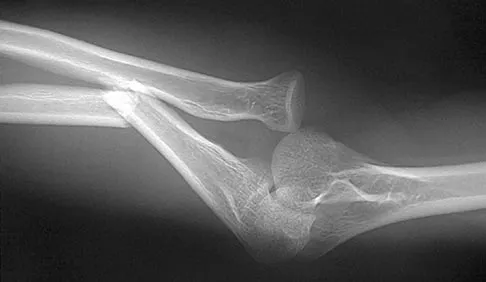
Figures 34a and 34b show the radiographs of a 28-year-old man who fell on his outstretched arm with significant force while mountain biking. The nerve deficit most likely to occur would result in weakness of

Explanation
The patient has a Monteggia fracture-dislocation (proximal ulnar fracture and radial head dislocation). The posterior interosseous nerve branch of the radial nerve is the most likely to be injured and could result in weakness of thumb extension and finger metacarpal extension. Considerably less likely are injuries to the more proximal radial nerve branches supplying the extensor carpi radialis longus and brevis, resulting in weak wrist extension; the ulnar nerve supplying the digital intrinsics, resulting in weak finger abduction; the anterior interosseous branch of the median nerve, resulting in weakness of the flexor pollicis longus; and the distal median nerve, resulting in weakness of thumb opposition. Bado JL: The Monteggia lesion. Clin Orthop 1967;50:71-86.
Question 802
High Yield
A 100-lb 9-year-old boy has a closed midshaft transverse femoral fracture. The oblique fracture is shortened by 3 cm with a 10-degree varus angulation. Surgical management consists of intramedullary, retrograde flexible titanium nailing. To optimize fracture stability, the surgeon should
Explanation
The technique of intramedullary nailing with titanium elastic nails is based on the concept of balanced forces across the fracture site with two equally sized nails. Implantation of the largest sized nails possible, with two equally sized nails, maximizes the stiffness at the fracture site, thereby optimizing fracture alignment and stability. Impacting the nails into the medullary canal can impact the fixation by minimizing distal purchase of the nail at the cortical insertion site. Closed reduction commonly permits bony reduction and passage of the nails; open reduction is reserved for inability to align the fracture. Luhmann SJ, Schootman M, Schoenecker PL, et al: Complications of titanium elastic nails for pediatric femur fractures. J Pediatr Orthop 2003;23:443-447. Lascombes P, Haumont T, Journeau P: Use and abuse of flexible intramedullary nailing in children and adolescents. J Pediatr Orthop 2006;26:827-834.
Question 803
High Yield
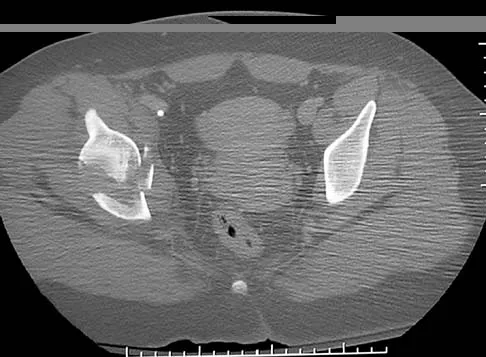
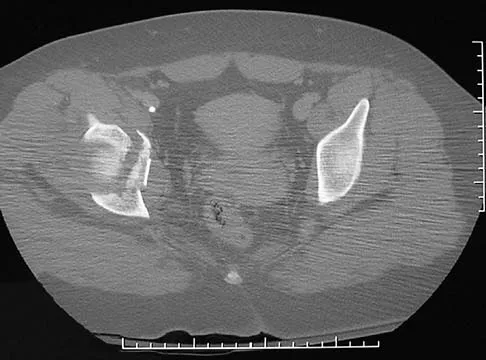
A 22-year-old right hand-dominant man who fell off his motorcycle onto the tip of his right shoulder 2 weeks ago now reports pain and difficulty raising his right arm. Examination reveals tenderness and gross movement over the lateral scapular spine and severe weakness during resisted abduction. A radiograph and 3D-CT scan are shown in Figures 24a and 24b. What is the next most appropriate step in management?


Explanation
The patient has a displaced scapular spine fracture that has resulted in shoulder weakness from a poor deltoid lever arm. The downward tilt may lead to subacromial impingement and rotator cuff dysfunction. Open reduction and internal fixation would best allow normal deltoid and shoulder function. Bone stimulators and abduction bracing may lead to healing but in a malunited position. Arthroscopic acromioplasty and fragment excision should be avoided. Ogawa K, Naniwa T: Fractures of the acromion and the lateral scapular spine. J Shoulder Elbow Surg 1997;6:544-548.
Question 804
High Yield
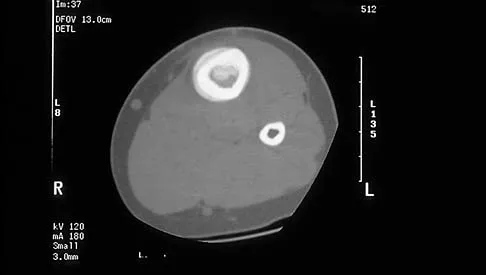
A 46-year-old man has acute tenderness along the ulnar aspect of the wrist after falling on his outstretched hand while playing basketball. Examination reveals tenderness and mild swelling along the volar ulnar aspect of the wrist. Radiogaphs are shown in Figures 14a through 14c. Management should consist of



Explanation
The PA view of the wrist shows a pisiform fracture. Pisiform fractures constitute 1% to 3% of all carpal bone fractures. This fracture can be further evaluated with a carpal tunnel view or a supination oblique view of the wrist. Initial management should consist of immobilization with a short arm cast. If nonsurgical measures fail, bony excision is warranted. Failla JM, Amadio PC: Recognition and treatment of uncommon carpal fractures. Hand Clin 1988;4:469-476.
Question 805
High Yield
Venous thrombolembolism is a common complication following total hip and total knee arthroplasty; therefore, prophylaxis is deemed efficacious. Several studies on low-molecular-weight heparin (LMWH) have shown which of the following findings?
Explanation
Prophylactic LMWH is associated with a risk of bleeding complications, especially if administered too soon after surgery. The risk of major bleeding is 0.3% for control, 0.4% for aspirin, 1.3% for warfarin, 1.8% for LMWH, and 2.6% for unfractionated heparin. Colwell and associates conducted a prospective, randomized trial on over 1,500 total hip arthroplasty patients. Overall, the risk of clinically apparent venous thrombolembolism was 3.6% for LMWH and 3.7% for warfarin. LMWH acts in several sites of the coagulation cascade, with its principal action being inhibition of factor 10a. Thrombocytopenia is less common with LMWH than with unfractionated heparin. The use of LMWH is a relative contraindication with indwelling epidural anesthesia. Colwell CW Jr, Collis DK, Paulson R, et al: Comparison of enoxaparin and warfarin for the prevention of venous thromboembolic disease after total hip arthroplasty:. Evaluation during hospitalization and three months after discharge. J Bone Joint Surg Am 1999;81:932-940.
Question 806
High Yield
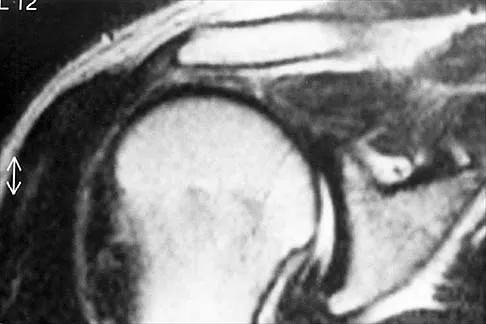
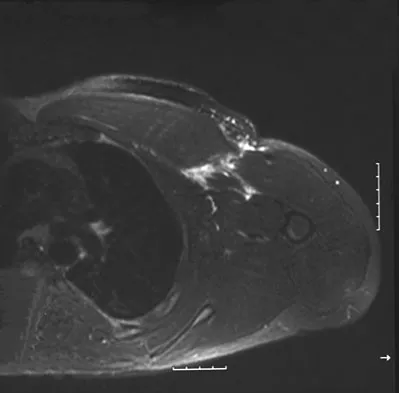
Figures 49a and 49b show MRI scans of the shoulder. What is the most likely diagnosis?

Explanation
The supraspinatus tendon shows clear detachment and retraction from its greater tuberosity attachment by the absence of the normal dark subacromial signal extending to the attachment on the greater tuberosity. There is no anterior inferior glenoid labral detachment that usually is seen in a Bankart lesion. The acromioclavicular joint shows no evidence of separation. The humeral head is migrated cranially, indicating a chronic rotator cuff tear. Iannotti JP, Zlatkin MB, Esterhai JL, Kressel HY, Dalinka MK, Spindler KP: Magnetic resonance imaging of the shoulder: Sensitivity, specificity, and predictive value. J Bone Joint Surg Am 1991;73:17-29. Seeger LL, Gold RH, Bassett LW, Ellman H: Shoulder impingement syndrome: MR findings in 53 shoulders. Am J Roentgenol 1988;150:343-347.
Question 807
High Yield
Of the following clinical situations, which is most likely to lead to osteonecrosis associated with a slipped capital femoral epiphysis (SCFE)?

Explanation
Osteonecrosis of the femoral head is the most devastating complication of SCFE. There is a 47% incidence of ischemic necrosis associated with an unstable SCFE. By definition, the patient with an unstable SCFE is unable to bear weight even with crutches. Osteonecrosis is most likely associated with the initial femoral head displacement rather than the result of either tamponade from hemarthrosis or from gentle repositioning prior to stabilization. Age, sex, and obesity are not risk factors for osteonecrosis. Loder RT, Richards BS, Shapiro PS, et al: Acute slipped capital femoral epiphysis: The importance of physeal stability. J Bone Joint Surg Am 1993;75:1134-1140.
Question 808
High Yield
What is the most common complication associated with scalene regional anesthesia for shoulder procedures?
Explanation
Failure of the scalene block, necessitating general anesthesia or the immediate administration of narcotic medications, is the most common complication, occurring in 3% to 18% of patients. Cardiac arrest or cardiovascular collapse has been reported in anecdotal occurrences. Seizure that is the result of intravascular injection of local anesthetic is a rare complication, with an incidence reported of 0% to 6%. Neurologic complications, including laryngeal and phrenic nerve injuries, are rare although parathesias lasting up to 2 weeks have been reported in up to 3% of patients. Weber SC, Jain R: Scalene regional anesthesia for shoulder surgery in a community setting: An assessment of risk. J Bone Joint Surg Am 2002;84:775-779.
Question 809
High Yield
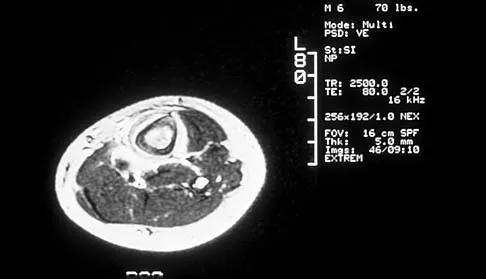
Figures 45a and 45b show the radiographs of a 46-year-old man who reports the acute onset of right knee pain and is unable to bear weight on the extremity. His medical history is unremarkable. The next most appropriate step in management should consist of


Explanation
The patient has a pathologic fracture of the right distal femur; therefore, given the patient's age, the most likely diagnosis is metastatic carcinoma. Staging studies should be obtained prior to surgical treatment. Immediate intramedullary fixation is contraindicated before a diagnosis is made by biopsy. Surgical stabilization should be performed prior to radiation therapy.
Question 810
High Yield
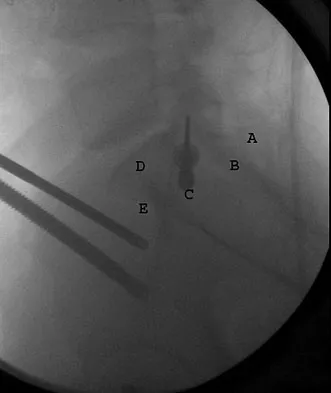
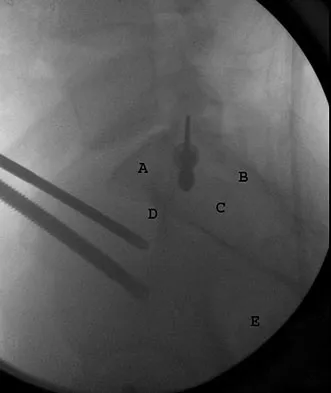
What letter in Figure 33 marks the correct starting point for a transiliac pelvic screw?
Explanation
Iliosacral screws cannot always be placed safely due to variations in pelvic anatomy. Transiliac bars are an alternative method for fixation but are placed using an open technique. A screw can be placed percutaneously through both iliac wings posterior to the posterior border of the sacrum. The starting point is visualized using a lateral C arm shot and is located on the posterior iliac crest at about the level of the S1 body where the crest has its largest area posterior to the sacrum. This area is labeled A in the figure, B represents the sacral canal, C is S1, D is the area cephalad to the iliocortical density, and E is the anterior border of the sacrum. The radiograph demonstrates a well-placed sacroiliac screw. Moed BR, Fissel BA, Jasey G: Percutaneous transiliac pelvic fracture fixation: Cadaver feasibility study and preliminary clinical results. J Trauma 2007;62:357-364.
Question 811
High Yield
A 25-year-old student sustains the injury shown in Figures 13a through 13c after falling off a curb. Initial management should consist of



Explanation
The radiographs reveal a fracture entering the 4-5 intermetatarsal articulation, consistent with a zone 2 injury. This classically is also referred to as a Jones fracture. The history and radiographic findings indicate this is an acute fracture, which guides management. A zone 1 fracture enters the fifth tarsometatarsal joint, and a zone 3 fracture is a proximal diaphyseal fracture distal to the 4-5 articulation. Initial management is usually nonsurgical and consists of non-weight-bearing in a short leg cast. This method has been shown to result in a better healing rate compared to weight bearing as tolerated. Rosenberg GA, Sterra JJ: Treatment strategies for acute fractures and nonunions of the proximal fifth metatarsal. J Am Acad Orthop Surg 2000;8:332-338.
Question 812
High Yield
A 35-year-old man has had a mass on the bottom of his foot for the past 6 months. He reports that initially the mass was exquisitely painful but now is minimally tender. Examination reveals a 2.5- x 2.0-cm firm, noncompressible, nonmobile mass contiguous with the plantar fascia in the distal arch. The mass is particularly prominent with passive dorsiflexion of the ankle and toes. What is the best course of action?
Explanation
The history is most consistent with a plantar fibroma. The nodules typically are located within the substance of the plantar aponeurosis. The clinical appearance is usually diagnostic without the need for advanced imaging studies. While the lesion may be prominent and painful to direct palpation, the anatomic location is usually off of the weight-bearing surface. Observation with or without an accommodative orthotic is the treatment of choice. Recurrence is common following attempted excision. Sammarco GJ, Mangone PG: Classification and treatment of plantar fibromatosis. Foot Ankle Int 2000;21:563-569.
Question 813
High Yield
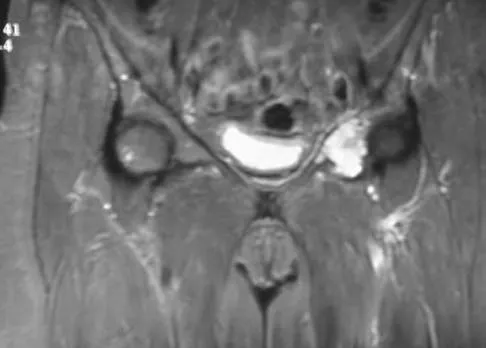
A 10-year-old boy who has had progressive low back and right buttock pain for the past 3 days is now unable to bear weight on the right side secondary to pain. He has a temperature of 101.3 degrees F (38.5 degrees C). Examination reveals full hip range of motion; but he reports pain on the right side with external rotation. Pain is elicited with compression of the iliac wings and with direct palpation of the right sacroiliac (SI) joint. An MRI scan of the pelvis shows no abscess, but there is inflammation of the SI joint. Management should consist of
Explanation
The clinical presentation and MRI findings are consistent with an acute infection of the SI joint. Bed rest and nonsteroidal anti-inflammatory drugs alone are insufficient to treat the problem. Staphylococcus aureus is the causative organism in most of these infections; therefore, unless there is an unusual factor in the history such as IV drug use, immune system compromise, or unusual travel, SI joint aspiration is unnecessary. It is often difficult to enter the SI joint, even under radiographic guidance. Management should consist of hospital admission and IV antibiotics. Blood cultures may be positive and should be obtained prior to starting antibiotics. Surgical fusion of the SI joint is not indicated. Morrissey RT: Bone and Joint Sepsis in Pediatric Orthopaedics. Philadelphia, PA, JB Lippincott, 1990. Beaupre A, Carroll N: The three syndromes of iliac osteomyelitis in children. J Bone Joint Surg Am 1979;61:1087-1092.
Question 814
High Yield
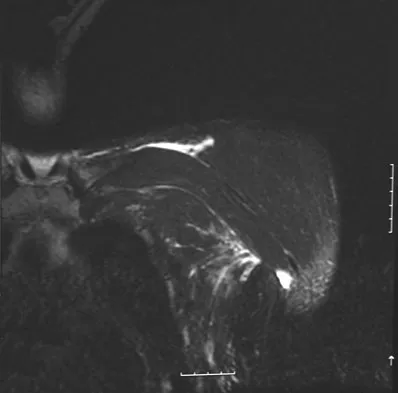
A 38-year-old left hand-dominant bodybuilder reports ecchymosis in the left axilla and anterior brachium after sustaining an injury while bench pressing 3 weeks ago. Coronal and axial MRI scans are shown in Figures 16a and 16b. What treatment method yields the best long-term results?
Explanation
The MRI scans show a rupture of the sternocostal portion of the pectoralis major tendon. This is the most common site of rupture and bench pressing is the most common etiology. Surgical repair yields better functional outcomes and patient satisfaction for tears not only at the tendon/bone interface but also at the myotendinous junction. Bak K, Cameron EA, Henderson IJ: Rupture of the pectoralis major: A meta-analysis of 112 cases. Knee Surg Sports Traumatol Arthrosc 2000;8:113-119.
Question 815
High Yield
Radiographs of a pediatric patient reveal a suspected osteosarcoma of the distal femur. Additional staging studies should consist of
Explanation
CT of the abdomen and pelvis is not part of the staging of osteosarcoma. Staging studies should consist of CT of the chest, radiographs of the chest and primary tumor, MRI of the primary tumor, and a bone scan. The MRI should be obtained prior to the biopsy.
Question 816
High Yield
Mechanical reduction of the pain associated with the condition shown in Figure 6 can be accomplished through the use of a cane on the contralateral side. Similarly, if this patient must carry any type of load in his or her arms, it should be carried

Explanation
Patients with diseased hips often must carry objects while walking, yet they are rarely instructed on which hand to use. The patient should be directed to carry the object on the ipsilateral side, just the opposite of the side he or she would use a cane. The cane pushes up on the weight of the body so that when the patient is carrying a load, the weight in the hand on the same side as the hip pushes up on the weight of the body, but now the patient has the fulcrum of the hip in between. Tan and associates mathematically determined the hip forces that result when a load is carried in the ipsilateral hand versus the contralateral hand. Using a free-body diagram of a single-leg supported stance, they found that when a load was carried in the contralateral hand, the resultant forces on the hip were increased considerably. Conversely, when the weight was carried in the ipsilateral hand, the forces were actually lower than when no weight was carried at all. Therefore, carrying a weight on the opposite side resulted in hip forces that were substantially greater than when the weight was carried on the same side.
Question 817
High Yield
Tension force in the anterior cruciate ligament during passive range of motion is highest at
Explanation
Tension forces in the healthy, as well as the reconstructed, anterior cruciate ligament were measured and found to be highest with the knee in full extension and decreased as the flexion increased. Markolf KL, Burchfield DM, Shapiro MM, et al: Biomechanical consequences of replacement of the anterior cruciate ligament with a patellar ligament allograft. Part II: Forces in the graft compared with forces in the intact ligament. J Bone Joint Surg Am 1996;78:1728-1734.
Question 818
High Yield
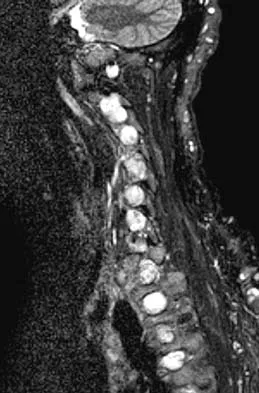
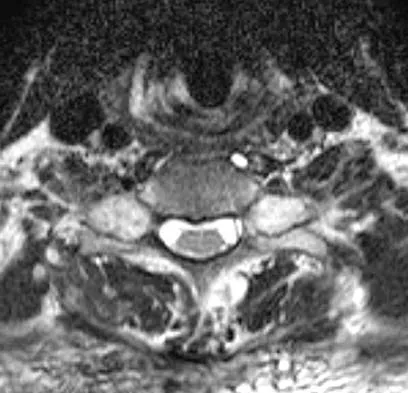
A 65-year-old man with ankylosing spondylitis sustains an extension injury to his cervical spine. Two days later, a progressive neurologic deficit develops at the C6 level. An MRI scan is shown in Figure 1. What is the most likely diagnosis?

Explanation
It is common for patients with ankylosing spondylitis to sustain extension-type fractures, typically near the cervicothoracic junction. These fractures can be minimally displaced, making them difficult to diagnose. In addition, the vertebral bodies are vascular and their canals are relatively enclosed, making them vulnerable to epidural bleeding. The MRI scan shows an epidural hematoma posteriorly compressing the cord. Bohlman HH: Acute fractures and dislocations of the cervical spine. J Bone Joint Surg Am 1979;61:1119-1142. Weinstein PR, Karpman RR, Gall EP, et al: Spinal cord injury, spine fracture and spinal stenosis in ankylosing spondylitis. J Neurosurg 1982;57:609-616.
Question 819
High Yield
Figure 19 shows the current radiograph of a 48-year-old man who reports hip pain and marked difficulty walking after undergoing revision of a failed total hip replacement 2 years ago. What is the mechanism of failure?

Explanation
Fatigue from repetitive loading of the stem with the distal aspect well-fixed resulted in stem failure. If the stem had loosened, it would not have broken. Crevice corrosion occurs at a taper interface; galvanic corrosion occurs at the junction of two metals of differing electrochemical potentials, not along a uniform portion of the implant. Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 449-486.
Question 820
High Yield
Figure 7 shows the radiograph of a 64-year-old man who has neck pain and weakness of the upper and lower extremities following a motor vehicle accident. Examination reveals 3/5 quadriceps and 4/5 hip flexors but no ankle dorsiflexion or plantar flexion. His intrinsics are 1/5, with finger flexors of 3/5. He is awake, alert, and cooperative. Management should consist of

Explanation
In patients with facet dislocations and an incomplete neurologic deficit, early decompression of the canal via reduction of the dislocation generally is considered safe if the patient is alert and can cooperate. However, patients who cannot cooperate with serial neurologic examinations during the reduction are at risk for increased deficit secondary to herniated nucleus pulposus, and MRI should be performed prior to either closed or open reduction. Star AM, Jones AA, Cotler JM, et al: Immediate closed reduction of cervical spine dislocations using traction. Spine 1990;15:1068-1072.
Question 821
High Yield
The arrow in the axial T1-weighted MRI scan shown in Figure 18 is pointing to which of the following structures?

Explanation
The arrow is pointing to the ulnar nerve within Guyon's canal. Guyon's canal is approximately 4 cm long, beginning at the proximal extent of the transverse carpal ligament and ending at the aponeurotic arch of the hypothenar muscles. Many structures comprise the boundaries of Guyon's canal. The floor, for example, consists of the transverse carpal ligament, the pisohamate and pisometacarpal ligaments, and the opponens digiti minimi. Within Guyon's canal, the ulnar nerve bifurcates into the superficial and deep branches, with the deep branch of the ulnar nerve persisting distal to the canal. The ulnar artery is immediately adjacent and radial to the ulnar nerve. The median nerve is visualized within the carpal tunnel. The radial artery is on the radial side of the wrist. The hook of the hamate is clearly seen in the figure, orienting the observer to the ulnar side of the wrist. Goss MS, Gelberman RH: The anatomy of the distal ulnar tunnel. Clin Orthop 1985;196:238-247.
Question 822
High Yield
A 35-year-old man is seen in the emergency department with a bullet wound to the foot that occurred 2 hours ago. Examination reveals a 0.5-cm entrance wound on the dorsum of the foot and a 1.5-cm exit wound on the plantar aspect. Exploration of the plantar wound in the emergency department reveals bone and metal fragments. Radiographs reveal a comminuted, unstable fracture of the base of the first metatarsal and cuneiform. Management should consist of tetanus toxoid, and
Explanation
The patient sustained a type I unstable fracture that requires debridement of superficial fragments from the sole and surgical stabilization. Low-velocity wounds less than 8 hours old are considered type I open fractures. In contrast, gunshot wounds with associated fractures more than 8 hours old are considered type II open fractures using the Gustilo and Anderson classification. Gustilo type I stable fractures due to gunshot wounds and seen within 8 hours can be treated with tetanus toxoid (if no history of immunization or booster within 5 years), surface irrigation, and casting or a hard sole shoe. Antibiotics are not required unless gross contamination is present. However, if the extent of contamination is unclear, or if a joint is penetrated, then routine antibiotic prophylaxis is recommended. Indications for surgery include: articular involvement, unstable fractures, presentation 8 or more hours after injury, tendon involvement, and superficial fragments in the palm or sole. Type I unstable fractures may be stabilized with internal or external fixation. Type II unstable fractures should be treated with external fixation and repeat debridements until clean. Holmes GB Jr: Gunshot wounds of the foot. Clin Orthop Relat Res 2003;408:86-91.
Question 823
High Yield
A 72-year-old man was involved in an automobile accident 4 weeks ago. Initially he noted pain about his nondominant left shoulder, which resolved within a few weeks after the accident. He now describes trouble with gripping and carrying items in his left hand. Radiographs are shown in Figures 20a through 20c. His signs and symptoms are the result of injury to which of the following ligaments?



Explanation
The radiographs reveal a gap between the scaphoid and lunate bones, indicative of disruption of the scapholunate ligament complex. The three components of the complex are the dorsal scapholunate ligament, the volar (or palmar) scapholunate ligament, and the proximal fibrocartilaginous membrane, listed in decreasing yield strength. Disruption of the stout dorsal interosseous ligament is required for scapholunate dissociation to occur. Berger RA: The ligaments of the wrist: A current overview of anatomy with considerations of their potential functions. Hand Clin 1997;13:63-82.
Question 824
High Yield
Which of the following orthotic features best reduces pain in patients with hallux rigidus?
Explanation
Nonsurgical care for hallux rigidus involves limiting the motion of the first metatarsophalangeal joint during toe-off and ensuring that there is a deep enough toe box to accommodate dorsal osteophytes. A rigid shank or forefoot rocker both help to reduce the forces of extension during toe-off. Beskin JL: Hallux rigidus. Foot Ankle Clin 1999;4:335-353.
Question 825
High Yield
A 35-year-old woman reports an 8-week history of neck pain radiating to her right upper extremity. She denies any history of trauma or provocative event. Examination reveals decreased pinprick sensation in her right middle finger, otherwise sensation is intact bilaterally. Finger flexors and interossei demonstrate 5/5 motor strength bilaterally. Finger extensors are 4/5 on the right and 5/5 on the left. The triceps reflex is 1+ on the right and 2+ on the left. The most likely diagnosis is a herniated nucleus pulposus at what level?
Explanation
The patient's neurologic examination is consistent with a C7 radiculopathy on the right side. In a patient with this symptom complex in the absence of trauma, a cervical disk herniation is the most common etiology for a C7 radiculopathy. There are eight cervical nerve roots and the C7 nerve exits at the C6-7 disk space and is most frequently impinged by a disk herniation at this level. Houten JK, Errico TJ: Cervical spondylotic myelopathy and radiculopathy: Natural history and clinical presentation, in Clark CR (ed): The Cervical Spine, ed 4. Philadelphia, PA, Lippincott Williams & Wilkins, 2005, pp 985-990.
Question 826
High Yield
Figure 3 shows the radiograph of an asymptomatic 10-year-old boy. Management should consist of

Explanation
Asymptomatic spondylolysis in a child or adolescent should be observed for the possible development of spondylolisthesis, but no other active intervention is needed. The initial treatment of choice for symptomatic spondylolysis includes rest and activity modifications, nonsteroidal anti-inflammatory drugs, physical therapy, bracing, and casting. Immobilization with a TLSO or pantaloon spica cast may permit healing of an acute pars fracture. Rarely, surgical treatment may be necessary. Surgical options include posterolateral L5-S1 fusion or direct repair of the pars defect. Pizzutillo PD, Hummer CD III: Nonoperative treatment for painful adolescent spondylolysis or spondylolisthesis. J Pediatr Orthop 1989;9:538-540.
Question 827
High Yield
What is the most frequent location of entrapment of the deep peroneal nerve?
Explanation
The most frequently described entrapment of the deep peroneal nerve is the anterior tarsal tunnel syndrome. This syndrome refers to entrapment of the deep peroneal nerve under the inferior extensor retinaculum. Entrapment can also occur as the nerve passes under the tendon of the extensor hallucis brevis. Compression by underlying dorsal osteophytes of the talonavicular joint and an os intermetatarseum (between the bases of the first and second metatarsals) have previously been described in runners. Kopell HP, Thompson WA: Peripheral entrapment neuropathies of the lower extremity. N Engl J Med 1960;262:56-60.
Question 828
High Yield
A young man sustains a lumbar strain in an on-the-job motor vehicle accident. Both he and his treating physician feel that he is capable of limited duty with appropriate restrictions shortly after the injury. What term best describes his work status?
Explanation
Because the man is only recently removed from his injury and is judged capable of returning to work with some restrictions, the term that best describes his work status is temporary partial disability.
Question 829
High Yield
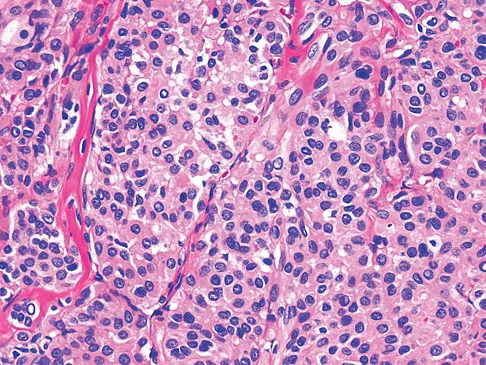
A 23-year-old woman reports right knee pain and fullness. The pain is worse with activity but also present at rest. Radiographs are shown in Figures 20a and 20b. What is the most likely diagnosis?


Explanation
The radiographs reveal a predominantly lytic, destructive lesion of the distal femur, although there is a hint of some blastic change as well. The lesion has violated the cortex, and there is mineralization outside the cortex laterally. The lateral radiograph suggests a soft-tissue density. These aggressive changes on radiographs in this age group are strongly suggestive of osteosarcoma. Sanders TG, Parsons TW: Radiographic imaging of musculoskeletal neoplasia. Cancer Control 2001;8:221-231.
Question 830
High Yield
A 35-year-old recreational basketball player reports shoulder pain following a sprawl for a rebound. While examination reveals that he can actively elevate the arm with pain, a subacromial injection fails to provide relief. An MRI scan reveals medial subluxation of the long head of the biceps. Which of the following structures most likely has also been injured?
Explanation
Subscapularis tears can be associated with disruption of the transverse ligament supporting the biceps. The remaining aspects of the rotator cuff, superior labrum, and capsule can be intact with this injury. Petersson CJ: Spontaneous medial dislocation of the tendon of the long biceps brachii. Clin Orthop 1986;211:224-227.
Question 831
High Yield
What is the most prevalent adverse event associated with allogeneic blood transfusion?

Explanation
Clerical error leading to acute hemolysis and even death occurs in 1:12,000 to 1:50,000 transfusions. Bacterial contamination leading to sepsis/shock occurs in 1:1 million transfusions. HIV transmission is approximately 1:500,000 transfusions and hepatitis C is 1:103,000 transfusions. Anaphylactic reactions occur in 1:150,000 transfusions. Aubuchon JP, Birkmeyer JD, Busch MP: Safety of the blood supply in the United States: Opportunities and controversies. Ann Intern Med 1997;127:904-909.
Question 832
High Yield
A 14-year-old boy sustains a twisting injury to his right shoulder and recalls feeling a snap during a wrestling match. Examination shows hesitancy to raise the arm away from the side, diffuse tenderness and swelling of the upper arm, and no evidence of neurovascular compromise. Figures 6a and 6b show an AP radiograph and MRI scan. What is the most likely diagnosis?


Explanation
While difficult to appreciate on the AP radiograph of the shoulder, the increased physeal signal demonstrated on the axial MRI scan is consistent with a nondisplaced growth plate fracture. A comparison radiograph of the left shoulder also could be considered and the injured shoulder evaluated for physeal widening. Proximal humeral fractures in children are somewhat unusual, representing less than 1% of all fractures seen in children and only 3% to 6% of all epiphyseal fractures. Physeal injuries are classified according to the Salter-Harris classification scheme. Salter-Harris type I fractures represent approximately 25% of physeal injuries to the proximal humerus in adolescents. The proximal humeral physis is responsible for 80% of the longitudinal growth of the humerus; therefore, there is tremendous potential for remodeling of fractures in this region. Management for nondisplaced Salter-Harris type I fractures is limited to a short period of immobilization followed by a gradual return to activities as clinical symptoms resolve. Curtis RJ, Rockwood CA Jr: Fractures and dislocations of the shoulder in children, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, pp 991-1007.
Question 833
High Yield
A still active 86-year-old pastry chef falls in her kitchen and notes pain and deformity of her little finger. There are no open wounds. Radiographs are shown in Figures 49a and 49b. What is the most appropriate management?


Explanation
The fracture of the proximal phalanx is clearly displaced. There is slight comminution at the area of the fracture. Closed reduction is likely to fail due to the forces of the extensor, flexor, and intrinsic mechanisms. Percutaneous fixation, unlike open fixation techniques, avoids likely problems with stiffness. Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC, et al (eds): Green's Operative Hand Surgery, ed 5. Philadelphia, PA, Elsevier, 2005, p 281.
Question 834
High Yield
What tendon is closest to an appropriately placed anterolateral portal for ankle arthroscopy?

Explanation
The appropriate placement of the anterolateral portal provides access to the lateral gutter of the joint while avoiding the superficial peroneal nerve. The safest location for the portal is approximately 4 mm lateral to the peroneus tertius tendon, the closest of the tendons listed to the anterolateral portal. Because the superficial peroneal nerve location is variable, attempts to visualize, palpate, or transilluminate the nerve are mandatory.
Question 835
High Yield
A 35-year-old woman who underwent open reduction and internal fixation of a calcaneal fracture 14 months ago reports pain that has failed to respond to nonsurgical management. Examination reveals limited painful subtalar motion but no hindfoot deformity. A lateral radiograph is shown in Figure 6. Surgical reconstruction is best accomplished with

Explanation
The patient has posttraumatic subtalar joint arthrosis that developed following a calcaneal fracture. Because there is no hindfoot deformity, in situ subtalar joint arthrodesis is the treatment of choice. Calcaneal osteotomy or distraction bone block arthrodesis is beneficial in patients with severe talar dorsiflexion or malunion of the calcaneal body. Triple arthrodesis is not warranted without changes at the transverse tarsal joint, and typically even with injury into the calcaneocuboid joint, this joint is often asymptomatic. Pantalar arthrodesis is not indicated as the pathology is occurring at the subtalar joint and not in the ankle joint. Sanders R: Fractures and fracture-dislocations of the calcaneus, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1422-1464. Juliano TJ, Myerson MS: Fractures of the hindfoot, in Myerson MS (ed): Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 1297-1340.
Question 836
High Yield
A 35-year-old woman who is training for a triathlon has had a 2-month history of heel pain with weight bearing and is unable to run. History reveals that she is amenorrheic. Examination reveals that she is thin and has pain over the heel that is exacerbated with medial and lateral compression. Range of motion and motor and sensory function are normal. Radiographs are normal. What is the most likely diagnosis?
Explanation
The most likely diagnosis is a stress fracture of the calcaneus and is supported by the history of running, female gender, and amenorrhea. Reproducing pain with medial and lateral compression of the heel also supports the diagnosis. A bone scan or MRI would most likely confirm the diagnosis. Plantar fasciitis would result in pain on the bottom of the heel with point tenderness. The lack of other areas of involvement or other symptoms does not support a seronegative inflammatory arthritis. Tarsal tunnel syndrome and peripheral neuropathy are unlikely because of the normal neurologic examination. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 597-612.
Question 837
High Yield
A 16-year-old girl sustained the injury shown in Figure 7a. CT scans are shown in Figures 7b through 7d. The results of treatment of this injury have been shown to most correlate with which of the following factors?


Explanation
The patient has a very low T-type acetabular fracture; however, the head is not congruent under the dome so surgical reduction is necessary. The anterior and posterior columns are displaced and will move independent from each other. The extended iliofemoral is the only approach allowing for visualization and reduction of each column. A combined anterior and posterior approach may also be used. The timing of surgery should be within the first 3 weeks of injury to optimize chances of obtaining an accurate reduction because this is an important factor in determining outcome. Letournel E, Judet R (eds): Fractures of the Acetabulum, ed 2. Berlin, Germany, Springer-Verlag, 1991.
Question 838
High Yield
Figure 2 shows the AP radiograph of an 18-year-old woman with progressive and severe right hip pain. Nonsteroidal anti-inflammatory drugs no longer control her pain. What is the next most appropriate step in management?

Explanation
A concentric hip with acetabular dysplasia in a symptomatic patient is best treated by periacetabular osteotomy. The Salter osteotomy is less optimal because the method has limited correction, is uniaxial, cannot be tailored to the deformity, and lateralizes the entire hip joint, thereby increasing the joint reactive forces. Because the hyaline cartilage of the joint is histologically normal, rotating the hyaline cartilage into an optimal position is preferable to augmenting the acetabulum with a shelf or by Chiari osteotomy. Varus intertrochanteric osteotomy has no significant role in the treatment of acetabular dysplasia. Total hip arthroplasty may be required in the future but should not be the first choice.
Question 839
High Yield
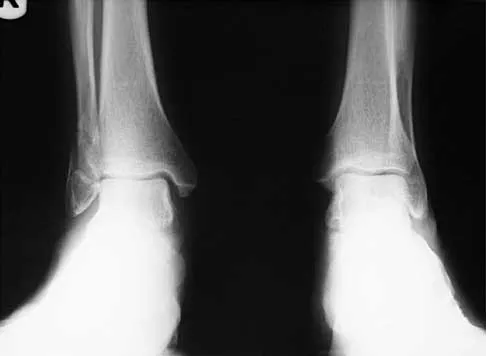
Figures 4a through 4c show the radiographs of a 43-year-old woman who sustained a twisting injury to her right ankle. She has ankle pain and tenderness medially and laterally. To help determine the optimal treatment, an external rotation stress radiograph of the ankle is obtained. This test is designed to evaluate the integrity of what structure?



Explanation
In the presence of a supination external rotation-type fracture of the distal fibula (Weber type B), stability of the ankle is best assessed by performing an external rotation stress AP view of the ankle. This test is used to assess the integrity of the deltoid ligament. The presence of a deltoid ligament rupture results in instability and generally is best managed surgically. The gravity stress test can also be used. Egol KA, Amirtharajah M, Tejwani NC, et al: Ankle stress test for predicting the need for surgical fixation of isolated fibular fractures. J Bone Joint Surg Am 2004;86:2393-2398. McConnell T, Creevy W, Tornetta P III: Stress examination of supination external rotation-type fibular fractures. J Bone Joint Surg Am 2004;86:2171-2178.
Question 840
High Yield
What is the primary indication for performing a total wrist arthroplasty in a patient with painful rheumatoid arthritis?
Explanation
The most conservative indications for a total wrist arthroplasty are to spare motion on one side and to improve activities of daily living. Component loosening, dislocation, and wound problems are frequent. Suitable patients can be of various ages, wrist motion, and radiographic stages of arthritis. Ipsilateral total elbow arthroplasty, type III degenerative changes of the wrist, age older than 55, and limited range of motion are neither primary indications nor contraindications to a total wrist arthroplasty. Divelbiss BJ, Sollerman C, Adams BD: Early results of the universal total wrist arthroplasty in rheumatoid arthritis. J Hand Surg Am 2002;27:195-204. Vicar AJ, Burton RI: Surgical management of rheumatoid wrist-fusion or arthroplasty. J Hand Surg Am 1986;11:790-797.
Question 841
High Yield
When performing an inside-out lateral meniscal repair, capsule exposure is provided by developing the

Explanation
Capsular exposure for an inside-out lateral meniscal repair is performed by developing the interval between the iliotibial band and biceps tendon. Posterior retraction of the biceps tendon exposes the lateral head of the gastrocnemius. Posterior retraction of the gastrocnemius provides access to the posterolateral capsule. Miller DB Jr: Arthroscopic meniscus repair. Am J Sports Med 1988;16:315-320.
Question 842
High Yield
Survival rates for children with soft-tissue sarcoma other than rhabdomyosarcoma are best correlated with
Explanation
In review of 154 patients with nonrhabdomyosarcoma, Rao reported that histologic grade, tumor invasiveness, and adequate surgical margin were the most important prognostic factors. Histologic subtype, use of adjuvant chemotherapy, and patient age were not as important. Size related to degree of invasiveness was not statistically significant. Rao BN: Nonrhabdomyosarcoma in children: Prognostic factors influencing survival. Semin Surg Oncol 1993;9:524-531. Andrassy R, et al: Non-rhabdomyosarcoma Soft-Tissue Sarcomas: Pediatric Surgical Oncology. Philadelphia, PA, WB Saunders, p 221.
Question 843
High Yield
A 6-year-old boy has leg pain. A radiograph, MRI, CT, and bone scans, and a biopsy specimen are shown in Figures 14a through 14e. What is the most likely diagnosis?


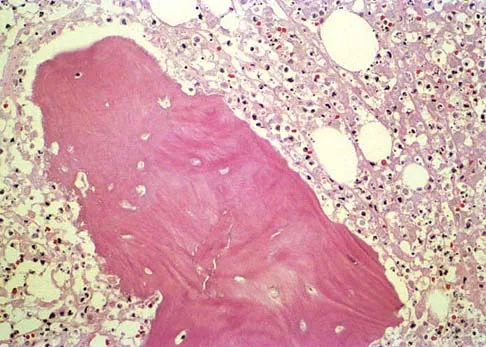
Explanation
From an imaging point of view, all of the diagnoses are possible. Biopsy results and cultures are necessary to make the diagnosis. The biopsy specimen shows inflammatory cells and necrotic bone, consistent with osteomyelitis. Fletcher BD, Hanna SL: Pediatric musculoskeletal lesions simulating neoplasms. Magn Reson Imaging Clin N Am 1996;4:721-747.
Question 844
High Yield
A 54-year-old man undergoes uneventful anterior cervical diskectomy and interbody fusion at C4-5 for focal disk herniation and C5 radiculopathy. At the 3-week follow-up examination, the patient reports a persistent cough. Pulmonary evaluation reveals a mild but persistent aspiration. Laryngoscopy reveals partial paralysis of the left vocal cord, most likely caused by
Explanation
The exact anatomic event responsible for vocal cord paralysis associated with anterior cervical surgery remains a question. Apfelbaum and associates, in an excellent review of 900 anterior cervical surgeries, identified 30 patients with vocal cord paralysis, 3 of which were permanent. They showed that retractors placed under the longus coli for anterior cervical exposures can compress the laryngeal-tracheal branches within the larynx against the tented endotracheal tube rather than the recurrent laryngeal nerve, which is extrinsic to the larynx. By releasing the endotracheal cuff and allowing the tube to recenter itself after placement of the retractors, they were able to decrease vocal cord injury from 6.4% to 1.7%. Jewett and associates suggested that a left-sided approach may result in a lower incidence of injury. Endotracheal intubation is the second most common cause of vocal cord injury, with an incidence of approximately 2%. Apfelbaum RI, Kriskovich MD, Haller JR: On the incidence, cause, and prevention of recurrent laryngeal nerve paralysis during anterior cervical spine surgery. Spine 2000;25:2906-2912.
Question 845
High Yield
A previously healthy 29-year-old man reports a 2-day history of severe atraumatic lower back pain. He denies any bowel or bladder difficulties and no constitutional signs. Examination is consistent with mechanical back pain. No focal neurologic deficits or pathologic reflexes are noted. What is the most appropriate management?
Explanation
In general, a previously healthy patient with an acute onset of nontraumatic lower back pain does not need diagnostic imaging before proceeding with therapeutic treatment. In the absence of any "red flags" during the history and physical examination, such as trauma or constitutional symptoms (ie, fevers, chills, weight loss), the appropriate treatment for acute onset lower back pain is purely symptomatic treatment including limited analgesics and early range of motion. Diagnostic imaging is not necessary unless the initial treatment is unsuccessful and symptoms are prolonged. Miller and associates suggested that the use of radiographs can lead to better patient satisfaction but not necessarily better outcomes. Miller P, Kendrick D, Bentley E, et al: Cost effectiveness of lumbar spine radiographs in primary care patients with low back pain. Spine 2002;27:2291-2297.
Question 846
High Yield
What is the most common pediatric soft-tissue sarcoma?

Explanation
Soft-tissue sarcomas are the sixth most common cancer in children. Rhabdomyosarcoma is the most common type of pediatric soft-tissue sarcoma. Nearly 50% of rhabdomyosarcomas are diagnosed in children who are age 5 years or younger. Unfortunately, there has not been a significant increase in survival in children with metastatic rhabdomyosarcoma despite aggressive therapy including multiple-drug chemotherapy regimens.
Question 847
High Yield
A 42-year-old woman has a history of nontraumatic ankle swelling with tenderness over the Achilles tendon and plantar fascia. She reports that while vacationing in Connecticut 2 months ago she noted the presence of a "red bull's eye" rash. Management should consist of
Explanation
The most likely diagnosis is Lyme disease because of the patient's recent vacation in an area with a high risk of exposure. The most effective treatment is doxycycline. Neu HC: A perspective on therapy of Lyme infection. Ann NY Acad Sci 1988;539:314-316.
Question 848
High Yield
A 7-year-old boy is seen in the emergency department with an isolated and displaced supracondylar humerus fracture and absent radial and ulnar pulses. Despite a moderately painful attempt at realignment, examination reveals that his hand remains pulseless. What is the next most appropriate step in management?
Explanation
Displaced supracondylar humerus fractures in children may have associated vascular compromise. Decreased blood flow may be due to vessel injury, entrapment within the fracture site, kinking from fracture displacement, or from vessel spasm. Optimal initial treatment in the emergency department includes gentle realignment of the limb and vascular assessment. Angiography is not required in isolated injuries as the level of the vessel compromise is always at the site of the fracture. When blood flow is not restored, the next best step in treatment is to proceed urgently to the operating room. A formal closed reduction and pinning is performed, and then the vascular status is reassessed. Exploration and vascular repair is required if the hand is cool, white, and without pulses. Ay S, Akinci M, Kamiloglu S, et al: Open reduction of displaced pediatric supracondylar humeral fractures through the anterior cubital approach. J Pediatr Orthop 2005;25:149-153. Sabharwal S, Tredwell SJ, Beauchamp RD, et al: Management of pulseless pink hand in pediatric supracondylar fractures of humerus. J Pediatr Orthop 1997;17:303-310.
Question 849
High Yield
What is the most anatomic location for placement of the femoral tunnel in anterior cruciate ligament reconstruction?

Explanation
It is critical for graft isometry and knee stability that the femoral tunnel be placed as far posterior as possible on the lateral femoral condyle. Superiorly, the graft should be at the one o'clock position on the left knee. Resident's ridge is a false posterior shelf that often seems like the extreme posterior cortex. Abnormal tunnel placement results in a variety of complications, including an unstable knee, early graft failure, and joint stiffness. Johnson RJ, Beynnon BD, Nichols CE, Renstrom PA: The treatment of injuries of the anterior cruciate ligament. J Bone Joint Surg Am 1992;74:140-151.
Question 850
High Yield
Radiating pain associated with a posterolateral thoracic disk herniation typically follows what pattern?
Explanation
Although symptomatic thoracic disk herniations can affect more caudal structures, even to the point of paralysis, the pattern of radiating pain has been described as either following the dermatomal band around the chest or feeling to the patient as if the pain passes straight anteriorly to the chest wall.
Question 851
High Yield
A 13-year-old girl is diagnosed with a stage IIB osteosarcoma of the proximal tibia. Following neoadjuvant chemotherapy, local control should consist of
Explanation
Local control of osteosarcoma consists of wide resection and reconstruction. Radiation therapy is not recommended except in unresectable lesions or for palliation. Curettage and bone grafting result in intralesional resection with an unacceptable high rate of local recurrence. Chemotherapy alone is not adequate for local control. Simon M, Springfield D, et al: Osteogenic Sarcoma: Surgery for Bone and Soft Tissue. Philadelphia, PA, Lippincott Raven, 1998, p 274.
Question 852
High Yield
Which of the following is a recognized consequence of hip fusion?

Explanation
Low back pain is an expected long-term complication of fusion; ipsilateral knee laxity is frequently encountered, as is degeneration of the contralateral hip. Hip fusion is equally valuable for both men and women, with both genders reporting satisfactory sexual function. Female patients often deliver by elective Cesarean section, although vaginal deliveries are reported. Liechti R (ed): Hip Arthrodesis and Associated Problems. Berlin, Germany, Springer-Verlag, 1978, pp 109-117.
Question 853
High Yield
Which of the following treatments of polyethylene results in the highest amount of oxidative degradation?
Explanation
Oxidative degradation of polyethylene occurs as a function of time in an air environment. In an environment such as argon, nitrogen, or a vacuum, the process is reduced. Ethylene oxide is an alternative for sterilization in which the cross-link degradation is minimized because of the absence of oxidative interactions. Gamma sterilization or use of ethylene oxide gas is the industry standard; however, oxygen concentrations are now reduced to a minimal level to retard the oxidation phenomenon. Sanford WM, Saum KA: Accelerated oxidative aging testing of UHMWPE. Trans Orthop Res Soc 1995;20:119. Sun DC, Schmidig G. Stark C, et al: On the origins of a subsurface oxidation maximum and its relationship to the performance of UHMWPE implants. Trans Soc Biomater 1995;18:362. Callaghan JJ, Dennis DA, Paprosky WA, Rosenberg AG (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 35-41.
Question 854
High Yield
A 3-year-old boy has a rigid 40-degree lumbar scoliosis that is the result of a fully segmented L5 hemivertebra. All other examination findings are normal. Management should consist of

Explanation
Near complete correction and rebalancing of the spine can be achieved by hemivertebral resection that may be done as either a simultaneous or a staged procedure in the young patient. This eliminates the problem of future progression and possible development of compensatory curves. Nonsurgical management is not indicated in congenital scoliosis. Convex hemiepiphyseodesis is best suited for patients younger than age 5 years who have a short curve caused by fully segmented hemivertebrae that correct to less than 40 degrees with the patient supine. Hemiepiphyseodesis and isolated posterior fusion are not indicated. Bradford DS, Boachie-Adjei O: One-stage anterior and posterior hemivertibral resection and arthrodesis for congenital scoliosis. J Bone Joint Surg Am 1990;72:536-540.
Question 855
High Yield
Figure 40 shows the plain radiograph of a 30-year-old woman who has had a long history of standing bilateral anterior knee pain and a sense of patellar instability without frank dislocation. Nonsurgical management consisting of anti-inflammatory drugs and physical therapy has failed to provide relief. Examination reveals full range of motion of both knees, with moderate patellofemoral crepitance. Patellar apprehension and patellar grind tests are positive. The Q-angle measures 20 degrees. Management should now consist of

Explanation
The history, physical examination, and radiographs indicate that the patellofemoral pain is most likely caused by excessive lateral patellar pressure and patellar maltracking. Because the radiographs reveal the lateral tilt of the patella and lateral subluxation, the treatment of choice is bilateral lateral releases with anteromedialization of the tibial tubercles. This procedure corrects not only the excessive lateral patellar pressure, but also the lateral subluxation. The use of patella-stabilizing braces or taping may provide temporary relief, but these implements are not well-tolerated and they will not change the underlying biomechanics of the knee. Simple lateral release is indicated for isolated lateral tilt, but it does not correct the lateral subluxation. The use of thermal capsular shrinkage for the medial retinaculum has not been proven to provide long-term correction of the deformity. Boden BP, Pearsall AW, Garrett We Jr, et al: Patellofemoral instability: Evaluation and management. J Am Acad Orthop Surg 1997;5:47-57.
Question 856
High Yield
A 32-year-old woman with systemic lupus erythematosus treated with methotrexate and oral corticosteroids reports right groin pain with ambulation and night pain. Examination reveals pain with internal and external rotation and flexion that is limited to 105 degrees because of discomfort. Laboratory studies show a serum WBC of 9.0/mm3 and an erythrocyte sedimentation rate of 35 mm/h. Figures 5a and 5b show AP and lateral radiographs of the right hip. Further evaluation should include


Explanation
The radiographs show Ficat and Arlet stage 2 osteonecrosis. The femoral head remains round, and there are sclerotic changes in the superolateral quadrant. Patients with systemic lupus erythematosus are at risk for osteonecrosis because of prednisone use and the underlying metabolic changes associated with the condition (hypofibrinolysis and thrombophilia). MRI is the best diagnostic method for detecting osteonecrosis, with a greater than 98% sensitivity and specificity. For this patient, an MRI can assess the contralateral hip for any involvement and can quantify the extent of the lesion. Mont MA, Jones LC, Sotereanos DG, Amstutz HC, Hungerford DS: Understanding and treating osteonecrosis of the femoral head. Instr Course Lect 2000;49:169-185.
Question 857
High Yield
A 14-year-old girl has had mild pain and nail deformity of the great toe for the past 4 months. A radiograph is shown in Figure 50. What is the most likely etiology of the lesion?

Explanation
The lesion is typical of a subungual exostosis, which is most often found on the medial aspect of the great toe in children and young adults. The diagnosis is confirmed on radiographs and usually requires excision for relief. Lokiec F, Ezra E, Krasin E, Keret D, Wientraub S: A simple and efficient surgical technique for subungual exostosis. J Pediatr Orthop 2001;21:76-79. Letts M, Davidson D, Nizalik E: Subungual exostosis: Diagnosis and treatment in children. J Trauma 1998;44:346-349.
Question 858
High Yield
A 25-year-old man reports wrist pain following a motorcycle accident. Examination reveals minimal swelling, slightly limited active range of motion, and point tenderness in the snuff box region. AP and oblique radiographs are shown in Figures 40a and 40b. Management should consist of


Explanation
The radiographs reveal a scaphoid fracture with displacement and comminution and an unstable fracture pattern. Treatment should consist of open reduction and internal fixation. In displaced scaphoid fractures and fractures with unstable fracture patterns, closed reduction is ineffective and is likely to lead to nonunion. Limited intercarpal fusion and proximal row carpectomy are used to correct a variety of traumatic and posttraumatic problems of the wrist. Amadio PC, Taleisnik J: Fractures of the carpal bone, in Green DP, Hotchkiss RN, Pederson WC (eds): Green's Operative Hand Surgery, ed 4. Philadelphia, PA, 1999, pp 809-823. Rettig ME, Kozin SH, Cooney WP: Open reduction and internal fixation of acute displaced scaphoid waist fractures. J Hand Surg Am 2001;26:271-276. Cooney WP, Dobyns JH, Linscheid RL: Fractures of the scaphoid: A rational approach to management. Clin Orthop 1980;149:90-97.
Question 859
High Yield
Baseball pitchers who have internal impingement will most likely demonstrate what changes in range of motion?

Explanation
Pitchers tend to have a decrease in internal rotation and an increase in external rotation. The increase in external rotation is felt to be multifactorial. An increase in humeral retroversion occurs from repeated throwing. This results in increased soft-tissue stretching and results in a posterior capsular contracture. Meister K, Buckley B, Batts J: The posterior impingement sign: Diagnosis of rotator cuff and posterior labral tears secondary to internal impingement in overhand athletes. Am J Orthop 2004;33:412-415.
Question 860
High Yield
Figures 3a and 3b show the MRI scans of a patient with neck pain. What is the most likely diagnosis?
Explanation
Muliple neurofibromas result in marked foraminal enlargement as seen on the sagittal MRI scan. Collagen disorders leading to dural ectasia may show similar enlargement, but none of these is listed as a possible answer. Kim HW, Weinstein SL: Spine update: The management of scoliosis in neurofibromatosis. Spine 1997;22:2770-2776.
Question 861
High Yield
A 37-year-old woman has had intermittent paresthesias and numbness in the plantar foot for the past 6 months. She reports that the symptoms are worse with activity, and the paresthesias are beginning to awaken her at night. MRI scans are shown in Figures 6a and 6b. What is the most likely diagnosis?
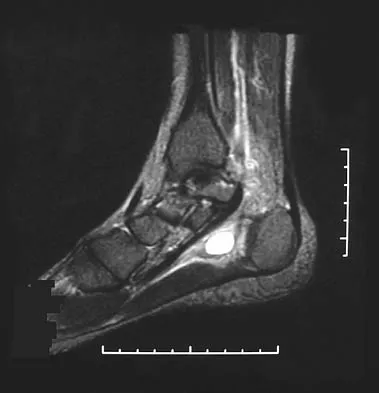
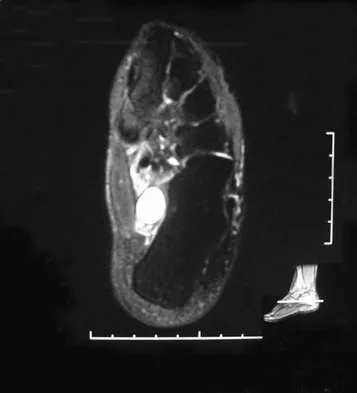
Explanation
The symptoms are consistent with tarsal tunnel syndrome. Ganglion cysts are a well-known cause of tarsal tunnel syndrome. The MRI scans show a high intensity, well-circumscribed mass in the tarsal tunnel that is consistent with a fluid-filled cyst. Patients usually respond well to excision of the ganglion and resolution of the tarsal tunnel symptoms. The surrounding fat is a different signal intensity on the MRI scans, which rules out a lipoma. Synovial cell sarcoma has a heterogeneous appearance on an MRI scan. Metastatic tumors are most commonly found in the osseous structures of the foot, not the soft tissues. Rozbruch SR, Chang V, Bohne WH, et al: Ganglion cysts of the lower extremity: An analysis of 54 cases and review of the literature. Orthopedics 1998;21:141-148. Llauger J, Palmer J, Monill JM, et al: MR imaging of benign soft-tissue masses of the foot and ankle. Radiographics 1998;18:1481-1498.
Question 862
High Yield
The 5-year outcome for patients with sciatica secondary to lumbar disk herniation shows which of the following results?
Explanation
Atlas and associates, in the Maine Lumbar Spine Study, reported that overall, patients treated initially with surgery reported better outcomes. By 5 years, 19% of surgical patients had undergone at least one additional lumbar spine operation, and 16% of nonsurgical patients had opted for at least one lumbar spine operation. At the 5-year follow-up, 70% of patients initially treated surgically reported improvement in their predominant symptom (back or leg pain) versus 56% of those initially treated nonsurgically. They also noted that there was no difference in the proportion of patients receiving disability compensation at the 5-year follow-up.
Question 863
High Yield
Figure 25 shows an arthroscopic thermal capsular shrinkage device being used in the anterior inferior quadrant of a patient with a subluxating shoulder. Which of the following neurologic complications is most frequently reported with this technique?

Explanation
The axillary nerve lies within millimeters of the anterior inferior capsule. The inferior capsule is of varying thickness, and thermal energy used in shortening the ligament can cause damage to the sensory fibers of the axillary nerve. Clinically, this is manifested as a burnt skin sensation in the axillary nerve distribution area. The motor branch of the axillary nerve is usually spared. The suprascapular nerve and the radial nerve are far from the shrinkage zone. The musculocutaneous nerve, frequently at risk with open procedures, lies well anterior. Fanton GS: Arthroscopic electrothermal surgery of the shoulder. Op Tech Sports Med 1998;6:157-160.
Question 864
High Yield
Figures 21a and 21b show the clinical photograph and radiograph of a 15-year-old girl who has a deformity of her feet. Her parents are concerned because there is a family history of Charcot-Marie-Tooth disease. The patient reports some mild instability of the ankle and has noticed mild early callosities; however, she is not having any significant pain. Coleman block testing reveals a forefoot valgus and supple hindfoot. She has weakness to eversion and dorsiflexion. Initial management should consist of


Explanation
Initial management of a young patient with a cavovarus deformity of the foot and a family history of Charcot-Marie-Tooth disease should focus on mobilization and strengthening of the weakening muscular units and an accommodative insert. Surgical intervention should be delayed until progression of the deformity begins to cause symptoms and/or weakness of the muscular units, resulting in contractures of the antagonistic muscle units. Pinzur MS: Charcot's foot. Foot Ankle Clin 2000;5:897-912. Holmes JR, Hansen ST Jr: Foot and ankle manifestations of Charcot-Marie-Tooth disease. Foot Ankle 1993;14:476-486.
Question 865
High Yield
A 55-year-old woman has slowly increasing pain at the distal end of her little finger that is exacerbated by cold temperatures. She denies any history of trauma to her hands and is employed as a school teacher. The histology of the resected specimen is shown in Figure 71. What is the most likely diagnosis?
Explanation
Glomus tumors are rare vascular lesions typically occurring about the nail of the distal phalanx of the hand. The diagnostic "triad" of glomus tumors consists of local pain, sensitivity to cold, and paroxysmal pain. They tend to present with pain as the most typical symptom and this can be exacerbated by changes in temperature that is felt to cause a vascular response within the lesion. The biopsy specimen confirms a glomus tumor showing the typical vascular spaces surrounded by glomus epithelioid glomus cells. Zook EG, Brown RE: The perionychium, in Green DP, Hotchkiss RN, Pederson WC (eds): Green's Operative Hand Surgery, ed 4. Philadelphia, PA, Churchill Livingstone, 1999, vol 2, pp 1353-1380.
Question 866
High Yield
A 10-year-old girl who is Risser stage 0 has back deformity associated with neurofibromatosis type 1 (NF1). She has no back pain. Examination shows multiple cafe-au-lait nevi with normal lower extremity neurologic function and reflexes. Standing radiographs of the spine show a short 50-degree right thoracic scoliosis with a kyphotic deformity of 55 degrees (apex T8). A 10-degree progression in scoliosis has occurred during the past 1 year. There is no cervical deformity. MRI shows mild dural ectasia, primarily in the upper lumbar region. Management should consist of

Explanation
Scoliotic deformities in patients with NF1 are often dysplastic with short, angular curves. Posterior arthrodesis is made more difficult by the presence of kyphosis and of weak posterior elements caused by dural ectasia. Combined anterior and posterior spinal arthrodesis is generally preferred for progressive dysplastic curves to maximize deformity correction and to decrease the risk of pseudarthrosis. Anterior fusion may also prevent crankshaft phenomenon in young children. Brace treatment is not effective for large, rigid, or dysplastic curves. Kim HW, Weinstein SL: Spine update: The management of scoliosis in neurofibromatosis. Spine 1997;22:2770-2776.
Question 867
High Yield
Pacinian corpuscles are lamellated nerve endings that are responsible for providing the perception of

Explanation
Pacinian corpuscles are nerve endings that provide the perception of pressure.
Question 868
High Yield
Figures 26a and 26b show the radiograph and MRI scan of an 18-year-old man who fell from a trampoline. Examination reveals exquisite local tenderness at the thoracolumbar junction, but he is neurologically intact. Management should consist of


Explanation
Based on the radiographic findings of marked disruption of the posterior ligamentous complex with a relatively small anterior bony fracture, the patient has a classic Chance-type ligamentous flexion-distraction injury. The pathology is mostly in soft tissues with limited healing potential. The treatment of choice is posterior reconstruction of the tension band with a short segment fusion with instrumentation. Casting or bracing may result in a painful kyphosis with ligamentous insufficiency. The anterior bony column is mostly intact, so anterior reconstruction is not necessary. Carl AL: Adult spine trauma, in DeWald RL (ed): Spinal Deformities: A Comprehensive Text. New York, NY, Thieme, 2003, pp 406-423.
Question 869
High Yield
A 57-year-old man has had right ankle pain for the past 10 months following an injury that went untreated. Radiographs are shown in Figures 30a through 30c. Management should consist of


Explanation
The radiographs reveal a malunited distal fibular fracture with shortening. Because there appears to be an adequate cartilage space within the ankle joint, the role of reconstruction would be to prevent arthrosis and the need for ankle arthrodesis, as well as to decrease symptoms. The treatment of choice is restoration of fibular length, alignment, and rotation with osteotomy plating, and bone grafting as needed. There is no indication for ligament reconstruction of a mechanically stable ankle, and tibial shortening osteotomy will not assist in correcting the deformity. Cast immobilization may assist with improvement of symptoms but will not correct the overall process. Determination of fibular length is best done by comparing the talocrural angle of the injured side with the uninjured side. The goal is to perfectly reduce the talus in the ankle mortise. Marti RK, Raaymakers EL, Nolte PA: Malunited ankle fractures: The late results of reconstruction. J Bone Joint Surg Br 1990;72:709-713. Geissler W, Tsao A, Hughes J: Fractures and injuries of the ankle, in Rockwood CA Jr, Green DP, Bucholz RW, Heckman JD (eds): Rockwood and Green's Fractures in Adults, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 2201-2206.
Question 870
High Yield
A 16-year-old snowboarder has significant pain and is still unable to bear weight after sustaining a lateral ankle injury in a fall 1 week ago. Examination reveals swelling and tenderness in the sinus tarsi. AP, lateral, and mortise radiographs of the ankle are unremarkable. Management should consist of
Explanation
Because there is a significant possibility that the patient may have a fracture of the lateral process of the talus, there is some disagreement as to the best radiographic study to identify this injury. A CT scan is an appropriate diagnostic tool to visualize the fracture and identify any displacement. Displaced lateral process fractures are best treated surgically. Kirkpatrick DP, Hunter RE, Janes PC, Mastrangelo J, Nicholas RA: The snowboarder's foot and ankle. Am J Sports Med 1998;26:271-277.
Question 871
High Yield
A 25-year-old woman has had continuous pain after falling on her outstretched wrist 12 weeks ago. A current radiograph is shown in Figure 11. Management should consist of

Explanation
The patient has a scaphoid fracture with cystic resorption of the distal aspect of the midthird of the scaphoid. This fracture is unlikely to heal without intervention. Percutaneous pinning, closed manipulation, and bone grafting will not restore alignment. Treatment requires restoration of scaphoid length, bone grafting, and internal fixation to obtain healing with normal alignment. Cooney WP, Linscheid RL, Dobyns JH, Wood MB: Scaphoid nonunion: Role of anterior interpositional bone grafts. J Hand Surg Am 1988;13:635-650. Fernandez DL: A technique for anterior wedge-shaped grafts for scaphoid nonunions with carpal instability. J Hand Surg Am 1984;9:733-737. Stark HH, Rickard TA, Zemel NP, Ashworth CR: Treatment of ununited fractures of the scaphoid by illiac bone grafts and Kirschner-wire fixation. J Bone Joint Surg Am 1988;70:982-991.
Question 872
High Yield
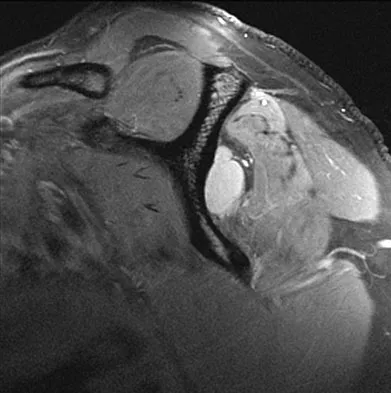
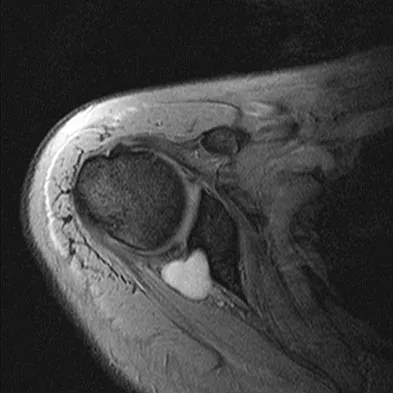
A 25-year-old tennis player has shoulder pain and weakness to external rotation. MRI scans are shown in Figures 16a and 16b. What is the most likely cause of his weakness?
Explanation
The MRI scans show a paralabral cyst, which is most commonly associated with labral tears. Compression of the suprascapular nerve results in weakness of the supraspinatus and/or infraspinatus depending on the level of compression. Piatt BE, Hawkins RJ, Fritz RC, et al: Clinical evaluation and treatment of spinoglenoid notch ganglion cysts. J Shoulder Elbow Surg 2002;11:600-604.
Question 873
High Yield
A previously asymptomatic 14-year-old girl sustained a twisting injury to her ankle. Radiographs are shown in Figures 2a and 2b. Management should consist of


Explanation
The radiographs show a well-defined, irregular, eccentric lesion in the distal tibia metaphysis with a thin sclerotic margin. The radiographs are diagnostic of nonossifying fibroma, a common entity in this age group and in this location. No further work-up is indicated. The patient was asymptomatic prior to the injury and the lesion is small and thus not worrisome for an impending pathologic fracture; therefore, no treatment is indicated beyond observation. The natural history of these lesions is to gradually ossify as the patient reaches skeletal maturity. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 69-75.
Question 874
High Yield
A 73-year-old man has stiffness after undergoing primary posterior cruciate ligament-retaining total knee arthroplasty 18 months ago. Extensive physiotherapy, dynamic splinting, and manipulations under anesthesia have failed to result in improvement. Examination reveals range of motion from 30 degrees to 60 degrees of flexion. The components are well fixed, and the evaluation for infection is negative. In discussing the possibility of revision arthroplasty, the patient should be advised that
Explanation
Stiffness following primary total knee arthroplasty remains a vexing problem. Treatment options have included extensive physical therapy, dynamic splinting, manipulation under anesthesia, arthroscopic arthrolysis, open arthrolysis with polyethylene exchange, and ultimately revision arthroplasty. Results are not as gratifying as would be expected. Babis and associates performed an open arthrolysis and polyethylene exchange on seven patients who were followed for a mean of 4.2 months. The results were poor. The mean improvement in arc of motion was only 20 degrees. Nicholls and Dorr treated 13 patients for stiffness. Only 40% of those patients obtained good to excellent results. Four patients (30%) required manipulation because of recurrent stiffness postoperatively. They noted they could not predictably improve the arc of motion with a revision operation. Haidukewych and associates reported on 15 patients who underwent revision of well-fixed components after total knee arthroplasty for stiffness. Of the 15 patients, 10 (66%) were satisfied with the outcome revision. Interestingly, they noted that in patients for whom the total arc of motion did not improve but who regained near full extension, there was a greater amount of satisfaction with the procedure than for those who did not regain full extension. Babis GC, Trousdale RT, Pagnano MW, et al: Poor outcomes of isolated tibial insert exchange and arthrolysis for the management of stiffness following total knee arthroplasty. J Bone Joint Surg Am 2001;83:1534-1536. Nicholls DW, Dorr LD: Revision surgery for stiff total knee arthroplasty. J Arthroplasty 1990;5:S73-S77.
Question 875
High Yield
A 43-year-old woman has had pain in the left hip for the past 2 months. A radiograph, CT scan, MRI scan, and biopsy specimens are shown in Figures 16a through 16e. What is the most likely diagnosis?


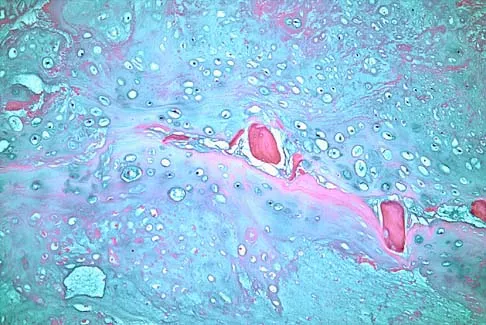
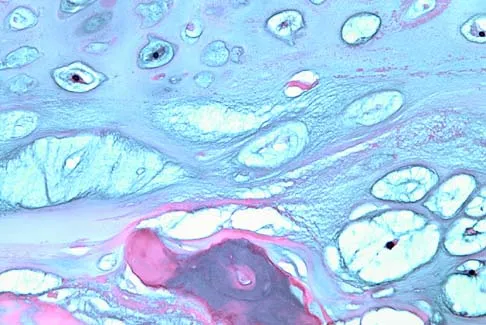
Explanation
The imaging studies are consistent with a chondrosarcoma. The radiograph shows a radiolucent lesion in the pelvis, and there are stippled calcifications on the CT scan. The histology shows a low-grade cellular hyaline cartilage neoplasm with stellate, occasionally binucleated chondrocytes. Enchondroma has a more benign histologic appearance.
Question 876
High Yield
A 12-year-old boy has had progressive pain and flatfeet for the past year. Pain is increased with weight-bearing activities. Examination reveals that subtalar motion is absent. On standing, the patient has obvious hindfoot valgus and loss of the normal arch bilaterally. Plain radiographs are shown in Figures 43a through 43c, and a CT scan is shown in Figure 43d. What is the most likely diagnosis?



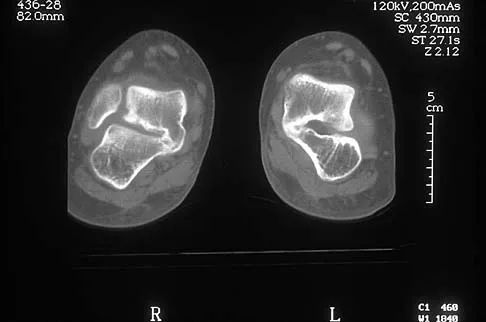
Explanation
The axial views show fusion of the talus and calcaneus at the medial facet (talocalcaneal coalition). Peroneal spastic flatfoot is a descriptive term applying to the symptoms of painful flatfoot associated with apparent peroneal spasm and is sometimes caused by tarsal coalition; however, this is not the most appropriate diagnosis for this patient. Flexible flatfoot with a short Achilles tendon often causes symptoms similar to the ones listed above, but subtalar motion should be normal. A diagnosis of calcaneonavicular coalition can be made based on plain oblique views of the foot but is not seen in these views. Posterior tibial tendon dysfunction in the absence of other pathology is uncommon in children. Vincent KA: Tarsal coalition and painful flatfoot. J Am Acad Orthop Surg 1998;6:274-281.
Question 877
High Yield
A 19-year-old woman fell onto her nondominant hand 6 weeks ago. Radiographs are shown in Figures 37a and 37b. A decision has been made to treat this fracture surgically. What is the best approach to treat this fracture?


Explanation
Displaced fractures of the scaphoid are best treated with compression screw fixation. Proximal third fractures (as in this patient) are optimally approached via a dorsal approach to ensure proper reduction and compression. Fractures of the scaphoid waist can be approached either by a volar or a dorsal approach. Kirschner wire fixation is limited to proximal pole fractures that are too small to accommodate the trailing head of a compression screw. Retting ME, Raskin KB: Retrograde compression screw fixation of acute proximal pole fractures. J Hand Surg Am 1999;24:1206-1210.
Question 878
High Yield
A 52-year-old man who was a former high school pitcher now reports loss of elbow flexion and extension with pain at the extremes of motion. Nonsurgical management has failed to provide relief. Examination reveals movement from 50 degrees to 110 degrees and is painful only at the limits of motion. A radiograph is shown in Figure 12. Treatment should consist of

Explanation
Based on the history, examination, and radiograph, the patient has typical degenerative arthritis of the elbow. This condition is found almost exclusively in men, and there is almost universally a history of repetitive heavy use or overuse of the elbow. Patients report pain at terminal extension and usually have a flexion contracture. Radiographs reveal osteophytes on the coronoid and olecranon and in the coronoid and olecranon fossae. The osteophytes are often associated with loose bodies that sometimes are attached to the soft tissues. Treatment should consist of removal of all loose bodies and impinging osteophytes using open technique or by arthroscopy. The capsular contractures should be released at the same time. Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 283-294. Morrey BF: Primary degenerative arthritis of the elbow: Treatment by ulnohumeral arthroplasty. J Bone Joint Surg Br 1992;74:409-413. Redden JF, Stanley D: Arthroscopic fenestration of the olecranon fossa in the treatment of osteoarthritis of the elbow. Arthroscopy 1993;9:14-16.
Question 879
High Yield
Following preoperative chemotherapy, the percent of tumor necrosis has been shown to be of prognostic value for which of the following tumors?

Explanation
The grading of response to chemotherapy for osteosarcoma was introduced by Huvos and associates. Patients with tumors that show more than 90% necrosis after neoadjuvant chemotherapy are considered to have had a good response and have better survival rates than those with less than 90% necrosis. However, it should be noted that survival rates for patients with a poor response are still better than in patients who do not receive neoadjuvant chemotherapy. More recently, similar results have been reported in patients with Ewing's sarcoma. Chemotherapy is not typically used for giant cell tumor of bone. Meyers PA, Heller G, Healey J, Huvos A, Lane J, Marcove R, et al: Chemotherapy for nonmetastatic osteogenic sarcoma: The Memorial Sloan- Kettering experience. J Clin Oncol 1992;10:5-15.
Question 880
High Yield
A 30-year-old woman sustained a nondisplaced unilateral facet fracture of C5 in a motor vehicle accident. She is neurologically intact and has no other injuries. Management should consist of

Explanation
The patient has a stable bony fracture that will heal with immobilization in a rigid collar. Flexion-extension radiographs may be obtained at 6 weeks to verify that there is no instability; mobilization may then be begun.
Question 881
High Yield
The tibiofibular overlap used to diagnose syndesmotic diastasis on an AP view is most commonly measured between the
Explanation
The tibiofibular overlap is measured between the medial border of the fibula and the lateral border of the anterior tibial tubercle. Plain radiographic assessment of the distal tibiofibular syndesmosis requires AP and mortise views. The following criteria have been used as the normal limits in adults: a talocrural angle of + or - 83 degrees with up to 5 degrees of normal difference between both sides, a medial clear space of less than 4 mm, a talar tilt of less than 2 mm, a tibiofibular clear space of less than 5 mm, a tibiofibular overlap of greater than or equal to 0 mm, and a talar subluxation that is a subjective assessment of congruity of the tibial articular surface and the talar dome; any incongruity is abnormal. It has been recommended to obtain the first three measurements on the mortise view and the other three on the AP view. Wuest TK: Injuries to the distal lower extremity syndesmosis. J Am Acad Orthop Surg 1997;5:172-181.
Question 882
High Yield
Treatment of adhesive capsulitis has a high failure rate when the underlying cause is

Explanation
Diabetes mellitus has been associated with resistant cases of adhesive capsulitis. With other causes of onset, adhesive capsulitis frequently responds to nonsurgical management such as stretching exercises or, when this fails, manipulation under anesthesia and/or arthroscopic release. Manipulation is rarely successful for the treatment of adhesive capsulitis associated with diabetes mellitus, and arthroscopic release may be preferred. Fisher L, Kurtz A, Shipley M: Association between cheiroarthropathy and frozen shoulder in patients with insulin-dependent diabetes mellitus. Br J Rheumatol 1986;25:141-146. Janda DH, Hawkins RJ: Shoulder manipulation in patients with adhesive capsulitis and diabetes mellitus: A clinical note. J Shoulder Elbow Surg 1993;2:36-38.
Question 883
High Yield
A 24-year-old man is ejected from his motorcycle and sustains a significant hip injury. The fracture shown in Figures 64a through 64e is best described as what type of fracture?





Explanation
The radiographs and CT scans reveal an anterior column acetabular fracture. The fracture has quadrilateral plate extension but does not exit out the posterior column. The CT scans confirm an intact posterior column and no wall fracture. A transverse fracture is best seen on the CT scan and runs in the sagittal plane, not the coronal plane. Letournel E, Judet R: Fractures of the Acetabulum, ed 2. New York, NY, Springer-Verlag, 1993, pp 115-140.
Question 884
High Yield
Figures 34a through 34c show an axial proton density (spin echo long TR, short TE) image, a sagittal inversion recovery (STIR) image, and a sagittal T1-weighted (short TR, short TE) image of the left thigh. What is the most likely diagnosis?
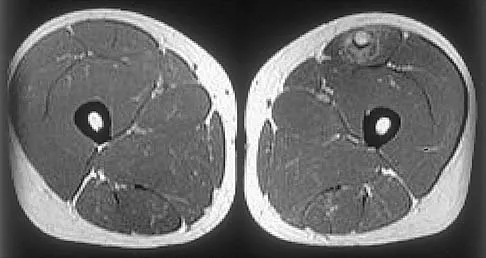

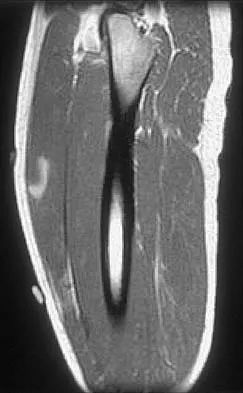
Explanation
The images reveal a region of increased signal within the rectus femoris muscle with mild, ill-defined surrounding edema. The presence of high intensity signal on the T1-weighted image favors acute blood, in this case associated with a rectus femoris muscle tear or fatty tissue. However, because of fat suppression, a fatty lesion or lipoma would be dark on STIR, rather than bright as in this image. Most foreign bodies are low intensity signal and if small, are difficult to evaluate with MRI. The lack of adjacent subcutaneous soft-tissue edema or surrounding fluid makes pyomyositis an unlikely diagnosis.
Question 885
High Yield
Figures 12a through 12e show the radiograph, MRI scans, and biopsy specimens of a 17-year-old boy. What is the most likely diagnosis?

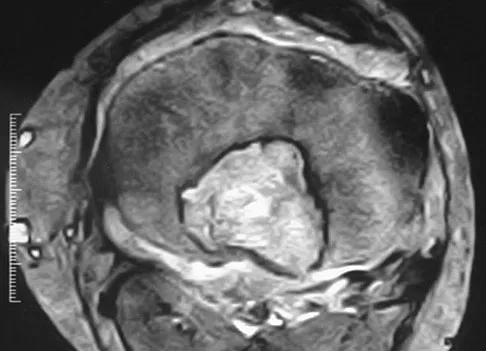

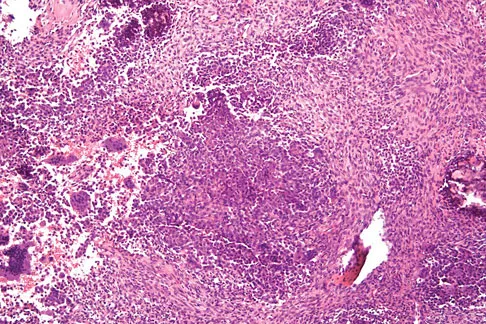
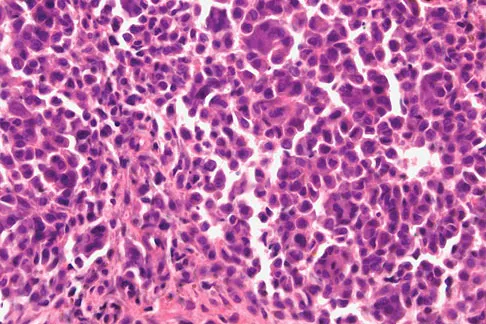
Explanation
The images show an epiphyseal lesion. The MRI scan shows extensive bone edema surrounding the lesion, consistent with chondroblastoma. Histology shows polygonal chondroblasts in a cobblestone-like pattern and areas of calcification consistent with chondroblastoma. Although some giant cells are seen, the age of the patient and the polygonal chondroblasts differentiate this lesion from giant cell tumor. Clear cell chondrosarcoma is an epiphyseal lesion that occurs in an older population, and the cells have clear cytoplasm. This lesion is not producing bone on imaging or histologic specimen, eliminating osteosarcoma. Tuberculous septic arthritis can be an epiphyseal lesion, but granulomas would be seen on histology. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 103-111.
Question 886
High Yield
A 50-year-old man reports left shoulder pain and weakness after undergoing a lymph node biopsy in his neck 2 years ago. Examination reveals winging of the left scapula. Electromyography shows denervation of the trapezius. Surgical treatment for this condition involves
Explanation
The muscle transfer procedure most commonly performed for trapezius paralysis is the Eden-Lange procedure. Trapezius paralysis in this patient is secondary to iatrogenic injury to the spinal accessory nerve during lymph node biopsy. In this procedure, the levator scapulae and rhomboid minor and major muscles are transferred laterally. Pectoralis transfer to the inferior border of the scapula is used as a dynamic transfer for serratus anterior winging. Kuhn JE, Plancher KD, Hawkins RJ: Scapular winging. J Am Acad Orthop Surg 1995;3:319-325. Langenskiold A, Ryoppy S: Treatment of paralysis of the trapezius muscle by Eden-Lange operation. Acta Orthop Scand 1973;44:383-388.
Question 887
High Yield
Why is tendon considered an anisotropic material?
Explanation
Anisotropic materials have mechanical properties that vary based on the direction of loading. The relative values of Young's modulus for tendon, ligament, and bone are not relevant to isotropy. The mechanical properties of tendon do change with preconditioning, but this change is related to viscoelasticity. The intrinsic mechanical properties of tendon do vary with the rate of loading, but this variance is related to viscoelasticity. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 134-180.
Question 888
High Yield
A 56-year-old woman who underwent axillary node dissection 4 months ago now reports shoulder pain, weakness of forward elevation, and obvious winging of the scapula. What structure has been injured?
Explanation
The long thoracic nerve, which innervates the serratus anterior, is prone to injury because of its superficial location along the chest wall. The long thoracic nerve is derived from the roots of C5, C6, and C7. The spinal accessory nerve innervates the trapezius, and the thoracodorsal nerve innervates the latissimus dorsi. The posterior cord of the brachial plexus provides the axillary and the radial nerves. Hollinshead WH: Anatomy for Surgeons: The Back and Limbs, ed 3. Philadelphia, PA, Harper and Row, 1982, pp 259-340.
Question 889
High Yield
Figure 25 shows the CT scan of an adult patient who has neck pain following a motor vehicle accident. What is the most likely diagnosis?

Explanation
If the atlanto-dens interval is greater than 3 mm in an adult, a transverse ligament rupture usually is suspected. The atlanto-dens interval can be seen with CT or in lateral radiographs of the upper cervical spine. Transverse ligament rupture can occur as an isolated entity or in association with an odontoid or a Jefferson's fracture. Patients with this type of injury usually require fusion. Dickman CA, Greene KA, Sonntag VK: Injuries involving the transverse atlantal ligament: Classification and treatment guidelines based upon experience with 39 injuries. Neurosurgery 1996;38:44-50.
Question 890
High Yield
What percent of the adult human meniscus is vascularized?
Explanation
The adult menisci are considered to be relatively avascular structures, with the peripheral blood supply originating predominately from the lateral and medial genicular arteries. Branches of these vessels form the perimeniscal capillary plexus, which supplies the peripheral border throughout its attachment to the joint capsule. Vascular penetration studies have shown that 10% to 30% of the peripheral portion of the medial meniscus and 10% to 25% of the lateral meniscus are vascularized. Arnoczky SP, Warren RF: Microvasculature of the human meniscus. Am J Sports Med 1982;10:90-95.
Question 891
High Yield
A 7-year-old patient has had a painless limp for several months. Examination reveals pain and spasm with internal rotation, and abduction is limited to 10 degrees on the involved side. Management consists of 1 week of bed rest and traction, followed by an arthrogram. A maximum abduction/internal rotation view is shown in Figure 40a, and abduction and adduction views are shown in Figures 40b and 40c. The studies are most consistent with



Explanation
The radiographs show classic hinge abduction. The diagnostic feature is the failure of the lateral epiphysis to slide under the acetabular edge with abduction, and the abduction view shows medial dye pooling because of distraction of the hip joint. Persistent hinge abduction has been shown to prevent femoral head remodeling by the acetabulum. Radiographic changes are characteristic of severe involvement with Legg-Calve-Perthes disease.The Catterall classification cannot be well applied without a lateral radiograph, but this degree of involvement would likely be considered a grade III or IV. Because the lateral pillar is involved, this condition would be classified as type C using the Herring lateral pillar classification scheme.
Question 892
High Yield
Figures 47a through 47f show the AP radiograph, bone scan, CT scan, MRI scan, and biopsy specimens of a 30-year-old woman who has had vague left shoulder pain for 1 year. Management should consist of




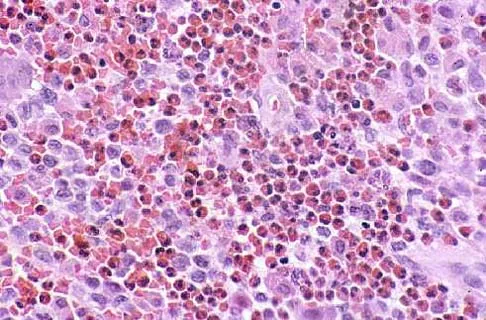
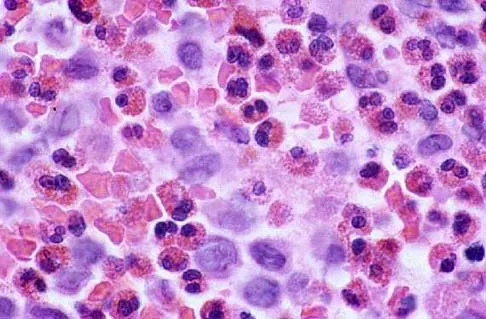
Explanation
The histology shows eosinophils with a background of larger cells (Langerhans' cells). This is consistent with eosinophilic granuloma. Localized sites are best treated with curettage, steroid injection, or observation. Chemotherapy is used only if there is systemic involvement. Mirra JM: Eosinophilic granuloma, in Bone Tumors: Clinical, Radiologic, and Pathologic Correlations. London, England, Lea and Febiger, 1989, pp 1023-1060. Sessa S, Sommelet D, Lascombes P, Prevot J: Treatment of Langerhans-cell histiocytosis in children: Experience at the Children's Hospital of Nancy. J Bone Joint Surg Am 1994;76:1513-1525.
Question 893
High Yield
A 69-year-old woman has just undergone an uncomplicated total shoulder arthroplasty for glenohumeral osteoarthritis. A press-fit humeral stem and a cemented all-polyethylene glenoid component were placed. At this point, what is the postoperative rehabilitation plan?

Explanation
The patient needs to immediately begin an active assisted range-of-motion program emphasizing forward elevation and external rotation to the side. Sling immobilization without stretching for either 3 or 6 weeks will result in severe stiffness that will compromise her ultimate range of motion. Since she has a good quality subscapularis tendon, there is no need to avoid beginning external rotation to the side. However, starting a strengthening program at 3 weeks risks tearing the subscapularis tendon repair. Active strengthening should not begin for 6 weeks postoperatively to allow the subscapularis tendon repair time to heal. Boardman ND III, Cofield RH, Bengston KA, et al: Rehabilitation after total shoulder arthroplasty. J Arthroplasty 2001;16:483-486.
Question 894
High Yield
What is the most important factor regarding the risk of recurrent instability in a patient with an acute anterior dislocation of the shoulder?

Explanation
The recurrence rate of anterior dislocation of the shoulder after the first episode in athletes younger than age 20 years is thought to be as high as 90%, making surgery after the initial episode a consideration. The rate drops from 50% to 75% in the 20- to 25-year age group and down to 15% in patients older than age 40 years. An excellent prospective study of 257 patients in Sweden showed that there was no difference in those who did or did not complete 3 weeks of immobilization. The study also showed variability among different age groups in the importance of athletic participation; athletes in the 12- to 22-year age group had a higher recurrence rate, whereas the more sedentary patients in the 23- to 29-year age group had a higher rate. Hovelius L: The natural history of primary anterior dislocation of the shoulder in the young. J Orthop Sci 1999;4:307-317.
Question 895
High Yield
A 21-year-old college student reports hearing a pop and has acute pain laterally over the ankle after twisting it during a recreational basketball game. Examination 1 hour after the injury reveals minimal swelling and ecchymosis. The anterior drawer sign is positive. Radiographs reveal no evidence of a fracture. What is the best course of action?

Explanation
Even though the patient has a grade 3 ankle ligament injury, studies have shown that 95% of patients with a grade 3 injury that may include a complete tear of the ligaments will heal successfully with conservative functional management. Extensive diagnostic evaluation with stress radiographs, CT, and MRI is not indicated. Surgical reconstruction is not indicated because of the overwhelming success of conservative management; however, in the few patients where late instability develops, surgical reconstruction offers an excellent outcome. Carne P: Nonsurgical treatment of ankle sprains using the modified Sarmiento brace. Am J Sports Med 1989;17:253-257.
Question 896
High Yield
In Figure 49, line AB connects the anterior arch of C1 to the posterior margin of the foramen magnum. Line CD connects the anterior margin of the foramen magnum to the posterior arch of C1. What is the normal ratio of displacement from CD to AB (Power's ratio)?
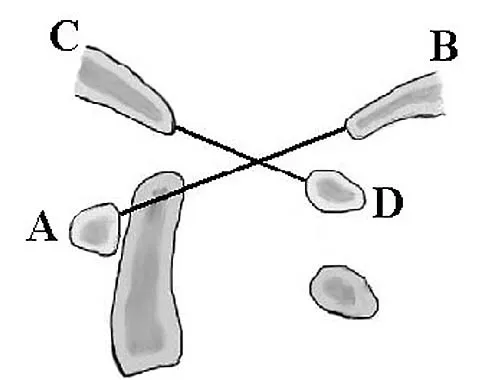
Explanation
The ratio of displacement from CD to AB normally equals 1.0. If the ratio is greater than 1.0, an anterior atlanto-occipital dislocation may exist. Ratios slightly less than 1.0 are normal except in posterior dislocations, fractures of the odontoid process or ring of the atlas, or congenital abnormalities of the foramen magnum. In these conditions, the ratio may approach 0.7. Powers B, Miller MD, Kramer RS, et al: Traumatic anterior atlanto-occipital dislocation. Neurosurgery 1979;4:12-17.
Question 897
High Yield
A 52-year-old woman reports the sudden onset of intense pain in the right shoulder. She denies any history of injury or previous shoulder problems. At a 2-week follow-up examination, she notes that the pain has decreased, but she now has severe weakness of the external rotators and abductors. Her cervical spine and remaining shoulder examination are otherwise unremarkable. Radiographs of the shoulder and neck are normal. What is the most likely diagnosis?

Explanation
Patients with brachial neuritis or Parsonage-Turner syndrome usually report the sudden onset of intense pain that subsides in 1 to 2 weeks, followed by weakness for a period of up to 1 year in the muscle that is supplied by the involved nerve. Calcific tendinitis usually can be diagnosed radiographically, with calcium deposits seen in the rotator cuff. Bursitis and rotator cuff tendinosis usually are seen after an increase in activity, and both decrease with rest and medication. Glenohumeral arthritis is a slow, progressive problem that results in a loss of range of motion. Misamore GW, Lehman DE: Parsonage-Turner syndrome (acute brachial neuritis). J Bone Joint Surg Am 1996;78:1405-1408.
Question 898
High Yield
A 64-year-old man who was involved in a high-speed motor vehicle accident 6 weeks ago has been in the ICU with a closed head injury. Examination reveals that his range of motion for external rotation to the side is -30 degrees. Radiographs are shown in Figures 28a and 28b. What is the most likely diagnosis?


Explanation
The patient has a posterior shoulder dislocation. The AP radiograph shows overlapping of the humeral head on the glenoid. The scapular Y view shows his humeral articular surface posterior to the glenoid. The posterior shoulder dislocation is frequently missed because the patient is comfortable in the "sling" position with the arm adducted and internally rotated across the abdomen. The marked restriction in external rotation on examination raises the suspicion of a posterior dislocation, adhesive capsulitis, or glenohumeral osteoarthritis. The posterior dislocation is diagnosed based on the radiographic findings. An axillary view or CT is recommended to better evaluate the dislocation. Robinson CM, Aderinto J: Posterior shoulder dislocations and fracture-dislocations. J Bone Joint Surg Am 2005;87:639-650.
Question 899
High Yield
The use of multiagent adjuvant chemotherapy is associated with a clear survival benefit in which of the following diseases?
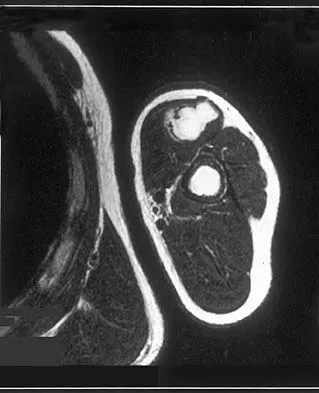
Explanation
The use of multiagent chemotherapy has been shown to be associated with a survival benefit in patients with osteosarcoma. The use of chemotherapy in adults with soft-tissue sarcoma remains somewhat controversial. It has not been associated with improved survival rates in patients with renal carcinoma, dedifferentiated chondrosarcoma, or melanoma. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 53.
Question 900
High Yield
Figures 19a and 19b show the AP and lateral radiographs of an 18-year-old man who has had knee pain for 3 months. Figure 19c shows a histopathologic photomicrograph of the biopsy specimen. Which of the following factors is most likely to affect his survival?


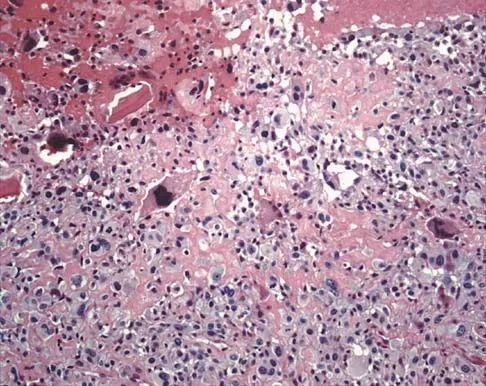
Explanation
The presence of metastatic disease at diagnosis is the most significant prognostic factor in a patient with osteosarcoma. Limb-sparing surgery, when compared with amputation, is not noted to be associated with any difference in the rate of survival. The presence of a mutated p53 gene has been noted in a minority of patients with osteosarcoma; however, the prognostic importance on an individual basis is unclear. Tumor location and a relative poor response to chemotherapy would be secondary to the presence of metastatic disease in estimating a patient's prognosis. Weis L: Common malignant bone tumors: Osteosarcoma, in Simon MA, Springfield DS (eds): Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott-Raven, 1998, pp 265-274.
