HY 2026
00:00
Start Quiz
Question 701
High Yield
A 60-year-old patient had the procedure shown in Figure 7 performed 5 years ago. When converting this patient to a total knee arthroplasty (TKA), what patellar problem is commonly encountered intraoperatively?

Explanation
Patella baja is commonly encountered when converting a high tibial osteotomy (HTO) to a TKA. Patella baja most likely occurs because of scarring. Meding and associates' study did not show an increased rate of lateral release when converting a knee that had undergone a previous HTO. Yoshino N, Shinro T: Total knee arthroplasty after failed high tibial osteotomy, in Callaghan JJ, Rosenberg AG, Rubash HE, et al (eds): The Adult Knee. Philadelphia, PA, JB Lippincott, 2003, vol 2, pp 1265-1271.
Question 702
High Yield
A 12-year-old Little League pitcher reports lateral elbow pain and "catching." Examination reveals painful pronation and supination and tenderness over the lateral elbow. Radiographs are shown in Figures 22a and 22b. Initial management should consist of


Explanation
Osteochondritis of the capitellum is a common problem in young throwing athletes and gymnasts. The mechanism of injury involves lateral compression and axial loading of the capitellum. Repetitive trauma causes ischemia with resultant osteochondral necrosis and sometimes eventual separation. Initial management includes rest for a minimum of 6 weeks; occasionally bracing is used. At long-term follow-up, there is typically an observed radiographic abnormality indicating incomplete healing even in asymptomatic patients. Arthroscopy with in situ drilling is reserved for symptomatic lesions that have an intact articular surface. Lesions with partial separation often require fixation. Lateral column osteotomy is a new investigational procedure designed to relieve lateral compression forces and may be used in salvage cases. Kobayashi K, Burton KJ, Rodner C, et al: Lateral compression injuries in the pediatric elbow: Panner's disease and osteochondritis dissecans of the capitellum. J Am Acad Orthop Surg 2004;12:246-254.
Question 703
High Yield
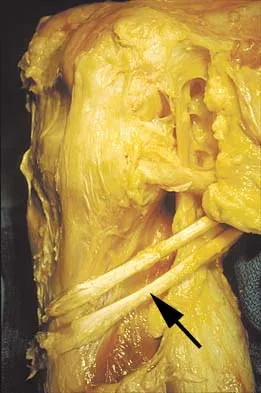
Figure 11 shows the anatomic dissection of the medial side of the knee joint after removal of the superficial fascia. The arrow is pointing to what structure?
Explanation
The semitendinosus and gracilis tendons lie beneath the superficial fascia and superficial to the medial collateral ligament. The semitendinosus is located more inferior to the gracilis tendon. The sartorius is more posterior and distal as is the medial collateral ligament. The semimembranosus is posterior. Pagnani MJ, Warner JJ, O'Brien SJ, Warren RF: Anatomic considerations in harvesting the semitendinosus and gracilis tendons and a technique of harvest. Am J Sports Med 1993;21:565-571.
Question 704
High Yield
A 62-year-old man with diabetes mellitus has had a persistent 2-cm ulcer under the third metatarsal head for the past 4 months. He reports that he has had similar ulcers twice before, and both healed with nonsurgical management. He has used multiple types of commercial walking braces, shoes, and commercial dressings without resolution. He is insensate to the Semmes-Weinstein 5.07 monofilament. When the wound is probed with culture swab, there is no communication with the metatarsal head. Radiographs, bone scans, and laboratory studies reveal no evidence of osteomyelitis. What is the most predictable method of accomplishing wound healing without recurrence?
Explanation
The patient has a persistent diabetic foot ulcer without evidence of osteomyelitis. He has evidence of a sensory peripheral neuropathy and a concomitant motor neuropathy, leading to a dynamic motor imbalance. Use of a total contact cast would offer a high probability of healing the resistant ulcer but with a high potential for recurrence. Combining the total contact cast with Achilles tendon lengthening allows wound healing without a high risk for recurrence. Excision of the noninfected metatarsal head would make the patient vulnerable to the development of a transfer lesion under one of the remaining metatarsal heads. Robertson DD, Mueller MJ, Smith KE, et al: Structural changes in the forefoot of individuals with diabetes and a prior plantar ulcer. J Bone Joint Surg Am 2002;84:1395-1404.
Question 705
High Yield
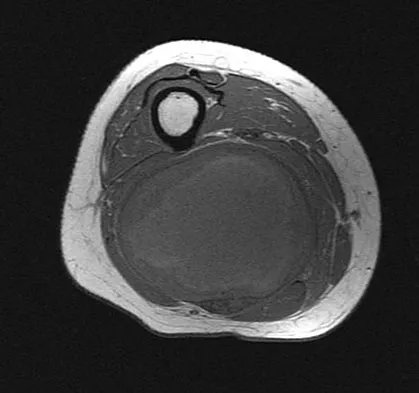
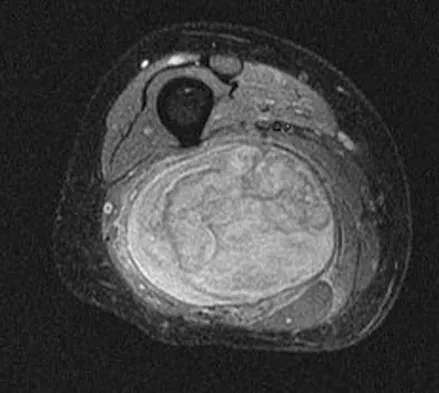
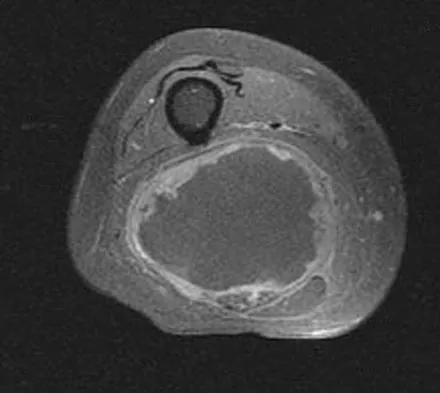
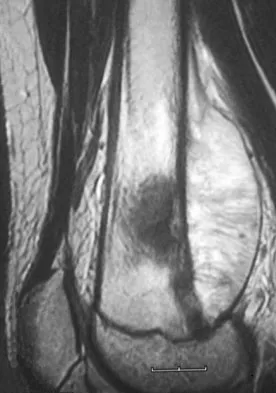
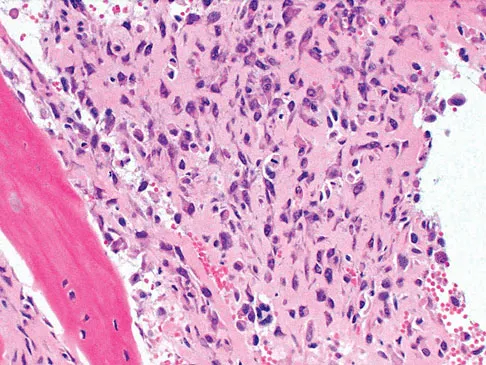
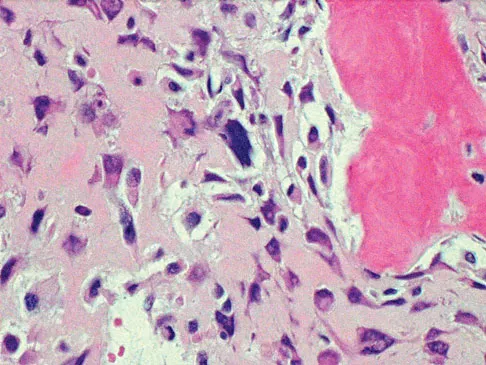
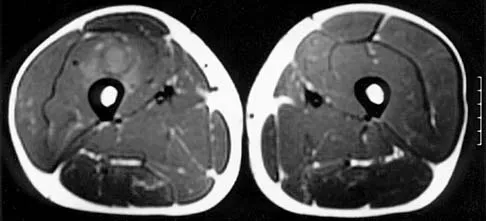
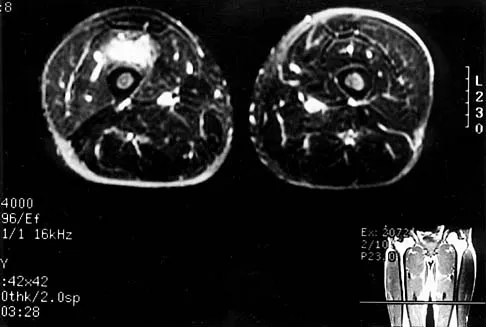
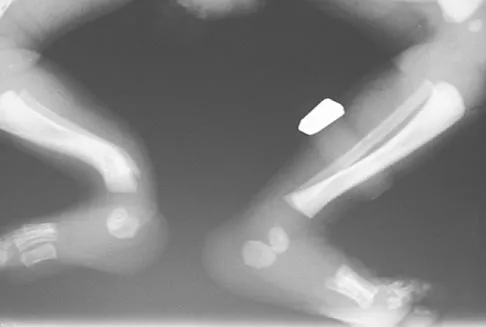
A 36-year-old woman with familial neurofibromatosis has an enlarging mass in the posterior thigh. The lesion has slowly increased in size and is now constantly painful. Pressure on the mass causes dysesthesias in the foot. Figures 44a through 44c show T1-weighted, STIR, and T1-weighted fat-saturated gadolinium scans, respectively. Figure 44d shows a PET scan. What does this lesion most likely represent?

Explanation
The images reveal a large mass in the posterior thigh arising from the sciatic nerve. The lesion is edematous, and the gadolinium image reveals rim enhancement, suggesting necrosis, given that the STIR image is not uniformly bright as would be seen in a cystic lesion. The PET scan has increased uptake, in this case a standard unit value (SUV) of greater than 2.0. These findings are all very suggestive of a malignant process. The history of neurofibromatosis makes a malignant peripheral nerve sheath tumor, or neurofibrosarcoma, the most likely diagnosis. The term "peripheral nerve sheath tumor" has replaced neurolemmoma and schwannoma. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 225-230.
Question 706
High Yield
A 5-year-old boy has had pain in the right foot for the past month. Examination reveals tenderness and mild swelling in the region of the tarsal navicular. Radiographs are shown in Figure 30. Management should consist of

Explanation
The child has the classic findings of Kohler's disease or osteochondrosis of the tarsal navicular. The cause of this condition is not known, but osteonecrosis and mechanical compression have been proposed. Children generally report midfoot pain over the tarsal navicular and limping. Physical findings include tenderness, swelling, and occasionally redness in the region of the tarsal navicular. Radiographs show sclerosis and narrowing of the tarsal navicular. The natural history of the condition is spontaneous resolution and reconstitution of the navicular. Symptomatic treatment with restriction of weight bearing or casting is recommended. Karp M: Kohler's disease of the tarsal scaphoid. J Bone Joint Surg 1937;19:84-96.
Question 707
High Yield
What structure is most often injured in a volar proximal interphalangeal joint dislocation?

Explanation
Closed ruptures of the central slip of the extensor tendon may occur with volar proximal interphalangeal joint dislocation, forced flexion of the proximal interphalangeal joint, or blunt trauma to the dorsum of the proximal interphalangeal joint. The other structures are not typically injured in proximal interphalangeal joint dislocations. Treatment typically requires static splinting of the proximal interphalangeal joint. In the more common dorsal proximal interphalangeal joint dislocation, the volar plate is injured, and early range of motion may be started after reduction. Doyle JR: Extensor tendons: Acute injuries, in Green DP, Hotchkiss RN (eds): Operative Hand Surgery, ed 3. New York, NY, Churchill Livingstone, 1993, p 1925.
Question 708
High Yield
A professional baseball player has had intermittent, mild shoulder pain for the past 2 years. Nonsurgical management has consisted of anti-inflammatory drugs. Examination reveals atrophy of the infraspinatus muscle but not the supraspinatus. There is weakness in external rotation with the arm at his side but not at 90 degrees of abduction. He has no weakness or pain with resisted abduction. Electromyography confirms an isolated lesion of the suprascapular nerve branch to the infraspinatus. He is otherwise neurologically intact. An MRI scan of the shoulder shows no cysts but confirms atrophy of the infraspinatus muscle. What is the next most appropriate step in management?

Explanation
Suprascapular nerve injuries are more commonly seen in athletes who participate in overhead activities. When a patient is evaluated for posterior shoulder pain and infraspinatus muscle weakness or atrophy, electrodiagnostic studies are an essential part of the evaluation. In addition, imaging studies are indicated to exclude other diagnoses that can mimic a suprascapular nerve injury. Initial management should consist of cessation of the aggravating activity along with an organized shoulder rehabilitation program. If nonsurgical management fails to provide relief within 6 months to 1 year, surgical exploration of the suprascapular nerve should be considered. Release of the spinoglenoid ligament with resultant suprascapular nerve decompression may result in pain relief and a return of normal shoulder function. In this patient, who has a chronic neuropathy and mild symptoms, surgery is indicated only if nonsurgical management fails to provide relief and he is unable to perform at his position. Cummins CA, Bowen M, Anderson K, et al: Suprascapular nerve entrapment at the spinoglenoid notch in a professional baseball pitcher. Am J Sports Med 1999;27:810-812. Cummins CA, Messer TM, Nuber GW: Suprascapular nerve entrapment. J Bone Joint Surg Am 2000;82:415-424.
Question 709
High Yield
Figures 29a and 29b show the radiographs of a 13-year-old competitive gymnast who has had elbow pain for the past 2 weeks. The pain is worse with tumbling activities. Examination reveals a mild effusion and slight limitation of extension and forearm rotation with no locking. Initial management should consist of


Explanation
The radiographs show a lesion in the capitellum that is consistent with osteochondritis dissecans. There is no evidence of a loose body at this time. Initial management should consist of cessation of gymnastic activities. Nonsteroidal anti-inflammatory drugs and ice may help to alleviate acute symptoms; most symptoms usually resolve in 6 to 12 weeks. The patient may then begin range-of-motion and strengthening exercises, with a slow return to activities once full range of motion and good strength have been achieved. However, the prognosis for a return to high-level competitive gymnastics is guarded. Surgery is indicated for intra-articular loose bodies, a locked elbow, or failure of nonsurgical management. Surgery may be done either open or arthroscopically. Loose bodies should be removed, and cartilage flaps should be debrided. The results of bone grafting and internal fixation generally have been poor. Drilling the base of the defect may stimulate replacement with fibrocartilage, but the benefits of this procedure are not well documented. Maffulli N, Chan D, Aldridge MJ: Derangement of the articular surfaces of the elbow in young gymnasts. J Pediatr Orthop 1992;12:344-350. Bauer M, Jonsson K, Josefsson PO, Linden B: Osteochondritis dissecans of the elbow: A long-term follow-up study. Clin Orthop 1992;284:156-160.
Question 710
High Yield
A 30-year-old right hand-dominant woman is seen in the trauma unit after a high-speed motor vehicle accident. She sustained a right shoulder anterior dislocation that is gently reduced under sedation. A CT scan is shown in Figure 3. If left untreated, the patient is at greatest risk for

Explanation
Large, displaced anterior inferior glenoid rim fractures predispose patients to recurrent anterior instability due to loss of the normal concavity compression effect of the glenoid. These defects require open reduction and internal fixation to reestablish shoulder stability. Although intra-articular fractures may lead to arthrosis, recurrent instability is more common. Robinson CM, Kelly M, Wakefield AE: Redislocation of the shoulder during the first six weeks after a primary anterior dislocation: Risk factors and results of treatment. J Bone Joint Surg Am 2002;84:1552-1559.
Question 711
High Yield
Which of the following activities can improve posterior capsular contractures?
Explanation
Posterior capsule stretching is performed in the cross-chest and behind the back positions. Stretching in internal rotation in the abducted shoulder will further stretch the posterior capsule. Wide grip stretch, and anterior capsule and strengthening exercises will not necessarily stretch the capsule. Ellenbacher TS: Shoulder internal and external rotation strength and range of motion of highly-skilled junior tennis players. Isokinetic Exercise Sci 1992;2:1-8.
Question 712
High Yield
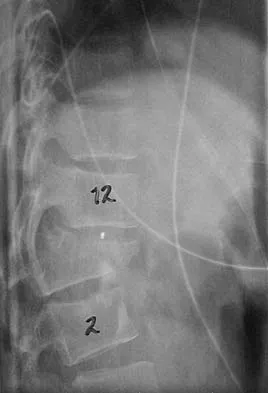
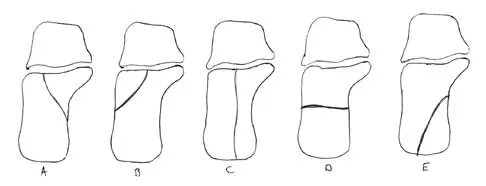
Figures 27a and 27b show the radiographs of a 32-year-old woman who was involved in a high-speed motor vehicle accident. She is neurologically intact. After stabilization and assessment, treatment should consist of

Explanation
The radiographs show a fracture-dislocation with translation in both the coronal and sagittal planes, evidence of significant instability requiring surgical stabilization. Anterior instrumentation is not as effective as posterior instrumentation in restoring stability, and because there is little bony destruction, the anterior column can be successfully reconstructed with simple realignment. The treatment of choice is multisegment posterior fusion with instrumentation. Lewandrowski KU, McLain RF: Thoracolumbar fractures: Evaluation, classification, and treatment, in Frymoyer JW, Wiesel SW (eds): The Adult and Pediatric Spine. Philadelphia, PA, Lippincott Williams and Wilkins, 2004, pp 817-843.
Question 713
High Yield
A 52-year-old man has a stage IIB malignant fibrous histiocytoma of the distal femur. Local treatment should consist of
Explanation
Local control of malignant fibrous histiocytoma of bone typically consists of wide excision. Curettage and bone grafting is a procedure with an intralesional surgical margin, with an unacceptable rate of local recurrence. Prophylactic fixation is considered for patients with metastatic disease. Radiation therapy alone is not adequate for local control of this tumor. Neoadjuvant chemotherapy is often used primarily for systemic tumor control.
Question 714
High Yield
A 69-year-old man reports pain over his bunion while wearing shoes and pain in the joint with push-off when barefoot. Nonsurgical management has failed to provide relief. Radiographs are shown in Figures 8a and 8b. What is the surgical procedure of choice?


Explanation
Arthrodesis is indicated for severe bunion and hallux valgus deformities, but particularly with extensive degenerative disease of the first metatarsophalangeal joint. The other bunionectomy procedures have different indications, none of which include symptomatic first metatarsophalangeal degenerative disease. Richardson EG(ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 3-15.
Question 715
High Yield
Figures 6a through 6d show the radiographs and biopsy specimens of an 8-year-old girl with leg pain. Management of the lesion should consist of


Explanation
The biopsy specimens show a chondromyxoid fibroma with varying amounts of cartilage, benign fibrous tissue, giant cells, and loose myxoid areas. Chondromyxoid fibroma is a benign active bone lesion that is best treated with aggressive curettage and bone grafting. Although recurrences are common, more aggressive treatment is not warranted initially. Wilson AJ, Kyriakos M, Ackerman LV: Chondromyxoid fibroma: Radiographic appearance in 38 cases and in a review of the literature. Radiology 1991;179:513-518.
Question 716
High Yield
A 71-year-old woman who reports long-term use of oral steroids for asthma is referred for treatment of a distal humerus fracture. Radiographs reveal diffuse osteopenia and a severely comminuted intra-articular fracture. What is the most appropriate treatment?
Explanation
Several studies have documented the satisfactory outcomes of total elbow arthroplasty when osteosynthesis is not feasible for fixation of a distal humerus fracture, particularly in the physiologically older patient with low functional demands. Total elbow arthroplasty should be considered when a comminuted intra-articular distal humerus fracture occurs in a woman older than age 65 years, particularly with such associated comorbidities as systemic steroid use, osteoporosis, or rheumatoid arthritis. Kamineni S, Morrey BF: Distal humeral fractures treated with noncustom total elbow replacement. J Bone Joint Surg Am 2004;86:940-947. Frankle MA, Herscovici D Jr, DiPasquale TG, et al: A comparison of open reduction and internal fixation and primary total elbow arthroplasty in the treatment of intraarticular distal humerus fractures in women older than 65. J Orthop Trauma 2003;17:473-480.
Question 717
High Yield
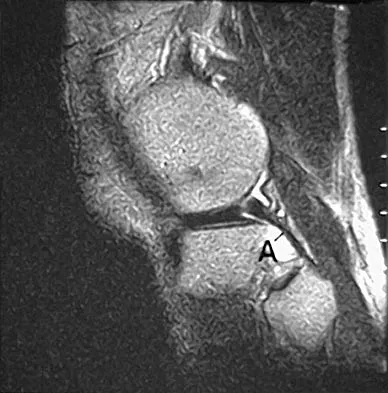
The primary function of structure "A" in Figure 29 is to limit
Explanation
The primary function of the popliteofibular ligament is to resist posterolateral rotation of the tibia on the femur, although it also secondarily resists varus angulation and posterior displacement of the tibia on the femur. The posterior cruciate ligament resists posterior tibial displacement, especially at 90 degrees of flexion. The lateral collateral ligament primarily resists varus displacement at 30 degrees of flexion but also resists posterolateral rotatory displacement with flexion that is less than approximately 50 degrees. The anterior and posterior cruciate ligaments resist varus displacement (along with the lateral collateral ligament) at 0 degrees of flexion. The anterior cruciate ligament primarily resists anterolateral displacement of the tibia on the femur. Sugita T, Amis AA: Anatomic and biomechanical study of the lateral collateral and popliteofibular ligaments. Am J Sports Med 2001;29:466-472.
Question 718
High Yield
A 34-year-old man sustains an extra-articular fracture of the proximal phalanx of his right index finger in a fall. Examination reveals that the fracture is closed and oblique in orientation. Closed reduction and splinting fail to maintain the reduction. Management should now consist of
Explanation
The patient has an unstable oblique fracture of the proximal phalanx that is easily reducible but unstable; therefore, the treatment of choice is closed reduction and percutaneous pin fixation, followed by casting. Closed reduction and percutaneous pin fixation offers a better functional result than open reduction and plate fixation. Repeat closed reduction and buddy taping is inadequate because of the inherently unstable fracture pattern. Buddy taping will allow the dislocation to recur. The other options represent more aggressive surgical techniques than are necessary to treat this fracture. Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC (eds): Green's Operative Hand Surgery, ed 4. Philadelphia, PA, 1999, pp 711-771.
Question 719
High Yield
Which of the following anatomic structures is labeled 6 in Figure 27?
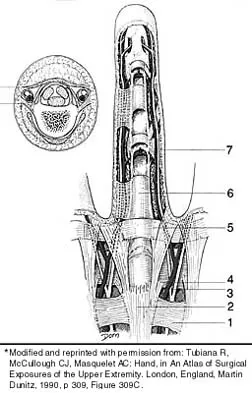
Explanation
The line labeled 6 points to the A2 pulley. This structure is the condensation of the digital flexor tendon sheath corresponding to the proximal aspect of the proximal phalanx. Grayson's ligament is volar to the digital nerve and artery. Cleland's ligament is dorsal to the digital nerve and artery. The sagittal band anchors the extensor tendons over the metacarpophalangeal joints. The triangular ligament connects the lateral bands just proximal to the terminal tendon inserting onto the base of the distal phalanx. Hollinshead WH: Anatomy for Surgeons: The Back and Limbs, ed 3. Philadelphia, PA, Harper and Row, 1982, p 467.
Question 720
High Yield
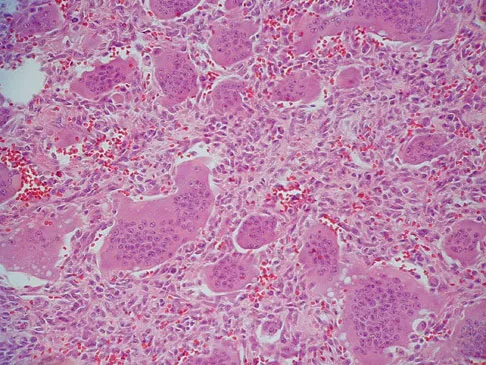
A 16-year-old girl has had painless swelling in her posterior left arm for the past 4 months. A radiograph, MRI scans, and an incisional biopsy specimen are shown in Figures 43a through 43d. What is the cytogenetic translocation most commonly associated with this tumor?

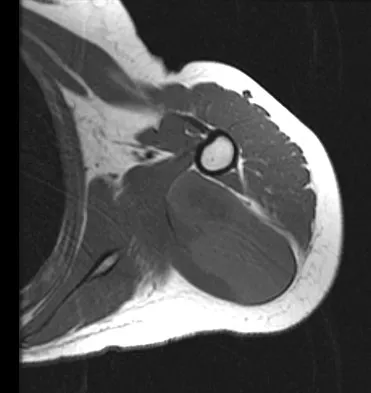
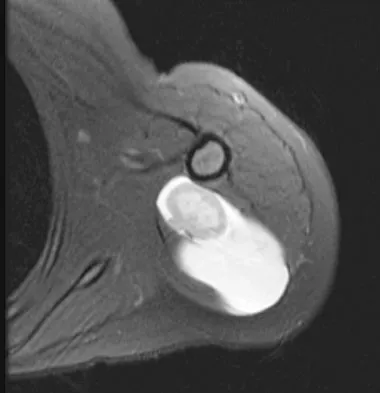
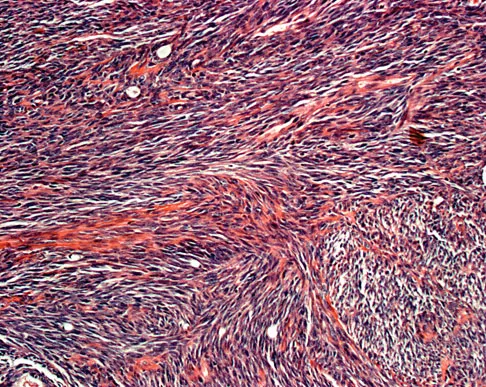
Explanation
This is a case of synovial sarcoma. The radiograph shows some soft-tissue swelling in the upper arm. The MRI scans show a lesion that has increased signal on T2-weighted images and low signal on T1-weighted images. There is a suggestion of a large cystic component to this lesion. The pathology shows a biphasic population of cells, a spindle cell component, and an epithelioid component. Up to 20% of synovial cell sarcomas have areas of cyst formation. The most common cytogenetic translocation with synovial cell sarcoma is X; 18. The 11; 22 translocation is most commonly associated with Ewing's sarcomas; the 12; 22 translocation is most commonly associated with clear cell sarcomas; the 2; 13 translocation is most commonly associated with alveolar rhabdomyosarcomas, and the 12; 16 translocation is most commonly associated with myxoid liposarcomas. Kawai A, Woodruff J, Healey JH, et al: SYT-SSX gene fusion as a determinant of morphology and prognosis in synovial sarcoma. New Engl J Med 1998;338:153-160.
Question 721
High Yield
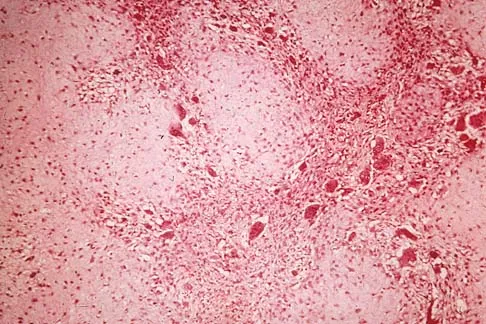
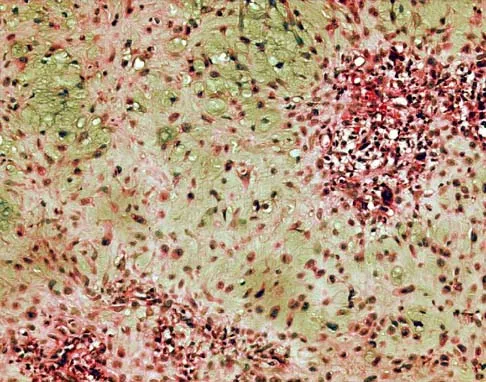
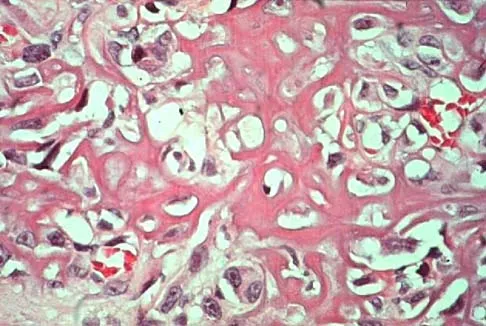
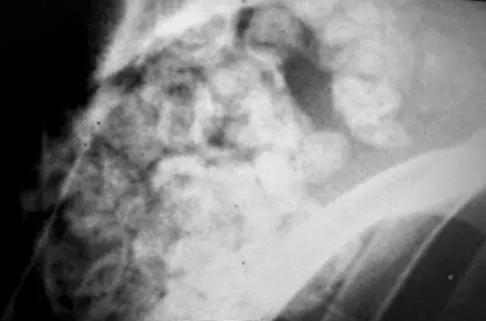
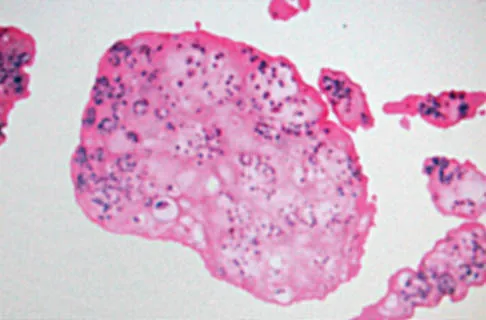
A 10-year-old child has leg discomfort with activity. A radiograph, bone scan, and biopsy specimen are shown in Figures 1a through 1c. What is the most likely diagnosis?


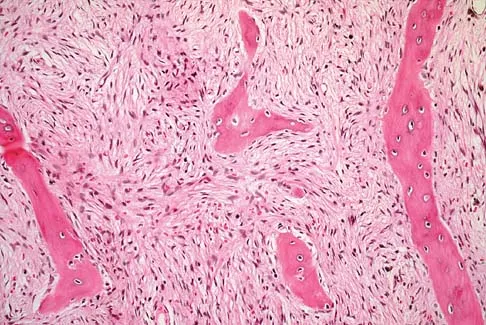
Explanation
The ground glass appearance on the radiograph, the hot bone scan, and histologic findings of bony spicules without osteoblastic rimming in a background of bland fibrous tissue all suggest fibrous dysplasia. Stress-related pain is common with activity because of the dysplastic bone. Parosteal osteosarcomas are surface lesions. Simple cysts, aneurysmal bone cysts, and eosinophilic granuloma are all possible radiographically; however, the histology is most consistent with fibrous dysplasia. Harris WH, Dudley HR Jr, Barry RS: The natural history of fibrous dysplasia: An orthopaedic, pathological and roentgenographic study. J Bone Joint Surg Am 1962;44:207.
Question 722
High Yield
A 23-year-old man who was the restrained driver in a car involved in a high-speed motor vehicle accident sustained the closed injury shown in Figures 32a through 32c. Which of the following factors has the greatest impact on the risk of osteonecrosis?



Explanation
The incidence of osteonecrosis following displaced talar neck fractures is most related to the extent of initial fracture displacement. With increasing fracture displacement, the tenuous vascular supply to the talar body is more at risk for damage, thereby increasing the risk of osteonecrosis. Although displaced talar neck fractures have historically been considered a surgical emergency, recent studies have shown that the timing of surgical intervention bears no impact on the development of osteonecrosis. While nicotine use has an influence on fracture healing, it has never been shown to be a factor in osteonecrosis, nor has posterior-to-anterior screw fixation or the quality of fracture reduction. Lindvall E, Haidukewych G, Dipasquale T, et al: Open reduction and stable fixation of isolated, displaced talar neck and body fractures. J Bone Joint Surg Am 2004;86:2229-2234.
Question 723
High Yield
Which of the following is considered a potential advantage in prophylaxis for the prevention of deep venous thrombosis associated with the use of low-molecular weight heparin (LMWH) as compared with fixed-dose unfractionated heparin?

Explanation
One possible reason for improved efficacy of LMWHs is the relative improved bioavailability compared with that of unfractionated heparin. This is, in part, the result of a more predictable dose response and a longer half-life. There is no alteration of venous flow, and the rate of bleeding complications is the same or slightly higher than that of other prophylactic agents. Colwell CW Jr, Spiro TE, Trowbridge AA: Use of enoxaparin, a low-molecular weight heparin, and unfractionated heparin for the prevention of deep venous thrombosis after elective hip replacement: A clinical trial comparing efficacy and safety. J Bone Joint Surg Am 1994;76:3-14. Bara L, Billaud E, Kher A, Samama M: Increased anti-Xa bioavailability for a low-molecular weight heparin (PK 10169) compared with unfractionated heparin. Semin Thromb and Hemost 1985;11:316-317.
Question 724
High Yield
A 19-year-old woman has a painful right knee. A radiograph, MRI scan, CT scan, and histopathologic specimen are shown in Figures 24a through 24d. What is the most likely oncologic stage of the lesion?



Explanation
The patient has a high-grade osteosarcoma of the distal femur with a skip lesion, and pulmonary metastasis is seen on the CT scan. This corresponds to a stage III lesion according to the Musculoskeletal Tumor Society System as adopted from Enneking.
Question 725
High Yield
Figures 29a and 29b show a clinical photograph and radiographs of a patient who sustained an open calcaneus fracture in a motor vehicle accident. The patient received immediate IV antibiotics and an emergent irrigation and debridement. The swelling has subsided by 3 weeks and the medial wound is clean. What do you tell the patient about the likelihood of infection if a formal open reduction and internal fixation via a lateral approach is performed?


Explanation
Multiple authors have shown similar infection rates for grade 1 and 2 open medial fractures and closed fractures that have been treated with an extensile lateral approach and open reduction and internal fixation. Patients only need IV antibiotics for 2 to 3 days after surgery. Formal open reduction and internal fixation is not recommended for grade 3 medial wounds and most lateral wounds. Heier KA, Infante AF, Walling AK, et al: Open fractures of the calcaneus: Soft-tissue injury determines outcome. J Bone Joint Surg Am 2003;85:2276-2282.
Question 726
High Yield
A 78-year-old man being seen for routine follow-up studies reports mild to moderate pain in his left arm. The patient has a history of lung cancer and severe heart disease. A radiograph and a bone scan are shown in Figures 36a and 36b. Treatment should consist of


Explanation
The patient has lung cancer metastatic to the left humerus that is mildly to moderately symptomatic. Radiographically, the lesion is small and is not associated with significant cortical destruction. Metastatic lesions in the upper extremity have a lower incidence of pathologic fracture than lesions in the lower extremity.
Question 727
High Yield
A 9-year-old child sustained a fracture-dislocation of C-5 and C-6 with a complete spinal cord injury. What is the likelihood that scoliosis will develop during the remaining years of his growth?
Explanation
The incidence of late spinal deformity after complete spinal cord injury in children depends on the level of the spinal cord injury and the age of the patient at the time of injury. If a cervical level injury occurs before age 10 years, paralytic scoliosis will develop in virtually 100% of patients. Brown JC, Swank SM, Matta J, et al: Late spinal deformity in quadriplegic children and adolescents. J Pediatr Orthop 1984;4:456-461. Lancourt JE, Dickson JH, Carter RE: Paralytic spinal deformity following traumatic spinal-cord injury in children and adolescents. J Bone Joint Surg Am 1981;63:47-53.
Question 728
High Yield
A 69-year-old man sustains a traumatic amputation to the distal phalanx of his little finger while working with power tools. Radiographs are shown in Figures 27a and 27b. The patient was instructed how to perform wet-to-dry dressing changes in the emergency department. Clinical pictures taken in the office are shown in Figures 27c through 27e. What is the most appropriate management of this soft-tissue wound?





Explanation
The clinical photographs and radiographs reveal a distal phalangeal amputation with soft-tissue coverage over nonexposed bone. This is an ideal circumstance to allow healing by secondary intention with wet-to-dry dressing changes. There are few complications and the aesthetics surpass that of any soft-tissue reconstruction procedure. Volar advancement flaps (Moberg flaps) are limited to small defects about the thumb. A thenar flap will provide good coverage; however, the results are not comparable to simple dressing changes. A V-Y flap is useful when there is more tissue loss dorsally. Jebson PL, Louis DS: Amputations, in Green DP, Hotchkiss RN, Pederson WC, et al (eds): Green's Operative Hand Surgery, ed 5. Philadelphia, PA, Elsevier, 2005, p 1947.
Question 729
High Yield
An open biopsy specimen of a radiodense distal clavicle lesion in a 12-year-old girl shows chronic polyclonal inflammatory cells without granuloma formation. Laboratory studies show that bacterial, fungal, and acid-fast bacillus cultures are negative. Subsequently, a similar lesion is noted in the fibula. The next most appropriate step in management should consist of
Explanation
The most likely diagnosis is chronic multifocal osteomyelitis. This is a culture-negative polyostotic disease that is most commonly found in young people. The treatment of choice is anti-inflammatory drugs. The pathology does not suggest eosinophilic granuloma. Antiviral therapy, broad-spectrum antibiotics, and surgical resection are not indicated for this disease.
Question 730
High Yield
Figure 38 shows the radiograph of a 75-year-old woman who has had right shoulder pain, difficulty sleeping on the affected arm, and difficulties performing activities of daily living for the past 6 weeks. Initial nonsurgical management includes analgesics, a subacromial cortisone injection, and gentle range-of-motion exercises. However, these modalities have failed to provide relief, and the patient reports that she is unable to elevate her arm. Her pain is worse and she would like the most reliable treatment method for pain relief and functional improvement. What is the best surgical treatment?

Explanation
The authors of several studies conducted in Europe have reported promising results in the short- and medium-term with use of a reversed or inverted shoulder implant. The most recent investigation, a multicenter study in Europe in which 77 patients (80 shoulders) with glenohumeral osteoarthritis and a massive rupture of the rotator cuff were treated with the Delta III prosthesis, described an improvement in the mean constant score of 42 points, an increase of 65 degrees in forward elevation, and minimal or no pain in 96% of the patients. Hemiarthroplasty, the "nonconstrained" option, has long been the standard of care for rotator cuff tear arthropathy. However, careful examination of the literature reveals that the results have not been uniform. Favard L, Lautmann S, Sirveaux F, et al: Hemiarthroplasty versus reverse arthroplasty in the treatment of osteoarthritis with massive rotator cuff tear, in Walch G, Boileau P, Mole D (eds): 2000 Shoulder Prosthesis Two to Ten Year Follow-Up. Montpellier, France, Sauramps Medical, 2001, pp 261-268. Frankle M, Siegal S, Pupello D, et al: The reverse shoulder prosthesis for glenohumeral arthritis associated with severe rotator cuff deficiency: A minimum two-year follow-up study of sixty patients. J Bone Joint Surg Am 2005;87:1697-1705.
Question 731
High Yield
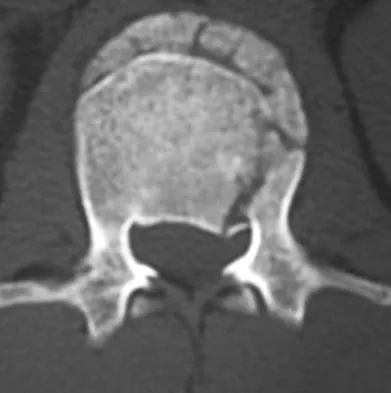
A 32-year-old motorcycle rider is involved in a motor vehicle accident and radiographs show a burst fracture at L2 with 20 degrees of kyphosis. The neurologic examination is consistent with unilateral motor and sensory involvement of the L5, S1, S2, S3, and S4 nerve roots. He has no other injuries. CT demonstrates 20% anterior canal compromise with displaced laminar fractures at the level of injury. What is the best option for management of this patient?
Explanation
The patient has a burst fracture with probable unilateral entrapment of the cauda equina within the elements of the fractured lamina. A dural tear is likely in this scenario as well. It is recommended that this type of burst fracture be treated surgically with laminectomy, freeing of the entrapped nerve roots, and dural repair followed by stabilization of the fracture by either a posterior or combined approach. The degree of kyphosis and the extent of anterior canal compromise does not warrant corpectomy in this patient. Therefore, after completing the laminectomy and dural repair, posterior fusion and instrumentation should be sufficient to stabilize the fracture. Cammisa FP Jr, Eismont FJ, Green BA: Dural laceration occurring with burst fractures and associated laminar fractures. J Bone Joint Surg Am 1989;71:1044-1052.
Question 732
High Yield
A 24-year-old professional football player underwent surgery for a symptomatic cervical disk herniation with radiculopathy 9 months ago. A current radiograph is shown in Figure 17. He has normal neurologic findings, no pain, and full range of motion. A CT scan shows a solid fusion. When can he expect to return to play?

Explanation
The radiograph shows that the two-level anterior cervical diskectomy and fusion has healed. In addition, the patient has good range of motion and the neurologic examination is normal. Based on these findings, the patient can return to play immediately. Patients with one- or two-level anterior cervical diskectomies and fusions that have healed fully can return to play. Any loss of motion, persistent neurologic deficit, or significant adjacent segment degeneration may preclude a player from returning. Thomas B, McCullen GM, Yuan HA: Cervical spine injuries in football players. J Am Acad Orthop Surg 1999;7:338-347.
Question 733
High Yield
A 40-year-old man sustains a fracture-dislocation of C4-5. Examination reveals no motor or sensory function below the C5 level. All extremities are areflexic. The bulbocavernosus reflex is absent. The prognosis for this patient's neurologic recovery can be best determined by
Explanation
The patient has spinal shock. Steroid administration and MRI are appropriate therapeutic and diagnostic procedures. Myelography with CT is of little value unless there is an unusual skeletal variant. Spinal cord-evoked potentials have no value. The best method to determine the patient's neurologic recovery is repeated physical examinations over the first 48 to 72 hours. Spivak JM, Connolly PF (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 183-184.
Question 734
High Yield
What is the most common clinical presentation of a patient with a malignant bone tumor?

Explanation
The most common clinical presentation of a patient with a malignant bone tumor is pain. Malignant bone tumors rarely are diagnosed as an incidental finding or pathologic fracture. In patients who have a pathologic fracture on initial presentation, a history of increasing pain prior to the fracture is typical. While 90% of malignant bone tumors are associated with a soft-tissue mass, in many patients the soft-tissue component of the tumor is not clinically apparent. Buckwalter JA: Musculoskeletal neoplasms and disorders that resemble neoplasms, in Weinstein SL, Buckwalter JA (eds): Turek's Orthopaedics: Principles and Their Application, ed 5. Philadelphia, PA, JB Lippincott, 1994, pp 290-295.
Question 735
High Yield
What is the recommended treatment of a skeletally immature 12-year-old boy who has an anterior cruciate ligament-deficient knee?
Explanation
Traditional surgeries for anterior cruciate ligament-deficient knees carry the potential risk of premature physeal closure in young athletes. Therefore, most surgeons are reluctant to recommend intra-articular reconstruction using bone tunnels with bone-patellar tendon-bone autografts or hamstring tendons. The current recommendation for young athletes is activity modification, rehabilitation, and functional bracing until the patient is near skeletal maturity. At that time, for the very symptomatic patient, the treatment of choice is intra-articular repair of the anterior cruciate ligament. If a skeletally immature patient continues to have instability despite rehabilitation and bracing, a modification of the femoral tunnel to the over-the-top position will not place the lateral femoral physis at risk for premature closure and deformity. A centrally placed tibial tunnel will minimize the risk of angular deformity and minimize limb-length discrepancy if physeal arrest occurs. Barry P: Anterior cruciate ligament injuries, in Andrews JR, Timmerman LA (eds): Diagnostic and Operative Arthroscopy. Philadelphia, Pa, WB Saunders, 1997, p 358. McCarroll JR, Shelbourne KD, Porter DA, Rettig AC, Murray S: Patellar tendon graft reconstruction for midsubstance anterior cruciate ligament rupture in junior high school athletes: An algorithm for management. Am J Sports Med 1994;22:478-484. Nottage WM, Matsuura PA: Management of complete traumatic anterior cruciate ligament tears in the skeletally immature patient: Current concepts and review of the literature. Arthroscopy 1994;10:569-573.
Question 736
High Yield
Which of the following accurately describes the biosynthetic materials tricalcium phosphate (TCP) and hydroxyapatite?
Explanation
TCP is resorbed more rapidly, at a rate of 10 to 20 times faster than hydroxyapatite, partially because its larger pore size makes it a weaker substance. It provides significantly less compressive strength than hydroxyapatite. It does partially convert to hydroxyapatite, thus slowing its resorption rate. The absorbing cell of hydroxyapatite is the foreign body giant cell, not the osteoclast. Optimum pore size appears to be between 150 and 500 um. Lane JM, Bostrom MP: Bone grafting and new composite biosynthetic graft materials. Instr Course Lect 1998;47:525-534.
Question 737
High Yield
In patients with displaced radial neck fractures treated with open reduction and internal fixation with a plate and screws, the plate must be limited to what surface of the radius to avoid impingement on the proximal ulna?

Explanation
The radial head is covered by cartilage on 360 degrees of its circumference. However, with the normal range of forearm rotation of 160 to 180 degrees, there is a consistent area that is nonarticulating. This area is found by palpation of the radial styloid and Lister's tubercle. The hardware should be kept within a 90-degree arc on the radial head subtended by these two structures. Smith GR, Hotchkiss RN: Radial head and neck fractures: Anatomic guidelines for proper placement of internal fixation. J Shoulder Elbow Surg 1996;5:113-117.
Question 738
High Yield
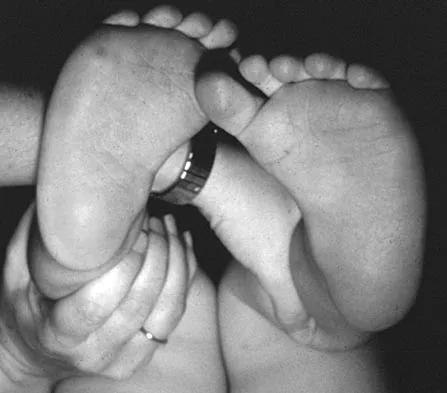
Figure 16 shows the clinical photograph of a 3-month-old infant with a foot deformity that has been nonprogressive since birth. Examination reveals that the deformity corrects actively and with passive manipulation. There is no associated equinus. Management should consist of
Explanation
The patient has bilateral metatarsus adductus deformities. In a long-term follow-up study by Farsetti and associates, deformities that were passively correctable spontaneously resolved and no treatment was required. More rigid deformities were successfully treated with serial manipulation, with good results in 90%. There were no poor results. Therefore, observation is the management of choice for passively correctable deformities. In feet that are more rigid, serial manipulation and casting is the management of choice.
Question 739
High Yield
Which of the following malignant tumors most commonly contains soft-tissue calcifications seen on radiographs or CT?
Explanation
Focal calcifications causing small radiopacities are found in 15% to 20% of synovial sarcomas. Their irregular contours differentiate them from the phleboliths found in a benign hemangioma. Ewing's sarcoma, clear cell sarcoma, and malignant fibrous histiocytoma do not commonly have calcifications within the lesions. Enzinger FM, Weiss SW: Soft Tissue Tumors, ed 3. St Louis, MO, Mosby, 1995, p 761.
Question 740
High Yield
A 13-year-old boy has knee pain after sustaining a mild twisting injury while playing basketball 4 weeks ago. Radiographs and MRI scans are shown in Figures 24a through 24d, and biopsy specimens are shown in Figures 24e and 24f. Treatment should consist of



Explanation
The imaging studies and histology are consistent with high-grade osteosarcoma. The standard treatment for osteosarcoma is neoadjuvant chemotherapy combined with wide surgical resection that can be performed with amputation or limb salvage depending on characteristics unique to each tumor and each patient. In most patients, limb salvage surgery can be performed with reconstruction using allografts and/or megaprostheses. Osteosarcoma is poorly responsive to radiation therapy. Chemotherapy alone, in the absence of appropriate surgery, has not proven effective. Simon MA, Springfield DS: Surgery for Bone and Soft-Tissue Tumors. Philadelphia, PA, Lippincott-Raven, 1998, pp 265-274.
Question 741
High Yield
Figures 8a through 8c show the lateral radiograph and T1- and T2-weighted MRI scans of a 14-year-old soccer player who reports aching thigh pain. The next most appropriate step in management should consist of

Explanation
Although the MRI findings could be misinterpreted as an aggressive soft-tissue process, the periosteal-based ossification on the radiograph in an athlete most likely suggests myositis ossificans. The radiograph should be repeated to see further maturation of the ossification with a typical "zoning" pattern. The zoning pattern is one of peripheral ossification. This is often best seen on a CT scan. King JB: Post-traumatic ectopic calcification in the muscles of athletes: A review. Br J Sports Med 1998;32:287-290.
Question 742
High Yield
A 58-year-old woman is seen in the emergency department after falling at home. History reveals that she underwent right total knee arthroplasty 2 years ago. Radiographs are shown in Figures 56a and 56b. What is the most appropriate treatment?


Explanation
The radiographs show an oblique periprosthetic distal femoral fracture. Of the options listed, open reduction and internal fixation is the most appropriate surgical option because a well-fixed, posterior stabilized closed box femoral component is present. Nonsurgical methods are not favored because of the highly displaced, unstable fracture pattern and prolonged immobility. Revision with a stemmed component is an option but would sacrifice more bone stock in this younger patient. Moran MC, Brick GW, Sledge CB, et al: Supracondylar femoral fracture following total knee arthroplasty. Clin Orthop 1996;324:196-209. Raab GE, Davis CM III: Early healing with locked condylar plating of periprosthetic fractures around the knee. J Arthroplasty 2005;20:984-989.
Question 743
High Yield
What is the most important feature in choosing an outcome instrument to assess shoulder disorders?
Explanation
There has been a recent increase in the use of outcome instruments to document and measure effects of treatment of medical conditions, including shoulder disorders. The most important feature of an instrument is whether it actually measures what it purports to measure; this is defined as its validity. Leggin BG, Iannotti JP: Shoulder outcome measurement, in Iannotti JP, Williams GR (eds): Disorders of the Shoulder: Diagnosis and Management. Philadelphia, PA, Lippincott Williams and Wilkins, 1999, p 1027.
Question 744
High Yield
Figure 23 shows the radiograph of a 55-year-old man who underwent a total hip arthroplasty 5 years ago. Management should now consist of

Explanation
Because the radiograph shows that the femoral stem is loose within the femoral canal and there is a fracture in the distal cement mantle, the stem should be revised. The Ogden-type plate and the allograft bone plates will reconstruct the femur but will not restore stability to the stem. Similarly, traction may allow the femur to heal but will not restore stability to the femoral stem within the femur. Resection arthroplasty is considered a salvage option following failure of the other procedures. Lewallen DG, Berry DJ: Periprosthetic fracture of the femur after total hip arthroplasty: Treatment and results to date, in Cannon WD Jr (ed): Instructional Course Lectures 47. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 243-249.
Question 745
High Yield
When polyethylene is exposed to radiation and subsequently heated, certain chemical changes occur in the material. Which of the following statements best describes these changes?
Explanation
Exposure of polyethylene to radiation and then heating it to quench the free radicals leads to a cross-linked material. It converts a high molecular weight polyethylene macromolecule to an interpenetrating network structure of polymer chains. The ductility of the material is decreased, hence the greater risk of fracture. While the wear rate (measured as fewer and smaller particles) against a smooth counterface is markedly reduced, cross-linked polyethylene has shown a larger increase in wear rate when a rougher counterface is used compared to noncross-linked material. Due to reduced mechanical strength, highly cross-linked polyethylene is less resistant to abrasive wear.
Question 746
High Yield
A 40-year-old man has a painful mass on his anterior ankle joint with limited range of motion. A radiograph, MRI scan, a gross specimen, and a hematoxylin/eosin biopsy specimen are shown in Figures 5a through 5d. What is the most likely diagnosis?


Explanation
Synovial chondromatosis results from chondroid metaplasia within the synovium. Male to female ratio is 2:1, with a peak incidence in early adult life. Radiographs can show speckled cal
Question 747
High Yield
A 21-year-old pitcher reports shoulder pain with hard throwing. He notes that the pain occurs in the early acceleration phase of his throw. Given his history, what structures are at greatest risk for injury?
Explanation
Internal impingement in the thrower's shoulder occurs in the abducted, externally rotated position as described by Walch and associates. The injury is thought to occur from repetitive contact between the posterosuperior portion of the labrum and glenoid against the articular side of the rotator cuff and greater tuberosity. Paley KJ, Jobe FW, Pink MM, et al: Arthroscopic findings in the overhand throwing athlete: Evidence for posterior internal impingement of the rotator cuff. Arthroscopy 2000;16:35-40. Jazrawi LM, McCluskey GM III, Andrews JR: Superior labral anterior and posterior lesions and internal impingement in the overhead athlete. Instr Course Lect 2003;52:43-63.
Question 748
High Yield
A 26-year-old man falls off a motorcycle and injures his left wrist. There are no open wounds and the neurovascular examination is normal. Radiographs are shown in Figures 10a and 10b. Definitive management should consist of


Explanation
The patient has a high-energy injury with resultant comminution of the distal radius metaphysis. Cast immobilization is likely to lead to radial shortening and angulation due to the comminution. Similarly, while external fixation and pinning has been successful in the past, some loss of radial length and volar angulation is typically noted. Present plate fixation devices for the distal radius employing locking screw technology have a superior ability to resist radial shortening and dorsal angulation. Fixation of the ulnar styloid is warranted when there is distal radioulnar joint instability or significant displacement of the styloid. This is more likely to occur with a fracture at the base of the styloid. In this instance, the distal radioulnar joint does not appear to be disrupted. May MM, Lawton JN, Blazar PE: Ulnar styloid fractures associated with distal radius fractures: Incidence and implications for distal radioulnar joint instability. J Hand Surg Am 2002;27:965-971.
Question 749
High Yield
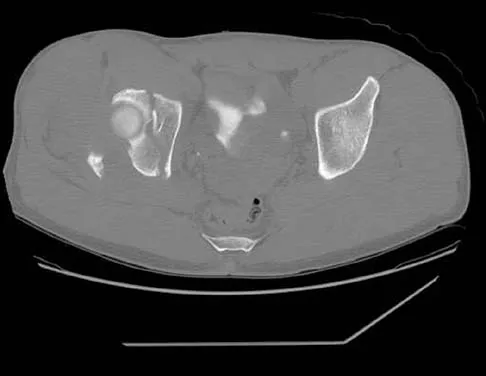
The radiographs and CT scan seen in Figures 28a through 28d reveal what type of acetabular fracture pattern?



Explanation
The AP, obturator oblique, and iliac oblique views of the pelvis reveal a fracture that disrupts the iliopectineal and ilioischial lines, indicating a fracture that involves both anterior and posterior columns. However, it does not have the other features of anterior or posterior column fracture patterns. A displaced posterior wall fracture is also present, best seen on the obturator oblique view. The anterior to posterior directed fracture line on the CT scan indicates a transverse fracture; therefore, the patient has a transverse with posterior wall fracture pattern. A T-type fracture would be similar but would have a break into the obturator ring. Tile M: Describing the injury: Classification of acetabular fractures, in Tile M, Helfet DL, Kellam JF (eds): Fractures of the Pelvis and Acetabulum, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 427-475.
Question 750
High Yield
A 52-year-old woman underwent open reduction and internal fixation for radial and ulnar shaft fractures 2 months ago. In a second fall she refractured her forearm and required revision surgery with bone grafting. One month after the second operation she notes erythema, swelling, and drainage from the volar radial incision. In addition to antibiotic treatment, management should consist of
Explanation
Deep infections after plating of closed fractures of the forearm are unusual. However, the risk increases with repeat surgeries. Debridement of all infected, nonviable tissue is the initial step in management. The fixation may be retained if it is stable, but if the plate and screws are loose, they should be removed and revision performed after removal of nonviable bone. Either external fixation or repeat plating may be performed. Late infections after fracture union may be treated with plate and screw removal, debridement, and IV antibiotics. Kellam JF, Fischer TJ, Tornetta P III, Bosse MJ, Harris MB (eds): Orthopaedic Knowledge Update: Trauma 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 53-63. Moed BR, Kellam JF, Foster RJ, Tile M, Hansen ST Jr: Immediate internal fixation of open fractures of the diaphysis of the forearm. J Bone Joint Surg Am 1986;68:1008-1017.
Question 751
High Yield
A 32-year-old man sustained an L1 burst fracture with 90% canal compromise, intact posterior elements, and kyphosis of 25% at the L1 level. He has an incomplete neurologic injury. Definitive management should consist of
Explanation
With an incomplete injury, the best chance for recovery occurs when the canal is cleared and the neural structures are decompressed. Anterior decompression, vertebral body reconstruction, and anterior stabilization have been shown to be highly effective in the treatment of burst-type injuries. Laminectomy alone is contraindicated because it increases the instability. Short segment posterior fixation has a high rate of failure in this type of injury at this level. Kaneda K, Abumi K: Burst fractures with neurologic deficits of the thoracolumbar spine. J Bone Joint Surg Am 1997;79:69-83.
Question 752
High Yield
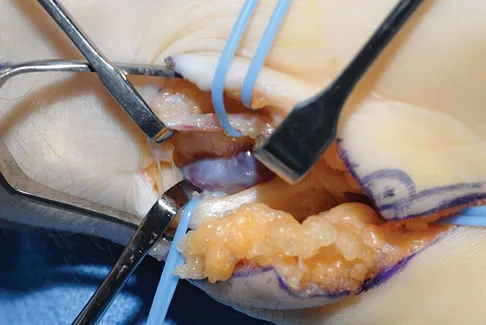
A patient with deficient anteroinferior bone stock undergoes a Latarjet procedure that transfers a portion of the coracoid to the glenoid rim and secures it with two screws. After surgery, the patient reports numbness on the anterolateral forearm. To verify the diagnosis, what muscle should be tested for strength?

Explanation
A Latarjet procedure is similar to a Bristow procedure, but with the Latarjet procedure a larger portion of the coracoid is transferred to the scapular neck at the anteroinferior glenoid. As in a Bristow procedure, if the fragment is pulled or twisted during the dissection or during fixation, the musculocutaneous nerve can be injured. With loss of biceps function, elbow flexion and forearm supination will be weaker. Ho E, Cofield RH, Balm MR, Hattrup SJ, Rowland CM: Neurologic complications of surgery for anterior shoulder instability. J Shoulder Elbow Surg 1999;8:266-270. Boardman ND 3rd, Cofield RH: Neurologic complications of shoulder surgery. Clin Orthop 1999;368:44-53.
Question 753
High Yield
A 24-year-old man sustains the injury shown in Figures 19a through 19e in a paragliding accident. He is neurologically intact. He also sustained fractures of his left femur and right distal radius. Which of the following represents the best option for management of the spinal injury?



Explanation
The injury pattern is that of a burst fracture at L1 contiguous with a compression fracture at T12. There is associated kyphosis and slight spondylolisthesis of T12 on L1. Treatment of this type of burst fracture in neurologically intact patients is somewhat controversial, with at least one study demonstrating equal long-term results comparing nonsurgical treatment to surgical treatment. In this study, however, body casts were used initially in the nonsurgical group. Moreover, because this patient has multiple fractures, spinal fracture stabilization should be considered to facilitate early mobilization. Surgical stabilization and fusion via a posterior approach is the best treatment option in this patient. Anterior decompression is not necessary since the patient is neurologically intact. McLain RF, Benson DR: Urgent surgical stabilization of spinal fractures in polytrauma patients. Spine 1999;24:1646-1654. Wood K, Butterman G, Mehbod A, et al: Operative compared with nonoperative treatment of a thoracolumbar burst fracture without neurological deficit: A prospective, randomized study. J Bone Joint Surg Am 2003;85:773-781.
Question 754
High Yield
A 12-year-old boy who pitches on two "select" baseball teams has had pain in his dominant right shoulder for the past 6 weeks. The pain is present only with throwing and is associated with decreased throwing velocity and control. He has no radiation of pain or paraesthesias of the upper extremity. An AP radiograph and MRI scan are shown in Figures 19a and 19b, respectively. Management should consist of


Explanation
The imaging study demonstrates characteristics of Little Leaguer's shoulder, including physeal widening. This condition is secondary to overuse (typically throwing) and responds well to rest from the inciting activity. There is no evidence from the patient's history or examination that he has an impingement syndrome, nor is there any indication of labral pathology on the MRI scan. The changes in the proximal humerus are classic for this condition and are not suggestive of a neoplastic process requiring biopsy for definitive diagnosis. Lipscomb AB: Baseball pitching injuries in growing athletes. J Sports Med 1975;3:25-34. Cahill BR, Tullos HS, Fain RH: Little league shoulder: Lesions of the proximal humeral epiphyseal plate. J Sports Med 1974;2:150-152.
Question 755
High Yield
A 64-year-old man with a history of diabetes mellitus underwent open reduction and internal fixation of a displaced ankle fracture 8 weeks ago. Examination now reveals recent onset erythema, warmth, and swelling of the midfoot. Radiographs are shown in Figures 23a through 23d. What is the most likely reason for the swelling of the foot?




Explanation
A Charcot flare in adjacent joints is not uncommon in patients with neuropathy who undergo surgery or other trauma. Venous thrombosis would present with swelling of the entire leg, while infection would present earlier in the postoperative period. The radiographs are pathognomonic of Charcot arthropathy, not an unrecognized fracture or gout. A compartment syndrome this late after injury is extremely rare, and there would be no bony distraction associated with compartment syndrome.
Question 756
High Yield
A 55-year-old man who runs on the weekends reports a 1-year history of continued pain directly posteriorly in the heel. Management consisting of anti-inflammatory drugs, icing techniques, a heel-counter in his shoe split, and physical therapy consisting of stretching, contrast baths, custom orthotics, and iontophoresis has failed to provide relief. Not only is his lifestyle disrupted with respect to running, but he now has pain with normal ambulation with all forms of shoe wear. He is not necessarily concerned with returning to running; he is primarily seeking pain relief. A lateral radiograph and clinical photograph are shown in Figures 32a and 32b. Treatment should now consist of


Explanation
The patient has severe calcifications at the insertion of the Achilles tendon. Failure to address the Haglund's exostosis and the calcifications will leave the patient with persistent pain. Steroids should not be injected directly into the tendon because of the increased risk of tendon rupture. Shock wave treatment may have some value in treating plantar fasciitis, but its efficacy has not been documented with insertional calcifications and Haglund's exostosis treatment. Brisement is injection of saline solution around the Achilles tendon in an attempt to decompress the peritenon. This may be valuable in intrasubstance Achilles tendinosis or peritendinitis but has no value with insertional disease. Symptoms persisting beyond 6 months are difficult to treat nonsurgically; therefore, the appropriate treatment protocol is aggressive and must address all pathology. The patient may not be able to run at the level achieved prior to surgery, but the goal of the surgery is pain relief. Clain M, Baxter D: Achilles tendinitis. Foot Ankle 1992;13:482-487. Schepsis A, Wagner C, Leach R: Surgical management of Achilles tendon overuse injuries: A long-term follow-up study. Am J Sports Med 1994;22:611-619. Schepsis A, Leach R: Surgical management of Achilles tendinitis. Am J Sports Med 1987;15:308-315.
Question 757
High Yield
A 19-year-old rugby player has severe knee pain after being injured in a game 2 weeks ago. Examination reveals a knee effusion, limited motion, and increased 3+ Lachman's test and anterior drawer. There is also increased external rotation at 30 degrees of knee flexion when the patient is placed in the prone position. Based on these findings, which of the following actions would most likely increase the risk of anterior cruciate ligament (ACL) reconstruction failure?
Explanation
The patient has a combined ACL and posterolateral corner injury. Failure to diagnose and treat an injury of the posterolateral corner in a patient who has a tear of the anterior or posterior cruciate ligament can result in failure of the reconstructed cruciate ligament. The tibial external rotation test is best performed with the patient in the prone position. A 10-degree side-to-side difference of external rotation at 30 degrees of knee flexion indicates injury to the posterolateral corner. Acute grade III isolated or combined injuries of the posterolateral corner are best treated early by direct repair or by augmentation or reconstruction of all injured ligaments. Postoperative arthrofibrosis after an ACL reconstruction has been observed with preoperative deficiencies of knee motion. Veltri DM, Warren RF: Posterolateral instability of the knee. J Bone Joint Surg Am 1994;76:460-472.
Question 758
High Yield
A 13-year-old girl who competes in gymnastics reports the insidious onset of lateral left elbow pain over the past 6 months. She also notes occasional catching episodes in the elbow; however, she denies any history of trauma. Examination reveals tenderness over the lateral epicondyle and extensor muscle origin. The elbow is stable and has full flexion, but lacks 10 degrees of full extension. An AP plain radiograph and an MRI scan are shown in Figures 17a and 17b. Management of the elbow should consist of


Explanation
The radiograph and MRI scan show osteochondritis dissecans of the capitellum, and the patient's history suggests a loose body. The treatment of choice is arthroscopic removal of the loose body and microfracture of the crater. Excision of the radial head, a cortisone injection, or tennis elbow release does not treat the pathology in the capitellum. Nonsurgical treatment would not relieve the mechanical symptoms of the loose body or promote healing in the crater. Baumgarten TE, Andrews JR, Satterwhite YE: The arthroscopic classification and treatment of osteochondritis dissecans of the capitellum. Am J Sports Med 1998;26:520-530. Jackson DW, Silvino N, Reiman P: Osteochondritis in the female gymnast's elbow. Arthroscopy 1989;5:129-136.
Question 759
High Yield
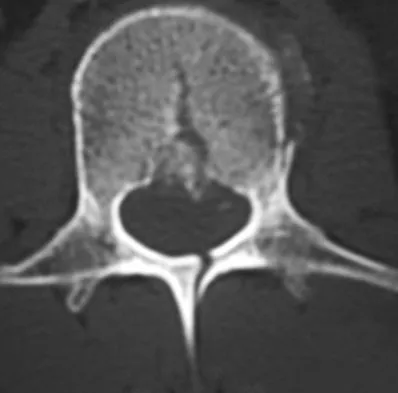
A 44-year-old farmer involved in a rollover accident on his tractor sustained an L1 burst fracture with a 20% loss of anterior vertebral body height, 30% canal compromise, and 15 degrees of kyphosis. He remains neurologically intact. The preferred initial course of action should consist of
Explanation
Surgical decompression is unnecessary in a patient with no neurologic deficit and canal compromise of less than 50%. A compression deformity of less than 50% and kyphosis of less than 30 degrees may be successfully treated with a TLSO extension brace. Deformity in this range will reliably heal with minimal risk for late deformity or residual pain. Although some studies suggest 6 weeks of bed rest as treatment, early mobilization and bracing is preferred. Hartman MB, Chrin AM, Rechtine GR: Nonoperative treatment of thoracolumbar fractures. Paraplegia 1995;33:73-76. Chow GH, Nelson BJ, Gebhard JS, Brugman JL, Brown CW, Donaldson DH: Functional outcome of thoracolumbar burst fractures managed with hyperextension casting or bracing and early mobilization. Spine 1996;21:2170-2175.
Question 760
High Yield
A 20-year-old man sustained an isolated displaced type II odontoid fracture in a motor vehicle accident. He is neurologically intact. Treatment consists of placement in halo traction, and the fracture is reduced. What is the next most appropriate step in treatment?
Explanation
The traditional treatment of a reduced type II fracture is a halo vest. A 20-year-old man will tolerate a halo vest better than the elderly or women. Anterior screw fixation has gained increasing support; however, it too has risks and requires a significant learning curve. More recently, C1 lateral mass screws have become more popular. The long-term results and benefits have not yet been determined. Spivak JM, Connolly PF (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, p 193. Kiovikko MP, Kiuru MJ, Koskinen SK, et al: Factors associated with nonunion in conservatively-treated type-II fractures of the odontoid process. J Bone Joint Surg Br 2004;86:1146-1151. Herkowitz HN, Garfin SR, Eismont FJ: Rothman-Simone The Spine, ed 5. Philadelphia, PA, Saunders Elsevier, 2006, p 1091.
Question 761
High Yield
An obese 4-year-old boy has infantile Blount's disease. Radiographs reveal a metaphyseal-diaphyseal angle of 18 degrees and a depression of the medial proximal tibial physis. Management should consist of

Explanation
The deformity is too severe for observation, and at age 4 years, the child is too old for orthotic treatment. To prevent recurrence, surgery should be performed before irreversible changes occur in the medial physis. A proximal tibial osteotomy should overcorrect the mechanical axis to 10 degrees of valgus. Bar resection has not been shown to be as effective in this severe deformity, especially without a concomitant osteotomy. Raney EM, Topoleski TA, Yaghoubian R, Guidera KJ, Marshall JG: Orthotic treatment of infantile tibia vara. J Pediatr Orthop 1998;18:670-674.
Question 762
High Yield
A 35-year-old man has had progressive right knee pain for the past 2 months. An AP radiograph, bone scan, MRI scan, and photomicrograph are shown in Figures 34a through 34d. What is the most appropriate treatment of this lesion?


Explanation
This is a classic case of giant cell tumor of bone. The radiograph and the MRI scan reveal a purely lytic lesion in the medial femoral condyle. The lesion is well-demarcated without a rim of sclerotic bone. It is eccentrically located and abuts the subchondral bone. The lesion demonstrates increased uptake on a technetium TC 99m bone scan. These imaging studies are highly suggestive of giant cell tumor arising in its most common location. The photomicrograph confirms the diagnosis of giant cell tumor. Based on these findings, the most widely accepted treatment is extended curettage plus a local adjuvant such as polymethylmethacrylate bone cement, argon beam coagulation, liquid nitrogen, and/or phenol. Lackman RD, Hosalkar HS, Ogilvie CM, et al: Intralesional curettage for grades II and III giant cell tumors of bone. Clin Orthop Relat Res 2005;438:123-127.
Question 763
High Yield
What is the most appropriate orthosis for hallux rigidus?

Explanation
A Morton's extension limits excursion of the first metatarsophalangeal joint. It also functions as a ground reaction stabilizer during the toe-off phase of gait and thus reduces torque and joint reaction force at the first metatarsophalangeal joint. The metatarsal arch pad and full-length semi-rigid longitudinal arch support may help by dorsiflexing the first metatarsal relative to the phalanx and thus decompress the first metatarsophalangeal joint. However, they are not as biomechanically effective as the Morton's extension. Both medial hindfoot and lateral forefoot posting are contraindicated because they increase ground reaction at the first metatarsophalangeal joint. Coughlin MJ: Arthritides, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, p 611.
Question 764
High Yield
A patient reports hyperesthesia over the base of the thenar eminence following volar locked plating of a distal radius fracture. A standard volar approach of Henry was used. What is the most likely cause of the hyperesthesia?
Explanation
The palmar cutaneous branch of the median nerve separates from the median nerve approximately 4 to 6 cm proximal to the wrist crease and travels between the median nerve and the flexor carpi radialis tendon. It supplies the skin of the thenar region. This nerve is at risk for injury with retraction of the digital flexor tendons in plating the distal radius. Wartenberg's syndrome is compression of the superficial radial nerve which innervates the dorsum of the thumb and the first dorsal web space. Carpal tunnel syndrome causes dysesthesias of the thumb, index, and/or middle fingers. C7 radiculopathy affects the index and middle fingers. Jupiter JB, Fernandez DL, Toh CL, et al: Operative treatment of volar intra-articular fractures of the distal end of the radius. J Bone Joint Surg Am 1996;78:1817-1828.
Question 765
High Yield
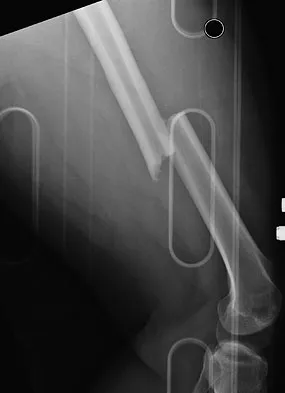
A 24-year-old man was thrown from a car and is seen in the emergency department with a Glasgow Coma Scale (GCS) score of 8. A CT scan of the head shows no significant bleeding. The patient is hemodynamically stable. The left femur has the closed injury shown on the radiographs in Figures 53a and 53b. What is the best treatment for this patient?

Explanation
Treatment of patients with a closed head injury and a femoral fracture remains controversial but recent data suggest that intramedullary nails done acutely with avoidance of intraoperative hypotension did not compromise the outcome related to the head injury. This was especially true for high-level GCS scores. A GCS score of lower than 8 and intraoperative hypotension have been associated with worsening outcomes following acute intramedullary nailing of the femur. Skin traction and distal femur skeletal traction in a young adult man with a femoral fracture is not well tolerated secondary to spasm and pain. External fixation is an option but an unnecessary step in the treatment of this patient. Ventriculostomy is not necessary in stable patients with no significant bleeding on a CT scan of the head. Starr AJ, Hunt JL, Chason DP, et al: Treatment of femur fracture with associated head injury. J Orthop Trauma 1998;12:38-45. Nau T, Kutscha-Lissberg F, Muellner T, et al: Effects of a femoral shaft fracture on multiply injured patients with a head injury. World J Surg 2003;27:365-369. McKee MD, Schemitsch EH, Vincent LO, et al: The effect of a femoral fracture on concomitant closed head injury in patients with multiple injuries. J Trauma 1997;42:1041-1045.
Question 766
High Yield
A 20-year-old woman with a history of subtotal meniscectomy has a painful knee. What associated condition is a contraindication to proceeding with a meniscal allograft?

Explanation
Patients with significant joint malalignment place increased stresses on the allograft, and this malalignment must be corrected to decrease the likelihood of meniscal allograft failure. None of the other options would lead to failure of the allograft.
Question 767
High Yield
A 12-year-old boy sustained a both bone forearm fracture 10 weeks ago and underwent closed reduction and casting. Examination now reveals that the injury is healed, but he is unable to extend his little and ring fingers of the injured hand with his wrist extended. Full extension is possible with the wrist flexed. A radiograph and clinical photograph are shown in Figures 15a and 15b. The remainder of his hand and wrist examination and neurologic evaluation in the hand are normal. What is the most likely diagnosis?


Explanation
In this patient, examination reveals an inability to extend the fingers with the wrist extended, but full extension is possible with wrist flexion. These findings demonstrate isolated tenodesis of the flexor digitorum to the ring and little fingers. These findings are not consistent with compartment syndrome or nerve injury. Scarring or entrapment of tendons in forearm fractures can occur. Watson PA, Blair W: Entrapment of the index flexor digitorum profundus tendon after fracture of both forearm bones in a child. Iowa Orthop J 1999;19:127-128. Shaw BA, Murphy KM: Flexor tendon entrapment in ulnar shaft fractures. Clin Orthop 1996;330:181-184. Kolkman KA, van Niekerk JL, Rieu PN, et al: A complicated forearm greenstick fracture: Case report. J Trauma 1992;32:116-117.
Question 768
High Yield
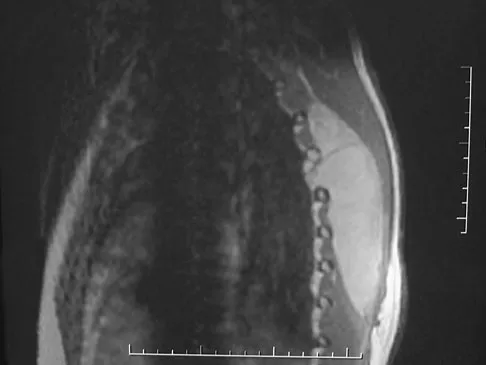
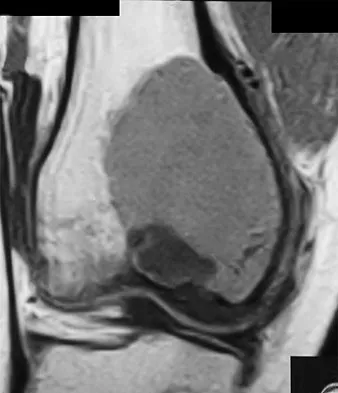
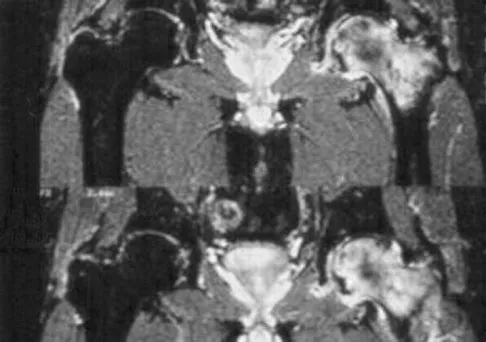
A 58-year-old man reports a 2-month onset of groin pain with no history of trauma. Examination reveals that range of motion of the hip is mildly restricted, and he has pain with both weight bearing and at rest. An MRI scan is shown in Figure 20. Treatment should consist of
Explanation
The MRI findings show highly increased signal through the entire femoral head and neck on STIR imaging, diagnostic of transient osteoporosis of the femoral head. This disease entity can be seen in middle-aged men, and should be treated nonsurgically. The natural history is that of self-resolution. Guerra JJ, Steinberg ME: Distinguishing transient osteoporosis from avascular necrosis of the hip. J Bone Joint Surg Am 1995;77:616-624.
Question 769
High Yield
Design factors that enhance the long-term survival of proximally coated cementless hip implants include both initial stability and
Explanation
Proximally coated femoral components were conceived in response to the proximal stress shielding seen with extensively coated total hip stems, but initial patient studies showed problems with osteolysis, thigh pain, and stability. However, Mont and Hungerford now report that second-generation devices that have been in use more than 5 years clinically have shown very low aseptic loosening rates (1% to 3%), and patients report less thigh pain (less than 5% in most studies). These results can be attributed to improved geometry, instruments, and technique, which ensure initial implant stability. The authors suggest that proximal coating must be circumferential to seal the diaphysis from wear debris, and they note that the concept of proximal coating for cementless femoral stems seems viable as long as the twin requirements of circumferential coating and rigid initial stability are realized. Mont MA, Hungerford DS: Proximally coated ingrowth prostheses: A review. Clin Orthop 1997;344:139-149. Engh CA, Hooten JP Jr, Zettl-Schaffer KF, Ghaffarpour M, McGovern TF, Bobyn JD: Evaluation of bone ingrowth in proximally and extensively porous-coated anatomic medullary locking prostheses retrieved at autopsy. J Bone Joint Surg Am 1995;77:903-910.
Question 770
High Yield
In 1980, a 32-year-old woman was found to have right breast mass, and a biopsy revealed adenocarcinoma. She underwent a mastectomy at that time, with no other treatment. Five years later, she noticed a lump in the left breast and underwent a left mastectomy. Seven lymph nodes were positive. In 2006, she now reports hip and thigh pain for the past 3 months. Figures 69a and 69b show AP and lateral radiographs of the femur. A bone scan shows a solitary lesion. Following radiographic staging, what is the next most appropriate step in management?


Explanation
Solitary bone lesions require biopsy, for there is the possibility that the lesion may represent a primary bone sarcoma, which will necessitate a different treatment plan. This is especially true in patients with remote histories of cancer. The most likely cause of a lytic bone lesion in a patient older than age 40 years is a metastatic lesion. Rougraff BT, Kneisl JS, Simon MA: Skeletal metastases of unknown origin: A prospective study of a diagnostic strategy. J Bone Joint Surg Am 1993;75:1276-1281.
Question 771
High Yield
Figures 11a and 11b show the clinical photograph and radiograph of a newborn. Based on these findings, what is the best course of action?

Explanation
The newborn has posteromedial bowing of the tibia and calcaneal valgus deformity of the foot. Both are thought to be caused by abnormal intrauterine positioning. The foot deformity typically responds to stretching. The tibial bowing straightens with growth. The long-term problem is limb-length discrepancy. Heyman CH, Herndon CH, Heiple KG: Congenital posterior angulation of the tibia with talipes calcaneus. J Bone Joint Surg Am 1959;41:476-488.
Question 772
High Yield
Which of the following is considered an inherent problem in using the distal oblique shortening (Weil) metatarsal osteotomy for dorsal metatarsophalangeal subluxation?

Explanation
The distal oblique shortening (Weil) metatarsal osteotomy has not been associated with transfer lesions to the extent of other shortening osteotomies, and malunions and nonunions are unusual complications. Recurrent dorsal contracture of the toe has been reported. Recommendations to reduce this problem include release of the dorsal capsule and tendons, as well as a flexor tendon transfer. A potential cause suspected for this phenomenon is the relatively dorsal positioning of the intrinsic tendons after plantar displacement of the metatarsal head. Trnka HJ, Nyska M, Parks BG, Myerson MS: Dorsiflexion contracture after the Weil osteotomy: Results of cadaver study and three-dimensional analysis. Foot Ankle Int 2001;22:47-50. Trnka HJ, Muhlbauer M, Zettl R, Myerson MS, Ritschl P: Comparison of the results of the Weil and Helal osteotomies for the treatment of metatarsalgia secondary to dislocation of the lesser metatarsophalangeal joints. Foot Ankle Int 1999;20:72-79.
Question 773
High Yield
What type of cementless femoral fixation results in the highest rate of distal femoral osteolysis?

Explanation
Despite the relatively few problems with porous-coated cementless stems, stress shielding and thigh pain do occur. One design feature of proximally coated stems that has been associated with a higher incidence of distal osteolysis is the presence of noncircumferential proximal porous coating. Tapered, modular with sleeve, and hydroxyapatite proximally porous-coated stems have all performed well. Fully porous-coated straight stems have a high survivorship rate as well. Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 175-180. Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 417-451.
Question 774
High Yield
An 82-year-old man is seen in consultation after being admitted for a fall from ground level. There was no loss of consciousness and the patient recalls striking his head and sustaining a hyperextension-type injury to the cervical spine. Examination reveals an 8-cm head laceration with only mild axial neck tenderness. He has generalized weakness throughout the upper extremities and maintained motor function of the lower extremities. There are no obvious sensory deficits, and the bulbocavernous reflex and deep tendon reflexes are maintained. What is the most appropriate diagnosis at this time?
Explanation
Incomplete cord syndromes have variable neurologic findings with partial loss of sensory and/or motor function below the level of injury. Incomplete cord syndromes include the anterior cord syndrome, the Brown-Séquard syndrome, central cord syndrome, and posterior cord syndrome. Central cord syndrome is characterized with greater motor weakness in the upper extremities than in the lower extremities. The pattern of motor weakness shows greater distal involvement in the affected extremity than proximal muscle weakness. Anterior cord syndrome involves a variable loss of motor function and pain and/or temperature sensation, with preservation of proprioception. The Brown-Séquard syndrome involves a relatively greater ipsilateral loss of proprioception and motor function, with contralateral loss of pain and temperature sensation. Posterior cord syndrome is a rare injury and is characterized by preservation of motor function, sense of pain, and light touch, with loss of proprioception and temperature sensation below the level of the lesion. Spinal shock is the period of time, usually 24 hours, after a spinal injury that is characterized by absent reflexes, flaccidity, and loss of sensation below the level of the injury. Penrod LE, Hegde SK, Ditunno JF: Age effect on prognosis for functional recovery in acute, traumatic central cord syndrome. Arch Phys Med Rehab 1990;71:963-968.
Question 775
High Yield
What is the most common presentation of a benign bone tumor in childhood?

Explanation
The most common benign bone tumors in childhood are discovered incidentally and include single bone cysts, fibrous cortical defects, nonossifying fibroma, and osteochondroma. Benign bone tumors can be classified as latent, active, or aggressive. Aggressive bone tumors usually present with pain, whereas active lesions present with pain or pathologic fracture. Only aggressive benign bone tumors are associated with a soft-tissue mass, and they are far less common than indolent bone tumors, especially in children. Aboulafia AJ, Kennon RE, Jelinek JS: Benign bone tumors of childhood. J Am Acad Orthop Surg 1999;7:377-388.
Question 776
High Yield
A young active patient with a complete isolated posterior cruciate ligament (PCL) tear undergoes a double bundle PCL reconstruction. The tensioning pattern of the anterolateral (AL) and posteromedial (PM) bundles most likely to reproduce the most normal knee kinematics would be to tension
Explanation
During flexion and extension of the normal knee, the AL bundle of the PCL is taut in flexion, and the PM bundle is taut when the knee is near extension. The AL bundle is approximately two times larger at its midsubstance, stiffer, and has a higher ultimate load than the PM bundle. In vitro testing has demonstrated that by tensioning the AL bundle at 90 degrees of flexion and the PM bundle at 0 degrees of flexion, essentially normal knee kinematics are restored. Tensioning the AL bundle at 45 degrees of flexion and the PM bundle at 0 degrees of flexion would result in increased laxity with flexion at 90+ degrees. Tensioning the AL bundle at 90 degrees of flexion and the PM bundle at 45 degrees of flexion would result in increased laxity near extension. Harner CD, Janaushek MA, Kanamori A, Yagi M, Vogrin T, Woo SL: Biomechanical analysis of a double-bundle posterior cruciate ligament reconstruction. Am J Sports Med 2000;28:144-151.
Question 777
High Yield
An elite skier training for the Olympics sustains an isolated traumatic dislocation of the peroneal tendons that have spontaneously reduced. The games are 9 months away and the athlete does not want to miss them. Treatment should consist of

Explanation
Most of these injuries occur in young, active patients. Success rates for nonsurgical management are only marginally better than 50%. The treatment of choice is early surgery for patients who desire a quick return to a sport or active lifestyle. Subluxation of the peroneal tendons leads to longitudinal tears over time. McLennan JG: Treatment of acute and chronic luxations of the peroneal tendons. Am J Sports Med 1980;8:432-436.
Question 778
High Yield
Which of the following complications occurs more commonly after antegrade femoral nail insertion when compared with retrograde insertion?
Explanation
There is no difference between the rates of union, malunion, range of motion of the hip or knee, muscle weakness, or infection for the two types of femoral nail insertion. The only difference is the location of the morbidity, which is around the insertion point of the rod. The antegrade technique has more morbidity about the hip, and the retrograde insertion technique has more morbidity about the knee. Morgan E, Ostrum RF, DiCicco J, McElroy J, Poka A: Effects of retrograde femoral intramedullary nailing on the patellofemoral articulation. J Orthop Trauma 1999;13:13-16. Ricci WM, Bellabarba C, Evanoff B, Herscovici D, DiPasquale T, Sanders R: Retrograde versus antegrade nailing of femoral shaft fractures. J Orthop Trauma 2001;15:161-169. Ostrum RF, Agarwal A, Lakatos R, Poka A: Prospective comparison of retrograde and antegrade femoral intramedullary nailing. J Orthop Trauma 2000;14:496-501.
Question 779
High Yield
A 42-year-old man who is right-hand dominant injured his right shoulder when he fell from a ladder onto his outstretched arm 1 hour ago. Radiographs reveal a two-part greater tuberosity anterior fracture-dislocation. Initial management should consist of
Explanation
Greater tuberosity anterior fractures associated with anterior glenohumeral dislocations respond very well to closed methods in the majority of patients. Closed reduction of the glenohumeral joint often anatomically reduces the greater tuberosity into its cancellous bed, without the need for open fixation or cuff repair. Once closed reduction of the joint is performed, tuberosity displacement and joint articulation should be evaluated radiographically with AP and scapular lateral views as well as an axillary view. The axillary view will not only definitively show the joint articulation but also demonstrate posterior displacement of the greater tuberosity missed on the AP and lateral views. If no or minimal (5 mm) displacement is found, then nonsurgical management consisting of a sling and gentle passive range-of-motion exercises can be instituted. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 271-286.
Question 780
High Yield
Which of the following statements about injury of the anterior vascular structures during lumbar disk surgery is true?
Explanation
Vascular injury most commonly occurs at L4-L5, followed by L5-S1 and are associated with use of the pituitary rongeur. Hohf reported that 17 of 58 patients died as a result. Early recognition and treatment of this complication is vital; unfortunately, intraoperative bleeding from the disk space may occur in up to 50% of these patients. Some may be first recognized in the recovery room. Common clinical findings include hypotension, tachycardia, and a rigid abdomen. Formation of an arteriovenous fistula is the most common vascular injury resulting from lumbar disk surgery but is usually not recognized until months after surgery. Cardiomegaly and high output cardiac failure are common presenting symptoms. Hohf RP: Arterial injuries occurring during orthopaedic operations. Clin Orthop 1963;28:21-37. Montorsi W, Ghiringhelli C: Genesis, diagnosis and treatment of vascular complications after intervertebral disk surgery. Int Surg 1973;58:233-235.
Question 781
High Yield
What form of fixation is associated with the highest incidence of osseous union when using segmental allograft reconstruction following tumor resection?

Explanation
Plate and screw fixation of allograft is associated with the highest incidence of union but also the highest prevalence of allograft fracture. Conversely, intramedullary fixation is associated with a higher incidence of nonunion but fewer fractures. Step-cut osteotomies are not associated with a higher incidence of union.
Question 782
High Yield
Osteonecrosis of the humeral head is a rare complication seen after dislocation of the glenohumeral joint in skeletally immature patients. When this complication is encountered, treatment should consist of
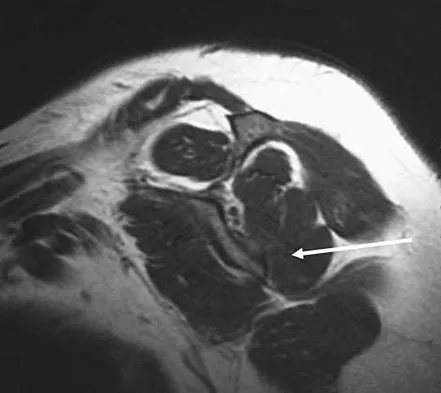
Explanation
This rare complication occurs after fracture-dislocation and has been seen after surgical stabilization in the adolescent. In most reported cases, prolonged observation has been shown to result in revascularization. Pateder DB, Park HB, Chronopoulos E, et al: Humeral head osteonecrosis after anterior shoulder stabilization in an adolescent: A case report. J Bone Joint Surg Am 2004;86:2290-2293.
Question 783
High Yield
Which of the following factors is associated with failure of arthroscopic excision of the distal clavicle?
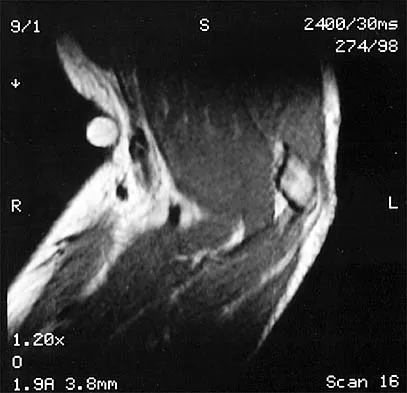
Explanation
Uneven resection of bone, typically leaving a retained posterolateral corner of the distal clavicle, can lead to failure of arthroscopic distal clavicle excision. The amount of bone resected, the gender of the patient, or the diagnosis (osteoarthritis versus osteolysis) does not appear to affect the results.
Question 784
High Yield
A 19-year-old woman reports persistent neck pain for 2 years. Pain is relieved with aspirin. A bone scan shows intense uptake in the superior, posterior portion of the C3 vertebral body. A sagittal CT reconstruction is shown in Figure 5. Treatment should consist of

Explanation
The CT scan shows an osteoblastic nidus pathognomic for an osteoid osteoma. Surgical treatment should include an en bloc excision of the lesion. Surgical treatment is not mandatory because the lesion often becomes asymptomatic over time. This lesion is not amenable to radiofrequency ablation due to its proximity to the spinal cord. A complete corpectomy is not necessary to adequately resect the lesion, as only the nidus needs to be removed. Radiation therapy and antibiotics are not appropriate treatments for an osteoid osteoma. Posterior C2-C3 fusion will not address the pathology. Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 351-366.
Question 785
High Yield
Which of the following factors is the strongest predictor of vertebral fracture in postmenopausal women?
Explanation
If a woman has two or more osteoporotic compression fractures, her risk of another is increased 12 fold. A decrease of two standard deviations in bone mineral density increases the risk four to six fold, a positive family history 2.7 fold, premature menopause 1.6 fold, and smoking 1.2 fold. It should be noted that these studies were carried out in Caucasian and Asian women. Melton LJ III: Epidemiology of spinal osteoporosis. Spine 1997;22:2S-11S.
Question 786
High Yield
A 33-year-old man had his foot run over by a forklift 1 hour ago. Examination reveals that the head of the fifth metatarsal is extruded through the plantar aspect of the foot. The foot is severely swollen and pale, there is no sensation in the toes, and the pulses are not palpable. Radiographs are shown in Figures 42a and 42b. Emergent management should consist of


Explanation
Following a severe crush injury, the patient has an acute compartment syndrome. Even though there is an open fracture, this is not sufficient to decompress the compartment syndrome. Therefore, splinting and observation are not appropriate. The surgical treatment of choice is fasciotomy with fixation of the multiple fractures. A primary amputation is not indicated because there is potential for salvage of this devastating injury. Fakhouri AJ, Manoli A II: Acute foot compartment syndromes. J Orthop Trauma 1992;6:223-228. Myerson MS: Management of compartment syndromes of the foot. Clin Orthop 1991;271:239-248.
Question 787
High Yield
Figure 9 shows the AP radiograph of a 65-year-old man who has knee pain and swelling. What is the most likely diagnosis?

Explanation
Although all the choices are known causes of joint degeneration (secondary osteoarthritis), only chondrocalcinosis shows distinct linear calcification of the cartilage due to deposition of calcium pyrophosphate crystals. Gout is a recurrent acute arthritis resulting from the deposition of monosodium urate from supersaturated hyperuricemic body fluids. Hemochromotosis is characterized by focal or generalized deposition of iron within body tissues. Arthritis may be present but is less common than other manifestations such as liver cirrhosis, skin pigmentation, diabetes mellitus, and cardiac disease. Rheumatoid arthritis is a nonspecific, usually symmetric inflammation of peripheral joints resulting in destruction of articular and periarticular structures. Ochronosis is a hereditary enzyme deficiency (homogentisic acid oxidase) resulting in deposition of homogentisic acid polymers in articular cartilage. Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, p 188.
Question 788
High Yield
A 30-year-old patient reports chronic medial knee pain and swelling. Figure 9a shows an articular cartilage lesion observed during arthroscopy. The surgeon decides to treat the lesion with the microfracture technique seen in Figure 9b. A biopsy of the repaired tissue 1 year after treatment is likely to show which of the following findings?
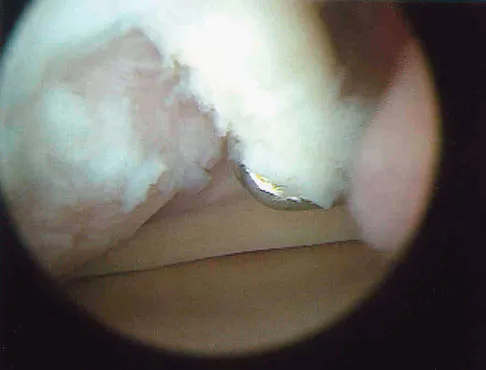
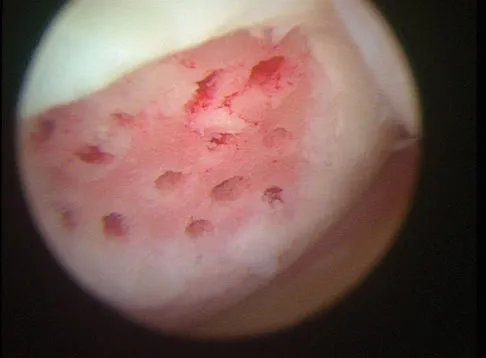
Explanation
Microfracture is a marrow stimulation technique where stem cells from the underlying subchondral bone marrow can form at the base of the lesion. The rationale for this technique is based on these cells differentiating into cells that will produce an articular cartilage repair. Biopsy findings in animals and humans have demonstrated primarily a fibrocartilagenous repair tissue and not articular cartilage. The collagen type found in hyaline or articular cartilage is of the type II variety. Fibrocartilage possesses mostly type I and III cartilage. Buckwalter JA, Mankin HJ: Articular cartilage: Degeneration and osteoarthritis, repair, regeneration, and transplantation. Instr Course Lect 1998;47:487-504.
Question 789
High Yield
A 38-year-old woman with metastatic thyroid carcinoma has had increasing pain in the left hip for the past 3 months. An AP radiograph and coronal T1-weighted MRI scan are shown in Figures 28a and 28b. Management should consist of


Explanation
The radiograph and MRI scan reveal a lytic lesion in the left femoral neck region that extends to the lesser trochanter. Although external beam radiation and radioactive iodine infusion may be helpful in controlling the local disease, the patient is at high risk for femoral neck fracture given the location of the lesion. Prophylactic surgery is indicated; therefore, the treatment of choice is a cemented bipolar hemiarthroplasty. The use of a compression hip screw and side plate or an intramedullary nail has a high likelihood of failure with disease progression. Postoperative treatment with radiation therapy and bisphosphonates is also indicated. Mirels H: Metastatic disease in long bones: A proposed scoring system for diagnosing impending pathologic fractures. Clin Orthop 1989;249:256-264. Swanson KC, Pritchard DJ, Sim FH: Surgical treatment of metastatic disease of the femur. J Am Acad Orthop Surg 2000;8:56-65.
Question 790
High Yield
Which of the following processes does not account for decreased hematopoiesis in patients with metastatic disease?
Explanation
Paucytopenia is a common problem in patients with metastatic disease. Causes include chemotherapy, external beam radiation, marrow replacement by tumor, and anemia of chronic disease. There is no correlation with decreased calcium and a decrease in hematopoiesis. Supportive care with granulocyte-colony stimulating factor (G-CSF) and neupogen can stimulate hematopoiesis.
Question 791
High Yield
A 40-year-old woman underwent an arthroscopic acromioplasty and mini-open rotator cuff repair 4 weeks ago. At follow-up examination, the incision is painful, erythematous, and draining fluid. The patient is febrile and has an elevated WBC count. What infectious organism should be under high suspicion of causing this outcome?
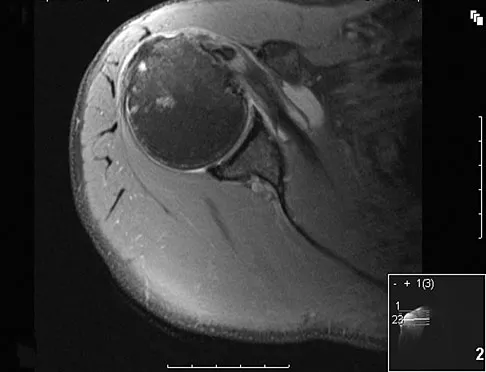
Explanation
Proprionobacter acnes has been a leading cause of indolent shoulder infections. During shoulder arthroscopy, the arthroscopic fluid may actually dilute the shoulder preparation and lead to a higher rate of infection during subsequent mini-open rotator cuff repair surgery. The remaining bacteria listed are rarely associated with shoulder infections after arthroscopy. Herrera MF, Bauer G, Reynolds F, et al: Infection after mini-open rotator cuff repair. J Shoulder Elbow Surg 2002;11:605-608.
Question 792
High Yield
With increasing abduction in the scapular plane, maintaining neutral rotation, contact area, and contact pressure per unit area between the humeral head and glenoid follows what pattern if the total load across the joint is held constant?
Explanation
The glenohumeral joint becomes more congruent at higher levels of abduction. As a consequence, contact area increases. As the load is spread more evenly across the joint, contact pressure per unit area decreases as long as the total load across the joint is held constant. Warner JJP, Bowen MK, Deng XH, et al: Articular contact patterns of the normal glenohumeral joint. J Shoulder Elbow Surg 1998;7:381-388.
Question 793
High Yield
A 71-year-old woman undergoes a posterior lumbar decompression and fusion from L4-S1. Thirty-six hours after the procedure, she reports severe right-sided chest pain and shortness of breath. Doppler ultrasound reveals a clot proximal to the knee within the femoral vein. A large pulmonary embolus is confirmed by CT angiography. The next most appropriate step in management should consist of

Explanation
In a review of 13,000 spinal procedures, nine patients were treated with heparin following development of pulmonary emboli. Of these patients, six had serious complications ranging from wound drainage to paralysis. Heparin therapy instituted within 10 days of the surgical procedure resulted in a 100% complication rate. Vena cava filter placement has a complication rate of 0.12% to 10.1%. Removable filters are currently in clinical trials. Cain JE Jr, Major MR, Lauerman WC, et al: The morbidity of heparin therapy after development of pulmonary embolus in patients undergoing thoracolumbar or lumbar spinal fusion. Spine 1995;20:1600-1603. Roberts AC: Venous imaging and inferior vena cava filters. Curr Opin Radiol 1992;4:88-96.
Question 794
High Yield
Joint contact pressure in normal or artificial joints can best be minimized by what mechanism?
Explanation
Joint contact pressure is a stress and as such is defined as the load transferred across the joint divided by the contact area between the joint surfaces (the area over which the joint load is distributed). Therefore, any mechanism that decreases the load across the joint (eg, a walking aid) will decrease the stress. Similarly, any mechanism that increases the area over which the load is distributed (eg, using a more conforming set of articular surfaces in a knee joint arthroplasty) will also decrease the stress. Other mechanisms that influence joint contact pressure include the elastic modulus of the materials (cartilage in the case of natural joints and polyethylene in joint arthroplasty) and the thickness of the structures through which the joint loads pass. Bartel DL, Bicknell VL, Wright TM: The effect of conformity, thickness, and material on stresses in UHMWPE components for total joint replacement. J Bone Joint Surg Am 1986;68:1041-1051.
Question 795
High Yield
A 22-month-old child has scrapes and bruises on his head and a severe deformity of the forearm after being thrown from a car as an unrestrained passenger in a motor vehicle accident. Examination reveals a Glasgow Coma Scale score of 12. Prior to treatment of the forearm, management should include
Explanation
As CT scanning has become available, the use of radiographs of the skull has decreased in importance for evaluation of head trauma. The indications for CT scanning for suspected head trauma include any degree of obtundation, focal neurologic deficit, history of a high-velocity injury, amnesia for the injury, progressive headache, persistent vomiting, children younger than age 2 years, serious facial injury, posttraumatic seizure, skull penetration, or a Glasgow Coma Scale score of 13 or less. Evidence of improved outcome with use of steroids in head trauma is lacking. Steroids are useful for increased intracranial pressure caused by brain tumors or abscesses. High-dose IV methylprednisolone is indicated for spinal cord trauma and improves the ultimate degree of recovery of function. When herniation is suspected in a patient with asymmetric neurologic findings or the patient's condition is deteriorating rapidly, a mannitol infusion may be used. Hall DE: Head injuries, in Hoekelman RA (ed): Primary Pediatric Care. St Louis, Mo, Mosby, 1997, pp 1709-1712. Nelson WE, Behrman RE, Kliegman RM (eds): Nelson Essentials of Pediatrics. Philadelphia, Pa, WB Saunders, 1998, p 712.
Question 796
High Yield
Following a vertebroplasty of L2, cement is noted to protrude directly anterior to the L2 vertebral body. The cement is closest to which of the following structures?
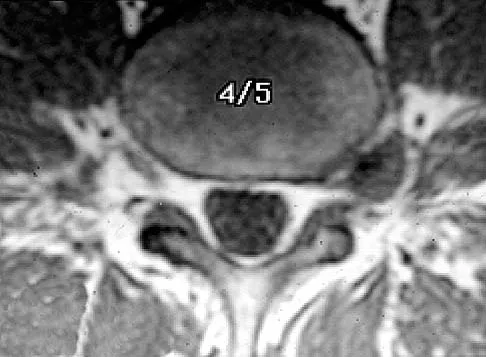
Explanation
At the level of L2, the liver and the vena cava lie to the right. The pancreas and duodenum are anterior to the aorta. The aorta lies in the midline just in front of the vertebral body. Clement CD: Anatomy: A Regional Atlas of Human Anatomy, ed 3. Baltimore, MD, Munich, Germany, Urban and Schwarzberg, 1987, Figure 331.
Question 797
High Yield
Figure 40 shows the MRI scan of a 23-year-old man with a history of recurrent anterior shoulder instability. What is the most likely diagnosis?
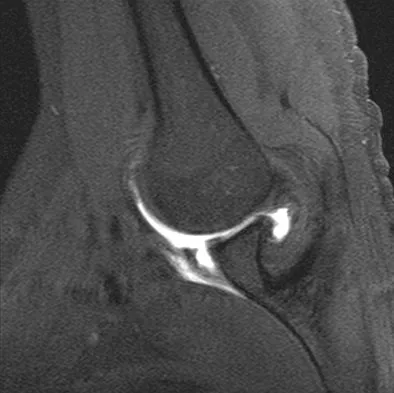
Explanation
The MRI scan shows an ALPSA lesion. This is also known as a medialized Bankart with medial displacement of the torn anterior labrum. During surgical stabilization, the labrum and periosteal sleeve must be mobilized and repaired laterally to reduce recurrent instability. A Perthes lesion is a nondisplaced labral tear. A GLAD lesion represents a nondisplaced anterior labral tear with an associated articular cartilage injury. Neviaser TJ: The anterior labroligamentous periosteal sleeve avulsion lesion: A cause of anterior instability of the shoulder. Arthroscopy 1993;9:17-21.
Question 798
High Yield
The sartorius muscle is innervated by which of the following nerves?

Explanation
The femoral nerve enters the thigh behind the inguinal ligament, lying on the surface of the iliopsoas muscle lateral to the femoral artery and vein. The nerve divides into numerous muscular and cutaneous branches in the femoral triangle. The first motor branch (sometimes two branches) is to the sartorius. There is a variable branch to the pectineus. Subsequent branches go to the rectus femoris and then the vastus muscles in variable order. The last motor branch is to the articularis genu. The muscular branches can be injured in anterior approaches to the hip, especially the middle window of the ilioinguinal approach. Hollinshead WH: Textbook of Anatomy, ed 3. Hagerstown, MD, Harper and Row, 1974, p 404.
Question 799
High Yield
What is the average linear wear rate of a conventional, noncross-linked ultra-high molecular weight polyethylene liner used in total hip arthroplasty?
Explanation
Several studies have shown that ultra-high molecular weight polyethylene liners used in total hip arthroplasties wear at a rate of 0.1 to 0.2 mm/yr. The orthopaedic surgeon performing total hip arthroplasties should be aware of the average wear rate so that potential problems can be identified when following patients postoperatively. Callaghan JJ, Albright JC, Goetz DD, Olejniczak JP, Johnston RC: Charnley total hip arthroplasty with cement: Minimum twenty-five year follow-up. J Bone Joint Surg Am 2000;82:487-497.
Question 800
High Yield
A 25-year-old woman has had pain and stiffness in her knee following a motor vehicle accident 9 months ago. The radiograph, CT scan, MRI scan, and biopsy specimen are shown in Figures 53a through 53d. What is the most likely diagnosis?

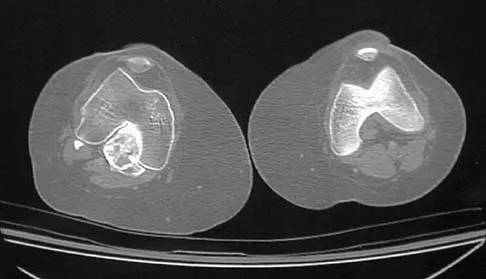
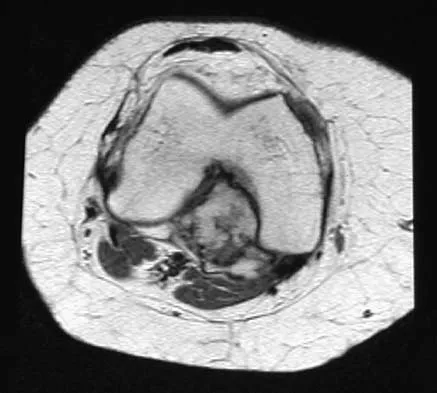
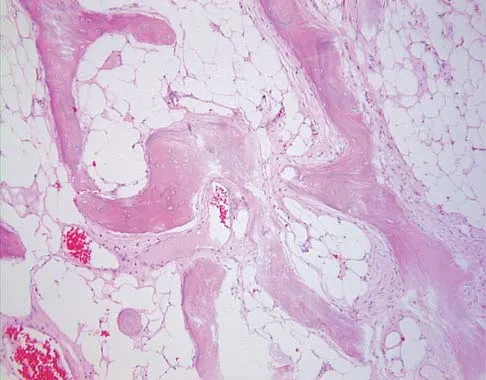
Explanation
Heterotopic ossification may occur spontaneously or following trauma. The imaging studies and histology reveal mature fatty bone marrow and trabecular bone. Osteochondromas are cortically based with the medullary canal extending into the lesion. This is not evident in this patient. Also, no obvious cartilage cap is present. Parosteal osteosarcoma commonly occurs in the posterior distal femoral cortex but is ruled out by the lack of the typical fibrous stromal cells forming the low-grade malignant osteoid. The histology and clinical presentation eliminate osteomyelitis and osteoblastoma. Horne LT, Blue BA: Intra-articular heterotopic ossification in the knee following intramedullary nailing of the fractured femur using a retrograde method. J Orthop Trauma 1999;13:385-388. Stannard JP, Wilson TC, Sheils TM, McGwin G Jr, Volgas DA, Alonso JE: Heterotopic ossification associated with knee dislocation. Arthroscopy 2002;18:835-839.
