HY 2026
00:00
Start Quiz
Question 601
High Yield
Examination of a 4-year old child with obstetrical palsy reveals weak deltoids, pectoralis major strength of 4-5, and normal hand function. External rotation of the shoulder is limited. What is the most appropriate surgical procedure to restore external rotation?
Explanation
Transfer of the latissimus dorsi and teres major to the posterior rotator cuff will restore external rotation and some abduction. The procedure should be performed in children who are approximately age 4 years, following spontaneous recovery and prior to significant stiffness. External rotation osteotomy is more appropriate for an older child. Fusion should not be performed until skeletal maturity. Distal biceps rerouting restores pronation for a supination deformity. Latissimus dorsi and teres major transfer to the subscapularis would accentuate the internal rotation. In younger patients without significant bony deformity, a subscapularis slide or lengthening can restore external rotation. Strecker WB, McAllister JW, Manske PR, Schoenecker PL, Dailey LA: Sever-L'Episcopo transfers in obstetrical palsy: A retrospective review of twenty cases. J Pediatr Orthop 1990;10:442-444.
Question 602
High Yield
Which of the following types of ultra-high molecular weight polyethylene has been associated with the poorest clinical performance?
Explanation
Numerous studies have documented the poor performance of heat-pressed ultra-high molecular weight polyethylene used in the porous-coated anatomic tibial inserts of both total knee and unicompartmental arthroplasty. The other processing and sterilization methods have not been associated with significantly high failure rates. Wright TM, Rimnac CM, Stulberg SD, et al: Wear of polyethylene in total joint replacements: Observations from retrieved PCA knee implants. Clin Orthop 1992;276:126-134. Landy MM, Walker PS: Wear of ultra-high molecular-weight polyethylene components of 90 retrieved knee prostheses. J Arthroplasty 1988;3:S73-S85.
Question 603
High Yield
A right-handed 24-year-old woman underwent an arthroscopic Bankart repair for recurrent anterior dislocations 9 months ago. Despite extensive physical therapy for 8 months, the patient has very limited range of motion (elevation to 130 degrees and external rotation to 10 degrees with the arm at the side). Shoulder radiographs are normal. The next step in management should consist of

Explanation
Arthroscopic capsular release is an effective means of treating stiffness that is the result of capsular contractures, such as in the case of a tight Bankart repair. Open release allows lengthening of a surgically shortened subscapularis, such as after a tight Putti-Platt repair. Additional physical therapy is unlikely to be effective because 8 months of treatment has failed to result in improvement. Accepting this degree of asymptomatic limited motion is not advisable because of the functional limitations for the patient and the increased risk of postoperative degenerative arthritis. Warner JJ, Allen AA, Marks PH, Wong P: Arthroscopic release of postoperative capsular contracture of the shoulder. J Bone Joint Surg Am 1997;79:1151-1158.
Question 604
High Yield
Which of the following drawbacks is associated with the Ganz periacetabular osteotomy?
Explanation
Although technically challenging, the Ganz periacetabular osteotomy offers advantages over other rotational pelvic osteotomies. Posterior column integrity is maintained, as is the acetabular vascular supply. Free mobility of the fragment makes large corrections in the center edge angle possible. Because of the asymmetric cuts and the need to restore anterior coverage, there is a tendency to anterior displacement of the joint while flexing the acetabulum. The procedure is commonly performed through a Smith-Petersen incision. Trousdale RT, Ganz R: Periacetabular osteotomy, in Callaghan JJ, Rosenberg AG, Rubash HE (eds): The Adult Hip. Philadelphia, Pa, Lippincott-Raven, 1998, pp 789-802. Ganz R, Klaue K, Vinh TS, Mast JW: A new periacetabular osteotomy for the treatment of hip dysplasias: Technique and preliminary results. Clin Orthop 1988;232:26-36.
Question 605
High Yield
What is the most common arthroscopic finding of internal impingement in an overhead athlete?
Explanation
Internal impingement occurs when the articular side of the supraspinatus abrades against the posterior superior glenoid in the cocking position. Damage may include a posterior labral tear where the contact occurs, not anteriorly as in a Bankart lesion. Biceps fraying and acromion spurs are more commonly seen in extrinsic impingement. Loose bodies may occur from multiple lesions associated with instability and articular cartilage disorders but are uncommon in internal impingement. Jobe CM: Posterior superior impingement of the rotator cuff on the glenoid rim as a cause of shoulder pain in the overhead athlete. Arthroscopy 1993;9:697-699.
Question 606
High Yield
Progressive paralysis is most likely to be seen in association with what type of congenital vertebral abnormality?
Explanation
Anterior failure of formation results in a progressive kyphosis that may lead to cord compression and progressive neurologic deficit. Anterior failure of segmentation can also produce progressive kyphosis but usually is not severe enough to cause cord compression. Posterior failure of formation is seen in conditions such as myelomeningocele in which the neurologic deficit is generally stable. Lateral abnormalities and posterior failure of segmentation are rarely associated with progressive neurologic deficit. McMaster MJ, Singh H: Natural history of congenital kyphosis and kyphoscoliosis: A study of one hundred and twelve patients. J Bone Joint Surg Am 1999;81:1367-1383.
Question 607
High Yield
In the posterior approach to the proximal radius (proximal Thompson approach), the supinator is exposed through the interval between what two muscles?
Explanation
The proximal exposure of the radius is most often used for internal fixation of fractures, resection of tumors, or decompression of the posterior interosseous nerve beneath the supinator muscle. The supinator muscle is exposed through the interval between the extensor carpi radialis brevis and the extensor digitorum comminus muscles. This interval can be more easily palpated further distal in the forearm. Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics, ed 2. Philadelphia, PA, Lippincott-Raven, 1994, pp 136-146.
Question 608
High Yield
Figure 20 shows the clinical photograph of a man who has had diabetes mellitus controlled with oral medication for the past 10 years. He wears soft-soled shoes and only uses leather-soled shoes for important business meetings. Examination reveals palpable dorsalis pedis and posterior tibial pulses, although they are somewhat diminished. He is insensate to pressure with the Semmes-Weinstein 5.07 monofilament. The ulcer heals after treatment with a full contact cast. What is the best course of action at this time?

Explanation
The patient has not undergone a trial of foot-specific patient education and accommodative/therapeutic shoe wear. He must use therapeutic shoe wear at all times, as even the occasional use of pressure-concentrating shoe wear has a high likelihood of leading to the development of a diabetic foot ulcer. Pinzur MS, Kernan-Schroeder D, Emmanuele NV, et al: Development of a nurse-provided health system strategy for diabetic foot care. Foot Ank Int 2001;22:744-746. Pinzur MS, Shields N, Goelitz B, et al: American Orthopaedic Foot & Ankle Society shoe survey of diabetic patients. Foot & Ankle Int 1999;20:703-707.
Question 609
High Yield
The main blood supply to the lateral two thirds of the talar body is provided by the
Explanation
The main blood supply to the lateral two thirds of the talar body is derived from the artery of the tarsal canal, a branch of the posterior tibial artery. The peroneal artery helps form a vascular plexis over the posterior tubercle and combines with other arteries to form the artery of the sinus tarsi, which is the principal blood supply of the intrasinus structures of the talus. The anterior tibial arteries send branches to the superior surface of the talar head and give rise to the anterolateral malleolar artery, which may anastomose with other vessels to form the artery of the tarsal sinus. Sanders R: Fractures and fracture-dislocations of the talus, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1465-1518.
Question 610
High Yield
During excision of a Baker cyst, the base or stalk is usually found between the

Explanation
Although there are several bursae in the posterior portion of the knee, the most prevalent one with a connection to the knee joint is the one in the interval between the semimembranosus and the medial head of the gastrocnemius muscle. The popliteus muscle and posterior cruciate ligament, the posterior cruciate ligament and lateral gastrocnemius muscle, and the medial gastrocnemius muscle and posterior cruciate ligament are all too lateral and uncommon. The semitendinosus and medial head of the gastrocnemius muscles do not come in contact in the posterior aspect of the knee. Resnick D: Diagnosis of Bone and Joint Disorders, ed 3. Philadelphia, PA, WB Saunders, 1995, p 379.
Question 611
High Yield
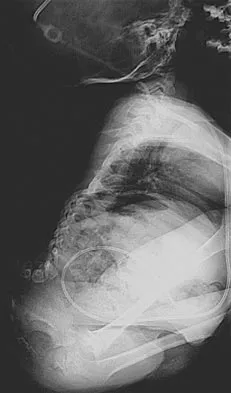
Figure 36 shows the radiograph of a patient who has hip pain and is unable to ambulate. What is the most appropriate management for this patient?

Explanation
The patient has a periprosthetic fracture of the greater trochanter - Vancouver A. The reason for the fracture of the greater trochanter is the extensive periarticular osteolysis that has occurred as a result of polyethylene wear. The latter is demonstrated by eccentric seating of the large femoral head in the acetabulum. The most appropriate management is to reverse the osteolysis process, which involves exchange of the acetabular liner with or without revision of the other components depending on their fixation and position. The greater trochanter can also be fixed during revision surgery. Duncan CP, Masri BA: Fractures of the femur after hip replacement. Instr Course Lect 1995;44:293-304.
Question 612
High Yield
Which of the following findings can cause a dorsal bunion in a patient with neuromuscular disease?
Explanation
Unopposed action of the tibialis anterior with weakness of the peroneus longus will lead to a dorsal bunion and supination deformity. Overpull of the gastrocnemius-soleus complex and posterior tibialis with weakness of the peroneus brevis will cause equinovarus deformity. A strong posterior tibialis with weakness of the peroneals will cause varus of the hindfoot. Unopposed peroneus brevis and incompetence of the posterior tibialis will lead to a flatfoot deformity. The etiology of a cavus foot is complex, but findings usually include a contracted plantar fascia and weakness of the tibialis anterior. Drennan JC (ed): The Child's Foot and Ankle. New York, NY, Raven Press, 1992, pp 289-302.
Question 613
High Yield
A 24-year-old baseball pitcher reports pain over the posterior aspect of his shoulder that occurs only during throwing. He notes that the discomfort is greatest during the late cocking and early acceleration phases. Examination reveals localized tenderness with palpation over the external rotators and posterior glenoid. Radiographs are shown in Figures 38a through 38c. What is the most likely diagnosis?



Explanation
The radiographs show a posterior glenoid osteophyte, often termed a "thrower's exostosis." These exostoses are best visualized on the Stryker notch view and may be missed on other more standard radiographic views of the shoulder. CT and MRI scans may be used, but usually add little information to the radiographic findings. Arthroscopic examination of patients with this condition commonly reveals undersurface tearing of the rotator cuff and posterior labrum. Treatment of this condition remains somewhat controversial, with avocation of both nonsurgical and surgical techniques. Meister K, Andrews JR, Batts J, Wilk K, Baumgarten T, Baumgartner T: Symptomatic thrower's exostosis: Arthroscopic evaluation and treatment. Am J Sports Med 1999;27:133-136. Ferrari JD, Ferrari DA, Coumas J, Pappas AM: Posterior ossification of the shoulder: The Bennett lesion. Etiology, diagnosis, and treatment. Am J Sports Med 1994;22:171-176.
Question 614
High Yield
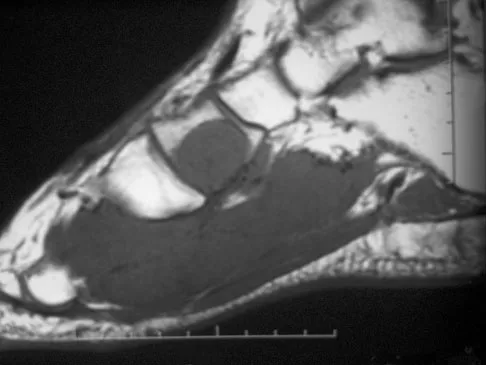
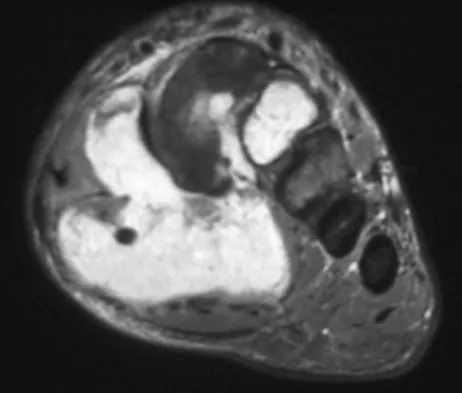
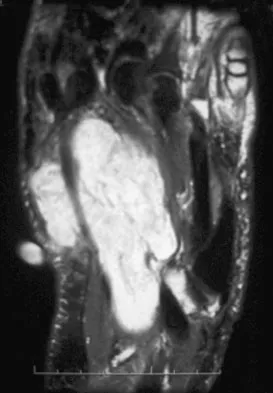
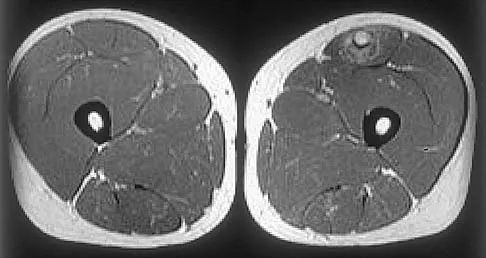
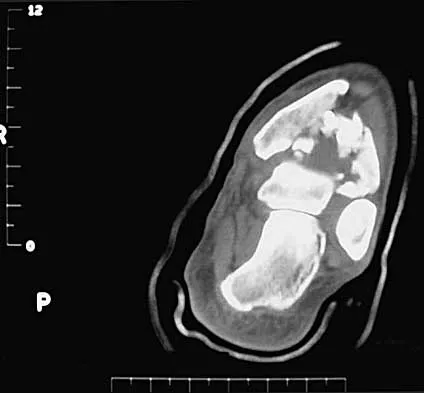
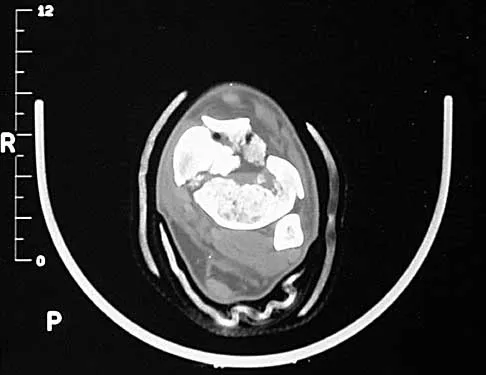
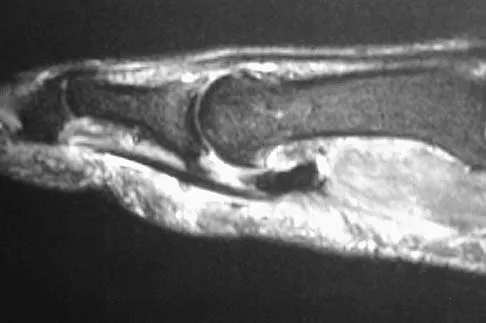
A 39-year-old man has had a foot mass for the past several months. MRI scans are shown in Figures 78a through 78c. A core biopsy specimen reveals synovial sarcoma, and a staging chest CT scan is normal. Which of the following treatments offers the best local tumor control and expedites the patient's return to normal function?
Explanation
Certain histologic subtypes of soft-tissue sarcoma have been noted to arise preferentially in the hand and the foot, such as epithelioid sarcoma, clear cell sarcoma, and synovial sarcoma. Synovial sarcoma is the most common foot sarcoma. Frequently there is a delay in diagnosis because the lesions are rare. The lesions tend to occur in younger adults, typically between the ages of 15 and 40 years. Patients with hand and foot sarcomas have been described as having improved overall survival, but this is likely a result of the smaller size of tumors arising in these locations. In this patient, the tumor has grown to a substantial size and involves many of the bones of the midfoot. Limb salvage may be a possibility when incorporated into a multidisciplinary treatment program, but this will entail months of adjuvant treatment and significant morbidity. Amputation and early prosthetic fitting still have a role in management of some soft-tissue sarcomas, most frequently in the foot. Ferguson PC: Surgical considerations for management of distal extremity soft tissue sarcomas. Curr Opin Oncol 2005;17:366-369.
Question 615
High Yield
During the application of halo skeletal fixation, the most appropriate position for the placement of the anterior halo pins is approximately 1 cm above the superior orbital rim and
Explanation
Halo fixation is the most rigid form of cervical orthosis, but complications can arise from improper placement of the initial halo ring. A relatively safe zone for anterior pin placement is located 1 cm above the orbital rim and superior to the lateral two thirds of the orbit. This position avoids the supraorbital and supratrochlear nerves and arteries over the medial one third of the orbit. The more lateral positions in the temporal fossa have very thin bone and can interfere with the muscles of mastication. Posterior pin site locations are less critical; positioning on the posterolateral aspect of the skull, diagonal to the contralateral anterior pins, is generally desirable. Botte MJ, Byrne TP, Abrams RA, et al: Halo skeletal fixation: Techniques of application and prevention of complications. J Am Acad Orthop Surg 1996;4:44-53.
Question 616
High Yield
A study is being designed to compare the effectiveness of an antibiotic. The choice of the number of patients (ie, the sample size) depends on several factors. What type of calculation assesses the potential of the study to successfully address the effectiveness of the antibiotic?
Explanation
Power analysis is used to determine the minimum number of specimens (sample size) such that, if a difference is found that is large enough to be clinically important, the associated level of statistical reliability will be high enough (ie, the P-value will be small enough) for the investigators to conclude that the difference observed in the study also holds in general. For the statistician to do a power analysis, the investigators must first decide on the minimum difference that they consider to be clinically important, for example, a reduction of 3% in the rate of infection. It is important to recognize that the choice of what constitutes the minimum difference in the rate of infection that is clinically (ie, medically) important cannot and should not be done by the statistician. Rather, this is a clinical-medical issue and must be done by the physician researcher based on a comprehensive assessment of the medical risks and benefits. The power analysis also requires an estimate of the variance in the data, which may be based on previous similar studies, if available. A statistician can then calculate the minimum sample size (number of patients) required such that, if a clinically important difference does, in fact, exist between the full populations, there is a reasonable probability or power (typically 80% to 90%) that a difference this large also will occur between the sample populations at the desired level of statistical significance (usually, but not necessarily, P < 0.05). The other answers refer to types of analyses that are usually conducted after the data are collected.
Question 617
High Yield
A football player sustains a traumatic anterior inferior dislocation of the shoulder in the last game of the season. It is reduced 20 minutes later in the locker room. The patient is neurologically intact and has regained motion. If the patient undergoes arthroscopic evaluation, what finding is seen most consistently?

Explanation
In an acute first-time dislocation, arthroscopy has been shown to reveal a Bankart lesion in most shoulders. The classic finding of labral detachment from the anterior inferior glenoid along with occasional hemorrhage within the inferior glenohumeral ligament is the most common sequelae of a traumatic anterior inferior dislocation. Acute treatment, if chosen, is repair of the labral tissue back to the glenoid plus or minus any capsular plication to address potential plastic deformation of the glenohumeral ligament. Acute treatment of a patient sustaining a first-time dislocation remains controversial. The potential indications may be patients whose dislocation occurs at the end of a season and when the desire to minimize risk of future instability outweighs the risks of surgical intervention. Taylor DC, Arciero RA: Pathologic changes associated with shoulder dislocations: Arthroscopic and physical examination findings in first-time, traumatic anterior dislocations. Am J Sports Med 1997;25:306-311. DeBerardino TM, Arciero RA, Taylor DC, et al: Prospective evaluation of arthroscopic stabilization of acute, initial anterior shoulder dislocations in young athletes: Two- to five-year follow-up. Am J Sports Med 2001;29:586-592.
Question 618
High Yield
Which of the following choices best describes the fracture pattern shown in Figures 2a through 2c?



Explanation
The fracture pattern shown in the radiographs is a fracture of the posterior column. The only line interrupted on the AP pelvis is the ilioischial line. The obturator oblique view shows that the iliopectineal line is intact as is the outline of the posterior wall. The iliac oblique view shows an interruption of the ilioischial line and an intact anterior wall. Therefore, this fracture is a fracture of the posterior column. Letournel E, Judet R: Fractures of the Acetabulum, ed 2. Berlin, Germany, Springer Verlag, 1993.
Question 619
High Yield
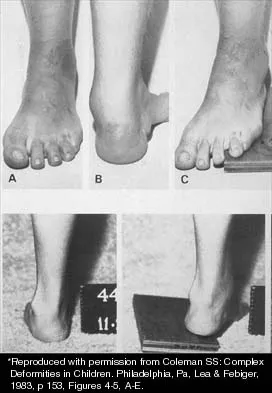
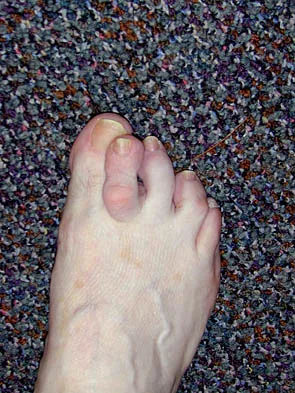
A 15-year-old boy with a type I hereditary sensory motor neuropathy (Charcot-Marie-Tooth disease) reports recurrent ankle sprains and significant pain in the hindfoot and midfoot despite orthotic management. Examination reveals that he walks with a drop foot and has dynamic clawing of the toes. Clinical photographs of the left foot are shown in Figure 7. Management should consist of
Explanation
The clinical photographs show a patient with a type I hereditary sensory motor neuropathy who has cavus feet with a flexible hindfoot. The Coleman block test shows that the hindfoot corrects into valgus. To prevent progressive cavus, patients with this condition may benefit from soft-tissue releases at a younger age while the foot is flexible. Once there is fixed deformity, combined soft-tissue and bone procedures usually are necessary. Metatarsal osteotomies will correct the cavus, but will do nothing for the drop foot. Transfer of the extensor hallucis longus to the neck of the first metatarsal and modified transfer of the extensor digitorum longus to the dorsum of the foot will prevent further claw toes and improve foot dorsiflexion. Anterior transfer of the posterior tibialis tendon will also aid in dorsiflexion. Calcaneal osteotomy should be reserved for fixed hindfoot varus that does not correct with block testing, and triple arthrodesis should be avoided as long as possible because the long-term outcome is poor. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1999, pp 235-245. Coleman SS: Complex Foot Deformities in Children. Philadelphia, Pa, Lea & Febiger, 1983, pp 147-165.
Question 620
High Yield
A 40-year-old woman with no history of back problems has a symptomatic L4-5 disk herniation with an L5 radiculopathy that has failed to respond to 12 weeks of nonsurgical management. In the preoperative discussion, the surgeon advises the patient that the chance of recurrence of the herniation after successful diskectomy is what percent?
Explanation
The incidence of recurrent disk herniation after a successful diskectomy is approximately 5% to 10%. Indications for surgical diskectomy for a recurrence are the same as for a primary diskectomy. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 685-698.
Question 621
High Yield
A 30-year-old elite marathon runner reports chronic pain over the lateral aspect of the distal right leg and dysesthesia over the dorsum of the foot with active plantar flexion and inversion of the foot. Examination reveals a tender soft-tissue fullness approximately 10 cm proximal to the lateral malleolus. The pain is exacerbated by passive plantar flexion and inversion of the ankle. There is also a positive Tinel's sign over the site of maximal tenderness. There is no motor weakness, and deep tendon reflexes are normal. Radiographs and MRI of the leg are normal. What is the next most appropriate step in management?

Explanation
The patient has entrapment of the superficial peroneal nerve against its fascial opening in the distal leg. It is typically exacerbated by passive or active plantar flexion and inversion of the foot, which leads to traction of the nerve as it exits this opening. Treatment involves release of the fascial opening to reduce this traction phenomenon. Closure of the defect will only aggravate the condition and potentially result in an exertional compartment syndrome. A four-compartment fasciotomy is only indicated for an established compartment syndrome of the leg. Styf J: Diagnosis of exercise-induced pain in the anterior aspect of the lower leg. Am J Sports Med 1988;16:165-169. Sridhara CR, Izzo KL: Terminal sensory branches of the superficial peroneal nerve: An entrapment syndrome. Arch Phys Med Rehabil 1985;66:789-791.
Question 622
High Yield
What tendon has an intra-articular (instrasynovial) location in the knee joint?
Explanation
The popliteal tendon arises from the posterior aspect of the tibia and courses through the knee joint through the popliteus hiatus of the lateral meniscus before attaching on the lateral femur anterior to the lateral collateral ligament. It is the only tendon in the knee joint that can be viewed directly on arthroscopy. Kimura M, Shirakura K, Hasegawa A, Kobayashi Y, Udagawa E: Anatomy and pathophysiology of the popliteal tendon area in the lateral meniscus: 1. Arthroscopic and anatomical investigation. Arthroscopy 1992;8:419-423.
Question 623
High Yield
Optimal management of the injury shown in Figure 31 should include which of the following?

Explanation
The radiograph shows a displaced calcaneal beak fracture, a tongue-type fracture variant. The fracture fragment typically includes the insertion point of the Achilles tendon, which places marked tension on the thin overlying soft-tissue envelope and can lead to full-thickness necrosis if not acutely addressed. Cast immobilization does not adequately address the increased soft-tissue tension, as the fragment will be difficult to control. Arthroscopic-assisted techniques or primary arthrodesis are not indicated because calcaneal beak fractures are typically extra-articular. Sanders RW, Clare MP: Fractures of the calcaneus, in Coughlin MJ, Mann RA, Saltzman CL (eds): Surgery of the Foot and Ankle, ed 8. Philadelphia, PA, Mosby-Elsevier, 2007, vol 2, pp 2017-2073.
Question 624
High Yield
Which of the following findings is seen in the chest radiograph shown in Figure 13?

Explanation
Orthopaedic surgeons are often responsible for interpreting radiographs of general examinations such as the chest radiograph shown. For accurate interpretation, it is important to systematically review all of the information available on the radiograph. Using this approach, the fracture of the left proximal humerus is readily recognized. Linear air soft-tissue density at the lung periphery would suggest a pneumothorax, but this finding is not shown on the radiograph. The upper thoracic spine is well aligned. The sternoclavicular and distal clavicles are normal.
Question 625
High Yield
Figure 21 shows the AP radiograph of a 41-year-old patient who sustained a closed bicolumnar fracture of the distal humerus that resulted in a painful nonunion. What is the best initial construct for rigid stabilization of this fracture pattern?

Explanation
The dual plate fixation construct is significantly stronger than single plate or "Y" plate fixation. Two-plate constructs at right angles, the ulnar plate medially and the lateral plate posteriorly, would appear to be biomechanically optimal. This approach usually is feasible at the time of surgery. Clinically, dual 3.5-mm reconstruction or dynamic compression plates are superior to one third tubular plate fixation. Supplementary external fixation is not considered a better treatment option. Failure of fixation and nonunion are often the result of inadequate fixation and osteoporosis. Helfet DL, Hotchkiss RN: Internal fixation of the distal humerus: A biomechanical comparison of methods. J Orthop Trauma 1990;4:260-264.
Question 626
High Yield
Retrograde ejaculation is most commonly associated with what surgical approach?
Explanation
Retrograde ejaculation is the sequela of an injury to the superior hypogastric plexus. This structure needs protection, especially during anterior exposure of the lumbosacral junction. Although the superior hypogastric plexus can be injured with anterior or anterolateral spine surgery at any lumbar level, it is most at risk with anterior transperitoneal approaches to the lumbosacral junction. To avoid this complication, the use of monopolar electrocautery should be avoided during deep dissection in this region. The ideal anterior exposure starts with blunt dissection just to the medial aspect of the left common iliac vein sweeping the prevertebral tissues toward the patient's right side. Flynn JC, Price CT: Sexual complications of anterior fusion of the lumbar spine. Spine 1984;9:489-492. Watkins RG (ed): Surgical Approaches to the Spine. New York, NY, Springer-Verlag, 1983, p 107.
Question 627
High Yield
A 2-year-old girl has had a 2-day history of fever and refuses to move her left shoulder following varicella. Laboratory studies show an erythrocyte sedimentation rate of 75 mm/h and a peripheral WBC count of 18,000/mm3. What is the most common organism in this scenario?

Explanation
The most common bacterial etiologic agent following varicella is group A beta-hemolytic streptococcus. The other organisms are much less common. Staphylococcus aureus is the most common bone infection organism. Staphylococcus epidermidis is increasingly a bone infection organism. Group B streptococcus occurs more commonly in newborns. Kingella kingae is a common joint pathogen but is not as common following varicella. Schreck P, Schreck P, Bradley J, et al: Musculoskeletal complications of varicella. J Bone Joint Surg Am 1996;78:1713-1719.
Question 628
High Yield
A 24-year-old woman fell from a horse and landed on her outstretched right arm. Radiographs reveal an elbow dislocation with a type II coronoid fracture and a nonreconstructable comminuted radial head fracture. What is the most appropriate management?

Explanation
The combination of an elbow dislocation and a fracture of the radial head and coronoid is known as a terrible triad injury. To restore elbow stability, each injury must be addressed. The nonreconstructable radial head fracture requires implant arthroplasty. Open reduction and internal fixation of the coronoid is also necessary as is repair of the lateral collateral ligament complex which is usually avulsed from the lateral epicondyle region. Ring D, Quintero J, Jupiter JB: Open reduction and internal fixation of fractures of the radial head. J Bone Joint Surg Am 2002;84:1811-1815. Ring D, Jupiter JB, Zilberfarb J: Posterior dislocation of the elbow with fractures of the radial head and coronoid. J Bone Joint Surg Am 2002;84:547-551.
Question 629
High Yield
Which of the following studies is considered most sensitive in monitoring a therapeutic response in acute hematogenous osteomyelitis?

Explanation
C-reactive protein declines rapidly as the clinical picture improves. Failure of the C-reactive protein to decline after 48 to 72 hours of treatment should indicate that treatment may need to be altered. Blood culture is positive only 50% of the time and will be negative soon after antibiotics are administered, even if treatment is not progressing satisfactorily. WBC count is highly variable and poorly correlated with treatment. The ESR rises rapidly but declines too slowly to guide treatment. Radiographic findings may not change but can take up to 2 weeks to show changes.
Question 630
High Yield
The patient shown in Figure 44 reports that her toes hurt when she walks. Management should consist of

Explanation
Brachymetatarsia is a congenital hypoplasia of one or more metatarsals. Shortening of the fourth metatarsal is the most common form of brachymetatarsia and is often bilateral. Taping and manipulative reduction attempts are ineffective, and extensor tenotomy and capsulotomy are not likely to sufficiently correct the deformity. Fusion or metatarsal lengthening result in complications and generally are not indicated. Shoe modifications, such as extra-depth or extra-wide shoes, generally will improve symptoms. If pressure and trauma persist in the older child, metatarsal lengthening or amputation may be indicated. Stevens PM: Toe deformities, in Drennan JC (ed): The Child's Foot and Ankle. New York, NY, Raven Press, 1992, p 195.
Question 631
High Yield
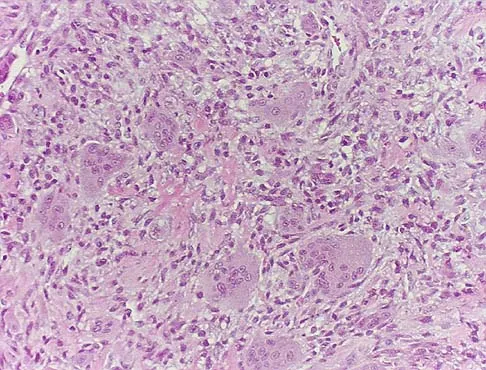
A 20-year-old patient has foot pain. A radiograph and T1-weighted MRI scan are shown in Figures 8a and 8b. A biopsy specimen is shown in Figure 8c. Treatment should consist of


Explanation
Giant cell tumors occur near articular surfaces in young adults. The histology shows abundant giant cells with nuclei resembling the surrounding cells. Although the MRI scan shows soft-tissue involvement, curettage is still the preferred treatment. Chemotherapy is not necessary for benign lesions, and amputation is too aggressive. Cementation, phenol, and cryosurgery (liquid nitrogen) are all acceptable local adjuvants to curettage. Packing the cavity with bone graft rather than cement is also acceptable. Dahlin DC, Unni KK: Bone Tumors: General Aspects and Data on 8,542 Cases. Springfield, IL, Charles C. Thomas, 1986.
Question 632
High Yield
A 9-year-old girl reports the immediate onset of severe groin pain and the inability to walk after tripping on a curb. Examination reveals marked hip pain with passive range of motion. A radiograph is shown in Figure 21. Regardless of treatment, what is the most common complication following this injury?

Explanation
The patient has an unstable slipped capital femoral epiphysis (SCFE). According to the classification system based on physeal stability, an unstable SCFE is one in which the patient is unable to walk, even with crutches. Ishemic necrosis, or osteonecrosis, of the femoral head is the most devastating complication of SCFE. One study found a 47% incidence of ischemic necrosis following unstable slips. This complication is most likely the result of vascular injury associated with initial femoral head displacement rather than the result of either tamponade from joint effusion or gentle repositioning prior to stabilization. Chondrolysis is a relatively uncommon complication following treatment of SCFE. This complication has been associated with persistent penetration of the hip joint with screws or pins used to stabilize the femoral head or with spica cast immobilization. There are no reports to suggest that osteochondritis dissecans, nonunion, or coxa magna follows treatment of SCFE. Loder RT, Richards BS, Shapiro PS, et al: Acute slipped capital epiphysis: The importance of physeal stability. J Bone Joint Surg Am 1993;75:1134-1140.
Question 633
High Yield
Which of the following findings is considered the strongest indication for surgical treatment of a mallet fracture of the distal phalanx?
Explanation
The majority of mallet fractures can be treated nonsurgically with a distal interphalangeal joint extension splint. Excellent results can be obtained in most patients with splinting alone. The fragment size, amount of displacement, and degree of articular incongruity usually do not affect final outcome, as long as the joint is reduced. Surgical fixation takes on several forms but is fraught with complications including skin/wound problems, loss of fixation, nonunion, and stiffness of the distal interphalangeal joint. Volar subluxation of the distal phalanx remains the primary indication for surgical treatment. Green DP, Butler TE Jr: Fractures and dislocations in the hand, in Rockwood CA, Green DP, Bucholz RW, Heckman JD (eds): Rockwood and Green's Fractures in Adults, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 621-623.
Question 634
High Yield
An 11-year-old boy stepped on a nail and sustained a puncture to the right forefoot 6 days ago. He was wearing tennis shoes at the time of injury. Treatment in the emergency department consisted of local debridement and tetanus prophylaxis; a radiograph was negative for foreign body, chondral defect, or fracture. He was discharged with a 3-day prescription of amoxicillin and clavulanate. The patient now has increasing pain and tenderness at the puncture site. What is the best course of action?
Explanation
The initial treatment consisting of oral antibiotics was appropriate but with progressive symptoms, surgical debridement is necessary. Ciprofloxacin is contraindicated in children, and at this stage, oral antibiotics are inadequate. Intravenous antibiotics may be necessary, but surgical debridement is paramount. Failure to respond to the initial management precludes further observation. Riegler HP, Routson T: Complications of deep puncture wounds of the foot. J Trauma 1979;19:18-22.
Question 635
High Yield
Mutations of what gene are associated with subsequent development of osteosarcoma?
Explanation
The mutation of the retinoblastoma gene has been associated with an increased prevalence of osteosarcoma. The mutation resulting in EWS-FLI1 is associated with Ewing's sarcoma. The other mutations are associated with tumor formation and proliferation but not necessarily with osteosarcoma formation. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 4. Scholz R, Kabisch H, Delling G, Winkler K: Homozygous deletion within the retinoblastoma gene in a native osteosarcoma specimen of a patient cured of a retinoblastoma of both eyes. Pediatr Hematol Oncol 1990;72:65.
Question 636
High Yield
What are the most common portals for arthroscopic surgery of the ankle?

Explanation
The most commonly used portals are the anterolateral, anteromedial, and posterolateral portals. They have been shown to be the safest areas for portal placement, allowing no penetration of neurovascular structures. All the other portals involve placing another structure at risk. The anterocentral portal is close to the deep peroneal nerve and anterior tibular artery. The trans-Achilles portal is not recommended because of its limited utility and potential to injure the Achilles tendon. The posteromedial portal is too close to the posterotibial artery and nerve, the flexor hallucis longus and flexor digitorum longus tendons, and the branches of the calcaneal nerve. Stetson WB, Ferkel RD: Ankle arthroscopy: I. Technique and complications. J Am Acad Orthop Surg 1996;4:17-23.
Question 637
High Yield
Which of the following factors is associated with the worst prognosis in soft-tissue sarcomas?

Explanation
Although factors such as a high-grade tumor and large size are associated with decreased survival, the presence of metastases carries the worst prognosis. Good results are very rare when metastases are present. Soft-tissue sarcomas, as a whole, respond poorly to chemotherapy, leading to a poor prognosis when metastases are present. Collin C, Goobold J, Hadju SI, Brennan MF: Localized extremity soft tissue sarcoma: An analysis of factors affecting survival. J Clin Oncol 1987;5:601-612.
Question 638
High Yield
When compared with fresh-frozen bone allograft, freeze-dried bone allograft (FDBA) is characterized by
Explanation
The compaction of FDBA is faster than that of fresh-frozen bone. The maximal stiffness reached by both materials when tested was the same (55 MPa), but the FDBA required fewer impactions to achieve that stiffness. Because it is easier to impact, the FDBA may be mechanically more efficient than the fresh-frozen bone in surgical conditions. The brittleness of irradiated FDBA, caused by loss of the capacity to absorb energy in a plastic way, increases the compactness and stiffness of morcellized grafts. The failure rate of fusion in adolescent idiopathic scoliosis has been shown to be much higher in FDBA than in either iliac crest bone graft or composite autograft with demineralized bone matrix. There is a greater erosive surface response to allograft when compared to autograft or frozen allograft, with a larger number of osteoclast and osteoblast nuclei seen microscopically. Cornu O, Libouton X, Naets B, et al: Freeze-dried irradiated bone brittleness improves compactness in an impaction bone grafting model. Acta Orthop Scand 2004;75:309-314. Price CT, Connolly JF, Carantzas AC, et al: Comparison of bone grafts for posterior spinal fusion in adolescent idiopathic scoliosis. Spine 2003;28:793-798.
Question 639
High Yield
Figure 9 shows the radiograph of a 75-year-old woman who reports the sudden onset of disabling medial knee pain. What is the most likely diagnosis?

Explanation
Idiopathic osteonecrosis of the medial femoral condyle occurs predominantly in women older than age 60 years. It is characterized by pain centered in the medial anterior aspect of the knee, and onset is sudden. Flattening, sclerosis, and the radiolucent crescent sign are radiographic indicators of osteonecrosis. The radiographs show no narrowing of the joint space or osteophyte formation to indicate osteoarthritis, and there are no loose bodies to indicate synovial osteochondromatosis. A meniscal tear is not consistent with the radiographic findings shown here. Meniscal tears can coexist with osteonecrosis, but the pain is not eliminated merely by partial meniscectomy. Metastatic lesions to the distal femoral epiphysis are exceedingly rare. Urbaniak JR, Jones JP Jr (eds): Osteonecrosis: Etiology, Diagnosis, and Treatment. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 413-418.
Question 640
High Yield
Mutations of what gene are associated with the subsequent development of osteosarcoma?
Explanation
Patients with a mutation of the retinoblastoma gene (RB) have an increased likelihood for the development of osteosarcoma. The EWS-FLI1 gene is the fusion product of a chromosomal translocation of 11:22. EGF-R and IGF-R are growth factor receptors, but mutations in these genes have not been correlated with osteosarcoma. VEGF is a proangiogenic molecule that is involved in tumor formation in multiple sites but not the development of osteosarcoma. Scholz RB, Kabisch H, Delling G, et al: Homozygous deletion within the retinoblastoma gene in a native osteosarcoma specimen of a patient cured of a retinoblastoma of both eyes. Pediatr Hematol Oncol 1990;7:265-273.
Question 641
High Yield
A 79-year-old woman reports a history of left leg pain with walking. Her pain is exacerbated with walking and stair climbing, and her symptoms are improved by standing after she stops walking. Lumbar flexion does not provide any significant improvement of the symptoms and sitting does not significantly change symptoms. Her leg pain is worse at night and she obtains relief by hanging her leg over the side of the bed. The neurologic examination is essentially normal. Examination of the lower extremities demonstrates mild early trophic changes, and her pulses distally are palpable but are diminished bilaterally. Radiographs are shown in Figures 15a and 15b. What is the next most appropriate step in management?


Explanation
The patient has symptoms that are more consistent with vascular claudication than with the pseudoclaudication anticipated from lumbar spinal stenosis. Therefore, the patient is a candidate for further vascular work-up. The radiographs reveal early spinal stenosis and spondylolisthesis at L4-5 but also show significant calcification of the iliac arteries, suggestive of peripheral vascular disease. Vascular claudication is a manifestation of peripheral vascular disease and presents with crampy leg pain that is exacerbated by physical exertion. The pain is easily relieved by standing still or sitting. Unlike pseudoclaudication, a forward-flexed posture and/or sitting does not improve the symptoms. Night pain is common in vascular claudication due to the elevation of the extremities and patients often report pain improvement by hanging their extremities in a dependent position. In evaluation of a patient with suspected vascular claudication, the five "P's" of vascular insufficiency should be monitored, including pulselessness, paralysis, paresthesia, pallor, and pain. While pain and paresthesias can be common in both vascular claudication and pseudoclaudication, the presence of any of the remaining symptoms is suggestive of vascular disease. Aufderheide TP: Peripheral arteriovascular disease, in Rosen P, Barkin R (eds): Emergency Medicine: Concepts and Clinical Practice, ed 4. St Louis, MO, Mosby, 1998, pp 1826-1844.
Question 642
High Yield
What is the known manner in which the growth hormone-insulin-like growth factor-I (GH-IGF-I) system functions to stimulate bone growth?
Explanation
IGF-I, formerly known as somatomedin-C, possibly acts by both paracrine and endocrine hormone pathways. The products of the GH-IGF-I system induce proliferation without maturation of the growth plate and thus induce linear skeletal growth. The action of the thyroid hormone axis is via an active metabolite that enters target cells and signals a nuclear receptor to stimulate both proliferation and maturation of the growth plate. Increased amounts of the active steroid hormone metabolite promote proliferation and maturation of the growth plate. Calcitonin inhibits bone resorption. Binder G, Grauer ML, Wehner AV, et al: Outcome in tall stature: Final height and psychological aspects in 220 patients with and without treatment. Eur J Pediatr 1997;156:905-910. Wang J, Zhou J, Cheng CM, et al: Evidence supporting dual, IGF-I-independent and IGF-I-dependent, roles for GH in promoting longitudinal bone growth. Endocrinol 2004;180:247-255.
Question 643
High Yield
A 22-year-old college baseball pitcher reports the recent onset of anterior and posterosuperior shoulder pain in his throwing shoulder. Examination shows a 15-degree loss of internal rotation, tenderness over the coracoid, and a positive relocation test. Radiographs are normal, and an MRI scan without contrast shows no definitive lesions. A rehabilitation program is prescribed. Which of the following regimens should be initially employed?
Explanation
Throwing athletes, particularly pitchers, have a high incidence of shoulder pain. Recent evidence suggests that posteroinferior capsular tightness and scapular dyskinesis may play a substantial role in the pathologic cascade, culminating in the development of articular surface rotator cuff tears and tearing of the posterosuperior labrum. These patients have posterosuperior shoulder pain primarily. Furthermore, these athletes are susceptible to a muscular fatigue syndrome, the SICK (Scapular malposition, Inferior medial border prominence, Coracoid pain and malposition, and dysKinesis of scapular movement) scapula syndrome. This patient has an internal rotation deficit and tenderness over the coracoid. The internal rotation deficit is addressed by stretching the posterior capsule. The tenderness over the coracoid has been attributed to a contracture of the pectoralis minor tendon secondary to scapular malposition. The initial phase of the rehabilitation regimen is directed at stretching the posterior capsule and pectoralis minor tendon. Burkhart SS, Morgan CD, Kibler WB: The disabled throwing shoulder: Spectrum of pathology. Part III. Arthroscopy 2003;19:641-661.
Question 644
High Yield
The palmar cutaneous branch of the median nerve (PCBMN) originates from the
Explanation
The PCBMN originates from the median nerve proper between 3 and 21 cm proximal to the wrist with moderate variation. It virtually always originates from the radial side of the nerve and travels distally with the median nerve, radial to the palmaris longus, and ulnar to the flexor carpi radialis. Hobbs RA, Magnussen PA, Tonkin MA: Palmar cutaneous branch of the median nerve. J Hand Surg Am 1990;15:38-43.
Question 645
High Yield
Figure 40 shows the radiograph of a 16-year-old wrestler who injured his elbow when he was thrown to the mat by his opponent. Closed reduction is readily accomplished, and the elbow seems stable. Management should now consist of application of a splint for

Explanation
Flexion contractures are the most common complication of elbow dislocations. About 15% of patients lose more than 30 degrees of flexion. The risk of contracture is proportional to the duration of immobilization. Elbows should be moved within the first few days after reduction. The splinting is for comfort and protection only while the pain subsides. Mehlhoff TL, Noble PC, Bennett JB, Tullos HS: Simple dislocation of the elbow in the adult: Results after closed treatment. J Bone Joint Surg Am 1988;70:244-249. Linscheid RL, O'Driscoll SW: Elbow dislocations, in Morrey BF (ed): The Elbow and Its Disorders, ed 2. Philadelphia, PA, WB Saunders, 1993, pp 441-452. O'Driscoll SW, Jupiter JB, King GJ, Hotchkiss RN, Morrey BF: The unstable elbow. Instr Course Lect 2001;50:89-102.
Question 646
High Yield
A 32-year-old man sustained a closed injury after falling 25 feet from a roof. His ankle and foot are severely swollen. Radiographs and CT scans are shown in Figures 29a through 29d. Initial management should consist of


Explanation
The patient has a severe high-energy injury from axial loading to the left ankle and distal tibia. This is a closed injury, but the soft tissues are injured and severely swollen. Initial treatment should focus on skeletal stabilization, and incisions directly over the fracture area should be avoided until soft-tissue stabilization has occurred. Immediate spanning external fixation with plans for a delayed reconstruction as needed for the joint surface is the treatment of choice. Closed reduction and application of a constrictive long leg cast may lead to increased risk of tissue necrosis. Immediate open procedures to internally fix the fracture add the risks of soft-tissue necrosis and are to be avoided. Percutaneous plating may be one of the delayed fixation options but should not be used immediately. Primary ankle arthrodesis is not indicated. Thordarson DB: Complications after treatment of tibial pilon fractures: Prevention and management strategies. J Am Acad Orthop Surg 2000;8:253-265. Marsh JL, Bonar S, Nepola JV, DeCoster TA, Hurwitz SR: Use of an articulated external fixator for fractures of the tibial plafond. J Bone Joint Surg Am 1995;77:1498-1509.
Question 647
High Yield
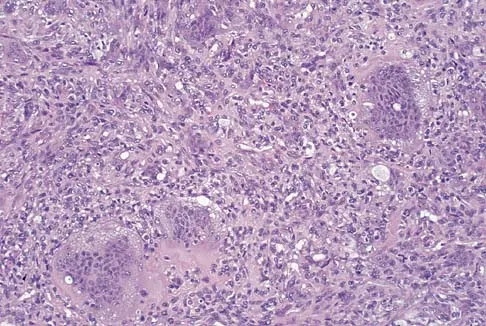
A 34-year-old woman reports constant midlateral arm pain after sustaining minimal trauma to the shoulder. Radiographs and a biopsy specimen are shown in Figures 29a and 29b. What is the most likely diagnosis?

Explanation
Eighty percent of giant cell tumors occur in patients older than age 20 years, with the peak incidence in the third decade of life. Most of these tumors are eccentrically located and epiphyseal in location. They are lytic in nature as in this patient. Although named for the hallmarked multinucleated giant cells seen in the lesion, the basic cell type is the spindle-shaped stromal cell. Chondroblastoma is highly cellular and contains large multinucleated giant cells with intercellular chondroid material, some of which is calcified. Chondromyxoid fibroma has chondroid tissue separated by strands of more cellular tissue with occasional multinucleated giant cells. Desmoplastic fibroma is characterized by poorly cellular fibrous tissue, and lymphoma is highly cellular with characteristic round cells. Campanacci M, Baldini N, Boriani S, et al: Giant cell tumor of bone. J Bone Joint Surg Am 1987;69:106-114.
Question 648
High Yield
Which of the following symptoms are most commonly associated with piriformis syndrome?
Explanation
Piriformis syndrome is best characterized by localized posterior hip pain and radicular symptoms in the sciatic distribution because of compression of the piriformis muscle on the sciatic nerve. Weakness in hip extension is not a characteristic finding, nor is pain with hip abduction or flexion. Hypesthesia of the lateral thigh would be more characteristic of a lesion of the lateral femoral cutaneous nerve. Radiating medial thigh pain would suggest hip joint pathology or upper lumbar nerve root irritation. Weakness in internal rotation is not a characteristic feature, and hypesthesia of the perineum would suggest possible involvement of the pudendal nerve. Byrd JWT: Thigh, hip, and pelvis, in Miller MD, Cooper DE, Warner JJP (eds): Review of Sports Medicine and Arthroscopy, ed 2. Philadelphia, PA, WB Saunders, 2002, pp 114-139.
Question 649
High Yield
A 25-year-old man sustained an L1 compression fracture in a fall from his roof. He is neurologically intact and has no other injuries. Radiographs reveal a 25% loss of height anteriorly and 5 degrees of kyphosis at the fracture site. A CT scan reveals no compromise of the posterior column. Management should consist of
Explanation
The patient has a stable fracture that can be initially treated with bed rest, followed by bracing and quick mobilization. The outcome is good and surgery is not required. These fractures can be treated nonsurgically if there is less than 50% compression, 15 degrees of angulation, and intact posterior structures. Cantor JB, Lebwohl NH, Garvey T, Eismont FJ: Nonoperative management of stable thoracolumbar burst fractures with early ambulation and bracing. Spine 1993;18:971-976.
Question 650
High Yield
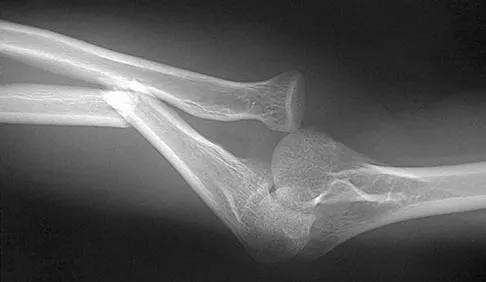
Figure 2 shows the radiograph of a 26-year-old auto mechanic who injured his right dominant elbow in a fall during a motocross race. Examination reveals pain and catching that limits his range of motion to 45 degrees of supination and 20 degrees of pronation. The interosseous space and distal radioulnar joint are stable. Management should consist of

Explanation
The radial head is an important secondary stabilizer of the elbow, helping to resist valgus forces. There has been a movement toward open reduction and internal fixation of the radial head when technically feasible, especially in a relatively high-demand athlete or laborer. The examination and radiograph suggest that displacement of the fragment is great enough to create a mechanical block. Extended splinting would only serve to encourage arthrofibrosis. Early range of motion is appropriate if there is minimal displacement of the radial head fragement, it is stable, and there is no mechanical block to motion. Fragments larger than one third of the joint surface should be excised only if it is not possible to reduce and repair the fragment. Primary excision of the radial head should be avoided if possible. Complications after excision of the radial head include muscle weakness, wrist pain, valgus elbow instability, heterotopic ossification, and arthritis. Hotchkiss RN: Displaced fractures of the radial head: Internal fixation or excision? J Am Acad Orthop Surg 1997;5:1-10.
Question 651
High Yield
A 70-year-old golfer has pain in her dominant shoulder. She reports that initially the pain was at night but now she is unable to play. Examination reveals weakness in external rotation and shoulder abduction. Radiographs reveal the humeral head articulating with a thin acromion. Management should consist of

Explanation
Chronic rotator cuff tears should be nonsurgically managed initially with a strengthening program. A cortisone injection may reduce inflammation. Surgery is reserved for patients who continue to have pain and lose sleep despite the use of physical therapy. Blood tests for infection or inflammation are nonspecific. Arthroscopy may play a role, but surgical replacement is reserved for advanced cases. Bokor DJ, Hawkins RJ, Huckell GH, et al: Results of nonoperative management of full-thickness tears of the rotator cuff. Clin Orthop 1993;294:103-110.
Question 652
High Yield
A knock-out mouse for the Vitamin D receptor has which of the following phenotypes?
Explanation
A knock-out mouse to the Vitamin D receptor would cause loss of vitamin D function, resulting in rickets. Renal failure would not occur; although Vitamin D is converted from 25 (OH) D to 1,25 (OH) D in the kidney, the active hormone acts on the gut and bone. Osteopetrosis can be seen as the phenotype for the c fos knock-out mouse; the Jansen-type metaphyseal dysplasia phenotype results from overactivation of the PTH/PTHrp receptor. Although compensatory hyperparathyroidism would occur, excessive PTH would not be able to rescue the skeletal loss and instead phosphoturia and phosphotasia would result. Glowacki J, Hurwitz S, Thornhill TS, et al: Osteoporosis and vitamin-D deficiency among postmenopausal women with osteoarthritis undergoing total hip arthroplasty. J Bone Joint Surg Am 2003;85:2371-2377.
Question 653
High Yield
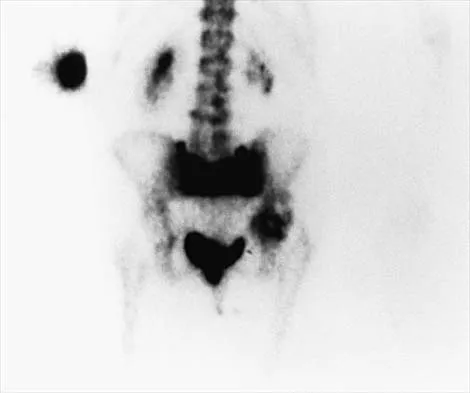
Figure 7 shows the AP radiograph of a 60-year-old man who has had pain in the thigh for past 6 months. History reveals that he underwent hip replacement 1 year ago. The radiographic changes are most likely the result of what process?

Explanation
The arrows in the radiograph point to circumferential radiolucencies that strongly support the diagnosis of septic loosening. Radiolucent lines that occur in such a short time are also typical of an infection. Garvin KL, Hanssen AD: Infection after total hip arthroplasty: Past, present, and future. J Bone Joint Surg Am 1995;77:1576-1588.
Question 654
High Yield
What is the most likely consequence of a vertebral compression fracture associated with osteoporosis?
Explanation
After an osteoporotic vertebral compression fracture, the risk of subsequent fractures at adjacent levels increases. This is felt to be the result of a shifting of the sagittal alignment more anteriorly, putting more stress on the osteopenic vertebral bodies and their anterior cortices. Pain generally resolves with rest, but this may take weeks or months. It has been demonstrated experimentally that osteoporotic vertebral bodies are actually less stiff and weaker after a compression fracture; therefore, deformity predisposes to further deformity. The extensor musculature often fatigues over time and usually does not hypertrophy. Frontal plane deformity is a rare development. Heaney RP: The natural history of vertebral osteoporosis: Is low bone mass an epiphenomenon? Bone 1992;13:S23-S26.
Question 655
High Yield
A 13-year-old boy hyperextends his knee while playing basketball and reports a pop that is followed by a rapid effusion. A lateral radiograph is shown in Figure 4. Initial management consists of attempted reduction with extension, with no change in position of the fragment. What is the next most appropriate step in management?

Explanation
Avulsion fractures of the tibial spine are rare injuries that result from rapid deceleration or hyperextension of the knee in skeletally immature individuals. This injury is the equivalent of ruptures of the anterior cruciate ligament in adults. These fractures are classified as types 1 through 3. Type 1 is a minimally displaced fracture, type 2 fractures have an intact posterior hinge, and type 3 fractures have complete separation. The radiograph demonstrates a completely displaced, or type III, tibial spine avulsion. Surgical reduction is indicated in type 2 fractures that fail to reduce with knee extension and in all type 3 fractures. Reduction may be arthroscopic or open, with fixation of the bony fragment using a method that maintains physeal integrity and prevents later growth arrest. Preferred techniques would be with suture or an intra-epiphyseal screw Wiley JJ, Baxter MP: Tibial spine fractures in children. Clin Orthop 1990;255:54-60. Mulhall KJ, Dowdall J, Grannell M, et al: Tibial spine fractures: An analysis of outcome in surgically treated type III injuries. Injury 1999;30:289-292. Owens BD, Crane GK, Plante T, et al: Treatment of type III tibial intercondylar eminence fractures in skeletally immature athletes. Am J Orthop 2003;32:103-105.
Question 656
High Yield
In the majority of patients with chronic anterior cruciate ligament (ACL)-deficient knees, analysis of the gait pattern during level walking will most likely reveal which of the following changes?
Explanation
Patients with chronic ACL-deficient knees typically have lower than normal net quadriceps activity during the middle portion of the stance phase; the net moment about the knee reverses from one that demands quadriceps activity to one that demands increased hamstring activity. This type of gait is termed "quadriceps avoidance." This avoidance is believed to be a functional adaptation to reduce anterior tibial translation, and it is most prevalent as the knee moves from 45 degrees of flexion toward full extension, the arc of motion through which the ACL is most responsible for stability. Hurwitz DE, Andriacchi TP, Bush-Joseph CA, Bach BR Jr: Functional adaptations in patients with ACL-deficient knees. Exerc Sport Sci Rev 1997;25:1-20. Andriacchi TP, Birac D: Functional testing in the anterior cruciate ligament-deficient knee. Clin Orthop 1993;288:40-47.
Question 657
High Yield
A 58-year-old woman with rheumatoid arthritis has progressive neck pain, upper extremity and lower extremity weakness, and difficulty with fine motor movements. Examination reveals hyperreflexia with mild to moderate objective weakness but the patient has no difficulty with ambulation for short distances. What is the most important preoperative imaging finding that predicts full neurologic recovery with surgical stabilization?
Explanation
Boden and associates' article presents compelling evidence that patients with rheumatoid arthritis and neurologic deterioration in C1-2 instability are more likely to achieve some improvement if the posterior atlanto-dens interval is greater than 10 mm on preoperative studies. All the patients in their series who had neurologic deterioration and a preoperative posterior atlanto-dens interval of greater than 14 mm achieved complete motor recovery. Boden SD, Dodge LD, Bohlman HH, et al: Rheumatoid arthritis of the cervical spine: A long-term analysis with predictors of paralysis and recovery. J Bone Joint Surg Am 1993;75:1282-1297. Boden SD, Clark CR: Rheumatoid arthritis of the cervical spine, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 755-764.
Question 658
High Yield
Locked plating techniques have been shown to have biomechanical advantages over standard plating in which of the following scenarios?
Explanation
Locked plating is becoming more common. Some biomechanical data comparing locked plating to standard plating have been reported for osteoporotic distal femoral fractures and humeral shaft fractures. Significant differences were seen mainly for osteoporotic fractures without cortical contact. Not all osteoporotic fractures and all comminuted fractures have been shown to demonstrate significant mechanical improvement with locked plating compared to standard plating. Spiral fractures often can be repaired with a lag screw, obtaining adequate cortical contact. Osteoporotic fractures with a torsion mode of failure failed earlier with locked plating systems than with standard plating systems. Zlowodzki M, Williamson S, Cole PA, et al: Biomechanical evaluation of the less invasive stabilization system, angled blade plate, and retrograde intramedullary nail for the internal fixation of distal femur fractures. J Orthop Trauma 2004;18:494-502.
Question 659
High Yield
A 50-year-old electrician who is right-hand dominant has had right shoulder pain and stiffness after sustaining an electric shock 2 months ago. An AP radiograph obtained at the time of injury was considered negative, and the patient was diagnosed with a shoulder sprain. The patient now reports continued shoulder pain and restricted motion. AP and axillary radiographs and a CT scan are shown in Figures 41a through 41c. Management should consist of



Explanation
Open reduction and transfer of the subscapularis and lesser tuberosity into the humeral head defect is the treatment of choice for chronic posterior dislocations in which the articular defect consists of 20% to 40% of the articular surfaces. Closed reduction can be used if the dislocation is recognized early and the articular defect is less than 20% of the articular surface. Humeral arthroplasty is reserved for patients with an articular defect that is greater than 45% to 50% of the head. Hawkins RJ, Neer CS II, Pianta RM, Mendoza FX: Locked posterior dislocation of the shoulder. J Bone Joint Surg Am 1987;69:9-18.
Question 660
High Yield
A 42-year-old man undergoes right total hip arthroplasty for hip dysplasia. Postoperatively, he has a significant limb-length increase with a foot drop. A preoperative radiograph is shown in Figure 19. Which of the following should have been considered preoperatively to avoid this complication?

Explanation
In a patient with bilateral hip dysplasia, there are significant technical challenges that need to be addressed to ensure a successful total hip arthroplasty. Restoring the center of the hip may cause significant lengthening and require femoral shortening. Lengthening of greater than 4 cm can lead to sciatic nerve palsy that will present clinically as a foot drop. A high hip center can be used when there is inadequate bone stock in the acetabulum to achieve adequate host bone coverage. A modular femoral implant may be used for a dysplastic hip with significant rotational deformity. Although an anterolateral approach to the hip may decrease the incidence of sciatic nerve palsy during the exposure, it will not be helpful when there is more than 4 cm of limb lengthening. Schmalzried TP, Amstutz HC, Dorey FJ: Nerve palsy associated with total hip replacement: Risk factors and prognosis. J Bone Joint Surg Am 1991;73:1074-1080. Papagelopoulos PJ, Trousdale RT, Lewallen DG: Total hip arthroplasty with femoral osteotomy for proximal femoral deformity. Clin Orthop 1996;332:151-162.
Question 661
High Yield
Reconstruction of the posterior cruciate ligament (PCL) via the inlay technique involves exposure of the PCL tibial insertion site by a posterior
Explanation
The posterior medial approach through the semimembranosus/medial gastrocnemius interval is used in the inlay technique for PCL reconstruction. Exposure of the posterior capsule of the knee through this interval provides the greatest margin of safety to avoid injury to the tibial nerve, motor branch of the medial gastrocnemius, and the peroneal nerve. The direct posterior approach using the medial sural cutaneous nerve allows exposure of the popliteal neurovascular structures, but deep dissection through this interval places the motor branch of the medial gastrocnemius at risk. The interval between the semitendinosus and semimembranosus is used in accessory incisions with medial meniscus repairs but does not allow exposure of the PCL insertion. Berg EE: Posterior cruciate tibial inlay reconstruction. Arthroscopy 1995;11:69-76.
Question 662
High Yield
What procedure can eliminate a sulcus sign?
Explanation
A sulcus sign represents inferior subluxation of the shoulder. The elimination of this sign and correction of the inferior subluxation is best achieved through either an open or arthroscopic rotator interval closure. A SLAP repair stabilizes the biceps anchor but does not affect the sulcus sign. A Bankart repair, which corrects anterior-inferior laxity, is not sufficient to eliminate a sulcus sign. Subacromial decompression and supraspinatus repairs have no effect on inferior subluxation. Field LD, Warren RF, O'Brien SJ, et al: Isolated closure of rotator interval defects for shoulder instability. Am J Sports Med 1995;23:557-563.
Question 663
High Yield
What is the most common complication following arthroscopic capsular release in a patient with adhesive capsulitis of the shoulder?

Explanation
Although all of the above are potential complications after arthroscopic capsular release for adhesive capsulitis, the most common problem is the failure to regain normal glenohumeral motion. An immediate physical therapy program is critical to prevent this complication. Ghalambor N, Warner JJP: Arthroscopic capsular release: Evolution of the technique and its applications. Tech Shoulder Elbow Surg 2000;1:52-60.
Question 664
High Yield
An 82-year-old woman reports right buttock pain after a car trip. Laboratory studies show an erythrocyte sedimentation rate of 30 mm/h and WBC of 4,600/mm3. Figure 34a shows a plain AP radiograph of the pelvis, and Figure 34b shows a delayed technetium Tc 99m bone scan. Management should consist of

Explanation
The radiograph shows bilateral cemented total hip arthroplasties. The acetabular components are loose bilaterally, but there has been no acute change. Therefore, it is unlikely that the acetabular loosening is contributing to the patient's pain. The bone scan is consistent with a sacral insufficiency fracture. This is best treated with bed rest and pain medication. Activity can be increased as the pain allows. Revision will not address the pain. Newhouse KE, el-Khoury GY, Buckwalter JA: Occult sacral fractures in osteopenic patients. J Bone Joint Surg Am 1992;74:1472-1477.
Question 665
High Yield
What type of brace is shown in Figures 22a and 22b?
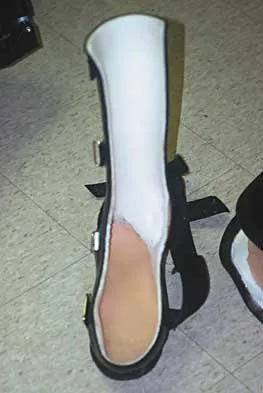

Explanation
The figures show a Charcot restraining orthotic walker (CROW). This brace has been used as a customized total contact fit removable brace to maintain foot alignment as the patient evolves from Eichenholz stage 1 to Eichenholz stage 3 Charcot arthropathy. Mehta JA, Brown C, Sargeant N: Charcot restraint orthotic walker. Foot Ankle Int 1998;19:619-623.
Question 666
High Yield
Which of the following best describes the use of epidural morphine and steroid paste after laminectomy?

Explanation
Kramer and associates conducted a retrospective review during an "epidemic" period to identify the risk factors associated with a sudden increase in the rate of surgical site infections. They found in a multivariate analysis that the use of morphine nerve paste resulted in a 7.6-fold increase in postoperative surgical wound debridement, and an 11% rate of surgical site complications. Kramer MH, Mangram AJ, Pearson ML, et al: Surgical-site complications associated with a morphine nerve paste used for postoperative pain control after laminectomy. Infect Control Hosp Epidemiol 1999;20:183-186.
Question 667
High Yield
For patients undergoing a surgical procedure where the risk of requiring a transfusion is less than 10%, the International Committee of Effective Blood Usage suggests

Explanation
Recent studies have shown a high rate of waste of autologous blood. Therefore, the Committee does not recommend autologous blood donation for procedures that carry a transfusion risk of 10% or less. Toy P, Beattie C, Gould S, et al: Transfusion alert: Use of autologous blood. National Heart, Lung, and Blood Institute Expert Panel on the use of autologous blood. Transfusion 1992;35:703-711.
Question 668
High Yield
A sentinel event is defined as an unexpected occurrence involving death or serious physical or psychological injury, or the risk thereof. What is the most common sentinel event related to spine surgery?
Explanation
Patient safety and prevention of medical errors is a major focus of recent national advocacy groups. Analysis has shown that the most common sentinel event in spine surgery is surgery on the wrong level. Therefore, it is recommended that every patient have the surgical site signed, the level of surgery marked intraoperatively, and a radiograph taken. Surgery on the wrong level is most likely to occur in single-level decompressive procedures. Wong DA, Watters WC III: To err is human: Quality and safety issues in spine care. Spine 2007;32:S2-S8.
Question 669
High Yield
A 9-year-old child sustains a proximal tibial physeal fracture with a hyperextension mechanism. What structure is at most risk for serious injury?
Explanation
The most serious injury associated with proximal tibial physeal fracture is vascular trauma. The popliteal artery is tethered by its major branches near the posterior surface of the proximal tibial epiphysis. During tibial physeal displacement, the popliteal artery is susceptible to injury. Injuries to the other structures are less common.
Question 670
High Yield
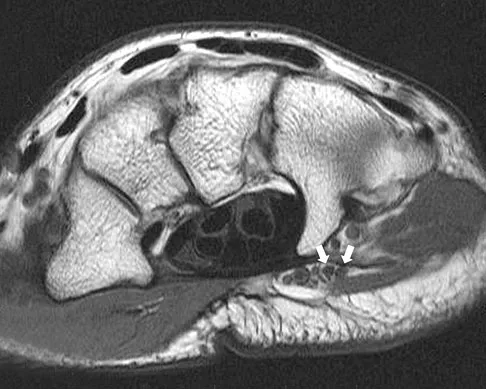
A patient notes pain under the first metatarsophalangeal joint following a soccer injury. The MRI scans shown in Figures 27a and 27b reveal what pathologic finding?
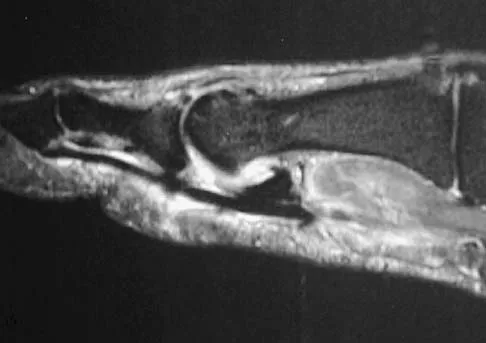
Explanation
The MRI scans show a complete disruption of the sesamoid complex with proximal retraction of the medial sesamoid and high signal originating from the site normally occupied by the plantar plate (metatarsophalangeal ligament). This injury is the result of a hyperextension injury and is a severe variant of a turf toe. Watson TS, Anderson RB, Davis WH: Periarticular injuries to the hallux metatarsophalangeal joint in athletes. Foot Ankle Clin 2000;5:687-713.
Question 671
High Yield
A 10-year-old boy with spastic diplegic cerebral palsy walks in a crouched position with the hips and knees flexed. Maximum knee flexion is 15 degrees during early swing phase. Instrumented gait analysis shows quadriceps activity from terminal stance throughout swing phase. Treatment should consist of
Explanation
The rectus femoris muscle spans two joints and is active during running, sprinting, and walking at a fast pace during the preswing and early swing phase of gait. In these situations, the muscle helps to generate power to initiate hip flexion while absorbing or controlling the rate of knee flexion during early swing phase. Quadriceps activity, including the rectus femoris, is not normally needed when walking at a routine cadence. However, rectus femoris activity is commonly noted during preswing and the swing phase in patients with cerebral palsy, particularly those with diplegia. In an effort to initiate swing phase, the rectus femoris is "overactive." As a result, the knee flexion that commonly occurs at terminal stance and initial swing is restricted. Instead of achieving the normal 50 to 60 degrees of flexion during early swing, this patient's knee flexion is limited to 15 degrees. The goal of treatment is to retain rectus femoris activity for initiation of hip flexion but to diminish its restraint on knee flexion. Studies have shown that transfer of the distal rectus femoris tendon provides more flexion of the knee during the swing phase of gait than simply releasing the tendon. V-Y lengthening of the quadriceps tendon or a Z lengthening of the patellar tendon causes too much weakening of the quadriceps muscle and worsens the crouch deformity. In addition to transfer of the rectus femoris tendon, other procedures are often done concomitantly to obtain the best balance and realignment of hip-knee-ankle activity. Aiona MD: Guidelines for managing lower extremity problems in cerebral palsy, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 1534-1541. Chambers H, Laure A, Kaufman K, Cardelia M, Sutherland D: Prediction of outcome after rectus femoris surgery in cerebral palsy: The role of cocontraction of the rectus femoris and vastus lateralis. J Pediatr Orthop 1998;18:703-711.
Question 672
High Yield
Figures 34a and 34b show the clinical photographs of a 46-year-old woman who has a painful deformity of the second toe. Surgical treatment consisting of metatarsophalangeal capsulotomy and proximal interphalangeal joint resection arthroplasty resulted in satisfactory correction, but the toe remains unstable at the metatarsophalangeal joint. What is the next most appropriate step?

Explanation
Crossover second toes are attributed to attenuation or rupture of the plantar plate and lateral collateral ligament and are associated with varying degrees of instability. Flexor-to-extensor transfer (Girdlestone/Taylor procedure) can provide intrinsic stability to the toe. Although plantar metatarsal head condylectomy can increase stability by resulting in scarring of the plantar plate, excision of the entire second metatarsal head carries a high risk of transfer metatarsalgia. Removal of the base of the proximal phalanx destabilizes the toe and should be reserved as a salvage procedure. Simple flexor tenotomy alone will not improve stability, and arthrodesis of the second metatarsophalangeal joint will limit motion and impair function. Coughlin MJ: Crossover second toe deformity. Foot Ankle 1987;8:29-39.
Question 673
High Yield
A 58-year-old reports pain and stiffness in his left shoulder following a seizure episode. Diagnosis at the time of the seizure is a frozen shoulder, and management consists of an aggressive physical therapy program of stretching exercises. Four months later he continues to have shoulder pain and has not gained any additional range of motion. A CT scan is shown in Figure 50. Management should now consist of

Explanation
Humeral arthroplasty is indicated for chronic posterior dislocations when the impression defect in the humeral head is greater than 45% to 50%. If the condition remains undiagnosed for more than 9 to 12 months, secondary degenerative changes on the glenoid may occur, necessitating total shoulder arthroplasty. Open reduction and transfer of the subscapularis and lesser tuberosity are used for impression defects that consist of 20% to 40% of the humeral articular surface. Closed reduction and immobilization with the arm in slight extension and external rotation is useful when the posterior dislocation is diagnosed within the first 6 weeks and the articular defect is less than 20%. Hawkins RJ, Neer CS II, Pianta RM, Mendoza FX: Locked posterior dislocation of the shoulder. J Bone Joint Surg Am 1987;69:9-18.
Question 674
High Yield
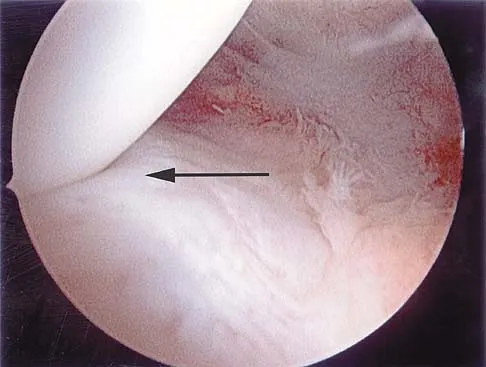
Figure 43 shows an arthroscopic view of the posteromedial compartment of a patient's left knee using a 70-degree arthroscope placed through the intercondylar notch. The arrow is pointing to what structure?
Explanation
Passing the 70-degree arthroscope through the intercondylar notch provides excellent visualization of the posteromedial corner of the knee. This view should be part of every knee arthroscopy because these structures are often not well visualized from the anterior portals. If this view is omitted, tears of the peripheral posterior horn of the medial meniscus can be overlooked. The arrow points to the peripheral aspect of the posterior horn of the medial meniscus. With an intact medial meniscus, the medial tibial plateau should not be seen from this view. The semimembranosus and gastrocnemius tendons are extra-articular and not visualized. Miller MD: Basic arthroscopic principles, in DeLee JC, Drez D Jr, Miller MD (eds): Orthopaedic Sports Medicine, ed 2. Philadelphia, PA, Saunders, 2003, pp 224-237.
Question 675
High Yield
A 7-year-old girl with spinal muscular atrophy (SMA) type II has popping of the left hip. Examination reveals painless subluxation of the joint in adduction with palpable reduction in abduction. Radiographs show coxa valga, subluxation of the left hip, and pelvic obliquity with elevation of the left hemipelvis. Treatment should consist of

Explanation
Observation is the treatment of choice. Hip subluxation and dislocation are not uncommon in patients with SMA type II who are unlikely to be ambulatory. Scoliosis occurs in these patients 100% of the time and frequently creates pelvic obliquity. However, in long-term follow-up, patients with SMA type II and hip dislocations had little associated pain or functional limitations because of hip instability. In addition, recurrent hip subluxation after surgical treatment has been documented. Given the rarity of symptoms from hip instability in long-term follow-up, and the possibility of recurrent dislocation, surgical intervention for hip instability may expose SMA type II patients to undue surgical risk for minimal if any functional gain. Sporer SM, Smith BG: Hip dislocation in patients with spinal muscular atrophy. J Pediatr Orthop 2003;23:10-14.
Question 676
High Yield
Figure 3 shows the AP radiograph of a patient with diabetes mellitus who has knee pain. A semiconstrained knee prosthesis was used in this patient to prevent which of the following complications?

Explanation
The radiographic appearance of the joint is highly suspicious for neuropathic joint (Charcot's joint). Evidence of bone loss on both the tibial and the femoral sides may necessitate the use of metal and/or bone augments. Patients with a neuropathic joint often have excellent range of motion, and postoperative stiffness is not a problem. The main problem with these patients is instability that occurs secondary to ligamentous laxity. Use of a semiconstrained prosthesis prevents the latter complication. Parvizi J, Marrs J, Morrey BF: Total knee arthroplasty for neuropathic (Charcot) joints. Clin Orthop 2003;416:145-150.
Question 677
High Yield
A 61-year-old man has a symptomatic bunionette that is refractory to nonsurgical management. A radiograph is shown in Figure 6. What is the optimal surgical correction?

Explanation
The patient has a bunionette with a large 4-5 intermetatarsal angle. This requires not only ostectomy of the lateral prominence but metatarsal osteotomy to decrease the intermetatarsal angle. Excising the head results in a flail joint and creates the possibility of a transfer lesion. Condylectomy can reduce plantar pressures but does not address the bunionette. The joint surface is well maintained, thus there are no indications for resection. Coughlin MJ: Treatment of bunionette deformity with longitudinal diaphyseal osteotomy with distal soft tissue repair. Foot Ankle 1991;11:195-203.
Question 678
High Yield
A 24-year-old man has had pain in the left knee for the past several months. He reports that initially the pain was associated with weight-bearing activities, but it has now become more constant. He denies any swelling but reports a lateral fullness at the tibial plateau. Figures 23a through 23e show radiographs, a bone scan, and T1- and T2-weighted MRI scans. What is the most likely diagnosis?





Explanation
The radiographs reveal a lytic subchondral lesion that has a poorly defined margin and lacks mineralization. The bone scan confirms an active lesion that has central photopenia, producing the characteristic doughnut configuration. The MRI scans confirm the presence of a subchondral lesion that is modestly expansile at the lateral plateau and has low signal intensity on the T1-weighted image and a mixed high signal on the T2-weighted image. These features strongly suggest giant cell tumor of bone, more than 50% of which appear around the knee. Simple cyst is excluded by the MRI characteristics. Fibrous dysplasia is unlikely to be in a subchondral location and typically does not show this intensity of uptake on bone scan. Parsons TW: Benign bone tumors, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 1027-1035.
Question 679
High Yield
A 21-year-old man sustains multiple gunshot wounds to his right upper extremity. He can not extend his digits or his thumb but can extend and radially deviate his wrist. An injury to the radial nerve or one of its branches has most likely occurred at which of the following locations?

Explanation
In this patient, the radial nerve is most likely injured at the level of the radial neck. The radial nerve emerges from the posterior cord of the brachial plexus and travels along the spiral groove of the humerus. At the level of the lateral humeral condyle, the radial nerve branches into the posterior interosseous nerve after giving off two cutaneous branches, the superficial radial and the posterior cutaneous. The posterior interosseous nerve travels through the supinator muscle and winds around the radial neck. At this level, the posterior interosseous nerve is vulnerable to injury, particularly following fracture or penetrating trauma. Netter F: The Ciba Collection of Medical Illustrations: The Musculoskeletal System, Part 1: Anatomy, Physiology and Metabolic Disorders. West Caldwell, NJ, Ciba-Geigy Corporation, 1987, vol 8, p 53.
Question 680
High Yield
What is the function of the rotator cuff during throwing?

Explanation
The coupled action of the rotator cuff prevents superior migration and controls anterior and posterior translation by depressing the humeral head. Poppen NK, Walker PS: Normal and abnormal motion of the shoulder. J Bone Joint Surg Am 1976;58:195-201.
Question 681
High Yield
What is the preferred treatment of a symptomatic curly toe deformity in a 6-year-old child?
Explanation
While some curly toe deformities spontaneously improve in younger children, the deformity is likely to persist in a 6-year-old child. Taping techniques result in no change or only a temporary decrease in deformity. Studies have shown that simple flexor tenotomy is as effective as flexor tendon transfer. Arthrodesis is rarely indicated. Hamer A, Stanley D, Smith TW: Surgery for curly toe deformity: A double-blind, randomized, prospective trial. J Bone Joint Surg Br 1993;75:662-663.
Question 682
High Yield
A 13-year-old girl has had right groin pain for the past 3 weeks. She denies any history of trauma. Examination of the hip reveals no palpable soft-tissue mass or lymphadenopathy, and there is full range of motion. A plain radiograph and MRI scan are shown in Figures 15a and 15b. Biopsy specimens are shown in Figures 15c and 15d. What is the most likely diagnosis?


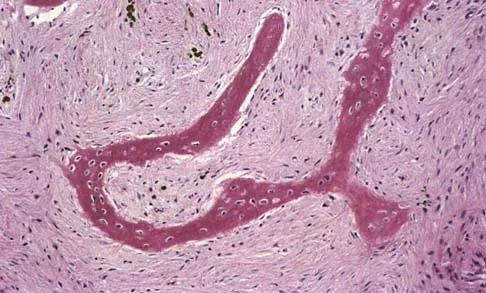
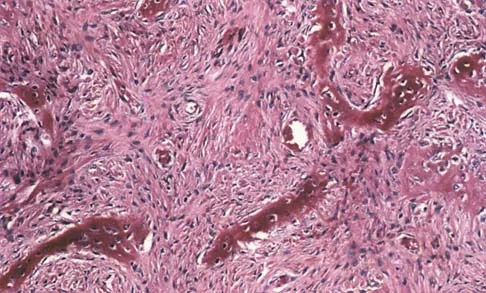
Explanation
Fibrous dysplasia frequently occurs in the proximal femur. Microfractures and remodeling can lead to the classic "Shepherd's crook deformity." The lesion has a ground-glass appearance on plain radiographs. The histologic appearance shows proliferating fibroblasts in a loose spindle cell background. Dysplastic metaplastic trabeculae are arranged in an irregular or "Chinese letter" appearance. Enneking WF, Gearen PF: Fibrous dysplasia of the femoral neck: Treatment by cortical bone grafting. J Bone Joint Surg Am 1986;68:1415-1422.
Question 683
High Yield
What region of the spine is most susceptible to changes in the vascular supply to the spinal cord during an anterior approach?
Explanation
The thoracic spinal cord is characterized by a variable and, at times, complicated blood supply. The artery of Adamkiewicz, also known as the great anterior medullary artery, most typically arises off the left side of the aorta between T8 and T12. It represents the sole medullary blood supply to the thoracic spine. When this artery is divided or injured, the blood supply to the thoracic cord may be interrupted. It is important to avoid electocautery of blood vessels within or near the thoracic foramen because this is a site of important, albeit limited, collateral circulation. Sharma M, Anderson FC: Spinal vascular lesions, in Frymoyer JW, Wiesel SW (eds): The Adult and Pediatric Spine. Philadelphia, PA, Lippincott Williams and Wilkins, 2004, pp 301-306.
Question 684
High Yield
A 29-year-old woman who underwent an anterior cruciate ligament (ACL) reconstruction 6 months ago now reports difficulty achieving full knee extension, and physical therapy fails to provide relief. The knee is stable on ligament testing. Figure 3 shows the findings at a repeat arthroscopy. Treatment should now include

Explanation
The patient has a cyclops lesion. This is a nodule of fibroproliferative tissue that originates from either drilling debris from the tibial tunnel or remnants of the ACL stump; more rarely it is the result of broken graft fibers. The treatment of choice is excision of the nodule and, if needed, additional notchplasty. Marked improvements in function and symptoms have been noted after removal of the extension block and resumption of a rehabilitation program. Delince P, Krallis P, Descamps PY, et al: Different aspects of the cyclops lesion following anterior cruciate ligament reconstruction: A multifactorial etiopathogenesis. Arthroscopy 1998;14:869-876.
Question 685
High Yield
A 21-year-old right hand-dominant male collegiate swimmer reports painful clicking in the right shoulder. He states that he can occasionally feel his shoulder "slip out" when he is working out. AP, true AP, and axillary radiographs are shown in Figures 39a through 39c. What is the next most appropriate step in management?



Explanation
The radiographs show glenoid hypoplasia. The common radiographic findings of glenoid hypoplasia include an inferior and posterior glenoid deficiency, enlargement of the distal end of the clavicle, and sometimes an indentation in the glenoid. It is usually bilateral and rarely associated with other syndromes; therefore, an echocardiogram, abdominal ultrasound, or a skeletal survey is unnecessary unless the patient has stigmata of a syndrome such as Holt-Oram or Apert's. Although posterior instability has been reported, the results of glenoid osteotomy have been variable and should not be considered initially. Physical therapy is the mainstay of initial management, but the patient should be counseled that this may be a recurrent problem with early osteoarthritis developing in many patients. Radiographs of the contralateral side should be obtained because this is usually bilateral. Wirth MA, Lyons FR, Rockwood CA Jr: Hypoplasia of the glenoid: A review of sixteen patients. J Bone Joint Surg Am 1993;75:1175-1184.
Question 686
High Yield
A 37-year-old recreational tennis player undergoes surgery for tennis elbow. Following surgery, she describes clicking and popping on the lateral aspect of the elbow. A lateral pivot shift test is positive. What is the most likely cause of her symptoms?
Explanation
The patient has a posterolateral rotatory instability (PLRI) of the elbow that is most likely the result of iatrogenic injury to the lateral ulnar collateral ligament, the main ligament implicated in PLRI. The anterior band of the medial collateral ligament is implicated in valgus instability. Injury to the radial nerve is unlikely, and the lateral radial collateral ligament makes less of a contribution to elbow stability than does the ulnar component. While the origin of the extensor carpi radialis brevis may contribute to elbow stability, it is not as important a stabilizer as the lateral ulnohumeral ligament. O'Driscoll SW, Morrey BF: Surgical reconstruction of the lateral collateral ligament, in Morrey BF (ed): The Elbow. Philadelphia, PA, Lippincott, Williams and Wilkins, 1994, pp 169-182.
Question 687
High Yield
An 18-year-old lacrosse player is diagnosed with infectious mononucleosis. What is the recommendation for return to play?
Explanation
Infectious mononucleosis commonly affects adolescents and young adults. It is a febrile illness accompanied by acute pharyngitis. Splenomegaly may occur and predispose the athlete to splenic rupture. Splenic rupture has been reported in nonathletes as well as in patients with normal-sized spleens. Clinical evidence supports a return to all sports 4 weeks after the onset of symptoms provided that the spleen has returned to normal size. Auwaerter PG: Infectious mononucleosis: Return to play. Clin Sports Med 2004;23:485-497.
Question 688
High Yield
A 30-year-old man who participates in recreational sports reports the spontaneous onset of intermittent pain and swelling about the right knee. Examination reveals a 3+ effusion, with a range of motion of 10 degrees to 60 degrees. He has mild diffuse tenderness but no instability. MRI scans and an arthroscopic view are shown in Figures 39a through 39c. Management should consist of
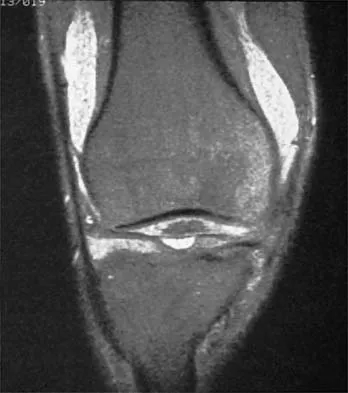
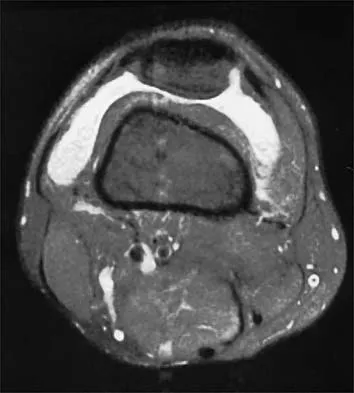

Explanation
The patient has synovial chondromatosis. The MRI scans show multiple small proscribed areas of signal intensity in the gutters and suprapatellar pouch, suggesting very small loose bodies. The arthroscopic view shows the classic appearance of multiple small chondral loose bodies. Synovial chondromatosis is a condition in which the synovium undergoes metaplasia, producing multiple chondral loose bodies that can subsequently ossify. The treatment of choice, removal of the loose bodies and arthroscopic synovectomy, results in a lower incidence of recurrence than other treatment methods. Coolican MR, Dandy DJ: Arthroscopic management of synovial chondromatosis of the knee: findings and results in 18 cases. J Bone Joint Surg Br 1989;71:498-500.
Question 689
High Yield
A collegiate golfer sustains a hook of the hamate fracture. After 12 weeks of splinting and therapy, the hand is still symptomatic. What is the most appropriate management to allow return to competitive activity?

Explanation
Excision of the fracture fragment typically leads to rapid return to function. Fixation techniques are difficult to perform because of the size of the bone; hardware prominence is common. Nerve deficits are not typically noted in this injury. The motor branch of the ulnar nerve in Guyon's canal must be protected during the surgical approach. Kulund DN, McCue FC III, Rockwell DA, et al: Tennis injuries: Prevention and treatment: A review. Am J Sports Med 1979;7:249-253.
Question 690
High Yield
In a retroperitoneal approach to the lumbar spine, what nerve is commonly found on the psoas muscle?
Explanation
The genitofemoral nerve and the sympathetic plexus consistently lie on the ventral surface of the psoas muscle. The ilioinguinal and iliohypogastric nerves are the most superior branches of the lumbar plexus and emerge along the upper lateral border of the psoas muscle traveling toward the quadratus lumborum. Both the obturator and femoral nerves are deep and lateral to the psoas muscle. Watkins RG (ed): Surgical Approaches to the Spine, ed 1. New York, NY, Springer-Verlag, 1983, p 107. Johnson R, Murphy M, Southwick W: Surgical approaches to the spine, in Herkowitz HH (ed): The Spine, ed 4. Philadelphia, PA, WB Saunders, 1992, p 1559.
Question 691
High Yield
What are the four most common soft-tissue sarcomas to spread via the lymph node system?

Explanation
Soft-tissue sarcomas most frequently metastasize to the lung, but certain histologic types have a predilection for the lymph node system as well. Rhabdomyosarcoma, clear cell sarcoma, epithelioid sarcoma, and synovial sarcoma are four of the most common types to spread in this fashion. Careful evaluation and/or sentinel lymph node biopsy plays a role in disease staging and prognosis. Riad S, Griffin AM, Liberman B, et al: Lymph node metastasis in soft-tissue sarcoma in an extremity. Clin Orthop Relat Res 2004;426:129-134.
Question 692
High Yield
A 12-year-old boy sustained a grade III open tibial fracture 1 week ago and underwent multiple debridements and fracture fixation. He now has a soft-tissue defect that measures 6 cm x 6 cm, with an area of exposed bone and muscle on the distal medial leg that is a few centimeters proximal to the ankle. Management of the soft-tissue defect should now consist of

Explanation
The soft-tissue defect is in a very difficult position - the distal tibia. The defect is too distal for a gastrocnemius flap, and the exposed bone precludes an immediate skin graft. A free flap and skin graft would be required for closure. VAC is very effective in soft-tissue defects such as this one. Healthy granulation tissues form quickly. VAC can be the definitive treatment, or it can be used before skin grafting. Wet-to-dry dressings could promote granulation, but the process is hastened substantially by VAC. Amputation is not a consideration because there are no signs of infection or fracture healing problems at this time. Mooney JF III, Argenta LC, Marks MW, et al: Treatment of soft tissue defects in pediatric patients using the V.A.C. system. Clin Orthop 2000;376:26-31.
Question 693
High Yield
What risk factor is most associated with progression of idiopathic scoliosis to a curve requiring surgery?

Explanation
The magnitude of the curve at the time of the peak height velocity is the most prognostic sign in relationship to surgery. More than 70% of curves that measure more than 30 degrees at this time are likely to reach surgical range. Little DG, Song KM, Katz D, et al: Relationship of peak height velocity to other maturity indicators in idiopathic scoliosis in girls. J Bone Joint Surg Am 2000;82:685-693.
Question 694
High Yield
Figure 11 shows the radiograph of a 2-year-old child with marked genu varum and tibial bowing. Based on these findings, what is the best initial course of action?

Explanation
The radiograph shows multiple wide physes, consistent with a diagnosis of rickets. A low serum phosphorous level and an elevated alkaline phosphatase level are the hallmarks in diagnosing familial hypophosphatemic Vitamin D-resistant rickets. Serum calcium is usually normal or low normal. This disease is inherited as an X-linked dominant trait and usually presents at age 18 to 24 months. The disease results from a poorly defined problem with renal phosphate transport in which normal dietary intake of vitamin D is insufficient to achieve normal bone mineralization. Renal tubular dysfunction is associated with urinary phosphate wasting. Treatment involves oral phosphate supplementation, which can cause hypocalcemia and secondary hyperparathyroidism. To prevent associated problems, high doses of Vitamin D are administered. While obtaining a scanogram may be clinically indicated in an associated limb-length discrepancy, and subsequent corrective surgery may be indicated, either of these choices would not be the first course of action. An orthosis may slow the progression of genu varum in this disorder but is less important than establishing the correct diagnosis to begin pharmacologic treatment. This amount of varum and tibial bowing far exceeds the normal limits of physiologic genu varum. Skeletal dysplasias usually are not associated with abnormal laboratory values. Herring JA: Metabolic and endocrine bone diseases, in Tachdjian's Pediatric Orthopaedics, ed 3. New York, NY, WB Saunders, 2002, pp 1685-1743.
Question 695
High Yield
A 39-year-old competitive cyclist sustains an injury to her left hip in a fall. Gadolinium arthrography, with an accompanying MRI scan, is shown in Figure 31. A cleft, or defect, identified by the arrow, indicates a detachment of the

Explanation
The area indicated by the arrow represents gadolinium contrast extending into a separation between the lateral labrum and its acetabular attachment. This can be a traumatic detachment, but occasionally a cleft may be present as a normal variant of the labral morphology. The capsular attachment of the iliofemoral ligament is peripheral to the labrum. The pulvinar is the common name applied to the fat and overlying synovium contained within the acetabular fossa above the ligamentum teres. The zona orbicularis is a circumferential thickening of the capsule around the femoral neck, and the retinacular vessels travel within the capsular synovium up the femoral neck to supply the femoral head. Petersilge CA, Haque MA, Petersilge WJ, Lewin JS, Lieberman JM, Buly R: Acetabular labral tears: Evaluation with MR arthrography. Radiology 1996;200:231-235. Czerny C, Hofmann S, Neuhold A, et al: Lesions of the acetabular labrum: Accuracy of MR imaging and MR arthrography in detection and staging. Radiology 1996;200:225-230.
Question 696
High Yield
A 13-year-old girl with hallux valgus reports pain after playing basketball. Radiographs show a hallux valgus angle of 20 degrees, an intermetatarsal angle of 11 degrees, a distal metatarsal articular angle of 10 degrees, and a congruent joint. Management should consist of
Explanation
Shoe wear modification is the most appropriate management based on the patient's age, high activity level, and relatively minor symptoms. She also has a mild hallux valgus. Normal radiographic measurements are an intermetatarsal angle of less than 9 degrees, a hallux valgus angle of less than 15 degrees, and a distal metatarsal articular angle of less than 9 degrees. Surgical procedures should be reserved for patients with more severe or progressive deformities. Stephens HM: Bunions, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 1510-1519.
Question 697
High Yield
Examination of an obese 3-year-old girl reveals 30 degrees of unilateral genu varum. A radiograph of the involved leg with the patella forward is shown in Figure 10. Management should consist of

Explanation
The clinical scenario describes infantile tibia vara (Blount's disease). The radiograph shows severe deformity with the characteristic Langenskiold stage 3 changes of the medial proximal tibial metaphysis that distinguish it from physiologic bowing. The preferred treatment is proximal tibiofibular osteotomy with acute correction into slight valgus to unload the damaged area of the physis. This method provides the best results in patients younger than age 4 years. Continued observation would result in progressive deformity. Bracing is most effective in younger children with less severe deformity. Lateral proximal tibial hemiepiphysiodesis relies on growth of the injured medial physis for correction and would result in severe tibial shortening in this young child. Complete epiphysiodesis also produces severe shortening and requires multiple lengthening procedures. Johnston CE II: Infantile tibia vara. Clin Orthop 1990;255:13-23.
Question 698
High Yield
Figure 50 shows the cross table lateral radiograph of a 31-year-old paratrooper who has recalcitrant groin pain. The pain is worse after activities such as standing or sitting (driving). Examination reveals that pain can be reproduced by internal rotation of the leg with the hip and knee in 90 degrees of flexion. Extensive nonsurgical managment has failed to provide relief. What is the treatment of choice?

Explanation
The radiograph reveals the classic "bump" that is seen in patients with femoroacetabular impingement (FAI). Ganz and associates described two types of FAI. This patient has cam impingement, which describes a nonspherical femoral head being forced into the acetabulum during hip motion and resulting in labral and chondral injury. Hip arthroscopy and labral debridement is unlikely to control the symptoms because the underlying anatomic abnormality is often difficult to address with arthroscopy. The treatment involves surgical dislocation of the hip with preservation of the blood supply to the femoral head, removal of the asphericity on the femoral side (femoral osteoplasty), and removal of the acetabular rim (acetabular osteoplasty) if the latter is found to contribute to impingement. Ganz R, Gill TJ, Gautier E, et al: Surgical dislocation of the adult hip a technique with full access to the femoral head and acetabulum without the risk of avascular necrosis. J Bone Joint Surg Br 2001;83:1119-1124. Ganz R, Parvizi J, Beck M, et al: Femoroacetabular impingement: A cause for early osteoarthritis of the hip. Clin Orthop 2003;417:112-120.
Question 699
High Yield
A 74-year-old woman with rheumatoid arthritis reports shoulder pain that has failed to respond to nonsurgical management. AP and axillary radiographs are shown in Figures 23a and 23b. Examination reveals active forward elevation to 120 degrees and external rotation to 30 degrees. What treatment option results in the most predictable pain relief and function?


Explanation
Most studies have shown that total shoulder arthroplasties yield better pain relief and improved forward elevation when compared to hemiarthroplasty in patients with rheumatoid arthritis. Although rotator cuff tears are more common in this patient population, this patient has good forward elevation and no significant superior migration of the humeral head; therefore, a reverse arthroplasty is not indicated. The arthritis is too advanced in this patient to consider arthroscopy, but in less advanced cases it can improve range of motion and decrease pain. Metal-backed glenoid components have shown higher rates of loosening. Collin DN, Harryman DT II, Wirth MA: Shoulder arthroplasty for the treatment of inflammatory arthritis. J Bone Joint Surg Am 2004;86:2489-2496. Baumgarten KM, Lashgari CM, Yamaguchi K: Glenoid resurfacing in shoulder arthroplasty: Indications and contraindications. Instr Course Lect 2004;53:3-11.
Question 700
High Yield
Which of the following is considered the most accurate test to determine the amount of limb-length discrepancy in a patient with a knee flexion contracture of 35 degrees?
Explanation
Flexion contractures and angular deformities of a limb cause inaccurate limb-length measurement results with most clinical methods. A CT scanogram is more accurate than standard scanograms for determining limb length in patients with knee flexion contractures of 30 degrees or more. The cost and time necessary to complete the examinations are comparable, but the CT scanogram delivers only 20% of the radiation needed for standard scanograms. Aaron A, Weinstein D, Thickman D, Eilert R: Comparison of orthoroentgenography and computed tomography in the measurement of limb-length discrepancy. J Bone Joint Surg Am 1992;74:897-902.
