HY 2026
00:00
Start Quiz
Question 501
High Yield
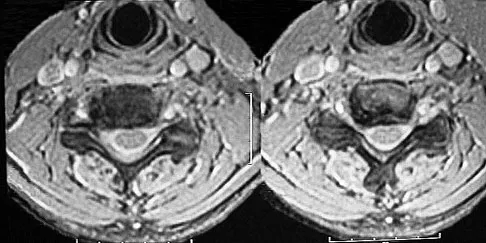
Figure 11 shows a consecutive sequence of MRI scans obtained in a 12-year-old boy who has had increasing lateral knee pain and catching for the past 6 months. Examination reveals pain localized to the lateral joint line. Range-of-motion testing reveals a 5-degree lack of full extension on the involved side. Plain radiographs and laboratory values are within normal limits. What is the most appropriate management?

Explanation
Discoid menisci are rare causes of lateral knee pain in children. Various etiologies have been proposed, including failure of central absorption of the developing meniscus and hereditary transmission. Patients with discoid menisci have pain, clicking, and locking with a loss of active extension on range-of-motion testing. Classification of discoid menisci according to the Watanabe classification include complete, incomplete, and Wrisberg ligament type. The Wrisberg variant contains an abnormal posterior meniscal attachment. MRI is the diagnostic tool of choice, revealing a thick, flat meniscus generally seen in three consecutive MRI images. Symptomatic knees are often associated with a meniscal tear or degeneration and are managed with arthroscopic partial excision to a more normal shape (saucerization). Vandermeer RD, Cunningham FK: Arthroscopic treatment of the discoid lateral meniscus: Results of long-term follow-up. Arthroscopy 1989;5:101-109.
Question 502
High Yield
A 40-year-old right hand-dominant construction worker has had a 6-month history of aching left shoulder pain that is worse after working a long day. Examination reveals limited range of motion and good strength when compared to his asymptomatic right arm. He has not had any orthopaedic intervention to date. Radiographs are shown in Figures 43a and 43b. What is the most appropriate treatment?


Explanation
The patient is a young laborer with osteoarthritis. Initial treatment should begin with nonsurgical management that may include anti-inflammatory drugs, cortisone injections, and physical therapy to diminish pain and improve motion. The other choices may eventually be necessary but should only follow a course of nonsurgical management. Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 257-266.
Question 503
High Yield
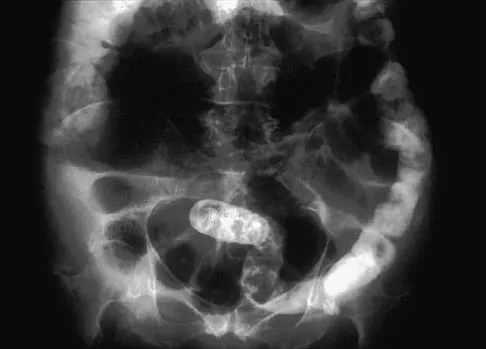
Figure 13 shows the radiographs of a 56-year-old woman who has pain and varus knee deformity after undergoing total knee arthroplasty 8 years ago. Aspiration and studies for infection are negative. During revision surgery, management of the tibial bone loss is best achieved by

Explanation
Massive bone loss encountered in revision total knee arthroplasty remains a significant challenge. Recent reports have shown high success rates using structural allograft to reconstruct massive bone defects. Custom and hinged prostheses in this setting are no longer favored. The defect shown is segmental and is too large to be filled with cement or iliac crest bone graft. Mow CS, Wiedel JD: Structural allografting in revision total knee arthroplasty. J Arthroplasty 1996;11:235-241. Engh GA, Herzwurm PJ, Parks NL: Treatment of major defects of bone with bulk allografts and stemmed components during total knee arthroplasty. J Bone Joint Surg Am 1997;79:1030-1039.
Question 504
High Yield
A 21-year-old football player had severe pain and immediate swelling in the left anteromedial chest wall while bench pressing near maximal weights several days ago. Examination at the time of injury revealed a mass on the anteromedial chest wall. Follow-up examination now reveals decreased swelling, and axillary webbing is observed. The patient has weakness to adduction and forward flexion. The injured muscle originates from the
Explanation
The patient has a pectoralis major rupture, an injury that occurs most commonly during weight lifting. Grade III injuries represent complete tears of either the musculotendinous junction or an avulsion of the tendon from the humerus, the most common injury site. Examination will most likely reveal ecchymoses and swelling in the proximal arm and axilla, and strength testing will show weakness with internal rotation and in adduction and forward flexion. Axillary webbing, caused by a more defined inferior margin of the anterior deltoid as the result of rupture of the pectoralis, can be seen as the swelling diminishes. Surgical repair is the treatment of choice for complete ruptures. Nonsurgical treatment is associated with significant losses in adduction, flexion, internal rotation, strength, and peak torque. The pectoralis major originates from the proximal clavicle and the border of the sternum, including ribs two through six. The pectoralis major inserts (rather than originates) on the humerus. The coracoid process is the insertion site for the pectoralis minor, as well as the origin for the conjoined tendon. The pectoralis major has no attachment or origin from the scapula. The anterior deltoid originates from the lateral one third of the clavicle and the anterior acromion. Miller MD, Johnson DL, Fu FH, Thaete FL, Blanc RO: Rupture of the pectoralis major muscle in a collegiate football player: Use of magnetic resonance imaging in early diagnosis. Am J Sports Med 1993;21:475-477.
Question 505
High Yield
Medial dislocation of the long head of the biceps tendon in the shoulder is most commonly caused by a
Explanation
Medial dislocation of the biceps tendon in the shoulder is commonly associated with subscapularis tendon tears. Although type II SLAP tears can result in bicipital instability, type I SLAP lesions do not. Congenitally shallow grooves and tears of the transverse ligaments usually do not lead to dislocation of the biceps tendon. Supraspinatus tendon tears are associated with long head of the biceps tendon ruptures but do not cause biceps tendon dislocations. Werner A, Mueller T, Boehm D, et al: The stabilizing sling for the long head of the biceps tendon in the rotator cuff interval: A histoanatomic study. Am J Sports Med 2000;28:28-31.
Question 506
High Yield
An 83-year-old woman with a long history of her foot slowly and progressively "turning out" now reports significant ankle pain. History reveals that she has significant cardiac disease and exercise-induced angina. Examination reveals a deficiency in the posterior tibial tendon; however, the hindfoot remains moderately supple. Radiographs reveal a valgus tilt of the tibiotalar joint and early arthrosis. What is the most appropriate orthotic management?
Explanation
The patient will continue to have pain secondary to the ankle arthrosis with both the UCBL and the molded articulated ankle-foot orthosis. The total contact orthotic does not provide enough hindfoot control to support the progressive collapse of the ankle into valgus positioning. A molded leather gauntlet will not only control tibiotalar motion but also control hindfoot motion and allow support of the longitudinal arch.
Question 507
High Yield
A 13-year-old boy injured his knee playing basketball and is now unable to bear weight. Examination reveals tenderness and swelling at the proximal anterior tibia, with a normal neurologic examination. AP and lateral radiographs are shown in Figures 1a and 1b. Management should consist of


Explanation
The patient has a displaced intra-articular tibial tuberosity fracture; therefore, the treatment of choice is open reduction and internal fixation. Periosteum is often interposed between the fracture fragments and prevents satisfactory closed reduction. Fortunately, most patients with this injury are close to skeletal maturity and therefore, growth arrest and recurvatum are unusual. Nondisplaced fractures can be treated with a cast, but displaced fractures are best treated with open reduction and internal fixation. Intra-articular fractures can disrupt the joint surface and are sometimes associated with a meniscal tear; therefore, arthroscopy may be needed at the time of open reduction and internal fixation. McKoy BE, Stanitski CL: Acute tibial tubercle avulsion fractures. Orthop Clin North Am 2003;34:397-403.
Question 508
High Yield
Flexion and extension of the elbow occur about an axis of rotation that

Explanation
The elbow mimics a true hinge and flexes and extends around an axis that is centered in the centers of the trochlea and capitellum. The medial epicondyle is not perfectly isometrically placed; rather the axis of rotation passes through a point on the anteroinferior aspect of the medial epicondyle. Application of a hinged external fixator is possible because of the fact that there is a single axis of rotation. Morrey BF (ed): The Elbow and Its Disorders, ed 2. Philadelphia, PA, WB Saunders, 1993, pp 53-54. London JT: Kinematics of the elbow. J Bone Joint Surg Am 1981;63:529-535.
Question 509
High Yield
Polyethylene wear of the bearing surface has been recognized as a mode of failure in total knee arthroplasty; therefore, many patients are offered polyethylene exchange. In terms of success rates, this surgical procedure has been reported to have a
Explanation
Engh and associates reported on the results of 63 knees (56 patients) following polyethylene exchange. The mean interval between exchange and the index total knee arthroplasty was 59 months. The mean follow-up after exchange was 7.4 years. Seven of 48 knees with adequate follow-up failed. Greater failure occurred if there was more severe wear before the exchange. Greater undersurface wear also resulted in a higher failure rate. Perioperative osteolysis or intraoperative observation of metallosis did not have an impact on the failure of polyethylene exchange. The risk of infection is no different from other total knee arthroplasty revisions. Wasielewski RC, Parks N, Williams I, et al: Tibial insert undersurface as a contributing source of polyethylene wear debris. Clin Orthop 1997;345:53-59.
Question 510
High Yield
A 23-year-old woman has had a 14-month history of ankle pain after surgical treatment of multiple injuries resulting from a motor vehicle accident. Weight bearing began 4 months after surgery. The pain occurs with weight bearing and motion, but there is very little pain at rest. She has no pertinent medical history and does not smoke. Figures 23a and 23b show current radiographs. What is the most appropriate surgical option?


Explanation
The radiographs reveal nonunion of a talar neck fracture. There is no radiographic evidence of osteonecrosis or significant degenerative arthritis. The results of talectomy are suboptimal. Arthrodesis would be indicated for degenerative arthritis. Revision ORIF is feasible and preserves motion. A vascularized graft should be considered whenever osteonecrosis is present, but the talar body appears viable in this case. Calvert E, Younger A, Penner M: Post talus neck fracture reconstruction. Foot Ankle Clin 2007;12:137-151.
Question 511
High Yield
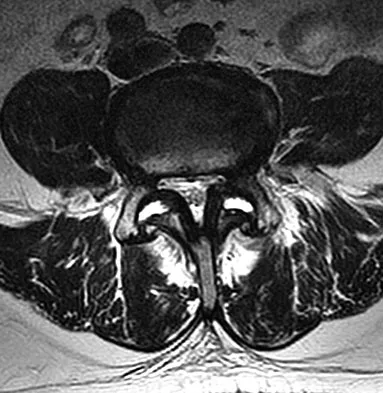
A 40-year-old woman sustains a flexion injury to her neck. Physical examination is normal. A lateral radiograph of the cervical spine is shown in Figure 57a. MRI scans of the cervical spine are shown in Figures 57b and 57c. Treatment should include


Explanation
This is a classic bilateral facet dislocation. When there is no evidence of a disk herniation, treatment should include careful skeletal traction, closed reduction, and posterior fusion. There is no role for anterior procedures. These fractures are unstable and require surgical intervention. Herkowitz HN, Garfin SR, Eismont FJ: Rothman-Simone The Spine, ed 5. Philadelphia, PA, Saunders Elsevier, 2006, pp 1120-1128.
Question 512
High Yield
Examination of a 7-year-old boy reveals 20 degrees of valgus following a lawn mower injury to the lateral femoral epiphysis. Treatment consists of total distal femoral epiphyseodesis and varus osteotomy. Following surgery, he has a limb-length discrepancy of 3 cm and 5 degrees of genu valgum. Assuming that he undergoes no further treatment, the patient's predicted limb-length discrepancy at maturity would be how many centimeters?
Explanation
The distal femoral epiphysis grows approximately 1 cm per year and in boys, growth ceases at approximately age 16 years. Therefore, the patient's limb-length discrepancy at maturity would be 12 cm (9 cm plus the 3-cm discrepancy he has from the previous surgery). Little DG, Nigo L, Aiona MD: Deficiencies of current methods for the timing of epiphyseodesis. J Pediatr Orthop 1996;16:173-179.
Question 513
High Yield
Which of the following structures runs through the site indicated by the arrow in Figure 11?

Explanation
The vertebral artery traverses through the arcuate foramen after exiting the lateral aspect of C1 and before entering the skull. The foramen usually is not fully formed, but a complete foramen such as this one has been reported in up to 18% of patients. Stubbs DM: The arcuate foramen: Variability in distribution related to race and sex. Spine 1992;17:1502-1504.
Question 514
High Yield
What postoperative complication occurs at a significantly higher rate in patients undergoing bilateral simultaneous total knee arthroplasty than in patients undergoing unilateral total knee arthroplasty?
Explanation
Parvizi and associates studied the 30-day mortality rate after more than 22,000 total knee arthroplasties and found that the rate after bilateral total knee arthroplasty was significantly higher than after unilateral total knee arthroplasty. Aseptic loosening, bleeding, and range of motion have not been shown to be statistically different between patients who had unilateral and simultaneous bilateral total knee arthroplasty.
Question 515
High Yield
Dislocation following primary total hip arthroplasty is more likely to occur in which of the following situations?
Explanation
Dislocation following total hip arthroplasty is twice as common in women than in men. It is more likely to occur in older patients. There is no clear association between dislocation and the method of fixation or the type of bearing, so long as the bearing diameter is the same.
Question 516
High Yield
A 57-year-old man with type I diabetes mellitus has had a tender, erythematous right sternoclavicular joint for the past 2 weeks. Radiographs reveal mild osteolysis without arthritic changes, within normal limits. Management should consist of

Explanation
Sternoclavicular joint sepsis is a rare condition that is most often restricted to patients who are immunocompromised, diabetic, or IV drug abusers. Examination commonly reveals a tender, painful, and possibly swollen sternoclavicular joint. If suspicion remains high following a thorough history, physical examination, radiographs, and routine blood tests, joint aspiration should be performed prior to incision and drainage or administration of antibiotics. Bremner RA: Monarticular noninfected subacute arthritis of the sternoclavicular joint. J Bone Joint Surg Br 1959;41:749-753.
Question 517
High Yield
A 12-year-old boy falls from a bicycle. A radiograph of his injured shoulder is shown in Figure 41. What is the optimal method of treatment?

Explanation
The radiograph reveals a distal clavicle fracture. In children, a periosteal sleeve will remain attached to the intact coracoclavicular ligament, and as such, remodeling can be expected. Therefore, nonsurgical management with a sling is preferred. Surgical treatment is not necessary, and a shoulder spica cast offers no advantage over a simple sling.
Question 518
High Yield
A 35-year-old man has profound deltoid weakness after sustaining a traumatic anterior shoulder dislocation 6 weeks ago. Electromyographic (EMG) studies confirm an axillary nerve injury. Follow-up examination at 3 months reveals no recovery of function. What is the best course of action?
Explanation
Documenting the status of recovery at this time is appropriate; therefore, repeat EMG studies should be conducted to check for early signs of reinnervation. Timing of nerve exploration in this setting is debated, with authors suggesting exploration if there is no sign of recovery at 6 to 9 months. Perlmutter GS: Axillary nerve injury. Clin Orthop 1999;368:28-36. Artico M, Salvati M, D'Andrea V, et al: Isolated lesions of the axillary nerves: Surgical treatment and outcome in twelve cases. Neurosurgery 1991;29:697-700. Vissar CP, Coene LN, Brand R, et al: The incidence of nerve injury in anterior dislocation of the shoulder and its influence on functional recovery: A prospective clinical and EMG study. J Bone Joint Surg Br 1999;81:679-685.
Question 519
High Yield
An 8-year-old boy with severe hemophilia A (factor VIII) and no inhibitor is averaging eight transfusions per month for bleeding into the right ankle. Examination shows synovial hypertrophy; range of motion consists of 0 degrees of dorsiflexion and 20 degrees of plantar flexion. The patient's knees, elbows, and left ankle have no restriction of motion. Standing radiographs of the right ankle are shown in Figure 18. Management should consist of

Explanation
The patient has bilateral hypertrophic synovitis that is causing repeated hemarthroses and progressive arthropathy. Ankle synovectomy in patients with hemophilia is effective in significantly reducing the rate of joint bleeding and in slowing the progression of the arthropathy; therefore, bilateral synovectomies is the treatment of choice. Range of motion can be effectively maintained after ankle synovectomy. Bracing and prophylactic transfusions would be ineffective at this time. Ankle arthrodesis should be reserved for patients with severe pain. Compared with patients who have juvenile rheumatoid arthritis, patients with hemophilia generally do not have involvement of the subtalar joint and rarely require a pantalar arthrodesis. Greene WB: Synovectomy of the ankle for hemophilic arthropathy. J Bone Joint Surg Am 1994;76:812-819.
Question 520
High Yield
Figure 30 shows an axial T1-weighted MRI scan of a patient's right shoulder. The arrows are pointing to what normal structure?

Explanation
Tears of the pectoralis major tendon are frequently missed during examination. MRI provides excellent visualization of the tendon if the study extends low enough down the arm. The pectoralis major tendon inserts on the crest of the greater tubercle of the humerus, just lateral to the long head of the biceps tendon. The latissimus dorsi tendon inserts medial to the long head of the biceps tendon on the lesser tubercle. The subscapularis tendon inserts on the lesser tuberosity more proximally. The deltoid insertion is more distal. Connell DA, Potter HG, Sherman MF, et al: Injuries of the pectoralis major muscle: Evaluation with MR imaging. Radiology 1999;210:785-791. Carrino JA, Chandnanni VP, Mitchell DB, et al: Pectoralis major muscle and tendon tears: Diagnosis and grading using magnetic resonance imaging. Skeletal Radiol 2000;29:305-313.
Question 521
High Yield
A 13-year-old boy is comatose and has irregular breathing after being struck by a car while riding his bicycle. Auscultation suggests a pneumothorax on the right side and swelling about the right arm and leg. Initial management should consist of
Explanation
The first priority is to gain control of the airway with intubation. Following intubation, management should consist of ventilation and placement of a chest tube if needed, vascular access and circulatory stabilization, radiographs of the cervical spine and chest, and CT of the brain. American College of Surgeons Committee on Trauma. Advanced Trauma Life Support Course. Instructor's Manual. Chicago, IL, American College of Surgeons, 1984.
Question 522
High Yield
Figures 22a and 22b show the radiograph and sagittal MRI scan of the upper cervical spine of a 62-year-old woman who has had a long history of rheumatoid arthritis. Following hospitalization and skeletal traction, her symptoms improve significantly, her neurologic examination returns to normal, and repeat radiographs show a normal occiput and C1-C2 relationship. Treatment should now include


Explanation
Although opinions differ on whether a decompression is indicated in a patient with symptomatic basilar invagination, it is generally agreed that occipitocervical stabilization is indicated. This has been done with and without concomitant arthrodesis. Crockard HA, Grob D: Rheumatoid arthritis upper cervical involvement, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, p 701.
Question 523
High Yield
Figure 18a shows the initial lateral radiograph of a 6-year-old girl who sustained a fracture in a motor vehicle accident and was treated in a cast 1 year ago. She now has the valgus deformity seen in Figure 18b. Treatment should consist of


Explanation
Proximal tibial metaphyseal fractures may result in late genu valgum as a result of asymmetric growth of the proximal tibia. These patients are best treated with observation because the deformity is likely to remodel. Osteotomy is not indicated and potentially will lead to recurrence. Stapling of the medial tibial physis is appropriate in patients who have a severe and progressive deformity. Cozen L: Knock-knee deformity in children: Congenital and acquired. Clin Orthop 1990;258:191-203. Jackson DW, Cozen L: Genu valgum as a complication of proximal tibial metaphyseal fractures in children. J Bone Joint Surg Am 1971;53:1571-1578. Brammar TJ, Rooker GD: Remodeling of valgus deformity secondary to proximal metaphyseal fracture of the tibia. Injury 1998;29:558-560. Ogden JA, Ogden DA, Pugh L, et al: Tibia valga after proximal metaphyseal fractures in childhood: A normal biologic response. J Pediatr Orthop 1995;15:489-494.
Question 524
High Yield
A 25-year-old man shot himself at the base of the right index finger while cleaning his handgun. Examination reveals that the finger is cool and cyanotic. A clinical photograph and radiograph are shown in Figures 44a and 44b. What is the recommended treatment?


Explanation
The gunshot wound has caused injury to multiple systems: bone, vascular, skin, and tendon; therefore, the treatment of choice is amputation. An immediate ray amputation allows for a more rapid return to activities and less time off work. Peimer CA, Wheeler DR, Barrett A, et al: Hand function following single ray amputation. J Hand Surg Am 1999;24:1245-1248.
Question 525
High Yield
An 8-year-old boy sustained an isolated distal radial fracture that was reduced and immobilized with 10 degrees of residual dorsal tilt. What is the next step in management?

Explanation
Distal radial fractures in children are common, and a large amount of displacement is acceptable. In general, 20 degrees of dorsal displacement and complete bayonet apposition in girls to age 12 years and in boys to age 14 years can be expected to remodel with an excellent outcome. The potential for increased fracture displacement and subsequent malunion may exist in up to one third of patients with displaced fractures with less than anatomic reduction. Therefore, early follow-up is recommended and remanipulation is indicated should loss in reduction occur. Consideration for percutaneous pinning of isolated distal radial fracture is reasonable in patients with little growth remaining. In these patients, higher rates of redisplacement exist with little chance for remodeling. Gibbons CL, Woods DA, Pailthorpe C, et al: The management of isolated distal radius fractures in children. J Pediatr Orthop 1994;14:207-210. McLauchlan GJ, Cowan B, Annan IH, et al: Management of completely displaced metaphyseal fractures of the distal radius in children. J Bone Joint Surg Br 2002;84:413-417. Proctor MT, Moore DJ, Patterson JH: Redisplacement after manipulation of distal radial fractures in children. J Bone Joint Surg Br 1993;75:453-454.
Question 526
High Yield
Figure 35 shows the AP radiograph of a patient who underwent a previous upper tibial osteotomy (UTO). The patient may be at risk for which of the following during total knee arthroplasty (TKA)?

Explanation
The results of TKA for patients with a prior UTO are reported to be slightly suboptimal. The major problems are patella baja, difficulty in exposure, and instability. Most of the patients exhibit some degree of instability prior to TKA, and ligamentous balancing may be difficult. Ligamentous structures are at risk of rupture during the difficult exposure. The problem of ligamentous balancing is exacerbated by the change in the joint slope that can occur after UTO. Parvizi J, Hanssen AD, Spangehl MJ: Total knee arthroplasty following proximal tibial osteotomy: Risk factors for failure. J Bone Joint Surg Am 2004;86:474-479.
Question 527
High Yield
Figure 27 shows the radiograph of a 26-year-old man who sustained a closed head injury and a closed elbow dislocation 6 weeks ago. Examination reveals 65 degrees to 115 degrees of flexion, and intensive physical therapy has resulted in no improvement. A decision regarding the timing of surgical correction of the contracture should be based on

Explanation
The patient has heterotopic ossification, a more common finding in patients who have sustained head injuries. Treatment will require removal of the heterotopic bone and anterior and posterior capsulectomies. The main concern about timing is the possible recurrence of heterotopic bone. While an extended wait was once thought necessary, this is no longer true. The timing is based on the time since injury and evidence of bone maturation on plain radiographs. A sharp marginal demarcation of the new bone and a trabecular pattern within it are usually present 3 to 6 months after onset, indicating that it is safe to proceed with surgical excision. It is not necessary to wait more than 6 months. Bone scan results are not good indicators because they may remain "hot" for long periods of time. The levels of alkaline phosphatase and serum calcium-phosphorus product do not need to be measured.
Question 528
High Yield
A 40-year-old woman has a symptomatic mass on the anterior aspect of the ankle. She reports no constitutional symptoms. An MRI scan is shown in Figure 12. What is the most likely diagnosis?

Explanation
The MRI scan reveals a lobular mass that is below the vitamin E tablet marker taped to the skin. This is juxtaposed to the tibialis anterior tendon. It is slightly more enhanced than the surrounding subcutaneous fat and is consistent with a ganglion. Osteosarcoma, aneurysmal bone cyst, or unicameral bone cyst all would demonstrate enhancement or pathology in the bone. This is clearly a well-defined soft-tissue mass. Gouty tophi show low to intermediate signal on T1- and T2-weighted images. Kransdorf MJ, Jelinek JS, Moser RP Jr, et al: Soft tissue masses: Diagnosis using MR imaging. Am J Roentgenol 1989;153:541-547. Wetzel LH, Levine E: Soft-tissue tumors of the foot: Value of MR imaging for specific diagnosis. Am J Roentgenol 1990;155:1025-1030.
Question 529
High Yield
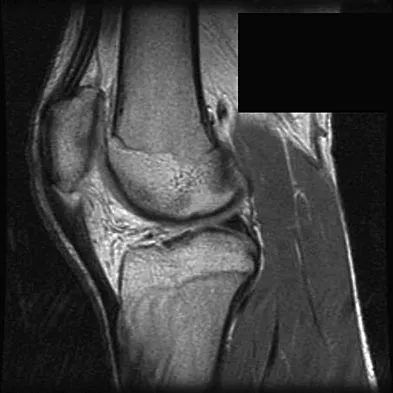
A 17-year-old basketball player and pole vaulter who has had anterior knee pain for the past 18 months now reports a recent inability to jump. Based on the MRI scan shown in Figure 11, management should consist of
Explanation
The MRI scan reveals a partial patellar tendon rupture in conjunction with chronic patellar tendinitis. Mild and moderate patellar tendinitis may be treated nonsurgically with rest, stretching, strengthening, and anti-inflammatory drugs. Severe tendinopathy or extensor mechanism disruption is best treated surgically with tendon debridement and repair. Al-Duri ZA, Aichroth PM: Surgical aspects of patella tendonitis: Techniques and results. Am J Knee Surg 2001;14:43-50.
Question 530
High Yield
A 16-year-old girl has had pain and swelling along the medial arch of her left foot for the past 3 months. She also reports pain from shoe wear and while running. Nonsteroidal anti-inflammatory drugs have failed to provide relief. Radiographs are shown in Figures 40a through 40c. What is the next most appropriate step in management?



Explanation
Nonsurgical management of a symptomatic accessory navicular should be attempted prior to surgery. Good relief is often obtained with a semi-rigid orthosis with a medial arch support. Myerson MS: Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, p 655.
Question 531
High Yield
A 21-year-old college defensive lineman sustains a minimally displaced (less than 1 mm) midthird scaphoid fracture during the first game of the season. Management should consist of
Explanation
The union rate for minimally displaced midthird scaphoid fractures is quite high with cast immobilization while allowing a return to sports. Inadequate immobilization results in a much higher nonunion rate. Early fixation and rehabilitation have been proposed for sports or positions that are not amenable to cast immobilization. While immobilization of a nondisplaced fracture results in an acceptably high union rate, there is no advantage to fixation in conjunction with immobilization in the course of healing. With adequate immobilization and protection, play restrictions until healing has occurred are unnecessary. Rettig AC, Kollias SC: Internal fixation of acute stable scaphoid fractures in the athlete. Am J Sports Med 1996;24:182-186. Rettig AC, Weidenbener EJ, Gloyeske R: Alternative management in midthird scaphoid fractures in the athlete. Am J Sports Med 1994;22:711-714.
Question 532
High Yield
A 55-year-old woman with polyarticular rheumatoid arthritis has had progressively increasing left shoulder pain for the past 2 years despite nonsurgical management. No focal weakness is noted during examination of the shoulder. AP and axillary radiographs are shown in Figures 47a and 47b. Treatment should consist of


Explanation
Unconstrained total shoulder arthroplasty has been found to yield satisfactory results in a high percentage of patients with rheumatoid involvement of the glenohumeral joint. Pain relief has been more predictable with total shoulder arthroplasty than humeral arthroplasty, and a glenoid component is favored when there is sufficient glenoid bone stock and an intact rotator cuff. Constrained or fixed-fulcrum devices have an unacceptably high failure rate because of loosening. Glenohumeral arthrodesis is avoided when the deltoid or rotator cuff is functioning because the functional results after arthroplasty are superior when compared with results of arthrodesis. Arthroscopic synovectomy may be helpful in early stages of the disease before extensive cartilage damage has occurred. Boyd AD Jr, Thomas WH, Scott RD, Sledge CB, Thornhill TS: Total shoulder arthroplasty versus hemiarthroplasty: Indications for glenoid resurfacing. J Arthroplasty 1990;5:329-336.
Question 533
High Yield
Intramembranous ossification during fracture repair is characterized by absence of which of the following elements?
Explanation
Intramembranous ossification occurs through the direct formation of bone without the formation of a cartilaginous intermediate. Clinically, both intramembranous and endochondral ossification occur simultaneously during fracture healing; however, the latter is characterized by the differentiation and maturation of chondrocytes, vascular invasion of a hypertrophic cartilage matrix, and bone formation. Collagens type II and X are cartilage specific and would be characteristic of endochondral ossification, not intramembranous ossification. Li J, Sandell LJ: Transcriptional regulation of cartilage-specific genes, in Rosier RN, Evans C (eds): Molecular Biology in Orthoapedics, Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 21-24.
Question 534
High Yield
Which of the following complications is associated with the use of a short cephalomedullary nail for fixation of intertrochanteric hip fractures?

Explanation
Implant-related fractures following hip fracture surgery were reported by Robinson and associates and showed that the risk of an ipsilateral femoral fracture is significantly increased with the use of short cephalomedullary nails as compared to a compression hip screw. The use of short cephalomedullary nails has not been shown to increase the risk of deep venous thrombosis or nonunion. Cephalomedullary nails overall have decreased surgical blood loss when compared to use of sliding-compression hip-screw devices. Robinson CM, Adams CI, Craid M, et al: Implant-related fractures of the femur following hip fracture surgery. J Bone Joint Surg Am 2002;84:1116-1122.
Question 535
High Yield
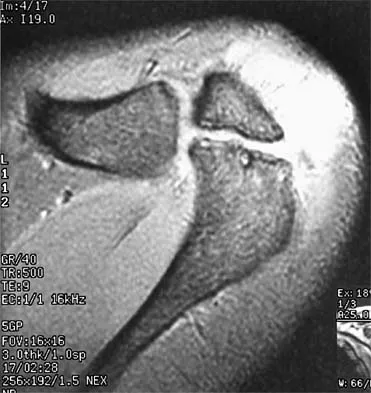
Figure 37 shows a coronal T2-weighted MRI scan. What is the name of the labeled torn structure?

Explanation
The labeled structure is the LCL, and it is avulsed from the lateral humeral epicondyle. This is the most common site of injury for the LCL. The biceps and brachialis tendon insertions are not well visualized in this section. The MCL and flexor/pronator origin are intact. Potter HG, Weiland AJ, Schatz JA, et al: Posterolateral rotatory instability of the elbow: Usefulness of MR imaging in diagnosis. Radiology 1997;204:185-189.
Question 536
High Yield
Which of the following statements best describes the outcome of the routine use of continuous passive motion (CPM) machines after total knee arthroplasty (TKA)?

Explanation
Although CPM machines are used widely in the United States for patients undergoing TKA, the benefit seems to be marginal, if any. Numerous randomized trials have shown that final outcomes after total knee arthroplasty are unaffected by the use of CPM machines postoperatively. Some studies have suggested that use of CPM may improve flexion in the first few weeks, but any short-term benefit from the machine was lost by intermediate-term follow-up. Aside from potential improvement in flexion within the first few postoperative weeks, there does not appear to be any benefit from the machines. There is no improvement in pain, ambulation, or extension. The cost-effectiveness of these machines has been questioned by many authors. Pellicci PM, Tria AJ, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 287-293. McInnes J, Larson MG, Daltroy LH, et al: A controlled evaluation of continuous passive motion in patients undergoing total knee arthroplasty. JAMA 1992;268:1423-1428.
Question 537
High Yield
A 22-year-old patient sustained a jamming injury to the right little finger. The lateral radiograph shown in Figure 18 reveals comminution of the base of the middle phalanx, with palmar and dorsal metaphyseal cortical involvement. The articular surface also is disrupted. Management should consist of

Explanation
This fracture, known as a pilon fracture, represents comminution of the base of the middle phalanx with both palmar and dorsal cortical disruption. The treatment method that allows the best function and fewest complications is indirect reduction achieved through specific dynamic splinting or the use of specifically designed proximal interphalangeal joint external fixators. Early mobilization can be achieved by either of these techniques. Volar plate arthroplasty is indicated for a simple fracture-dislocation of the proximal interphalangeal joint with comminution of the volar fracture fragment and dorsal dislocation of the remaining articular surface. Open reduction and internal fixation or percutaneous pinning adds surgical risks and scarring and typically will not provide added stability. Cast immobilization will not achieve the goal of early range of motion. Stern PJ, Roman RJ, Kiefhaber TR, McDonough JJ: Pilon fractures of the proximal interphalangeal joint. J Hand Surg Am 1991;16:844-850.
Question 538
High Yield
Which of the following is the strongest contraindication to unicompartmental knee arthroplasty (UKA)?
Explanation
UKA prostheses cannot substitute for an absent ACL, and if arthroplasty is indicated, these patients should receive a total knee arthroplasty rather than a UKA. Age is not an absolute contraindication, and the procedure has been advocated for young patients as well as older patients if they meet the appropriate indications for an arthroplasty. Varus deformities of the mechanical axis of up to 10 degrees generally are not a contraindication to unicompartmental arthroplasty, as long as the knee can be properly balanced at the time of surgery. Modest chondromalacia of the patellofemoral joint, especially if asymptomatic, is not a contraindication to UKA. Lotke PA (ed): Knee Arthroplasty: Master Techniques in Orthopaedic Surgery. New York, NY, Raven Press, 1995, pp 275-293. Insall JN, Windsor RE, Scott WN, et al (eds): Surgery of the Knee, ed 2. New York, NY, Churchill Livingstone, 1993, pp 805-814.
Question 539
High Yield
An otherwise healthy 35-year-old woman reports dorsal wrist pain and has trouble extending her thumb after sustaining a minimally displaced fracture of the distal radius 3 months ago. What is the next most appropriate step in management?
Explanation
Extensor pollicis longus tendon rupture can occur after a fracture of the distal radius, even a minimally displaced one. Poor vascularity of the tendon within the third dorsal compartment is the suspected etiology, not the displaced fracture fragments. Tendon transfer will suitably restore active extension of the thumb interphalangeal joint. Christophe K: Rupture of the extensor pollicis longus tendon following Colles fracture. J Bone Joint Surg Am 1953;35:1003-1005.
Question 540
High Yield
A 26-year-old man with chronic lateral ankle instability underwent a modified Broström procedure 8 months ago. He reports persistent pain and swelling of the lateral ankle. Examination reveals lateral ankle tenderness and swelling and a negative anterior drawer test. Laboratory studies show a WBC count of 6,500/mm3 and an erythrocyte sedimentation rate of 15 mm/h. Radiographs of the ankle are normal. What is the most likely cause of this problem?
Explanation
Chronic lateral instability is commonly associated with a longitudinal split tear of the peroneus brevis tendon. The interrelationship of lateral ankle instability with superior retinacular laxity and resultant peroneus brevis split can account for persistent lateral ankle pain in this patient. Surgical treatment must identify and correct the underlying tendon pathology and should attempt to repair or debride the peroneus brevis tendon, reconstruct the superior peroneal retinaculum, flatten the posterior edge of the fibula by removing the sharp bony prominence, or deepening the fibular groove, along with addressing lateral ankle ligamentous instability. The laboratory values are not consistent with infection. A negative anterior drawer test confirms stability of the repair. Ankle arthritis is not seen on radiographs and usually takes longer than 3 months to develop. Bonnin M, Tavernier T, Bouysset M: Split lesions of the peroneus brevis tendon in chronic ankle laxity. Am J Sports Med 1997;25:699-703.
Question 541
High Yield
Figures 28a and 28b show the sagittal and axial lumbar MRI scans of a 72-year-old man who reports dull aching back pain that spreads to his legs, calves, and buttocks. He has had the pain for several years and it is precipitated by standing and walking and relieved by sitting. His symptoms have been worsening over the past year and he notes that he is leaning forward while walking to help relieve his symptoms. He has had no treatment to date. What is his prognosis if he chooses to pursue nonsurgical management for this condition?

Explanation
The patient has lumbar spinal stenosis and the MRI scans reveal the pathology at L4-5, which is secondary to posterior disk bulging and hypertrophy and infolding of the ligamentum flavum, as well as degenerative facet arthrosis. The degree of spinal stenosis is moderate and his symptoms are positional in nature. Tadokoro and associates reported on a prospective study of 89 patients older than 70 years of age who underwent nonsurgical management for lumbar spinal stenosis. They found the prognosis to be relatively good with patients scoring at "excellent" or "good" for activities of daily living at final follow-up. However, they did note that patients with a complete block on myelography did not respond favorably to nonsurgical management. Amundsen and associates reported on a 10-year prospective study comparing surgical care to nonsurgical management. They concluded that, while the long-term results largely favored surgical treatment, more than half of the nonsurgically managed patients had a satisfactory outcome. They also concluded that a delay of surgery for some months did not worsen the prognosis. Therefore, their recommendation was for an initial primarily nonsurgical approach. Amundsen T, Weber H, Nordal HJ, et al: Lumbar spinal stenosis: Conservative or surgical management? A prospective 10-year study. Spine 2000;25:1424-1435. Hilibrand AS, Rand N: Degenerative lumbar stenosis: Diagnosis and management. J Am Acad Orthop Surg 1999;7:239-249.
Question 542
High Yield
A 35-year-old man is seen for evaluation of his left ankle following multiple previous ankle sprains and frequent episodes of the ankle giving way. Examination reveals marked laxity about the lateral ankle with associated tenderness along the peroneal tendons. Physical therapy, anti-inflammatory drugs, and supportive bracing have failed to provide relief. An MRI scan shows peroneal tenosynovitis and a possible tear. He elects to undergo a peroneal tendon repair and lateral ligament reconstruction. Which of the following best describes the structure labeled "A" in Figure 45?
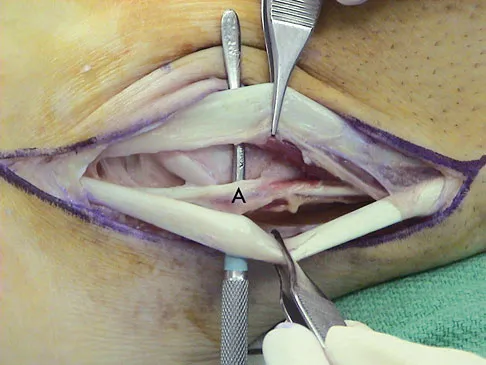
Explanation
The structure labeled "A" is a peroneus quartus, a supernumary muscle arising most commonly from the peroneus brevis. The presence of peroneus quartus is not uncommon, with an incidence of up to 21%, and is associated with lateral ankle pain and peroneal tendon symptoms, theoretically as a result of mass effect within the peroneal tendon sheath. Zammit J, Singh D: The peroneus quartus muscle: Anatomy and clinical relevance. J Bone Joint Surg Br 2003;85:1134-1137.
Question 543
High Yield
In the preoperative planning of revision acetabular reconstruction, the surgeon should identify significant posterior column deficiency by noting which of the following radiographic features?
Explanation
Proximal and medial migration of the femoral head usually indicates deficiencies of the dome or anterior column. Wear of the polyethylene may result in osteolysis and impingement, which are not indicative of any major bone deficiency. A significant osteolytic lesion in the ischium may represent a major posterior column deficiency that can create a technical challenge during the reconstruction. Paprosky WG, Magnus RE: Principles of bone grafting in revision total hip arthroplasty: Acetabular technique. Clin Orthop 1994;298:147-155.
Question 544
High Yield
Figure 51 shows the radiograph of a 42-year-old construction worker who has pain and limited motion in his dominant elbow. Management consisting of nonsteroidal anti-inflammatory drugs and cortisone has failed to provide relief. What is the next most appropriate step in treatment?

Explanation
The patient has symptomatic primary osteoarthritis of the elbow with multiple loose bodies. Given his age and occupation, an elbow arthroplasty is not an option. Arthroscopic debridement and removal of loose bodies has been shown to be effective for osteoarthritis of the elbow. Gramstad GD, Galatz LM: Management of elbow osteoarthritis. J Bone Joint Surg Am 2006;88:421-430.
Question 545
High Yield
During placement of an external fixator for a distal radius fracture, the most commonly injured nerve is a branch of which of the following nerves?

Explanation
Pin track infections and sensory injuries are among the most common complications of external fixation for distal radius fractures. The proximal pins of most distal radius external fixators are placed in the "bare area" of the distal radius, about four finger-breadths above the radial styloid. This corresponds to the area where the dorsal sensory branch of the radial nerve penetrates the fascia dorsal to the brachioradialis tendon to become a subcutaneous structure. Injury to the superficial radial nerve may produce painful dysesthesias and neuromas.
Question 546
High Yield
A 21-year-old male construction worker fell from a roof and sustained an injury to his left foot. Radiographs and CT scans are shown in Figures 24a through 24e. Compared to nonsurgical management, surgical treatment offers which of the following advantages?



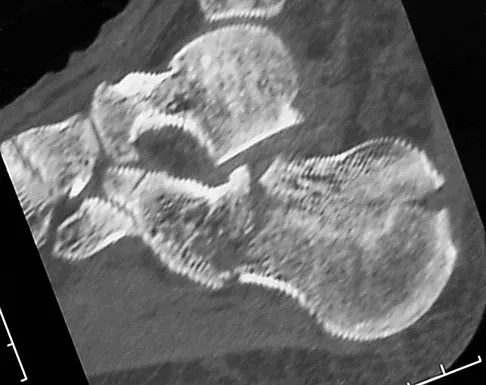
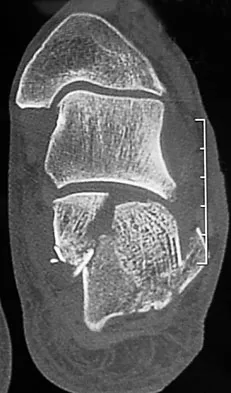
Explanation
The radiographs and CT scans show a displaced intra-articular calcaneal fracture, with loss of calcaneal height and length. Recent multicenter, randomized, prospective studies suggest that surgical treatment of displaced intra-articular calcaneal fractures is associated with an almost six-fold decrease in the risk of posttraumatic subtalar arthritis (necessitating subtalar arthrodesis) compared to nonsurgical treatment. Despite ongoing controversy, surgical treatment has not been shown to be advantageous with respect to activity, time to return to work, or subtalar joint range of motion. A nonunion of a calcaneal fracture is exceedingly rare regardless of the treatment method. Buckley R, Tough S, McCormack R, et al: Operative compared with nonoperative treatment of displaced intra-articular calcaneal fractures: A prospective, randomized, controlled multicenter trial. J Bone Joint Surg Am 2002;84:1733-1744.
Question 547
High Yield
A 12-year-old girl has progressive development of cavus feet. Examination reveals slightly diminished vibratory sensation on the bottom of the foot. Reflexes are 1+ at the knees and ankles. Motor examination shows that all muscles are 5/5 in the foot, except the peroneal and anterior tibial muscles are rated as 4+/5. Which of the following studies is considered most diagnostic?
Explanation
The patient most likely has a form of Charcot-Marie-Tooth disease, or hereditary motor sensory neuropathy (HMSN). The most common varieties can now be diagnosed by DNA testing. Mutations have been detected in the peripheral myelin protein-22 (PMP-22) gene in HMSN type IA and in the connexin gene in the x-linked HMSN. Specific DNA diagnosis is useful in genetic counseling. Routine chromosomal testing most likely would not detect these mutations. Nerve conduction velocity study results are normal in some types of HMSN, and delayed nerve conduction, when found, indicates a peripheral neuropathy but does not specify the type or inheritance pattern. Biopsy of the sural nerve or of the quadriceps can be informative in some patients, but is not as specific as DNA testing. These procedures are most often reserved for patients with negative DNA test results. Chance PF: Molecular genetics of hereditary neuropathies. J Child Neurol 1999;14:43-52.
Question 548
High Yield
Figure 24 shows the radiograph of a 4-year-old girl with spina bifida. Examination reveals an L3 motor level, excellent sitting and standing balance, and satisfactory range of motion at the hips. Management should consist of

Explanation
Children with spina bifida and bilateral symmetrical dislocation of the hips usually do not require treatment. A level pelvis and good range of motion of the hips are more important for ambulation than reduction of bilateral hip dislocations. Because the patient has good sitting and standing balance and good range of motion, maintenance of that range of motion and symmetry is more important than reduction. Surgery is not recommended.
Question 549
High Yield
What is the most likely complication following treatment of the humeral shaft fracture shown in Figure 6?
Explanation
The humerus was treated with an intramedullary nail. Findings from two prospective randomized studies of intramedullary nailing or compression plating of acute humeral fractures have shown approximately a 30% incidence of shoulder pain with antegrade humeral nailing. This is the most common complication in both of these series. Nonunions are present in approximately 5% to 10% of humeral fractures treated with an intramedullary nail. Infection has an incidence of approximately 1%. Elbow injury is unlikely unless the nail is excessively long. Rarely, injury to the radial nerve is possible if it is trapped in the intramedullary canal. Chapman JR, Henley MB, Agel J, et al: Randomized prospective study of humeral shaft fracture fixation: Intramedullary nails versus plates. J Orthop Trauma 2000;14:162-166.
Question 550
High Yield
Figure 38 shows the radiograph of a 16-year-old wrestler who injured his elbow when he was thrown to the mat by his opponent. To minimize additional trauma to the medial soft tissues, the elbow should be reduced in

Explanation
The elbow dislocates by a three-dimensional movement of supination and valgus during flexion. Additional trauma during reduction is minimized by recreating the deformity and reducing the elbow in supination. The actual maneuver includes full supination (actually hypersupination) of the elbow in a valgus position. This is followed by pushing the olecranon distally in line with the long axis of the ulna while swinging the elbow into varus, and then relaxing the supination torque. Postreduction stability is enhanced in pronation, except when the soft-tissue disruption is extensive. O'Driscoll SW: Elbow dislocations, in Morrey BF (ed): The Elbow and Its Disorders, ed 2. Philadelphia, PA, WB Saunders, 1993, p 414.
Question 551
High Yield
Removal of both hallucal sesamoids should be reserved as a salvage procedure because of the high incidence of which of the following postoperative complications?
Explanation
Removal of both sesamoids is associated with a high incidence of postoperative hallux valgus and cock-up deformity of the great toe because of weakening of the flexor hallucis brevis tendon. The sesamoids lie within these tendons and require meticulous repair following excision. Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2003, pp 17-25.
Question 552
High Yield
Following fixation of a displaced intra-articular fracture of the distal humerus through a posterior approach, what is the expected outcome?

Explanation
Following repair of a displaced intra-articular distal humerus fracture, the ability to regain full elbow range of motion is rare. Recent reports of olecranon osteotomy have yielded healing rates of between 95% to 100%. According to McKee and associates, patients can be expected to have residual loss of elbow flexion strength of 25%. McKee MD, Wilson TL, Winston L, et al: Functional outcome following surgical treatment of intra-articular distal humeral fractures through a posterior approach. J Bone Joint Surg Am 2000;82:1701-1707.
Question 553
High Yield
A 26-year-old man was thrown from a car and sustained the injury seen in Figures 44a and 44b. Nonsurgical management of this injury is recommended. Which of the following factors increases the risk of nonunion?


Explanation
The patient has a displaced comminuted clavicle middle one third fracture from a high-energy mechanism. Recent literature on high-energy clavicular fractures suggests a higher rate of nonunion than previously reported. A nonunion rate of 30% has been reported by Hill and associates when the fracture fragments are displaced more than 1.5 cm. In addition, several patients had neurologic symptoms related to the injury. Robinson and associates reported an increased risk of nonunion in women, elderly patients, comminuted fractures, and injuries with a lack of cortical contact. Hill JM, McGuire MH, Crosby LA: Closed treatment of displaced middle-third fractures of the clavicle gives poor results. J Bone Joint Surg Br 1997;79:537-539. Wick M, Muller EJ, Kollig E: Midshaft fractures of the clavicle with a shortening of more than 2 cm predispose to nonunion. Arch Orthop Trauma Surg 2001;121:207-211.
Question 554
High Yield
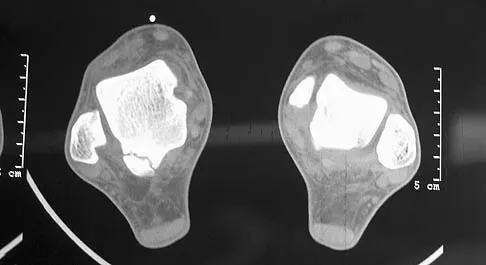
A 30-year-old man has had intermittent swelling of his right ankle for the past 6 months. He denies any history of trauma. Radiographs reveal osteolytic changes on both sides of the joint. An axial CT scan and a T2-weighted MRI scan are shown in Figures 40a and 40b. He undergoes surgical excision. An intraoperative photograph and a biopsy specimen are shown in Figures 40c and 40d. What is the most likely diagnosis?
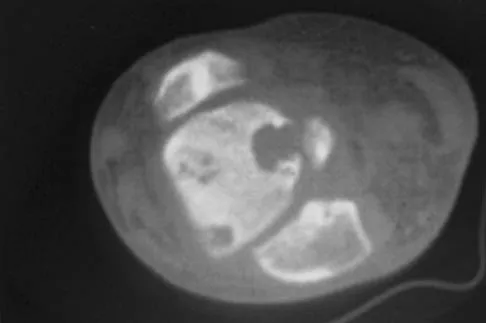
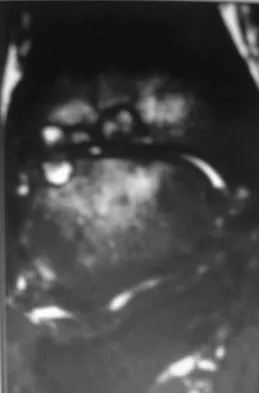
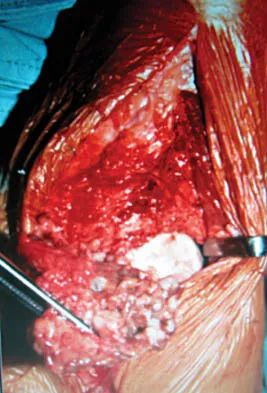
Explanation
Pigmented villonodular synovitis often presents with intermittent swelling and minimal pain. It often occurs around joints but may be found around tendon sheaths and bursal linings. Periarticular erosions involving both sides of joints are typical, and multiple joint involvement has been described. Portions of low-signal intensity on T1- and T2-weighted images are characteristic of hemosiderin-laden processes. High-signal content is suggestive of high water content. The combination of low-signal intensity areas in intra-articular lesions with or without osseous destruction is diagnostic of pigmented villonodular synovitis. Aspiration reveals bloody or brownish fluid. The treatment of choice is synovectomy performed arthroscopically or open. Recurrence is common. Walling AK: Soft tissue and bone tumors, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1007-1032.
Question 555
High Yield
Gaucher's disease is manifested by reticuloendothelial system macrophage accumulation of

Explanation
Gaucher's disease is characterized by macrophage accumulation of glucocerebroside that is caused by a deficiency of lysosomal enzyme glucocerebrosidase. It is an autosomal-recessive trait and is most commonly found in Ashkenazi Jews. Orthopaedic surgeons see patients with Gaucher's disease usually because of osteonecrosis of the hip. Calcium pyrophosphate is associated with pseudogout. Hydroxyproline is a breakdown product of collagen and is found in high levels in patients with Paget's disease. Homogentisic acid is associated with ochronosis (alkaptonuria). Beatty JH: Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 247-252. Goldblatt J, Sacks S, Beighton P: The orthopedic aspects of Gaucher disease. Clin Orthop 1978;137:208-214.
Question 556
High Yield
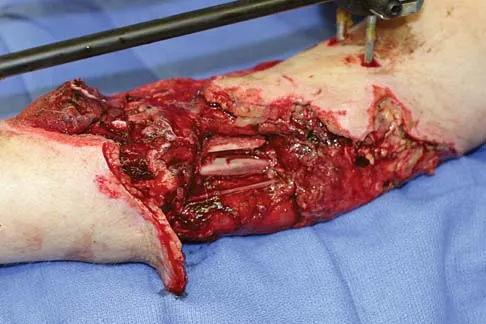
A 25-year-old left hand-dominant man has severe left shoulder pain after being involved in a high-speed motor vehicle accident. Examination reveals that he is unable to move the left shoulder. His neurovascular status is intact in the entire left upper extremity. A radiograph is shown in Figure 19. What is the most appropriate surgical management of this injury?

Explanation
In this young patient, every attempt must be made to retain the native proximal humerus; therefore, open reduction and internal fixation should be attempted of both the articular segment and tuberosities to the humeral shaft. This is best accomplished through an open approach. Shoulder arthroplasty should be reserved for the elderly and for failed internal fixation. Ko JY, Yamamoto R: Surgical treatment of complex fractures of the proximal humerus. Clin Orthop Relat Res 1996;327:225-237.
Question 557
High Yield
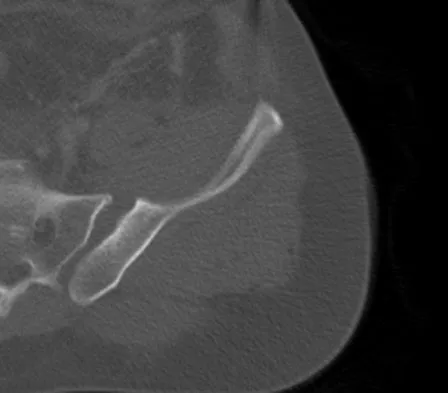
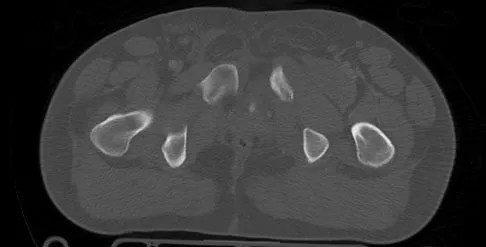
A 22-year-old cheerleader who fell from the top of a pyramid now reports anterior and posterior pelvic pain. A radiograph and CT scans are shown in Figures 43a through 43c. What is the best treatment for this injury?

Explanation
Symphyseal widening of greater than 2.5 cm and less than 5 cm denotes an AP II injury and a rotationally unstable pelvis. An AP II pelvic ring injury is best treated with anterior open reduction and internal fixation. Nonsurgical management is reserved for AP I injuries. Pelvic binders are used only acutely and should not be used for definitive management. Iliosacral screws usually are not necessary in the acute management of AP II injuries. Matta JM: Indications for anterior fixation of pelvic fractures. Clin Orthop Relat Res 1996;329:88-96. Templeman DC, Schmidt AH, Sems AS, et al: Diastasis of the symphysis pubis: Open reduction internal fixation, in Wiss D (ed): Masters Techniques in Orthopaedic Surgery-Fractures, ed 2. Philadelphia, PA, Lippincott Williams and Wilkins, 2006, pp 639-648.
Question 558
High Yield
A 17-year-old football player is unable to flex the distal interphalangeal (DIP) joint of his ring finger. He states that he injured the finger 6 weeks ago while attempting to tackle another player who pulled free from his grip, but he did not inform his coach at the time of the injury. Current radiographs show an observable fleck of bone volar to the base of the proximal phalanx. Treatment should consist of
Explanation
Flexor digitorum profundus ruptures are classified into three types. In type I, the tendon retracts into the palm. In type II, the tendon retracts to the level of the proximal phalanx, the vinculum remains intact, and the blood supply is preserved to the tendon. A small fleck of bony fragment observed at the A2 pulley is pathognomonic for a type II rupture. Successful primary repair of the type II rupture has been reported as late as 2 months after the injury. Type III injuries have large fragments of the distal phalanx attached and are caught distally by the A1 pulley. Type III ruptures can be repaired up to several months after the injury. Leddy JP: Avulsions of the flexor digitorum profundus. Hand Clin 1985;1:77-83.
Question 559
High Yield
Which of the following factors increases the risk of sciatic nerve injury in primary total hip arthroplasty (THA)?
Explanation
Injury to the sciatic nerve is a relatively rare but serious complication of THA. Dissection of the sciatic nerve is not typically done during primary THA, although the nerve can be identified during the surgical approach. An anterolateral approach to THA would not necessarily be associated with any greater incidence of sciatic nerve injury than other approaches. Screw fixation for the acetabular component is often a matter of surgeon preference. Provided that the anatomic safe zones for screw fixation (posterior inferior and posterior superior) are recognized, injury to the sciatic nerve from acetabular screws can be minimized. Restoration of anatomic length is important in primary THA. Overlengthening can result in sciatic nerve palsy. Developmental dysplasia of the hip can lead to a congenitally shortened extremity with concomitant congenital shortening of the associated neurovascular structures. Overlengthening of the extremity during THA for developmental dysplasia of the hip can lead to sciatic palsy. Osteonecrosis is not an associated risk factor for sciatic nerve palsy. DeHart MM, Riley LH Jr: Nerve injuries in total hip arthroplasty. J Am Acad Orthop Surg 1999;7:101-111.
Question 560
High Yield
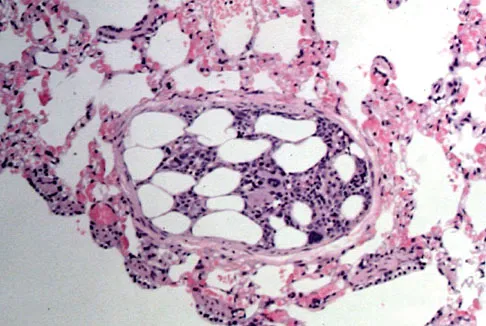
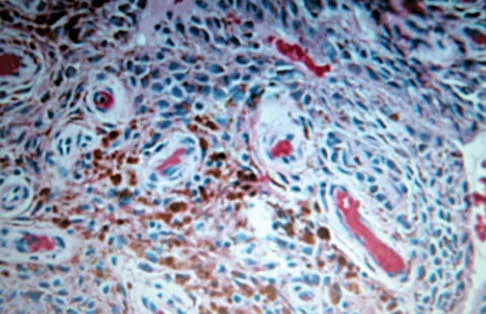
Figures 11a and 11b show the AP and lateral radiographs of a 32-year-old patient on hemodialysis who has increasing elbow pain and a visibly growing mass over the extensor surface. Figure 11c shows the photomicrograph of the biopsy specimen. What is the most likely diagnosis?


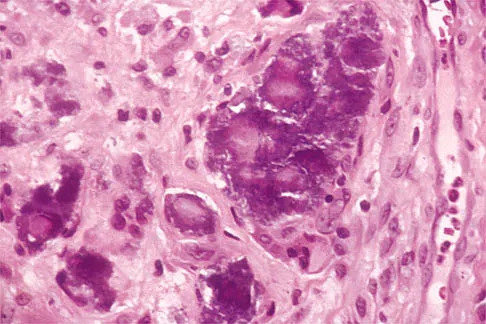
Explanation
The radiographic findings are classic for tumoral calcinosis; they are not consistent with myositis ossificans, fungal granuloma, or hemochromatosis. The condition typically appears as large aggregations of dense calcified lobules confined to the surrounding soft tissues. Hyperphosphatemia is a fundamental factor in many patients with this condition. Tumoral calcinosis also occurs in the setting of chronic renal failure when mineral homeostasis is not controlled. The histologic appearance is essentially a foreign body granuloma reaction. Multilocular cysts with purplish amorphous material are surrounded by thick connective tissue capsules. The fibrous walls contain numerous foreign body giant cells. Surgical excision is indicated if the tumor causes discomfort or interferes with function. Sisson HA, Murray RO, Kemp HBS (eds): Orthopaedic Diagnosis: Clinical, Radiological and Pathological Coordinates. New York, NY, Springer-Verlag, 1984.
Question 561
High Yield
A 16-year-old football player sustains a direct blow to the anterior aspect of his flexed right knee. Examination reveals a contusion over the anterior tibial tubercle and a small effusion. MRI scans are shown in Figures 33a through 33c. What is the most likely diagnosis?



Explanation
The MRI scans show disruption of the fibers of the PCL. Patients sustaining an isolated acute PCL injury can present with only minimal discomfort and have full range of motion. When examination reveals a contusion over the tibial tubercle and discomfort with the posterior drawer examination, with or without instability, a possible injury to the PCL should be considered. In acute injuries, the reported accuracy of MRI imaging for diagnosing PCL tears ranges from 96% to 100%. Resnick D, Kang HS: Internal Derangement of Joints: Emphasis on MRI Imaging. Philadelphia, PA, WB Saunders, 1997, pp 699-700. Harner CD, Hoher J: Evaluation and treatment of posterior cruciate ligament injuries. Am J Sports Med 1998;26:471-482.
Question 562
High Yield
Examination of a 45-year-old man with Charcot-Marie-Tooth disease reveals a cavus foot, a tight Achilles tendon, and forefoot callus formation. Radiographs reveal advanced degenerative changes in the hindfoot. Shoe wear modifications have failed to provide relief. Treatment should now consist of

Explanation
The patient has the typical end stage residuals from long-standing Charcot-Marie-Tooth disease. Initial management consisting of shoe wear modifications and orthotic devices is preferred, but these are not successful when the disease process has progressed. Surgical correction with calcaneal osteotomy or Achilles tendon lengthening and Steindler stripping is not indicated in the presence of significant hindfoot arthritis. Because this patient has findings consistent with hindfoot arthritis, a triple arthrodesis with correction of the cavus deformity is the preferred treatment. Roper BA, Tibrewal SB: Soft tissue surgery in Charcot-Marie-Tooth disease. J Bone Joint Surg Br 1989;71:17-20.
Question 563
High Yield
A 16-year-old girl injured her hip in a fall. Radiographs are shown in Figures 14a and 14b. She denies any history of pain prior to the fall and is currently asymptomatic. A bone scan, MRI scan, and biopsy specimens are shown in Figures 14c through 14f. What is the most likely diagnosis?



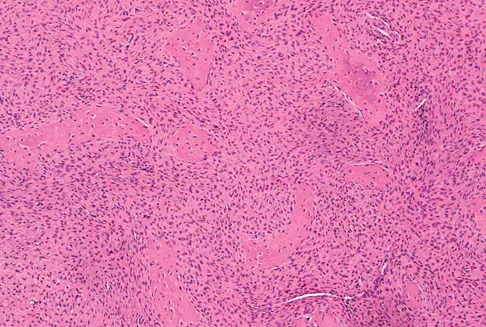
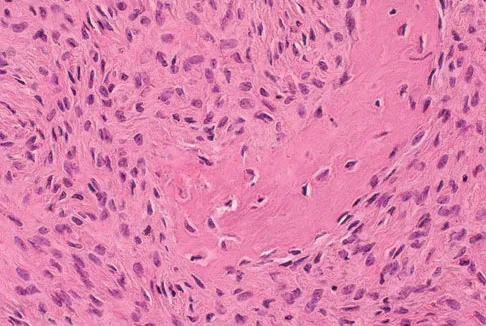
Explanation
Although the classic radiographic appearance of fibrous dysplasia is one of a central metaphyseal lesion with ground glass matrix, it is not unusual to see either a more radiodense-appearing lesion or a more peripheral location. The histologic finding of spicules of woven bone without osteoblastic rimming in a bland fibrous background is diagnostic of fibrous dysplasia. The imaging studies could be consistent with low-grade osteosarcoma, osteoblastoma, or osteomyelitis, but all have a very different histologic picture. Observation is indicated in the absence of symptoms, impending fracture, or deformity. Fibrous dysplasia most commonly occurs in the proximal femur. Huvos AG: Bone Tumors: Diagnosis, Treatment, and Prognosis. Philadelphia, PA, WB Saunders, 1991, pp 30-43.
Question 564
High Yield
When performing a total knee arthroplasty using modular components, what is the minimum recommended thickness of an ultra-high molecular weight polyethylene insert for a tibial component?
Explanation
Polyethylene wear has been identified as a major contributor to failure of total knee implants, of which thickness is an important factor. Several studies have shown that the minimum thickness should be 6 to 8 mm. While Wright and Bartel have shown that 6 to 8 mm has been recommended as the minimum thickness of an ultra-high molecular weight polyethylene insert for a tibial component in total knee arthroplasty, more recent work by Meding and associates and Worland and associates has verified the clinical efficacy of 4 mm of polyethylene in compression-molded anatomic graduated nonmodular components. Bartel DL, Bicknell VL, Wright TM: The effect of conformity, thickness, and material on stresses in ultra-high molecular weight components for total joint replacement. J Bone Joint Surg Am 1986;68:1041-1051. Wright TM, Bartel DL: The problem of surface damage in polyethylene total knee components. Clin Orthop 1991;273:261-263. Meding JB, Ritter MA, Faris PM: Total knee arthroplasty with 4.4 mm of tibial polyethylene: 10-year followup. Clin Orthop 2001;388:112-117.
Question 565
High Yield
What assay most directly assesses gene expression at the posttranslational level?
Explanation
Gene expression at the posttranslational level refers to proteins, as opposed to DNA or RNA. The only assay above that targets protein expression directly is the Western blot. Standard PCR is amplification of targeted DNA segments, regardless of whether or not they are actively expressed. Real-time PCR, Northern blot, and microarray expression profile analysis all quantify RNA as a means to determine posttranscriptional gene expression. Brinker MR: Cellular and molecular biology, immunology, and genetics in orthopaedics, in Miller MD (ed): Review of Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2001, pp 81-94.
Question 566
High Yield
Which of the following lumbar disk components has the highest tensile modulus to resist torsional, axial, and tensile loads?
Explanation
The annulus fibrosis has a multilayer lamellar architecture mode of type I collagen fibers. Each successive layer is oriented at 30 degrees to the horizontal in the opposite direction, leading to a "criss-cross" type pattern. This composition allows the annulus, which has the highest tensile modulus, to resist torsional, axial, and tensile loads.
Question 567
High Yield
Examination of an 18-year-old professional soccer player who was forcefully kicked across the shin while attempting a slide tackle reveals a marked effusion and limited motion of the knee. The tibia translates 12 mm posterior to the femoral condyles when the knee is held in 90 degrees of flexion. There is no posteromedial or posterolateral instability. Management should consist of

Explanation
The patient has an acute grade III posterior cruciate ligament injury. The majority of grade I and II injuries can be treated with protected weight bearing and quadriceps rehabilitation, and most patients can return to sports within 2 to 4 weeks. In contrast, grade III injuries require immobilization in full extension for 2 to 4 weeks to protect the posterior cruciate ligament and the other posterolateral structures presumed to be damaged. The mainstay of postinjury rehabilitation for all posterior cruciate ligament injuries is quadriceps strengthening exercises, which have been shown to counteract posterior tibial subluxation. Miller MD, Bergfeld JA, Fowler PJ, Harner CD, Noyes FR: The posterior cruciate ligament injured knee: Principles of evaluation and treatment. Instr Course Lect 1999;48:199-207.
Question 568
High Yield
The mother of an otherwise healthy 1-month-old infant reports that he is not moving his left leg after falling from his high chair 2 days ago. He has a temperature of 99.5 degrees F (37.5 degrees C). Examination reveals that the left thigh is moderately tender to palpation. Because the infant is apprehensive, range of motion is difficult to quantify, but appears to be normal at the hips and ankles. Range of motion of the left knee is approximately 25 degrees to 90 degrees. A radiograph of the leg is shown in Figure 27. Management should consist of

Explanation
The patient has a bucket-handle fracture of the distal femur with bilateral corner fractures of the distal femur and a transverse fracture of the proximal tibia. These fractures are virtually pathognomonic of child abuse. The infant should be admitted to the hospital, and child protection services should be notified for investigation of possible abuse. A skeletal survey should be obtained, along with laboratory studies that include a CBC, a platelet count, a prothrombin time, a partial thromboplastin time, and a bleeding time. Akbarnia BA: The role of the orthopaedic surgeon in child abuse, in Morrissy RT, Weinstein SL (eds): Lovell & Winter's Pediatric Orthopaedics, ed 4. Philadelphia, Pa, Lippincott-Raven, 1996, pp 1315-1334.
Question 569
High Yield
What is the most common organism found following a nail puncture wound through tennis shoes in a host without immunocompromise?
Explanation
The association of a nail puncture wound with a gram-negative infection (Pseudomonas aeruginosa) has been attributed to the local environmental factors in shoes. Osteomyelitis is rare, occurring only in about 1% of patients. Tetanus prophylaxis should be given if it is not up to date. While the remaining organisms listed are periodically involved, they are more common in patients who are immunocompromised or who have diabetes mellitus. Therefore, obtaining a culture of the infected wound is appropriate in such individuals because of the multifactorial nature of the infection. Green NE, Bruno J III: Pseudomonas infections of the foot after puncture wounds. South Med J 1980;73:146-149.
Question 570
High Yield
A 44-year-old man who sustained an elbow dislocation 3 months ago now reports pain and restricted elbow motion. Radiographs are shown in Figures 27a and 27b. Management should consist of


Explanation
The treatment of choice for an ankylosed chronically dislocated elbow is surgical reduction. Open reduction with application of an external fixator provides excellent results for this complex problem. Radial head arthroplasty is indicated for a radial head fracture that cannot be reconstructed. Attempts at closed reduction will be unsuccessful and should not be attempted in a stiff elbow. In chronic dislocations, direct reinsertion of injured ligaments is not feasible because of soft-tissue contracture. Jupiter J, Ring D: Treatment of unreduced elbow dislocation with hinged external fixation. J Bone Joint Surg Am 2002;84:1630-1635.
Question 571
High Yield
During an anterior retroperitoneal approach to the low lumbar spine, the iliac vessels are mobilized along the lateral side, allowing them to be retracted toward the midline. To gain adequate mobility of the common iliac vein for exposure of L5, it is important to identify which of the following structures?

Explanation
The iliolumbar vein is a large tributary that sits along the lateral surface of the common iliac vein. It can be quite substantial in size and must be identified prior to mobilizing the common iliac vein toward the midline. The other structures are not of surgical significance in performing this exposure.
Question 572
High Yield
A 30-year-old woman injures her knee while skiing. Based on the MRI scan shown in Figure 5, treatment should consist of

Explanation
The MRI scan demonstrates a grade III MCL tear. Basic science and clinical studies have shown that nonsurgical management is preferred for MCL tears. Functional rehabilitation and early motion have led to consistently better results than has surgical repair.
Question 573
High Yield
A 42-year-old woman has persistent thumb pain that she notes is worse with opening jars and turning her car key. Opponens splinting provides some relief, but she is poorly tolerant of the splint. Finkelstein's test is negative, and a carpometacarpal grind test is positive. The radiographs shown in Figures 48a and 48b reveal minimal degenerative changes at the first carpometacarpal joint. What is the best course of action?


Explanation
The woman has early basilar thumb arthritis. An extension osteotomy will redirect the force to the dorsal, more uninvolved portion of the first carpometacarpal joint and has been reported to alleviate pain in these patients. Arthrodesis is usually reserved for young, typically male laborers. Thermal shrinkage and denervation are considered experimental at this time. Interposition arthroplasty is typically used for more advanced stages of arthritis. Tomaino MM: Treatment of Eaton stage I trapeziometacarpal disease with thumb metacarpal extension osteotomy. J Hand Surg Am 2000;25:1100-1106. Pellegrini VD Jr, Parentis M, Judkins A, et al: Extension metacarpal osteotomy in the treatment of trapeziometacarpal osteoarthritis: A biomechanical study. J Hand Surg Am 1996;21:16-23.
Question 574
High Yield
In a patient with vertebral tuberculosis, which of the following characteristics is most predictive of progression of the kyphosis?

Explanation
In patients with vertebral tuberculosis, involvement of the anterior and posterior elements creates an instability and severe kyphotic collapse can occur. This characteristic has been shown to have a stronger association than level of involvement, age, or pretreatment degree of deformity. In the absence of instability, anterior growth can resume after treatment, leading to a decrease in the deformity. Rajasekaran S: The natural history of post-tubercular kyphosis in children: Radiological signs which predict late increase in deformity. J Bone Joint Surg Br 2001;83:954-962.
Question 575
High Yield
A patient undergoes the procedure shown in Figure 19. An important part of this procedure is preservation of what wrist ligament?

Explanation
Proximal row carpectomy is a salvage wrist procedure that yields a surprisingly stable construct. This has been attributed to two factors: 1) the congruency of the head of the capitate in the lunate fossa (this articulation is less congruent than the native lunate/lunate fossa relationship, but surprisingly stable), and 2) preservation of the radioscaphocapitate ligament, the most radial of the palmar extrinsic ligaments, which prevents ulnar subluxation after proximal row carpectomy.
Question 576
High Yield
A 6-year-old girl is referred for the elbow injury seen in Figure 2. What is the most appropriate treatment?

Explanation
The patient has a displaced lateral condyle fracture; therefore, simple immobilization for 3 to 8 weeks is likely to result in malunion or nonunion. Closed reduction of such injuries is rarely successful. The fracture is unstable, so fixation is required after open reduction. Because the fixation must cross the physis, smooth pins are indicated for the skeletally immature elbow. Open reduction with fixation has been shown to reduce the risk of delayed union and malunion. Beaty JH, Kasser JR: The elbow: Physeal fractures, apophyseal injuries of the distal humerus, avascular necrosis of the trochlea, and T-condylar fractures, in Beaty JH, Kasser JR (eds): Fractures in Children, ed 5. Philadelphia, PA, Lippincott Williams & Wilkins, 2001, pp 625-703. Rutherford A: Fractures of the lateral humeral condyle in children. J Bone Joint Surg Am 1985;67:851-856.
Question 577
High Yield
Staphylococcus aureus develops methicillin resistance through production of which of the following agents?
Explanation
Organisms may develop resistance to antibiotics by production of specific enzymes. S aureus develops methicillin resistance by production of penicillin-binding protein 2a (PBP2a). The strains of S aureus that have acquired the mecA gene for PBP2a are designated as methicillin-resistant S aureus (MRSA). The enzyme manifests resistance to covalent modification by beta-lactam antibiotics at the active-site serine residue in two ways. First, the microscopic rate constant for acylation (k2) is attenuated by three to four orders of magnitude over the corresponding determinations for penicillin-sensitive PBPs. Second, the enzyme shows elevated dissociation constants (Kd) for the noncovalent preacylation complexes with the antibiotics, the formation of which ultimately would lead to enzyme acylation. The two factors working in concert effectively prevent enzyme acylation by the antibiotics in vivo, giving rise to drug resistance. Catalase and oxidase are enzymes produced by some bacteria that confer virulence to the organism but do not make the organisms methicillin resistant. Glycocalix is the pericellular layer produced by bacteria that serves many functions including attachment to surfaces. Beta-lactam describes a class of antibiotics. Fuda C, Suvorov M, Vakulenko SB, et al: The basis for resistance to beta-lactam antibiotics by penicillin-binding protein 2a (PBP2a) of methicillin-resistant staphylococcus aureus. J Biol Chem 2004;279:40802-40806. Lim D, Strynadka NC: Structural basis for the beta lactam resistance of PBP2a from methicillin-resistant Staphylococcus aureus. Nat Struct Biol 2002;9:870-876.
Question 578
High Yield
A posterolateral approach to the tibial plafond proceeds between what two muscles?

Explanation
A posterolateral approach to the posterior malleolus proceeds between the lateral and deep posterior compartments. Distally, the peroneus brevis muscle lies most medially within the lateral compartment, and the flexor hallucis longus lies most laterally in the deep posterior compartment. Henry AK: Extensile Exposure, ed 2. Edinburgh, UK, Churchill Livingstone, 1973, pp 269-270.
Question 579
High Yield
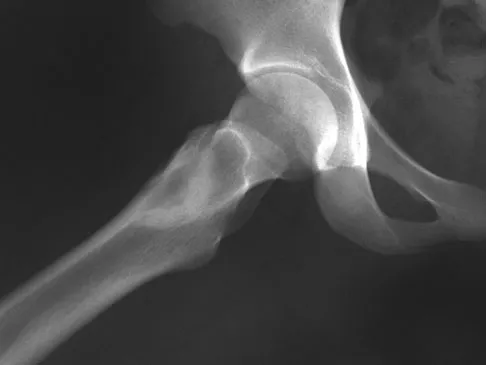
Figure 17 shows the AP radiograph of a 75-year-old man with right hip pain. The femoral component is loose. The mechanism of loosening is most likely secondary to

Explanation
The femoral construct shown in the radiograph has failed to produce ingrowth of the stem. The stem has subsided and rotated. Impingement of the trochanter did not occur until after the stem subsided. There is no evidence of osteolysis or third-body wear debris from the cerclage wire. A larger femoral stem needs to be implanted to achieve rigid fixation. Pelicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 217-238.
Question 580
High Yield
A 15-year-old wrestler sustains an abduction, hyperextension, and external rotation injury to his right shoulder. The MRI scan findings shown in Figures 27a and 27b are most consistent with

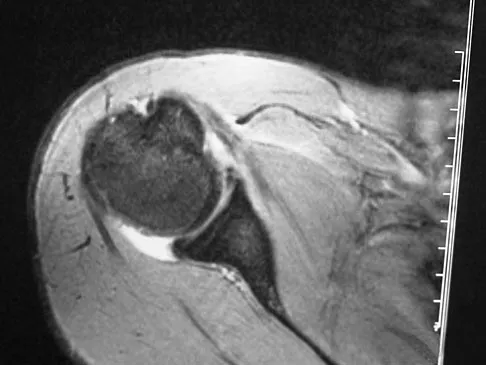
Explanation
An isolated avulsion of the lesser tuberosity occurs very rarely and usually is found in 12- and 13-year-old adolescents. The MRI scans reveal a tear of the humeral attachment of the inferior glenohumeral ligament, a so-called HAGL lesion. This injury to the inferior glenohumeral ligament occurs much less commonly than the classic Bankart lesion (anterior inferior labral tear). A tear of the subscapularis occurs with a similar mechanism of injury but generally occurs in older individuals. Bokor DJ, Conboy VB, Olson C: Anterior instability of the glenohumeral joint with humeral avulsion of the glenohumeral ligament: A review of 41 cases. J Bone Joint Surg Br 1999;81:93-96.
Question 581
High Yield
What pathology is most likely to result in failure of an arthroscopic Bankart repair?
Explanation
Recent studies have documented that an arthroscopic Bankart repair performed with good technique can produce success rates similar to an open repair. However, the results of an arthroscopic repair deteriorate significantly if there is a 25% or greater anterior-inferior glenoid rim defect (inverted pear configuration) or an engaging Hill-Sachs lesion in which the humeral head defect keys onto the glenoid rim in abduction and external rotation. If either of these entities exist or there is multidirectional instability with pathologic hyperextensible tissue laxity, an open repair is recommended. An associated SLAP lesion would not significantly affect the result of the Bankart procedure. Not infrequently, the anterior glenoid labrum is partially or completely disrupted and, in itself, is not a contraindication to arthroscopic Bankart repair. In almost all patients with predominantly unidirectional instability, some degree of capsular/anterior-inferior glenohumeral ligament attenuation is present and can be addressed during the arthroscopic repair. Burkhart SS, De Beer JF: Traumatic glenohumeral bone defects and their relationship to failure of arthroscopic Bankart repairs: Significance of the inverted-pear glenoid and the humeral engaging Hill-Sachs lesion. Arthroscopy 2000;16:677-694.
Question 582
High Yield
A 38-year-old man who is an avid runner reports a several month history of right hip pain. Based on the radiograph and cross-sectional CT scan shown in Figures 33a and 33b, what is the most likely diagnosis for the lesions seen on the femoral neck?


Explanation
Synovial herniation pits or Pitt's pits are tumor simulators and are incidentally identified on radiographs obtained for either pain or trauma. The main diagnostic pitfall with this lesion is mistakenly identifying it as an osteoid osteoma. Accurate diagnosis is achieved by knowledge of the location and the characteristic imaging appearance. These are common lesions in individuals with femoroacetabular impingement. Pitt MJ, Graham AR, Shipman JH, et al: Herniation pit of the femoral neck. Am J Roentgenol 1982;138:1115-1121.
Question 583
High Yield
A 21-year-old woman with scoliosis reports no pain, and her examination is unremarkable except for the scoliosis. Preoperative radiographs, including bending views, are shown in Figures 14a through 14e. The thoracic curve measures 62 degrees. Treatment should consist of





Explanation
The patient has a King type III curve with a very flexible lumbar spine that derotates and levels well on side bending. The fractional upper thoracic curve is also quite flexible and will not need to be addressed; therefore, treatment should consist of posterior spinal fusion from T4 to L1. An anterior spinal fusion at the very apex of the curve will not address the curve satisfactorily, and an approach across the diaphragm provides little benefit in this patient. King HA, Moe JH, Bradford DS, Winter RB: The selection of fusion levels in thoracic idiopathic scoliosis. J Bone Joint Surg Am 1983;65:1302-1313.
Question 584
High Yield
Which of the following increases radiation exposure to patients and personnel during surgery?
Explanation
Continuous fluoroscopy and cine radiography expose the patient and personnel to markedly increased levels of direct and scatter radiation exposure. Continuous fluoroscopy should be limited to only what is absolutely needed for safe completion of the procedure. By orienting the cathode ray tube beneath the patient and placing the image intensifier as close as clinically possible to the patient, scatter radiation exposure to the personnel is minimized.
Question 585
High Yield
An active 72-year-old woman sustained a mid-diaphyseal right humerus fracture 16 months ago. History reveals that she was first treated with a brace for 7 months. Additional treatment consisted of intramedullary nailing 9 months ago. Recently the rod was removed, and the patient now reports pain and gross motion at the fracture site. Current radiographs are shown in Figures 37a and 37b. What is the next most appropriate step in management?


Explanation
The patient has a well-established nonunion in a very porotic bone. Electrical stimulation has been found effective in treating tibial nonunions, but there is very little data on humeral nonunions, especially chronic well-established ones. Ultrasound stimulation is effective in accelerating fracture healing, but there is little data concerning the treatment of nonunions. Intramedullary nailing with bone graft is an option, but it maybe difficult to obtain a rigid construct in a very porotic bone. An Ilizarov-type external fixator would be an alternative, but there is little clinical data for the humerus and it may be poorly tolerated. A plate and screw construct with bone graft combines rigidity with the biologic advantage of the bone graft. A recent series reported on the use of a plate combined with onlay allograft for recalitrant nonunions. Cement augmentation for screw fixation either in the canal or added to the screw holes may be helpful in select cases. Hornicek FJ, Zych GA, Hutson JJ, Malinin TI: Salvage of humeral nonunions with onlay bone plate allograft augmentation. Clin Orthop 2001;386:203-209.
Question 586
High Yield
A 16-year-old boy has had thigh pain for the past several months. He denies any history of trauma. Examination reveals a large, deeply fixed, soft-tissue mass in the thigh. Laboratory results show an elevated erythrocyte sedimentation rate (ESR) and leukocytosis. A plain radiograph and MRI scan are shown in Figures 1a and 1b. Biopsy specimens are shown in Figures 1c and 1d. What is the most likely diagnosis?


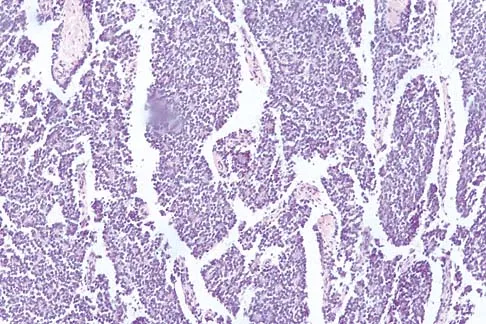
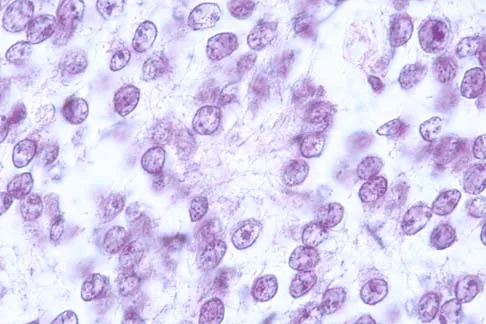
Explanation
Ewing's sarcoma typically can occur in the diaphysis of the long bones (50% to 55%). It is often accompanied by a large soft-tissue mass. Abnormal findings are common, including a low-grade fever, an elevated ESR, and leukocytosis. The histology is consistent with a small round blue cell tumor. The unique pathology and other findings exclude osteosarcoma. Giant cell tumor and chondrosarcoma have a different histologic appearance and typically are more metaphyseal in location. Chondrosarcoma typically is found in older age groups, has a different histologic pattern, and rarely occurs in the midshaft of the femur.
Question 587
High Yield
Figures 39a and 39b show the MRI scans of a 25-year-old man with right shoulder pain. Figure 39c shows the arthroscopic view from a posterior portal in the beach chair position. What is the most likely diagnosis?
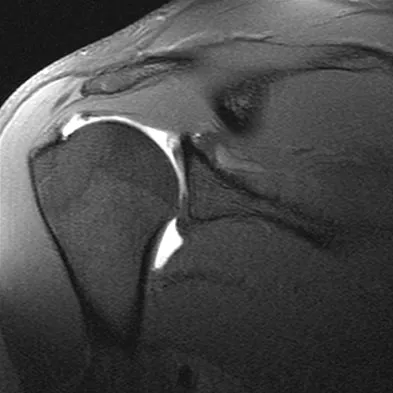
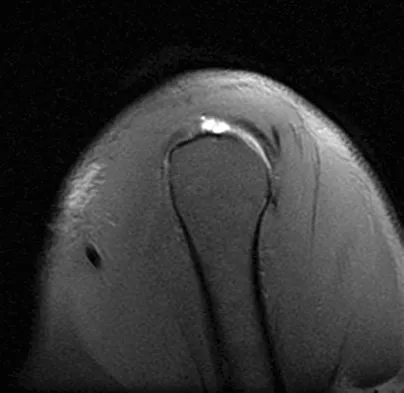

Explanation
The MRI scans show coronal oblique and sagittal oblique views of a partial articular surface supraspinatus tear or tendon avulsion (PASTA lesion). The arthroscopic view is a posterior portal of the glenohumeral joint viewing the articular surface of the supraspinatus. These tears are a common source of shoulder pain and are often amenable to transtendon arthroscopic repair without detachment of the intact bursal surface. Sanders TG, Miller MD: A systematic approach to magnetic resonance imaging interpretation of sports medicine injuries of the shoulder. Am J Sports Med 2005;33:1088-1105. McConville OR, Iannotti JP: Partial-thickness tears of the rotator cuff: Evaluation and management. J Am Acad Orthop Surg 1999;7:32-43.
Question 588
High Yield
An 8-year-old boy reports progressive difficulty with walking. Examination reveals muscle weakness, with proximal groups more affected than distal muscles. Deep tendon reflexes are within normal limits. Laboratory studies show a creatine kinase level of 7,200 IU. Based on these findings, what is the most likely diagnosis?

Explanation
Patients with Becker muscular dystrophy have an abnormality in dystrophin, but unlike patients with Duchenne muscular dystrophy, some dystrophin is present. As a result, the progression of muscle weakness is slower, with the diagnosis typically made after age 8 years. Similar to patients with Duchenne muscular dystrophy, patients with Becker muscular dystrophy have pseudohypertrophy of the calves, markedly increased creatine kinase levels, and X-linked transmission of the condition. In addition, these patients are more prone to cardiomyopathy; a condition that should be carefully evaluated if any surgery is required. Patients with spinal muscular atrophy also have proximal muscle weakness, but the onset of weakness occurs earlier in childhood. These patients also have absent deep tendon reflexes and fasciculations, but pseudohypertrophy is absent and creatine kinase levels are normal. Patients with Emery-Dreifuss dystrophy may have a similar clinical picture to Becker's muscular dystrophy, but pseudohypertrophy is absent and creatine kinase levels are only mildly elevated. In addition, neck extension, elbow flexion, and ankle equinus contractures develop at an early age. Limb girdle dystrophy is a group of progressive muscular dystrophies that is not associated with pseudohypertrophy or a significant elevation of creatine kinase levels. Guillain-Barre syndrome is a condition associated with results from postinfectious demyelination of the peripheral nerve. These patients have the acute onset of weakness, hypotonia, and areflexia; creatine kinase levels are normal. Sussman MD: Muscular dystrophy, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 1573-1583.
Question 589
High Yield
Figures 21a through 21c show the MRI scans of a 21-year-old football player who sustained a valgus knee injury while changing direction. Examination reveals swelling and tenderness along the medial aspect of the knee. There is a positive Lachman test, 3+ valgus laxity at 30 degrees, and 1+ valgus laxity at 0 degrees extension. The anterior drawer test is increased with the tibia in external rotation. The increase in the anterior drawer test with the tibia in external rotation is most likely the result of


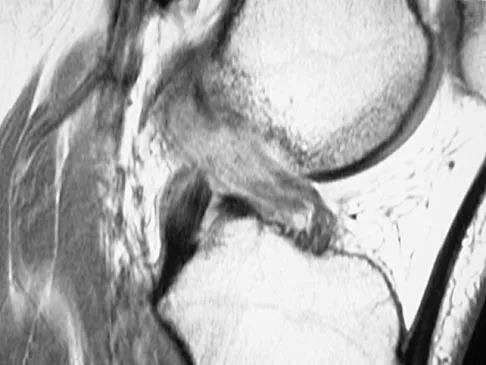
Explanation
The injury mechanism involves a valgus load applied to the knee with the foot in external rotation. The primary stabilizer to valgus laxity is the medial collateral ligament. The secondary restraints to valgus rotation are the cruciate ligaments. Examination indicates disruption of the medial collateral and anterior cruciate ligaments. Valgus opening in extension should also arouse suspicion for an injury to the posterior cruciate ligament; however, in this patient, the valgus opening in extension is mild. The slight opening in extension and the increased anterior drawer, especially with external rotation, indicates disruption of the posteromedial capsule and posterior oblique ligament. Figure 21a shows complete disruption of the superficial and deep medial collateral ligaments involving the meniscofemoral ligament. Figure 21b shows a more posterior coronal section with a torn posterior oblique ligament. Figure 21c shows disruption of the anterior cruciate ligament, while the posterior cruciate ligament at the tibial insertion appears with a homogenous normal signal. Warren LA, Marshall JL, Girgis F: The prime static stabilizer of the medial side of the knee. J Bone Joint Surg Am 1974;56:665-674.
Question 590
High Yield
A 42-year-old man reports a 12-month history of a painful fusiform swelling of the Achilles tendon. Physical therapy, heel lifts, and anti-inflammatory drugs have failed to provide relief. MRI scans are shown in Figures 44a and 44b. What is the treatment of choice?
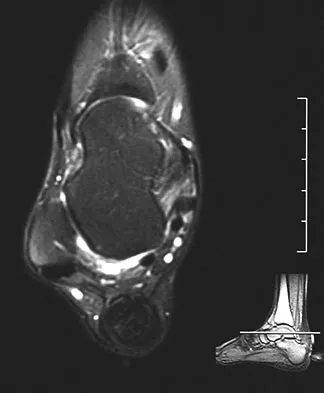

Explanation
The area of the tendon degeneration is greater than 50% of the width so a supplemental tendon transfer is needed. Debridement and repair alone do not provide adequate strength. Injection risks tendon rupture. Brisement is indicated for peritendinitis, not tendinosis. Nonsurgical management is unlikely to be of benefit after 12 months. Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 94-95.
Question 591
High Yield
A 20-year-old professional baseball pitcher has had a 3-year history of increased aching in his shoulder that is associated with pitching, and he is now seeking a second opinion. Nonsurgical management consisting of rest, anti-inflammatory drugs, ice, heat, and cortisone injections has failed to provide relief. A previous work-up that included radiographs and gadolinium-enhanced MRI arthrography was negative. Results of an arteriogram suggest quadrilateral space syndrome. Assuming that this is the correct diagnosis, what nerve needs to be decompressed?

Explanation
Quadrilateral space syndrome is a rare condition and is the result of compression of the contents of the quadrilateral space. The contents of the quadrilateral space include the posterior circumflex vessels and the axillary nerve. Cahill BR, Palmer RE: Quadrilateral space syndrome. J Hand Surg 1983;8:65-69.
Question 592
High Yield
A 4-month-old infant is referred for evaluation of congenital scoliosis. The child has no congenital heart anomalies, and a renal ultrasound shows that he has one kidney. Examination reveals mild scoliosis and a large hairy patch on the child's back. Neurologic evaluation is normal for his age. A clinical photograph and radiograph are shown in Figures 19a and 19b. Initial management should consist of

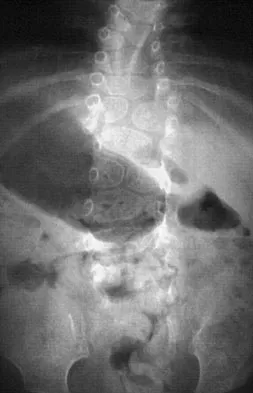
Explanation
Congenital anomalies of the spine, including failure of formation and failure of segmentation, are associated with other anomalies in other organ systems that develop at the same time. These include anomalies in the genitourinary system, cardiac anomalies, Sprengel's deformity, radial hypoplasia, and gastrointestinal anomalies including imperforate anus and trachealesophageal fistula. Spinal dysraphism is the most common associated abnormality. McMaster found an 18% incidence before the common use of MRI. Bradford and associates reported on 16 of 42 patients with congenital spinal anomalies and spinal dysraphism using MRI. Neural axis lesions may be associated with visible midline abnormalities such as a hairy patch or nevus. The child has already had a cardiac and renal work-up, and based on the findings of the hairy patch and congenital vertebral anomalies, MRI of the entire spine is prudent at this time. Spinal fusion is indicated for progressive congenital scoliosis or kyphosis. Physical therapy does not affect the natural history of congenital scoliosis. McMaster MJ: Occult intraspinal anomalies and congenital scoliosis. J Bone Joint Surg Am 1984;66:588-601. Bradford DS, Heithoff KB, Cohen M: Intraspinal abnormalities and congenital spine deformities: A radiographic and MRI study. J Pediatr Orthop 1991;11:36-41.
Question 593
High Yield
A 36-year-old professional baseball player reports the acute onset of severe right groin pain while attempting to avoid being hit by a baseball while at bat. Examination reveals tenderness, soft-tissue swelling, and ecchymosis in the right groin extending over the medial thigh. MRI scans are shown in Figures 8a and 8b. Management should consist of

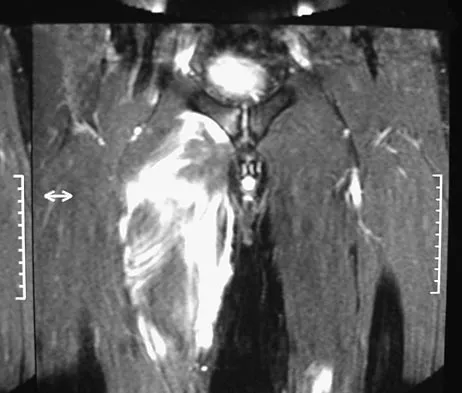
Explanation
The MRI scans reveal a severe avulsion injury of the adductor muscle from the pubic ramus with muscle edema and hemorrhage. Injury to the adductor muscle group, a "pulled groin," is caused by forceful external rotation of an abducted leg. Pain is immediate and severe in the groin region. Tenderness is at the site of injury along the subcutaneous border of the pubic ramus. Treatment is dictated by the severity of the symptoms but generally consists of rest, ice, and protected weight bearing, followed by a rehabilitation program that begins with gentle stretching and progresses to resistance exercise with a gradual return to sports. Immobilization should be avoided because this promotes muscle tightness and scarring. No data exist to suggest that open repair yields a better outcome than nonsurgical management. Tenotomy has been performed in high-level athletes with chronic groin pain following injury. Gilmore J: Groin pain in the soccer athlete: Fact, fiction, and treatment. Clin Sports Med 1998;17:787-793.
Question 594
High Yield
A characteristic genetic translocation has been noted in which of the following tumors?

Explanation
There have been no characteristic gene translocations or rearrangements noted in osteosarcoma, chondrosarcoma, neurofibrosarcoma, or epithelioid sarcoma. In contrast, Ewing's sarcoma has been noted to have a consistent genetic translocation t(11:22). Brockstein BE, Peabody TD, Simon MA: Soft tissue sarcomas, in Vokes EE Golomb HM (eds): Oncologic Therapies. New York, NY, Springer-Verlag, 1999, pp 925-952.
Question 595
High Yield
Figure 30 shows the radiograph of a 38-year-old man who reports persistent pain laterally and plantarly about the fifth metatarsal head. Examination reveals calluses dorsolaterally and plantarly about the fifth metatarsal head. Nonsurgical management has failed to provide relief. Surgical treatment should include

Explanation
The patient has painful lateral and plantar keratoses with metatarsus quintus valgus deformity. This combination of problems is best addressed with an oblique mid-diaphyseal osteotomy that allows the distal metatarsal to be displaced medially and dorsally. Lateral eminence resection alone will not address the painful plantar keratosis. A distal chevron osteotomy has a more limited ability to address the plantar keratosis (if translated medially and slight dorsally). Proximal diaphyseal osteotomies of the fifth metatarsal are associated with an increased risk of delayed union or nonunion secondary to the relative hypovascularity in the proximal diaphysis. Excision of the fifth metatarsal head can result in a floppy fifth toe and transfer metatarsalgia. Coughlin MJ: Treatment of bunionette deformity with longitudinal diaphyseal osteotomy with distal soft tissue repair. Foot Ankle 1991;11:195-203.
Question 596
High Yield
A 20-year-old man involved in a motor vehicle accident is brought to the emergency department with a C6-7 unilateral facet dislocation. His neurologic examination reveals a focal left-sided C7 nerve root palsy. He is awake and cooperative with questioning and has no other obvious traumatic injuries. What is the most appropriate treatment at this time?
Explanation
In the patient who is neurologically intact or has an incomplete injury from a cervical facet dislocation, a closed reduction with weighted tong traction is appropriate when the patient is awake, alert, and cooperative. Although there is a risk that a cervical facet dislocation could occur with an underlying cervical disk herniation, Vaccaro and associates have shown that closed reduction can be safely carried out in the awake, responsive patient. Closed reduction can be performed in the emergency department with traction with skull tongs or a halo ring. A slow stepwise application of weight is added until a reduction is achieved. Any worsening of the neurologic status of the patient requires immediate termination of the closed reduction and further diagnostic imaging before proceeding with further treatment. Vaccaro AR, Falatyn SP, Flanders AE, et al: Magnetic resonance evaluation of the intervertebral disc, spinal ligaments, and spinal cord before and after closed traction reduction of cervical spine dislocations. Spine 1999;24:1210-1217. Hart RA: Cervical facet dislocation: When is magnetic resonance imaging indicated? Spine 2002;27:116-117.
Question 597
High Yield
Figures 19a through 19c show radiographs of the cervical spine of an asymptomatic patient with Down syndrome who wants to participate in a Special Olympics running event. The neurologic examination is normal. Management should consist of



Explanation
An atlanto-dens interval (ADI) of up to 4 mm in children is considered normal. Children with Down syndrome have increased ligamentous laxity, with atlantoaxial instability occurring in as many as 15% to 20% of patients. These patients are at risk for catastrophic injury following minor trauma and should be routinely screened for instability, generally beginning when the patient starts to walk. Patients with an ADI of greater than 5 mm should avoid contact sports and high-risk activities such as gymnastics, diving, the high jump, and the butterfly stroke. The American Academy of Pediatrics Committee of Sports Medicine and Fitness guidelines recommend that lateral views of the cervical spine in neutral, flexion, and extension should be obtained in all children with Down syndrome who wish to participate in sports. Patients with normal radiographs and examinations do not need repeat radiographs, although some authors suggest that instability increases with age, and therefore recommend repeat radiographs every 5 years. Cervical spine fusion in patients with Down syndrome has a high rate of complications and should be performed only on patients with symptoms and evidence of myelopathy. American Academy of Pediatrics Committee of Sports Medicine and Fitness: Atlantoaxial instability in Down syndrome. Pediatrics 1995;96:151-154. Copley LA, Dormans JP: Cervical spine disorders in infants and children. J Am Acad Orthop Surg 1998;6:204-214.
Question 598
High Yield
A 22-year-old swimmer underwent thermal capsulorrhaphy treatment for recurrent anterior subluxation. Following 3 weeks in a sling, an accelerated rehabilitation program allowed him to return to swimming in 3 1/2 months. While practicing the butterfly stroke, he sustained an anterior dislocation. He now continues to have symptoms of anterior instability and has elected to have further surgery. Surgical findings may include a

Explanation
Complications of thermal capsule shrinkage or accelerated rehabilitation include capsule ablation. Since the original surgery did not include labral reattachment, findings of a Bankart lesion or a glenoid fracture from a nontraumatic injury are unlikely. Subscapularis detachment or biceps subluxation is a postoperative complication of open repairs. Failure of early postoperative instability treatment should not produce loose bodies. Abrams JS: Thermal capsulorrhaphy for instability of the shoulder: Concerns and applications of the heat probe. Instr Course Lect 2001;50:29-36.
Question 599
High Yield
Figure 33 shows the radiograph of a 28-year-old avid golfer who has chronic right wrist pain. Management should consist of
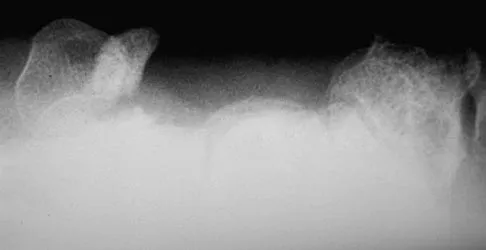
Explanation
The patient's chronic symptoms are associated with a fracture of the base of the hook of the hamate; therefore, the treatment of choice is simple excision of the fracture fragment, with reasonable expectations of functional return. Acute fractures may be difficult to treat because of the high incidence of nonunion, but once nonunion is discovered, nonsurgical management usually is unsuccessful. Bone grafting may be a surgical alternative, but successful outcomes with percutaneous fixation or trephination of the fibrous union have not been reported. Geissler WB: Carpal fractures in athletes. Clin Sports Med 2001;20:167-188.
Question 600
High Yield
A 52-year-old man has had right shoulder pain in the deltoid region that increases at night for the past 2 months. He denies any history of trauma. Examination reveals mild tenderness over the greater tuberosity, and the Neer and Hawkins impingement signs are positive. AP and outlet lateral radiographs are shown in Figures 24a and 24b. Initial management should consist of


Explanation
The patient has the findings of classic subacromial impingement. Initial management should consist of stretching exercises directed at the posterior capsule and a program of rotator cuff and deltoid strengthening exercises performed below the horizontal in a "safe" plane. The judicious use of subacromial cortisone injections (one or two) may be helpful. Anterior acromioplasty is reserved for patients who have failed to respond to nonsurgical management. Morrison DS, Frogameni AD, Woodworth P: Non-operative treatment of subacromial impingement syndrome. J Bone Joint Surg Am 1997;79:732-737. Neer CS: Impingement lesions. Clin Orthop 1983;173:70-77.
