HY 2026
00:00
Start Quiz
Question 401
High Yield
Lumbar instability may be surgically induced by
Explanation
In cadaveric studies, unilateral facetectomy, or excision of 50% or more of both facets, significantly decreases the biomechanic integrity of the motion segment and may increase the risk of iatrogenic instability. Sacrifice of the spinous process, interspinous ligaments, and ligamentum flavum weakens the motion segment but does not increase the risk for instability. Facetectomy, even unilateral, predisposes the patient toward lumbar instability.
Question 402
High Yield
A 6-year-old boy with acute hematogenous osteomyelitis of the distal femur is being treated with intravenous antibiotics. The most expeditious method to determine the early success or failure of treatment is by serial evaluations of which of the following studies?

Explanation
Successful antibiotic treatment of osteomyelitis should lead to a rapid decline in the CRP. The CRP should decline after 48 to 72 hours of appropriate treatment. Imaging studies will take much longer to show resolution of bone infection. Unkila-Kallio L, Kallio MJ, Eskola J, et al: Serum C-reactive protein, erythrocyte sedimentation rate, and white blood cell count in acute hematogenous osteomyelitis of children. Pediatrics 1994;93:59-62.
Question 403
High Yield
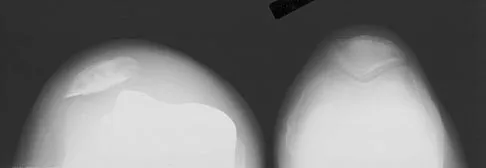
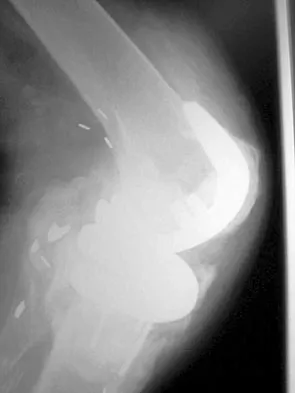
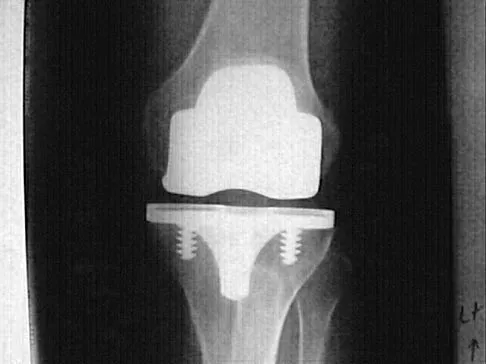
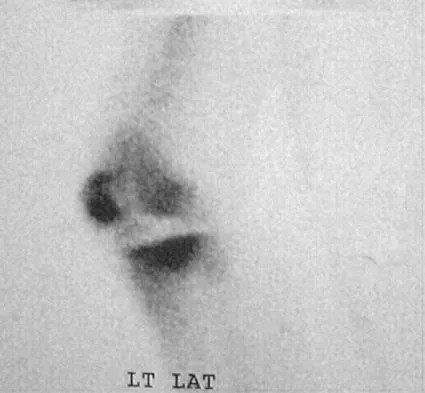
An 82-year-old woman reports activity-related knee pain. History reveals that she underwent total knee arthroplasty 16 years ago. AP and lateral radiographs and a bone scan are shown in Figures 38a through 38c. What is the most likely diagnosis?



Explanation
The radiographs reveal a large femoral metaphyseal lytic lesion with well-defined borders. Joint space narrowing medially is consistent with polyethylene wear. The most likely diagnosis is particle-mediated osteolysis. Metastatic tumors and primary sarcomas adjacent to an arthroplasty are extremely rare. In addition, malignant tumors and infection would more likely reveal a destructive lesion with poorly defined borders and increased uptake on a bone scan. Stress shielding with massive bone loss has not been described in knee arthroplasty literature, although this entity has been observed in fully porous-coated femoral implants in total hip arthroplasty. Robinson EJ, Mulliken BD, Bourne RB, et al: Catastrophic osteolysis in total knee replacement: A report of 17 cases. Clin Orthop Relat Res 1995;321:98-105. Archibeck MJ, Jacobs JJ, Roebuck KA, et al: The basic science of periprosthetic osteolysis. Instr Course Lect 2001;50:185-195.
Question 404
High Yield
A 45-year-old man undergoes an anterior cervical diskectomy and fusion at C5-6 and C6-7 with instrumentation. During the first postoperative visit at 1 week, the patient reports difficulty swallowing and mild anterior cervical tightness. The anterior wound is benign and the patient denies any dyspnea or shortness of breath. A postoperative radiograph is seen in Figure 25. What is the most appropriate management at this time?

Explanation
The radiograph shows significant prevertebral soft-tissue swelling following a two-level anterior cervical diskectomy and fusion. The incidence of dysphagia 2 years after anterior cervical spine surgery is 13.6%. Risk factors for long-term dysphagia after anterior cervical spine surgery include gender, revision surgeries, and multilevel surgeries. The use of instrumentation, higher levels, or corpectomy versus diskectomy did not significantly increase the prevalence of dysphagia. Lee and associates demonstrated that while dysphagia after anterior cervical spine surgery is a common early finding, it generally decreases significantly by 6 months with nonsurgical management. A minority of patients experience moderate or severe symptoms by 6 months after the procedure. Female gender and multiple surgical levels have been identified as risk factors for the development of postoperative dysphagia. Lee MJ, Bazaz R, Furey CG, et al: Risk factors for dysphagia after anterior cervical spine surgery: A two-year prospective cohort study. Spine J 2007;7:141-147.
Question 405
High Yield
Figures 5a and 5b show the radiograph and MRI scan of a patient who has severe mechanical neck pain but no neurologic problems. Biopsy and work-up show the lesion to be a solitary plasmacytoma. Treatment should consist of


Explanation
Plasmacytoma is very sensitive to radiation therapy and given the complexity of the resection and complications of surgery in the given location, radiation therapy is preferred. However, the patient has clear loss of bony structural integrity, and resultant instability would persist even with tumor irradiation; therefore, posterior stabilization is warranted. Chemotherapy and bone marrow transplant are reserved for systemic disease with multiple myeloma. Corwin J, Lindberg RD: Solitary plasmacytoma of bone vs. extramedullary plasmacytoma and their relationship to multiple myeloma. Cancer 1979;43:1007-1013.
Question 406
High Yield
Which of the following findings is a prerequisite for a high tibial valgus osteotomy for medial compartment gonarthrosis?

Explanation
The indications for high tibial valgus osteotomy include a physiologically young age, arthritis confined to the medial compartment, 10 to 15 degrees of varus alignment on weight-bearing radiographs, a preoperative arc of motion of at least 90 degrees, flexion contracture of less than 15 degrees, and a motivated, compliant patient. Contraindications include lateral compartment narrowing of the articular cartilage, lateral tibial subluxation of greater than 1 cm, medial compartment bone loss, ligamentous instability, and inflammatory arthritis. Naudie D, Bourne RB, Rorabeck CH, Bourne TT: The Insall Award: Survivorship of the high tibial valgus osteotomy. A 10- to 22-year followup study. Clin Orthop 1999;367:18-27.
Question 407
High Yield
A professional pitcher reports pain localized to the medial aspect of his throwing elbow. History reveals that he was pitching in a playoff game and heard and felt a pop in his elbow. MRI reveals a complete ulnar-sided avulsion of the medial collateral ligament (MCL). Examination reveals valgus instability and ulnar nerve involvement. What recommendations should be made based on the patient's desire to return to sport?
Explanation
Injuries to the MCL usually result from repetitive high valgus stress on the medial aspect of the elbow joint due to overhead throwing or racquet sports. Excessive stresses during the late cocking and acceleration phase of throwing can injure the anterior band of the MCL. Clinically, the injuries may present as chronic or acute, and a pop may be noted in the latter. Associated ulnar nerve involvement is common. Valgus instability is present in about 25% of patients. Patients typically are athletes who participate in throwing and have localized medial elbow pain and tenderness along the course of a ligament that extends from the medial epicondyle of the distal humerus to the sublime tubercle of the ulna. Surgical reconstruction is the procedure of choice in an athlete desiring a return to a high level of throwing. Miller MD, Cooper DE, Warner JJP (eds): Review of Sports Medicine and Arthroscopy. Philadelphia, PA, WB Saunders, 1995, p 230. Arendt EA (ed): Orthopaedic Knowledge Update: Sports Medicine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, p 227.
Question 408
High Yield
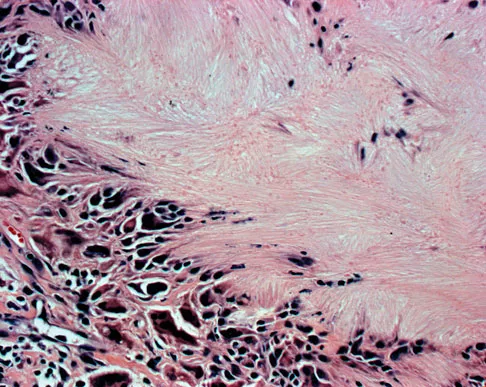
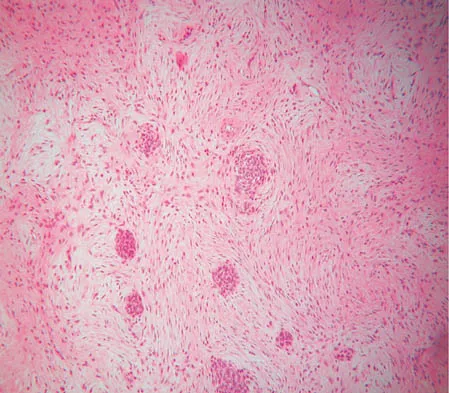
A 73-year-old man stepped off a street curb and felt a crack in his left hip. He is now unable to bear weight. A radiograph is shown in Figure 54a. Biopsy specimens are shown in Figures 54b and 54c. What is the most likely diagnosis?

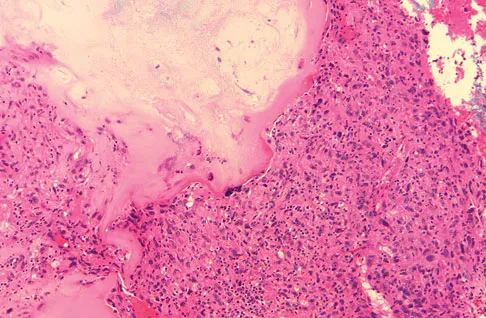
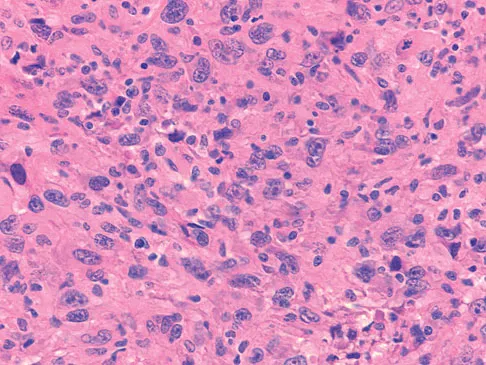
Explanation
The biopsy specimens reveal a high-grade spindle cell lesion adjacent to an area of benign cartilage. This is consistent with a dedifferentiated chondrosarcoma. The radiograph shows a pathologic fracture through a lesion characterized by calcification within the left greater trochanter. Distal to the area of calcification, there is a more osteolytic, destructive appearance. Synovial sarcoma has a biphasic appearance histologically with areas of glandular differentiation that stain positive with keratin. Metastatic prostate cancer, although osteoblastic in appearance, would have a glandular histologic appearance. There is no cartilage in these lesions. Classic low-grade chondrosarcoma does not have an area of high-grade pleomorphic spindle cells within the lesion. A periosteal osteosarcoma is a surface-based lesion with a sunburst radiographic pattern. Although there may be cartilage in the lesion histologically, there are also malignant cells producing osteoid. Dedifferentiated chondrosarcoma is an aggressive, high-grade variant of chondrosarcoma. Wold LE, Adler CP, Sim FH, et al: Atlas of Orthopedic Pathology, ed 2. Philadelphia, PA, WB Saunders, 2003, p 269.
Question 409
High Yield
A 64-year-old man undergoes a primary total knee arthroplasty. Three months after surgery he reports persistent pain, weakness, and difficulty ambulating. Postoperative radiographs are shown in Figures 6a through 6c. What is the best course of action at this time?


Explanation
The Merchant view reveals subluxation of the patellar component. The etiology of maltracking of the patella includes internal rotation of the femoral component, internal rotation of the tibial component, excessive patellar height, and lateralization of the patella component. The treatment of choice in this patient is revision total knee arthroplasty with external rotation of the femoral component. Preoperatively the patient also may require a lateral release, revision of the tibial component if it is internally rotated, and possibly a soft-tissue realignment. Component malalignment needs to be addressed first. Kelly MA: Extensor mechanism complications in total knee arthroplasty. Instr Course Lect 2004;53:193-199. Malkani AL, Karandikar N: Complications following total knee arthroplasty. Sem Arthroplasty 2003;14:203-214.
Question 410
High Yield
What is the most common diagnosis in a patient older than age 40 years with a destructive bony lesion?
Explanation
The most common destructive lesions in a patient older than age 40 years are, in decreasing incidence, metastatic carcinoma, multiple myeloma, lymphoma, and chondrosarcoma. Osteosarcoma is found primarily in younger patients.
Question 411
High Yield
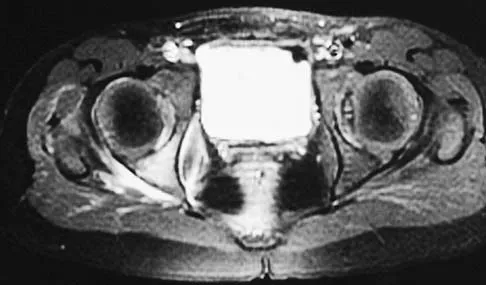
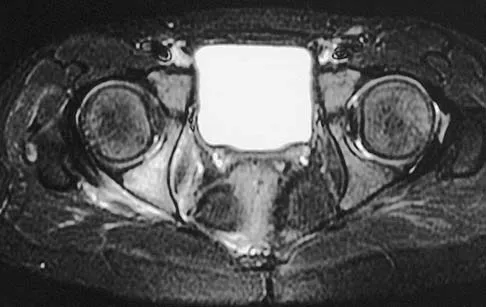
A 5-year-old girl has had a low-grade fever, right hip and buttock pain, and a right-sided limp for the past 5 days. Examination shows diffuse tenderness and extreme pain on range of motion of the hip. Laboratory studies show a peripheral WBC count of 13,500/mm3 and an erythrocyte sedimentation rate of 55 mm/h. A radiograph is shown in Figure 46a, and an axial postgadolinium T1-weighted MRI scan with fat suppression and an axial T2-weighted fast spin echo MRI scan are shown in Figures 46b and 46c. What is the most likely diagnosis?

Explanation
MRI findings of acute osteomyelitis include a decrease in the normally high signal intensity of bone marrow on T1-weighted imaging; however, a postgadolinium T1-weighted image with fat suppression will show osteomyelitis as a bright marrow signal compared to the surrounding fat. Osteomyelitis is also brighter than normal fat on T2-weighted imaging. There is no rim-enhancing lesion suggesting an abscess, although myositis is seen in the obturator internus and short external rotators. The clinical scenario and imaging studies do not support the diagnosis of septic hip, eosinophilic granuloma, or pelvic fracture. Dormans JP, Drummond DS: Pediatric hematogenous osteomyelitis: New trends in presentation, diagnosis and treatment. J Am Acad Orthop Surg 1994;2:333-341.
Question 412
High Yield
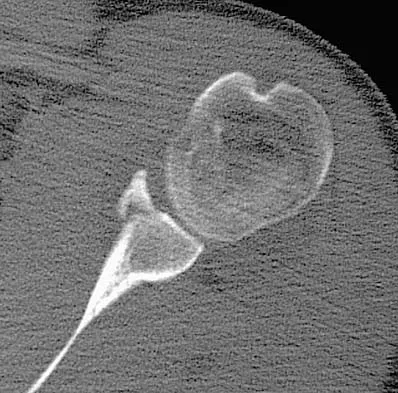
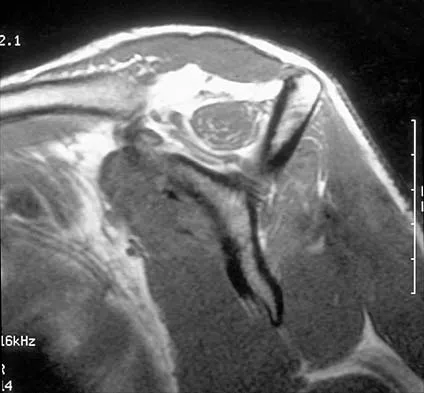
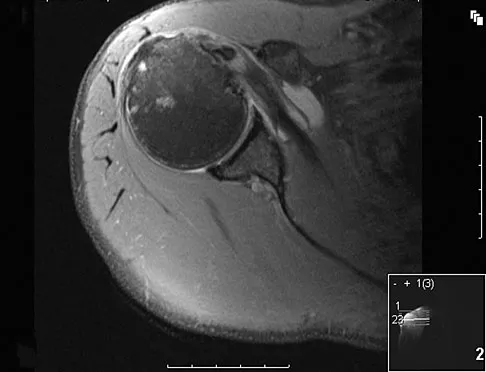
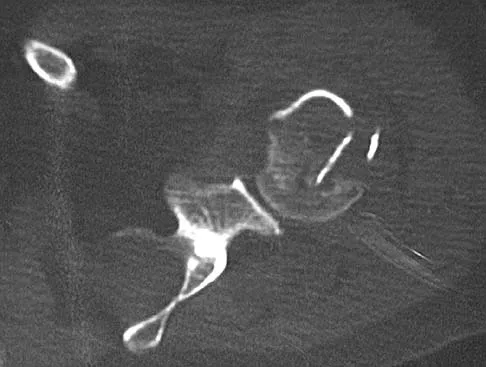
Figure 33 shows the CT scan of a 40-year-old man who injured his left shoulder while skiing. What structure is attached to the bony fragment?
Explanation
The scan reveals a bony Bankart lesion. The anterior band of the inferior glenohumeral ligament is the major restraint to anterior translation of the humeral head and is usually injured with anterior shoulder dislocations. It inserts onto the glenoid labrum at the anteroinferior aspect of the glenoid rim. The labrum most frequently avulses from the glenoid (Bankart lesion), but occasionally the bony attachment is avulsed. O'Brien SJ, Neves MC, Arnoczky SP, et al: The anatomy and histology of the inferior glenohumeral ligament complex of the shoulder. Am J Sports Med 1990;18:449-456.
Question 413
High Yield
Figure 10 shows the MRI scan of a 56-year-old woman with metastatic breast cancer who now reports progressive paraparesis. Her general health remains good. Treatment should consist of

Explanation
If the patient's medical condition and prognosis remain good in the presence of significant and progressive neurologic deficit from cord compression, then the most reliable means of restoring function is via surgical decompression and fusion. Decompression should be directed toward the compressing structure (eg, anteriorly if the compression is from the anterior side). This procedure can be done via a posterolateral technique, such as costotransversectomy in some cases.
Question 414
High Yield
A 29-year-old quarterback falls onto his dominant shoulder and sustains the injury shown in Figures 14a and 14b. Management should consist of


Explanation
Type V acromioclavicular dislocations are characterized by elevation of the clavicle of 100% to 300% and involve extensive soft-tissue stripping. The treatment of choice is surgical reduction of the acromioclavicular joint and some type of stabilization. Treatment of type III injuries is controversial. Lemos MJ: The evaluation and treatment of the injured acromioclavicular joint in athletes. Am J Sports Med 1998;26:137-144.
Question 415
High Yield
A 45-year-old man is seeking evaluation of an injury sustained in a motor vehicle accident 10 weeks ago. Current radiographs are shown in Figures 2a and 2b. Based on the radiographic findings, what is the most likely diagnosis?


Explanation
An increased density of the talar body compared to the distal tibia following fracture of the talar neck is highly suggestive of vascular compromise of the talar body. Subchondral osteopenia of the talus at 6 to 8 weeks (Hawkins sign) is a favorable sign but does not eliminate the possibility of osteonecrosis. Elgafy H, Ebraheim NA, Tile M, Stephen D, Kase J: Fractures of the talus: Experience of two level 1 trauma centers. Foot Ankle Int 2000;21:1023-1029.
Question 416
High Yield
An 83-year-old woman reports pain in her left middle finger after a minor injury. Laboratory studies show a WBC count of 7,000/mm3, an erythrocyte sedimentation rate of 3 mm/h, a uric acid of 10.4 mg/dL, and a normal serum protein electrophoresis. Radiographs are shown in Figures 49a and 49b. A core biopsy specimen is shown is Figure 49c. In addition to treatment of the finger fracture, treatment should include


Explanation
This clinical picture is most consistent with periarticular erosions from gout. The patient has multiple periarticular lytic lesions in the hand. The laboratory studies show an elevated serum uric acid level, and the biopsy specimen demonstrates acute and chronic inflammation with prominent clefts. Therefore, the preferred treatment is systemic control of her gout. Radiation therapy, chemotherapy, and/or amputation should be considered for a malignancy; however, the pathology does not demonstrate any evidence of pleomorphism, high nuclear-to-cytoplasmic ratio, nuclear atypia, or mitotic activity. Antibiotics for an infectious process is a consideration, but the minimal elevation in the WBC count and erythrocyte sedimentation rate does not support an infectious process. Wise CM: Crystal-associated arthritis in the elderly. Clin Geriatr Med 2005;21:491-511.
Question 417
High Yield
A 19-year-old man sustained the isolated injury seen in Figure 28a. He is adequately resuscitated. A closed reduction was performed in the emergency department, and postreduction radiographs are shown in Figures 28b and 28c. What is the next most appropriate step in management?



Explanation
Incarcerated fragments and nonconcentric reductions are best treated with urgent open reduction, retrieval of the fragments, and internal fixation. Delayed treatment increases the damage to the articular surface, even if traction is applied. There is no role for nonsurgical management with entrapped fragments and nonconcentric reduction of the hip. Epstein HC, Wiss DA, Cozen L: Posterior fracture dislocation of the hip with fractures of the femoral head. Clin Orthop Relat Res 1985;201:9-17.
Question 418
High Yield
A 15-year-old athlete collapses suddenly during practice and dies. What is the most likely cause of death?

Explanation
The number one cause of sudden death in the young athlete is myocardial pathology, with hypertrophic cardiomyopathy being most common. Because of cardiac muscle hypertrophy, the ventricular capacity is diminished and can result in decreased cardiac output. During exertional activities, the increased demand may not be able to be met and leads to sudden death. While the other choices can be the cause of sudden death in an otherwise healthy young athlete, their incidence is even more rare. Van Camp SP, Bloor CM, Mueller FO, et al: Nontraumatic sports death in high school and college athletes. Med Sci Sports Exerc 1995;27:641-647. Maron BJ, Shirani J, Pollac LC, et al: Sudden death in young competitive athletes: Clinical, demographic, and pathological profiles. JAMA 1996;276:199-204.
Question 419
High Yield
When the elbow is extended and an axial load is applied, what percent of stress distribution occurs across the ulnohumeral and radiohumeral articular surface, respectively?

Explanation
When load is applied to the wrist, most of the stress is absorbed by the radius. As the load is transferred through the forearm, the interosseous membrane transfers some of the load from the radius to the ulna. The load at the elbow is distributed with 40% at the ulnohumeral articulation and 60% at the radiohumeral articulation. Halls AA, Travill R: Transmission of pressure across the elbow joint. Anat Rec 1964;150:243.
Question 420
High Yield
A 16-year-old girl has had anterior leg pain and a mass for the past 8 months. Figures 2a and 2b show a radiograph and an H & E histologic specimen. Which of the following disorders is believed to be a precursor of this lesion?

Explanation
The radiograph and pathology are consistent with adamantinoma. While the mechanism underlying adamantinoma has not been identified, it is believed to be closely related to osteofibrous dysplasia, which may represent a precursor. The other diagnoses are not known to give rise to adamantinoma.
Question 421
High Yield
A 17-year-old girl has multidirectional instability of the shoulder. What is the most appropriate initial management?
Explanation
Multidirectional instability of the shoulder is defined as symptomatic instability in two or more directions (anterior, posterior) but must include a component of inferior instability. Initial treatment should always include physical therapy and instruction in a home exercise program that emphasizes periscapular and rotator cuff strengthening to improve the dynamic stability of the glenohumeral joint. Immobilization has not been shown to be effective. Open capsular shift and arthroscopic capsular plication remain the surgical options when appropriate nonsurgical management fails (typically a minimum of 6 months of dedicated therapy and home program). Thermal capsulorrhaphy remains controversial but is not recommended by many clinicians because of reported complications including recurrent instability, axillary nerve injury, chondrolysis, and capsular injury. Neer CS II, Foster CR: Inferior capsular shift for involuntary inferior and multidirectional instability of the shoulder: A preliminary report. J Bone Joint Surg Am 1980;62:897-908. D'Alessandro DF, Bradley JP, Fleischli JE, et al: Prospective evaluation of thermal capsulorrhaphy for shoulder instability: Indications and results, two- to five-year follow-up. Am J Sports Med 2004;32:21-33. Levine WN, Clark AM Jr, D'Alessandro DF, et al: Chondrolysis following arthroscopic thermal capsulorrhaphy to treat shoulder instability: A report of two cases. J Bone Joint Surg Am 2005;87:616-621.
Question 422
High Yield
As reflected by the SF-36 scores, patients with which of the following conditions demonstrate the most disability in physical function?

Explanation
Pollak and associates found that the average SF-36 score for patients who sustained a pilon fracture was significantly lower than patients with diabetes mellitus, AIDS, hypertension, asthma, migraines, pelvic fracture, polytrauma, and AMI. Moreover, patients having undergone pilon fixation scored lower on all but three of the SF-36 scales (vitality, mental health, and emotional health).
Question 423
High Yield
A 28-year-old man sustained a shoulder dislocation 2 years ago. It remained dislocated for 3 weeks and required an open reduction. He now reports constant pain and has only 60 degrees of forward elevation and 10 degrees of external rotation. He desires to return to some sporting activities. An AP radiograph and intraoperative photograph (a view of the humeral head through a deltopectoral approach) are shown in Figures 31a and 31b. What is the best treatment option to decrease pain and improve function?

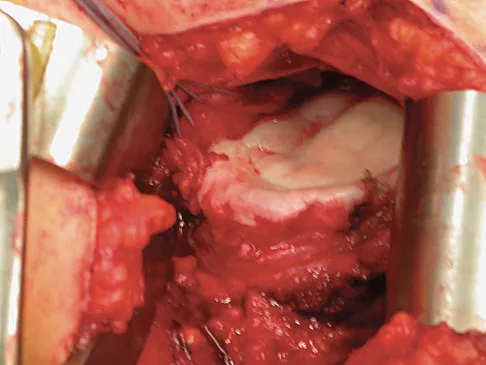
Explanation
The radiograph and intraoperative photograph show osteonecrosis with near complete head loss/collapse. A stemmed implant is more appropriate in this patient because there is very little bone to support a resurfacing implant. In a younger patient, a glenoid implant should be delayed as long as possible because of the eventual need for revision secondary to glenoid loosening and wear, especially in a young active male. The hemiarthroplasty may be converted to a total shoulder arthroplasty in the future. Levy O, Copeland SA: Cementless surface replacement arthroplasty of the shoulder: 5- to 10-year results with the Copeland mark-2 prosthesis. J Bone Joint Surg Br 2001;83:213-221.
Question 424
High Yield
Figure 23 shows the radiograph of a 7 year-old girl with a low thoracic-level myelomeningocele. She has a history of skin ulcers over the apex of the deformity, but her current skin condition is good. Management of the spinal deformity should consist of

Explanation
This form of severe kyphosis results in intractable difficulties with sitting position, compression of internal organs, and chronic skin breakdown. Kyphectomy and posterior fusion with instrumentation, while associated with a high rate of complications, provides one of the best solutions to this clinical dilemma. The other choices are either completely ineffective or inadequate in managing this degree of deformity. Lindseth RE: Spine deformity in myelomeningocele. Instr Course Lect 1991;40:273-279.
Question 425
High Yield
What mechanism contributes to strength gains during conditioning of the preadolescent athlete?
Explanation
Prepubescent athletes gain strength through neurogenic adaptations, including recruitment of motor units, reduced inhibition, and learned motor skills. Myogenic adaptations (muscle hypertrophy) occur after puberty and include increased contractile proteins, thickening of the connective tissue, and increased short-term energy sources such as creatine phosphate. Grana WA: Strength training, in Stanitski CL, DeLee JC, Drez D Jr (eds): Pediatric and Adolescent Sports Medicine. Philadelphia, PA, WB Saunders, 1994, pp 520-526.
Question 426
High Yield
Figures 2a and 2b show the radiographs of a 72-year-old man with aseptic loosening of the tibial component of his total knee arthroplasty. Optimal management should include

Explanation
The radiographs show massive subsidence of the lateral side of the tibia with severe tibial bone loss and a fractured proximal fibula. Reconstruction should consist of a large metal or bony lateral tibial augmentation, and a stem long enough to bypass the defect is required. The femoral and tibial components are articulating without any remaining polyethylene medially; therefore, the femoral component is damaged and needs revision. The insertions of the lateral ligaments are absent, thereby rendering the lateral side of the knee predictably unstable. Also, the large valgus deformity compromises the medial collateral ligament. The posterior cruciate ligament is also likely to be deficient with this much tibial bone destruction. The patient requires a posterior stabilized femoral component at the minimum, and possibly a constrained femoral component. Retention of the femoral component, even though it may be well-fixed, jeopardizes the outcome. Lotke PA, Garino JP: Revision Total Knee Arthroplasty. New York, NY, Lippincott-Raven, 1999, pp 137-250. Insall JN, Windsor RE, Scott WN, et al: (eds): Surgery of the Knee, ed 2. New York, NY, Churchill Livingstone, 1993, pp 935-957.
Question 427
High Yield
A 28-year-old man has a painful nodule on the plantar aspect of his foot in the midarch. Use of a soft orthosis has failed to provide relief. Examination reveals that the mass is approximately 2 1/2 cm in diameter, firm, and tender to palpation. An MRI scan confirms the presence of a plantar fibroma. Management should now consist of

Explanation
Plantar fibromas have an extremely high recurrence rate (approximately 60%) with local excision only. Resection of the entire plantar fascia is effective at irradicating the lesion. There is no role for chemotherapy or amputation with plantar fibromatosis. Radiation therapy may be helpful in combination with resection of the plantar fascia. Kirby EJ, Shereff MJ, Lewis MM: Soft-tissue tumors and tumor-like lesions of the foot: An analysis of 83 cases. J Bone Joint Surg Am 1989;71:621-626.
Question 428
High Yield
A 26-year-old woman is seen in the emergency department with an intra-articular distal tibia fracture and a fibular fracture (pilon). The patient, her husband, and three small children have recently immigrated to the United States from Mexico. The husband and wife have both been in a migrant labor camp but have no immediate relatives in the States. What factor is most important when considering her recommended care and treatment?

Explanation
With documented use of a competent interpreter, informed consent should not be an issue. In Hispanic families, the husband often makes the ultimate decision regarding proceeding with surgery; however, he would not be expected to withhold recommended treatment. Hispanics may have a higher risk of comorbidities, but you do not expect this to be a significant concern with this patient. Claustrophobia and some fear of the unfamiliar may make additional imaging studies more difficult to arrange, but not impossible. The real concern is that with no extended family and three small children, the postoperative demand on the patient could significantly jeopardize her ability to comply with weight-bearing restrictions and overall ambulatory demands. Discharge planning and appropriate help may be paramount for a good outcome.
Question 429
High Yield
An otherwise healthy 70-year-old man has back and bilateral leg pain in an L5 distribution that is aggravated by standing more than 10 minutes or walking more than 100 feet. He has to sit to get relief. Neurologic and pulse examinations are normal. A radiograph and MRI scan are shown in Figures 4a and 4b. Treatment should consist of

Explanation
The patient has a degenerative spondylolisthesis at L4-5 with associated spinal stenosis. His symptoms are consistent with neurogenic claudication. Based on these findings, the surgical treatment of choice is decompression and posterolateral fusion. Use of instrumentation is controversial. Laminectomy alone is reserved for the patient who is frail medically. There is no role for an anterior approach or for fusion alone without decompression. Fischgrund JS, Mackay M, Herkowitz HN, et al: Degenerative lumbar spondylolisthesis with spinal stenosis: A prospective, randomized study comparing decompressive laminectomy and arthrodesis with and without spinal instrumentation. Spine 1997;22:2807-2812.
Question 430
High Yield
Which of the following is considered the most common infectious organism causing osteochondritis in pediatric puncture wounds of the foot?
Explanation
Pseudomonas aeruginosa is the most common infectious organism causing osteochondritis in pediatric puncture wounds of the foot. Eikenella corrodens is found in human bites, and Pasteurella multocida is characteristically seen with animal bites. Serratia marcescens and Proteus mirabilis have been reported but are much less likely. Jacobs RF, Adelman L, Sack CM, et al: Management of pseudomonas osteochondritis complicating puncture wounds of the foot. Pediatrics 1982;69:432-435.
Question 431
High Yield
The blood supply to the anterior cruciate ligament is primarily derived from what artery?
Explanation
Microvascular studies have shown that the majority of the blood supply to the cruciate ligaments comes from the middle geniculate artery, although there is collateral flow through the other geniculates and from bone. Arnoczky SP: Blood supply to the anterior cruciate ligament and supporting structures. Orthop Clin North Am 1985;16:15-28.
Question 432
High Yield
A 47-year-old woman has a painful bunion of the right foot, and shoe wear modifications have failed to provide relief. Examination reveals a severe hallux valgus with dorsal subluxation of the second toe. Radiographs are shown in Figures 14a and 14b. The most appropriate management should include


Explanation
The radiographs do not show significant arthrosis of the hallux metatarsophalangeal joint; therefore, arthrodesis is unnecessary. Orthotics will not correct the deformity. A distally based osteotomy will not achieve sufficient correction of the incongruity of deformity, and a Keller resection is not indicated in the younger population. The treatment of choice is a proximal metatarsal osteotomy with second toe correction.
Question 433
High Yield
A 22-year-old female collegiate javelin thrower has shoulder pain. She notes that her pain is primarily located in the posterior aspect of her shoulder, is exacerbated with throwing, and she experiences maximal tenderness in the extreme cocking phase of the throwing cycle. On examination, she reports deep posterior shoulder pain when the arm is abducted 90 degrees and maximally externally rotated to 110 degrees. This reproduces her symptoms precisely. Shoulder radiographs are normal. What is the most likely diagnosis?
Explanation
The patient has internal impingement. Internal impingement is commonly seen in overhead throwing athletes. When positioned in the extreme cocking phase of the throwing cycle, the posterior glenoid impacts the articular surface of the infraspinatus and posterior fibers of the supraspinatus tendon. This impact can cause partial-thickness rotator cuff tearing and posterosuperior labral lesions. She has no evidence of anterior shoulder instability, and her range of motion is excellent which rules out adhesive capsulitis. Subacromial impingement is identified with anterolateral shoulder pain with internal rotation in the abducted position. A full-thickness rotator cuff tear in a 22-year-old individual would require significant trauma and would likely result in pain at rest and with lifting. Meister K, Buckley B, Batts J: The posterior impingement sign: Diagnosis of rotator cuff and posterior labral tears secondary to internal impingement in overhand athletes. Am J Orthop 2004;33:412-415.
Question 434
High Yield
In the normal adult, the distance between the basion and the tip of the dens with the head in neutral position is how many millimeters?
Explanation
In the normal adult, the distance between the basion and the tip of the dens is 4 mm to 5 mm. Any distance greater than 5 mm is considered abnormal. This is one way to detect occipitocervical dissociation other than using the Power's ratio, which relies on an anterior dislocation. Wiesel SW, Rothman RH: Occipitoatlantal hypermobility. Spine 1979;4:187-191.
Question 435
High Yield
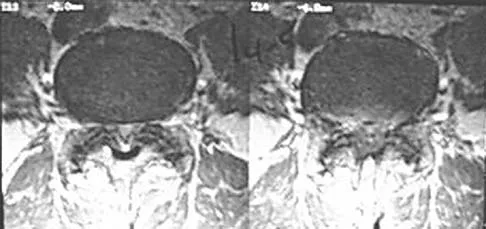
A 2-year-old child has been referred for management of congenital kyphosis. Neurologic examination is normal, and radiographs show a type I congenital kyphosis. Which of the following anomalies is seen in the MRI scan shown in Figure 6?

Explanation
There is a high incidence of intraspinal anomalies in patients with congenital scoliosis and kyphosis. Bradford and associates reported an incidence rate of 38% in 42 patients. The MRI scan shows that the filum terminale is thickened and adherent distally in the spinal canal. Although the conus is at L1, which may be normal, neurologic dysfunction may occur with further growth. There are no signals of high intensity within the cord that would suggest a syrinx. A Chiari II malformation would be found in the upper cervical region, not shown in this MRI scan. Meningocele and diastematomyelia are not present. Bradford DS, Heithoff KB, Cohen M: Intraspinal abnormalities and congenital spine deformities: A radiographic and MRI study. J Pediatr Orthop 1991;11:36-41.
Question 436
High Yield
Figures 36a and 36b show the MRI scans of a patient who has shoulder weakness. What is the most likely diagnosis?

Explanation
The sagittal image reveals increased signal and decreased size of the supraspinatus and infraspinatus muscles, indicating muscle atrophy. The rotator cuff tendon signal is normal. The subscapularis and teres minor muscles are unaffected. Muscular dystrophy and thoracic outlet syndrome would be expected to have a more global effect. Although muscular atrophy can occur in the setting of a rotator cuff tear, the coronal image shows an intact supraspinatus. The suprascapular nerve supplies the supraspinatus and infraspinatus muscles. Therefore, suprascapular nerve entrapment would result in atrophy of these muscles with sparing of the surrounding musculature. Any lesion within the suprascapular notch, including neoplastic disease, a venous varix, or neuroma, can place pressure on the suprascapular nerve. Suprascapular nerve entrapment most commonly results from extension of a paralabral cyst or ganglion, often with associated labral pathology. Spinal accessory nerve disruption would show trapezius muscle atrophy. Resnick D, Kang HS (eds): Internal Derangement of Joints: Emphasis on MR Imaging. Philadelphia, PA, WB Saunders, 1997, pp 308-317.
Question 437
High Yield
A 30-year-old woman who runs approximately 30 miles a week has had right hip and groin pain for the past 3 weeks. Examination reveals an antalgic gait, limited motion of the right hip, and pain, especially with internal and external rotation. Plain radiographs are normal, and an MRI scan is shown in Figure 21. Management should consist of

Explanation
A stress fracture of the hip is a relatively common problem in endurance sports. These fractures are classified as compression-side, tension-side, and displaced femoral neck fractures. The MRI scan shows a compression-side stress fracture. Compression-side fractures usually occur in the inferior or calcar area of the proximal femur, and non-weight-bearing crutch ambulation for 6 to 7 weeks will most likely result in healing. Once the patient is walking without pain or a limp, activities can be slowly increased. Because tension-side fractures have a high risk of displacement, treatment should consist of immediate internal fixation. Griffin LY (ed): Orthopaedic Knowledge Update: Sports Medicine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 239-253.
Question 438
High Yield
A 6-year-old child has a fixed flexion deformity of the interphalangeal (IP) joint of the right thumb. The thumb is morphologically normal, with a nontender palpable nodule at the base of the metacarpophalangeal joint. Clinical photographs are shown in Figures 42a and 42b. Based on these findings, what is the treatment of choice?


Explanation
The child has a trigger thumb deformity. A trigger thumb is a developmental mechanical problem rather than a congenital deformity. The anomaly generally is not noted at birth. A fixed flexion deformity of the IP joint of the thumb most commonly occurs in children in the first 2 years of life. A stretching and splinting program may correct the deformity in the first year of life, but nonsurgical management after age 3 years results in a success rate of only 50%. Release of the proximal annular pulley of the flexor sheath is recommended at this age. Tan AH, Lam KS, Lee EH: The treatment outcome of trigger thumb in children. J Pediatric Orthop B 2002;11:256-259. Slakey JB, Hennrikus WL: Acquired thumb flexion contracture in children: Congenital trigger thumb. J Bone Joint Surg Br 1996;78:481-483.
Question 439
High Yield
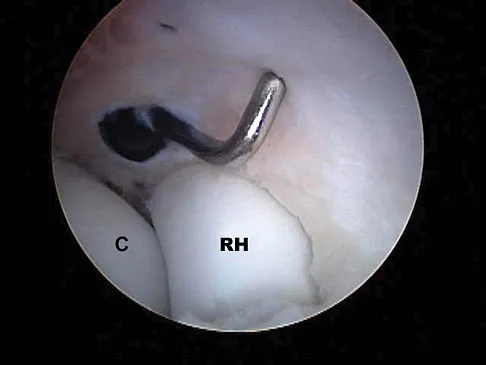
A 24-year-old athlete has a painful right shoulder. Figure 30 shows an intra-articular photograph that was obtained through a posterior portal during arthroscopy; the labrum is indicated by the arrow. Based on these findings, management should consist of
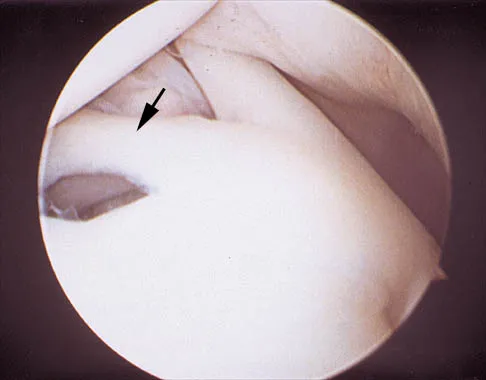
Explanation
The photograph shows a normal variant that is a sublabral hole beneath the anterosuperior labrum. In some instances, the labrum will become confluent with the middle glenohumeral ligament as a stout band. Because this variant is not abnormal, no treatment is necessary. Securing this portion of the labrum to the capsule may tighten the middle glenohumeral ligament complex and restrict external rotation of the arm. Andrews JR, Guerra JJ, Fox GM: Normal and pathologic arthroscopic anatomy of the shoulder, in Andrews JR, Timmerman LA (eds): Diagnostic and Operative Arthroscopy, ed 1. Philadelphia, PA, WB Saunders, 1997, pp 60-76.
Question 440
High Yield
An 18-year-old hockey player sustains an acute anterior shoulder dislocation that requires manual reduction. At arthroscopy, the lesion shown in Figure 24 will be observed in what percent of patients?
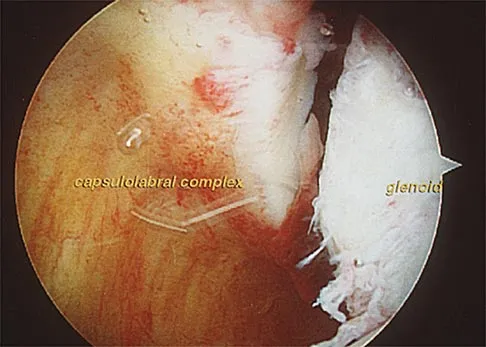
Explanation
The clinical photograph shows an acute capsulolabral avulsion from the anterior glenoid, also referred to as a Perthes-Bankart lesion. In patients who sustain an acute dislocation that requires a manual reduction, this pathologic lesion is observed with high frequency. In several research studies, it has been visualized in 80% to 95% of patients at arthroscopy. Taylor DC, Arciero RA: Pathologic changes associated with shoulder dislocations: Arthroscopic and physical examination findings in first-time, traumatic anterior dislocations. Am J Sports Med 1997;25:306-311.
Question 441
High Yield
Figure 36 shows an AP radiograph of a 65-year-old man who reports activity-related groin pain. History reveals that he underwent total hip arthroplasty 12 years ago. What is the most likely diagnosis?

Explanation
The AP radiograph demonstrates extensive periacetabular osteolysis. The central hole eliminator has dissociated from the shell and migrated into a lytic defect in the ischium. In a retrieval study, most periacetabular osteolytic lesions had a clear communication pathway with the joint space. Lesions with communication to the joint via several pathways or through a central dome hole (as in this patient) were larger and more likely to be associated with cortical erosion. Although periprosthetic tumors have been described, they are rare and particle-induced inflammation around a prosthesis does not seem to increase the risk for carcinogenesis. Visuri T, Pulkkinen P, Paavolainen P: Malignant tumors at the site of total hip prosthesis: Analytic review of 46 cases. J Arthroplasty 2006;21:311-323. Bezwada HP, Shah AR, Zambito K, et al: Distal femoral allograft reconstruction for massive osteolytic bone loss in revision total knee arthroplasty. J Arthroplasty 2006;21:242-248.
Question 442
High Yield
A 67-year-old woman is seen in the emergency department after falling at home. Radiographs before and after treatment are shown in Figures 49a and 49b, respectively. Which of the following best explains the 8-week postinjury clinical findings seen in Figure 49c?



Explanation
Patients older than age 40 years at the time of initial anterior dislocation have low rates of redislocation; however, 15% of these patients experience a rotator cuff tear. Moreover, there is a dramatic increase (up to 40%) in the incidence of rotator cuff tears in patients older than age 60 years. Axillary nerve injury may occur but is less common than rotator cuff tear. Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 273-284.
Question 443
High Yield
When compared to traditional open repair through a posterior incision, percutaneous Achilles tendon repair clearly results in a reduction of what complication?
Explanation
Prospective studies, including randomized and randomized multicenter reports, have shown that percutaneous or mini-open acute Achilles tendon repair has comparable functional results when compared to traditional open techniques. Calder and Saxby reported one superficial infection out of 46 patients with a mini-open repair; Assal and associates and Cretnik and associates had no wound complications or infections. The other complications have not proved to be less likely with the mini-open or percutaneous technique. Assal M, Jung M, Stern R, et al: Limited open repair of Achilles tendon ruptures: A technique with a new instrument and findings of a prospective multicenter study. J Bone Joint Surg Am 2002;84:161-170. Calder JD, Saxby TS: Early, active rehabilitation following mini-open repair of Achilles tendon rupture: A prospective study. Br J Sports Med 2005;39:857-859.
Question 444
High Yield
A newborn has been referred for evaluation of a deformed foot. Prenatal and birth history are unremarkable. Examination reveals a rocker bottom appearance to the foot, and a longitudinal arch cannot be created. A palpable lump is appreciated on the plantar medial surface. What is the best course of action?

Explanation
The patient has congenital vertical talus. The navicular is irreducibly dorsally dislocated on the talus with the talar head prominent on the plantar medial aspect of the foot. Initial management involves corrective casting for 3 months to stretch the dorsal tendons, skin, and neurovascular structures. Surgical reconstruction is often needed and is indicated when the patient is age 6 to 12 months. Reconstruction requires both bony and soft-tissue procedures. Napiontek M: Congenital vertical talus: A retrospective and critical review of 32 feet operated on by peritalar reduction. J Pediatr Orthop 1995;4:179-187.
Question 445
High Yield
An 8-year-old boy sustains nondisplaced midshaft fractures of the tibia and fibula after being struck by a car while he was riding his bicycle. No other injuries are noted, but the patient reports pain with passive motion of his toes. His neurovascular examination is otherwise normal. What is the best course of action?
Explanation
Pain with passive motion of the toes is a recognized early sign of increased compartment pressures. At a minimum, a baseline evaluation of the leg compartment pressures should be obtained. While it is normal for the patient to have pain related to the associated muscle contusions, any significant concerns should be addressed immediately in light of the severe consequences likely when a compartment syndrome occurs. Mubarak SJ, Owen CA, Hargens AR, et al: Acute compartment syndromes: Diagnosis and treatment with the aid of the wick catheter. J Bone Joint Surg Am 1978;60:1091-1095.
Question 446
High Yield
A patient reports persistent anterior shoulder pain following a forceful external rotation injury to the shoulder. An MRI scan is shown in Figure 4. The patient remains symptomatic despite 3 months of nonsurgical management. Treatment should now consist of
Explanation
The MRI scan reveals a subscapularis tear with a biceps that is out of the groove. Treatment in this patient is most predictable if the subscapularis is repaired. The biceps should either be tenodesed or tenotomized since it is unstable. Recentering of the biceps has been found to be unpredictable. Treatment of these lesions has been shown to have better results if the biceps is either released or tenodesed. This prevents recurrent biceps symptoms that can be source of surgical failure. Edwards TB, Walch G, Sirvenaux F, et al: Repair of tears of the subscapularis: Surgical technique. J Bone Joint Surg Am 2006;88:1-10. Deutsch A, Altcheck DW, Veltri DM, et al: Traumatic tears of the subscapularis tendon: Clinical diagnosis, magnetic resonance imaging findings, and operative treatment. Am J Sports Med 1997;25:13-22.
Question 447
High Yield
A 22-year-old volleyball player has atrophy of the infraspinatus muscle. This deficit is the result of entrapment of what nerve?
Explanation
Suprascapular deficits, as the result of repetitive forceful internal rotation with overhead ball striking, occur in the spinoglenoid notch. Compression interferes with distal suprascapular nerve innervation to the infraspinatus, while allowing the supraspinatus to function normally. A scapular notch entrapment of this nerve would involve both the supraspinatus and the infraspinatus. The axillary, dorsal scapular, and subscapular nerves do not affect the infraspinatus. Ferretti A, Cerullo G, Russo G: Suprascapular neuropathy in volleyball players. J Bone Joint Surg Am 1987;69:260-263.
Question 448
High Yield
A 59-year-old man underwent interposition arthroplasty for osteoarthritis of the elbow 9 years ago. Over the past year the patient has had increasing pain and elbow instability. There is no clinical evidence of infection, and radiographs show no new bony process. What is the best option for this patient?

Explanation
In a series reported by Blaine and associates, 12 patients were converted from interposition to total elbow arthroplasty. This procedure was successful in 10 out of 12 patients. Blaine TA, Adams R, Morrey BF: Total elbow arthroplasty after interposition arthroplasty for elbow arthritis. J Bone Joint Surg Am 2005;87;286-292.
Question 449
High Yield
A 21-year-old soccer player reports pain and is unable to straighten his knee following an acute injury during a game. He is unable to continue to play. An MRI scan is shown in Figure 3. What is the next most appropriate step in management?
Explanation
The patient has a locked knee that cannot be fully extended. This is most likely the result of the mechanical block of a bucket-handle tear that has flipped into the notch. Also, the pain may be so severe that the muscle spasm prevents the knee from straightening out. When the patient is anesthetized, the muscle spasm relaxes and the meniscus can be reduced out of the notch. Arthroscopy is the treatment of choice. A meniscal repair is usually possible in large bucket-handle tears because the meniscus is torn in the red-red zone where most of the vascular supply is located. If the handle portion is badly frayed or damaged, a partial meniscectomy should be performed. The classic finding on MRI is a "double PCL sign." This is due to the flipped portion of the meniscus in the notch. Critchley IJ, Bracey DJ: The acutely locked knee: Is manipulation worthwhile? Injury 1985;16:281-283.
Question 450
High Yield
Figure 11a shows the clinical photograph of a 46-year old woman who reports a 3-week history of pain and a "lump" at the base of her neck. She is otherwise in good health and denies any trauma. A 3-D reconstruction CT is shown in Figure 11b. What is the most likely diagnosis?

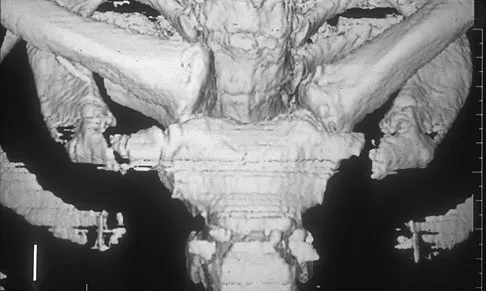
Explanation
Spontaneous subluxation of the sternoclavicular joint occurs without any significant trauma. It is usually accentuated by placing the extremity in an overhead position. Discomfort usually resolves within 4 to 6 weeks with nonsurgical management. Rockwood CA, Wirth MA: Disorders of the sternoclavicular joint, in Rockwood CA, Matsen FA, Wirth MA, et al (eds): The Shoulder. Philadelphia, PA, WB Saunders, 2004, vol 2, pp 1078-1079.
Question 451
High Yield
A 32-year-old woman sustained an injury to her left upper extremity in a motor vehicle accident. Examination reveals a 2-cm wound in the mid portion of the dorsal surface of the upper arm and deformities at the elbow and forearm; there are no other injuries. Her vital signs are stable, and she has a base deficit of minus 1 and a lactate level of less than 2. Radiographs are shown in Figures 9a and 9b. In addition to urgent debridement of the humeral shaft fracture, management should include


Explanation
With a severe injury to the upper extremity, the best opportunity for achieving a good functional result for a floating elbow is immediate debridement of the open fracture, followed by internal fixation of the fractures. The ability to do this depends on the patient's physiologic status. In this patient, the procedure is acceptable because she has normal vital signs and no chest or abdominal injuries, and normal physiologic parameters (base excess and lactate) show adequate peripheral perfusion. The surgical approaches will be determined by the associated injury patterns and open wounds. In this patient, the humerus was debrided and stabilized through a posterior approach as was the medial condyle fracture. The ulna was fixed through an extension of the posterior incision and the radius through a separate dorsal approach. Solomon HB, Zadnik M, Eglseder WA: A review of outcomes in 18 patients with floating elbow. J Orthop Trauma 2003;17:563-570.
Question 452
High Yield
What is the most common indication for revision following unconstrained elbow arthroplasty?

Explanation
Instability following unconstrained elbow arthroplasty occurs in 10% of patients. Subluxation is twice as common as frank dislocation; however, only 20% of these patients undergo revision. Instability following unconstrained elbow arthroplasty can be caused by component malposition or ligament insufficiency. King GJ, Itoi E, Niebur GL, et al: Motion and laxity of the capitellocondylar total elbow prosthesis. J Bone Joint Surg Am 1994;76:1000-1008.
Question 453
High Yield
The illustration shown in Figure 19 shows a Chamberlain line. What is the most likely diagnosis?
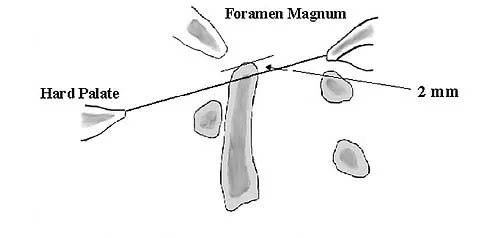
Explanation
Basilar invagination is best defined as vertical or compressive instability at the occiput-C1 joint. Such invaginations most commonly occur in patients with rheumatoid arthritis but also can occur secondary to trauma or tumor. A Chamberlain line is used as a method to determine basilar invagination. The odontoid tip should not be more than 5 mm above a Chamberlain line. Wiesel SW, Rothman RH: Occipito-atlantal hypermobility. Spine 1979;4:187-191.
Question 454
High Yield
An 18-year-old football player reports acute pain and swelling after a direct injury to his plantar flexed foot. Examination reveals midfoot swelling and tenderness. Nonstanding radiographs are normal. What is the next most appropriate step in management?

Explanation
Differentiating between a midfoot sprain and Lisfranc diastasis is critical in the management of the athlete with an acute injury to the midfoot. Greater than 2 mm of displacement between the first and second metatarsals on a weight-bearing radiograph is an indication for anatomic reduction with internal fixation of the tarsometatarsal joints. If no subluxation is noted, treatment should consist of a non-weight-bearing cast for 6 weeks, followed by a gradual return to activity. Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 39-54.
Question 455
High Yield
A 24-year-old woman has a spleen laceration and hypotension. Radiographs reveal a pulmonary contusion and a displaced mid-diaphyseal fracture of the femur. The trauma surgeon clears her for stabilization of the femoral fracture. What technique will offer the least potential for initial complications?

Explanation
A concern in the multiply injured patient who has a pulmonary contusion is the potential for further pulmonary compromise because of embolization of marrow, blood clot, or fat during manipulation of the medullary canal. Recent evidence has shown that the presence of a lung injury is the most important determining factor in future deterioration. However, despite the lung injury and its potential consequences, this patient's femur fracture needs stabilization. Because damage control in the multiply injured patient requires a technique that can be performed rapidly and consistently, the treatment of choice is application of an external fixator. By placing two pins above and below the fracture and with longitudinal traction, the fracture is quickly realigned and stabilized. This allows the patient to be resuscitated and treated at a later date when definitive management of the fracture can be carried out. There is little difference between plate fixation and intramedullary nailing. Bosse MJ, MacKenzie EJ, Riemer BL, et al: Adult respiratory distress syndrome, pneumonia, and mortality following thoracic injury and a femoral fracture treated with either intramedullary nailing with reaming or with a plate: A comparative study. J Bone Joint Surg Am 1997;79:799-809. Scalea TM, Boswell SA, Scott JD, Mitchell KA, Kramer ME, Pollak AN: External fixation as a bridge to intramedullary nailing for patients with multiple injuries and with femur fractures: Damage control orthopedics. J Trauma 2000;48:613-623.
Question 456
High Yield
A 25-year-old woman has significant pain and swelling in her left ankle after falling off her bicycle. Examination reveals that she is neurovascularly intact. Radiographs are shown in Figures 33a through 33c. What is the next most appropriate step in management?



Explanation
The radiographs show a displaced ankle fracture with widening of the syndesmosis. Open reduction and internal fixation is indicated with fixation of the mortise with syndesmotic screws. Wuest TK: Injuries to the distal lower extremity syndesmosis. J Am Acad Orthop Surg 1997;5:172-181.
Question 457
High Yield
A 36-year-old woman has neck pain in the upper cervical region and occipital discomfort after being involved in a motor vehicle accident. Examination reveals no forehead or scalp lacerations. The neurologic examination is normal. A CT scan shows no evidence of bony injury. Figures 39a and 39b show a lateral radiograph and an MRI scan. Management should consist of


Explanation
The lateral radiograph shows 8 mm of atlantoaxial translation. In the absence of a bony injury, this represents rupture of the transverse atlantal ligament. The MRI scan reveals soft-tissue swelling posterior to the odontoid and a high intensity zone in the atlanto-dens interval consistent with acute injury. These injuries require arthrodesis because nonsurgical measures will not provide stability. Techniques for C1-2 fusion include Gallie, Brooks, or triple wiring. Transarticular screw fixation across the C1-2 articulation provides the most rigid means of fixation and the highest arthrodesis rates but is technically demanding. Anterior C2-3 arthrodesis will not address the level of instability. The normal atlanto-dens interval is 3 mm in an adult and 4 mm in a child. Kurz LT: Transverse atlantal ligament insufficiency, in Clark CR (ed): The Cervical Spine. Philadelphia, PA, Lippincott-Raven, 1998, pp 401-407.
Question 458
High Yield
A 30-year-old man landed on his shoulder in a fall off his mountain bike. An AP radiograph and CT scan are shown in Figures 34a and 34b. Management should consist of

Explanation
The radiograph shows a valgus impacted four-part fracture. The humeral head is deeply depressed into the metaphysis but is still articulating with the glenoid as seen on the CT scan. Unlike a "classic" four-part fracture in which the head is dislocated out of the glenoid and devoid of any soft-tissue attachments (high risk of osteonecrosis), this valgus impacted head will have a medial soft-tissue hinge with a lower risk of osteonecrosis. It is most amenable to open reduction and internal fixation with minimal soft-tissue stripping techniques. Bone grafting may be necessary on occasion. Nonsurgical management for displaced proximal humeral fractures generally results in a poor outcome. This patient does not have a humeral head defect. A hemiarthroplasty is not indicated. Jakob RP, Miniaci A, Anson PS, et al: Four-part valgus impacted fractures of the proximal humerus. J Bone Joint Surg Br 1991;73:295-298.
Question 459
High Yield
Figure 20 shows the radiograph of a 21-year-old college basketball player who jammed his left index finger on the rim. He reports pain and tenderness over the dorsum of the distal interphalangeal (DIP) joint. Examination reveals that he is unable to actively extend the DIP joint; however, the skin is intact. Management should consist of

Explanation
Mallet fingers without DIP joint subluxation can be treated with extension splinting. Surgical fixation may be necessary in bony mallet injuries when the joint is subluxated. Size of the bony fragment, while often correlating with stability, is not always an indication for fixation. Buddy taping allows motion; therefore, the fragment will not heal in the appropriate position. Intermittent splinting with range-of-motion exercises also will not allow the fragment to heal in the appropriate position. Crawford GP: The molded polyethylene splint for mallet finger deformities. J Hand Surg Am 1984;9:231-237.
Question 460
High Yield
Figure 44 shows the radiograph of an 11-year-old girl who has hip pain. Further diagnostic workup should include

Explanation
The patient has severe acetabular protrusio, a condition that is frequently associated with Marfan syndrome. An echocardiogram is necessary to rule out the most serious consequence of this syndrome, aortic root widening, which can lead to aortic valve dysfunction or fatal aortic rupture. An electromyogram may be indicated for Charcot-Marie-Tooth disease, which is associated with acetabular dysplasia, but not protrusio. The renal ultrasound, the MRI scan, and the biopsy would be of no value in this patient. Protrusio can also be seen in patients with osteogenesis imperfecta and juvenile rheumatoid arthritis. Steel HH: Protrusio acetabuli: Its occurrence in the completely expressed Marfan syndrome and its musculoskeletal component and a procedure to arrest the course of protrusion in the growing pelvis. J Pediatr Orthop 1996;16:704-718.
Question 461
High Yield
New painful paresthesias near the site of the incision after an ulnar nerve transposition is the result of injury to what nerve?

Explanation
Branches of the medial antebrachial cutaneous nerve can often be identified during routine ulnar nerve surgery crossing the medial aspect of the elbow. It should be preserved to avoid development of painful paresthesias.
Question 462
High Yield
A 60-year-old man reports increasing pain in his right foot with limited ankle dorsiflexion and anterior ankle pain after sustaining a fracture of the calcaneus in a fall several years ago. Bracing, nonsteroidal anti-inflammatory drugs, and cortisone injections have failed to provide significant relief. Radiographs are shown in Figures 19a and 19b. What is the next most appropriate step in management?


Explanation
Following a calcaneal fracture, the patient has severe subtalar arthritis with loss of talar declination and shortening of the heel; therefore, the treatment of choice is subtalar distraction arthrodesis. Orthotics will not provide significant relief as bracing has failed. Ankle arthrodesis will not be beneficial because the arthritis is in the subtalar joint. Subtalar arthroscopy would only be helpful for a small area of arthrosis, and calcaneal osteotomy would not be beneficial given the extent of the arthritis of the subtalar joint.
Question 463
High Yield
An 82-year-old man has had episodic right thigh pain after undergoing a total hip arthroplasty 10 years ago. Initial postoperative radiographs are shown in Figures 26a and 26b, and current radiographs are shown in Figures 26c and 26d. What is the most likely cause of his pain?




Explanation
These radiographs are dominated by the subsidence of the femoral component. There is also evidence of polyethylene wear and femoral osteolysis in the region of the greater trochanter. There is no evidence of proximal (calcar) stress shielding, and there is a thick distal pedestal. Engh and associates defined two major signs of osseointegration - the absence of radiolucent lines around the porous-surfaced portion of the implant and new bone bridging the gap between the endosteal surface and the porous portion of the implant. Implant migration indicates failure of ingrowth. Osteolysis is a periprosthetic loss of bone secondary to particulate debris and it is often clinically silent unless it is accompanied by pathologic fracture. It is often globular. Acetabular loosening is based on radiolucent lines and implant migration. The current radiographs demonstrate subsidence of the stem with pedestal formation. Engh CA, Massin P, Suthers KE: Roentgenographic assessment of biologic fixation of porous-surface femoral components. Clin Orthop Relat Res 1990;257:107-128.
Question 464
High Yield
Figure 3 shows the radiographs of a 32-year-old man who fell 12 feet onto his outstretched arm and sustained a fracture-dislocation of the elbow. Initial management consisted of closed reduction of the dislocation. Surgical treatment should now include repair or reduction and fixation of the

Explanation
The radiographs show fractures of the coronoid and radial head. The medial collateral ligament has been avulsed from the ulnar insertion, and there is a valgus opening on the medial side. The lateral collateral ligament is always disrupted in elbow dislocations and fracture-dislocations that occur secondary to falls. This is known as the terrible triad injury (dislocation and fractures of the coronoid and radial head); it has a very poor prognosis because of its propensity for recurrent or persistent instability and late arthritis. The principle in treating this injury is to repair all of the injured parts or protect them with a hinged external fixator until they heal. Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 345-354. Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 283-294.
Question 465
High Yield
Figure 17 shows the clinical photograph of a 45-year-old female tennis player who has right arm pain and weakness with elevation after undergoing a cervical biopsy several months ago. The cause of her shoulder weakness is damage to the

Explanation
The patient has primary scapulotrapezius winging caused by surgical damage to the spinal accessory nerve during a lymph node biopsy. Other causes include blunt trauma, traction, and penetrating injuries. With spinal accessory palsy, the shoulder appears depressed and laterally translated because of unopposed serratus anterior muscle function. With primary serratus anterior winging that is the result of long thoracic nerve palsy, the scapula assumes a position of elevation and medial translation with the inferior angle rotated medially. The thoracodorsal nerve innervates the latissimus dorsi and is not associated with scapular winging. Kuhn JE, Plancher KD, Hawkins RJ: Scapular winging. J Am Acad Orthop Surg 1995;3:319-325.
Question 466
High Yield
An otherwise healthy 57-year-old woman has limited range of motion and moderate effusion after undergoing total knee arthroplasty 6 months ago. One of two cultures of joint aspirate reveals methicillin-resistant Staphylococcus epidermidis. Management should now consist of
Explanation
The rapidly increasing prevalence of infection from Staphylococcus epidermidis has made this the most frequently cultured organism. In most patients, the infection occurred intraoperatively, thereby resulting in a chronic infection if not detected within the first 6 weeks after surgery. Irrigation of the joint may be successful during this time in 60% of patients, but the most successful treatment is extirpation for 6 weeks, followed by delayed reimplantation. This approach may result in a salvage rate of as high as 90% in some patients. Drancourt M, Stein A, Argenson JN, et al: Oral rifampin plus ofloxacin for treatment of staphylococcus-infected orthopedic implants. Antimicrob Agents Chemother 1993;37:1214-1218. Duncan CP, Beauchamp C: A temporary antibiotic-loaded joint replacement system for the management of complex infections involving the hip. Orthop Clin North Am 1993;24:751-759.
Question 467
High Yield
Nutritional rickets is associated with which of the following changes in chemical blood level?
Explanation
Nutritional rickets is associated with decreased dietary intake of Vitamin D, resulting in low levels of Vitamin D that result in decreased intestinal absorption of calcium and low to normal serologic levels of calcium. To boost serum calcium levels, there is a compensatory increase in PTH and bone resorption, leading to increased alkaline phosphatase levels. Brinker MR: Cellular and molecular biology, immunology, and genetics in orthopaedics, in Miller MD (ed): Review of Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2001, pp 81-94. Pettifor J: Nutritional and drug-induced rickets and osteomalacia, in Farrus MJ (ed): Primer on the Metabolic Bone Diseases and Disorders of Mineral Metabolism, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2003, pp 399-466.
Question 468
High Yield
A 36-year-old woman sustained a tarsometatarsal joint fracture-dislocation in a motor vehicle accident. The patient is treated with open reduction and internal fixation. What is the most common complication?

Explanation
The most common complication associated with tarsometatarsal joint injury is posttraumatic arthritis. In one series, symptomatic arthritis developed in 25% of the patients and half of those went on to fusion. In another series, 26% had painful arthritis. Initial treatment should consist of shoe modification, inserts, and anti-inflammatory drugs. Fusion is reserved for failure of nonsurgical management. Hardware failure may occur, but it is clinically unimportant. Kuo RS, Tejwani NC, DiGiovanni CW, et al: Outcome after open reduction and internal fixation of Lisfranc joint injuries. J Bone Joint Surg Am 2000;82:1609-1618. Arntz CT, Veith RG, Hansen ST Jr: Fractures and fracture-dislocations of the tarsometatarsal joint. J Bone Joint Surg Am 1988;70:173-181.
Question 469
High Yield
Figures 20a and 20b show the radiographs of a 14-year-old boy who sustained a twisting injury to his ankle. If attempted closed reduction is unsuccessful, what is the primary reason to proceed with surgical treatment?


Explanation
Triplane fractures generally occur in children who are near skeletal maturity. The injury is generally caused by a supination external rotation mechanism. The number of fracture fragments present (two or three) depends on what part of the physes is closed at the time of injury. Articular congruity is the major concern in the management of these injuries since the patient has almost reached skeletal maturity. The goal is to restore articular congruity to minimize the development of posttraumatic arthritis. Vaccaro A (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 757-765. Kling TF Jr, Bright RW, Hensinger RN: Distal tibial physeal fractures in children that may require open reduction. J Bone Joint Surg Am 1984;66:647-657.
Question 470
High Yield
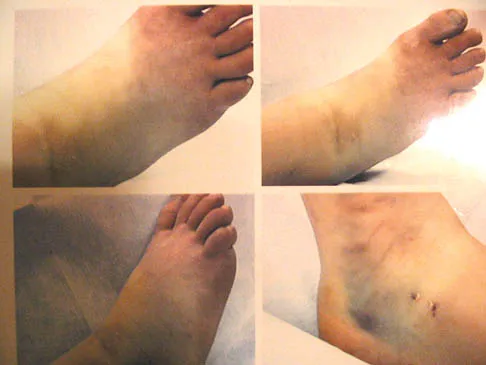
A 45-year-old man sustains a low-velocity gunshot wound to the base of the right thumb. The open wound is allowed to heal by secondary intention, resulting in a contracture of the first web space. Clinical photographs are shown in Figures 49a through 49c. Treatment should now consist of



Explanation
The contracture is too large for a Z-plasty, which allows a 75% increase in length. Excision of the scar with placement of a skin graft is prone to contracture. A posterior interosseous fasciocutaneous flap will provide enough well-vascularized tissue and is well suited to reach the first dorsal web space. Buchler U, Frey HP: Retrograde posterior interosseous flap. J Hand Surg Am 1991;16:283-292.
Question 471
High Yield
A 45-year-old man reports that he awoke 2 weeks ago with severe pain in his right arm. Examination reveals weakness in the biceps, brachialis, and wrist extensors. There is decreased sensation in the thumb and index finger and a diminished brachioradialis reflex. Assuming this patient has a posterolateral herniated nucleus pulposus, what level is involved?

Explanation
This is a classic C6 nerve injury, and it is most likely the result of a herniated nucleus pulposus at C5-6. The C5 nerve root controls the elbow flexors, shoulder abductors, and external rotators. The C7 nerve root controls the elbow extensors, wrist pronators, and the triceps reflex. Standaert CJ: The patient history and physical examination: Cervical, thoracic and lumbar, in Herkowitz HN, Garfin SR, Eismont FJ, et al (eds): Rothman-Simeone The Spine, ed 5. Philadelphia, PA, Saunders Elsevier, 2006, vol 1, pp 171-186.
Question 472
High Yield
The correct starting point for an external fixation half pin placed into the anterior inferior iliac spine (AIIS) is labeled by what letter in Figure 3?
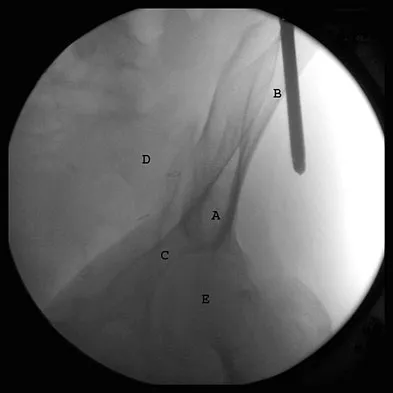
Explanation
Half pins placed in the AIIS are an alternative to pins placed in the iliac crest. A strong pillar of bone runs from the AIIS to the posterior iliac crest and less soft tissue is typically present in this area. The starting point is best seen on an obturator outlet view. The obturator outlet view is a combination of the pelvic outlet view and the obturator view of Judet and Letournel. The beam is rotated "over the top" of the patient since the iliac wing is externally rotated as well as cephalad to best visualize this column of bone running from the AIIS to the posterior iliac spine. This corridor of bone will appear as a teardrop. Once the correct view is obtained, the pin should be started at least 2 cm proximal to the hip joint to avoid placing a pin within the hip capsule. Blunt dissection and a guide sleeve should be used to prevent damage to the lateral femoral cutaneous nerve. An iliac oblique view is used after the pin has been partially inserted to make sure the pin is passing superior to the superior gluteal notch, and an obturator inlet view can be used at the completion of the procedure to make sure the pin is contained within the bone for its entire length. Gardner MJ, Nork SE: Stabilization of unstable pelvic fractures with supra-acetabular compression external fixation. J Orthop Trauma 2007;21:269-273. Haidukewych GJ, Kumar S, Prpa B: Placement of half-pins for supra-acetabular external fixation: An anatomic study. Clin Orthop Relat Res 2003;411:269-273.
Question 473
High Yield
A 48-year-old woman has knee pain that is worse with weight bearing. She reports no night pain or pain at rest. History reveals that she underwent total knee arthroplasty with cementless components 2 years ago. Examination reveals tenderness along the medial joint line. Figures 12a through 12c show radiographs and a bone scan. What is the most likely cause of the patient's pain?

Explanation
The radiographs show a halo-like sclerotic margin around the tibial stem and lucency under the baseplate. The bone scan shows markedly increased uptake under the tibial component, particularly on the medial side (not diffusely through the knee as seen with infection). These studies indicate lack of bone ingrowth fixation of the cementless porous-coated tibial component. The recent report of Fehring and associates has identified failure of ingrowth of a porous-coated implant as a dominant mode of early failure of total knee arthroplasties. Fehring TK, Odum S, Griffin WL, Mason B, Nadaud M: Early failures of total knee arthroplasty. Clin Orthop 2001;392:315-318.
Question 474
High Yield
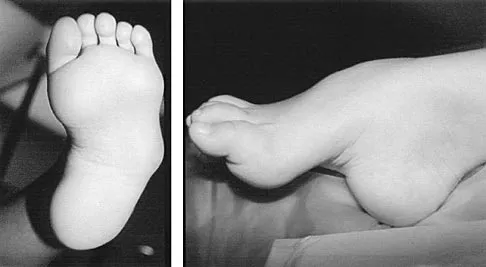
Figures 8a and 8b show the clinical photograph and radiograph of a 4-month-old infant who has a left foot deformity. Examination reveals that the foot deformity is an isolated entity, and the infant has no known neuromuscular conditions or genetic syndromes. Which of the following studies will best confirm the diagnosis?


Explanation
The clinical photograph shows a rocker-bottom deformity, and the lateral radiograph suggests a congenital vertical talus deformity. A lateral radiograph of the foot in maximum plantar flexion is needed to demonstrate the fixed position of the deformity with malalignment of the talar-metatarsal axis. A fixed dislocation of the navicular on the talus differentiates a congenital vertical talus from the oblique talus with talonavicular subluxation. Kumar SJ, Cowell HR, Ramsey PL: Vertical and oblique talus. Instr Course Lect 1982;31:235-251. Kodros SA, Dias LS: Single-stage correction of congenital vertical talus. J Pediatr Orthop 1999;19:42-48.
Question 475
High Yield
What is the typical MRI signal intensity of bone marrow affected by acute osteomyelitis?

Explanation
The classic MRI findings of osteomyelitis are a decrease in the normally high signal intensity of marrow on T1-weighted images and normal or increased signal intensity on T2-weighted images. This is the result of replacement of marrow fat by inflammatory cells and edema, which causes lower signal intensity than fat on T1-weighted images and higher signal intensity than fat on T2-weighted images. The addition of gadolinium to a T1-weighted sequence reveals increased signal intensity in the hyperemic marrow. Unger E, Moldofsky P, Gatenby R, et al: Diagnosis of osteomyelitis by MR imaging. Am J Roentgenol 1988;150:605-610. Dormans JP, Drummond DS: Pediatric hematogenous osteomyelitis: New trends in presentation, diagnosis and treatment. J Am Acad Orthop Surg 1994;2:333-341.
Question 476
High Yield
A 14-year-old boy has medial ankle pain, progressive unilateral flatfoot deformity, and pain with most activities of daily living. He denies any recent injury. His parents recall that at age 7 years he sustained an injury that was treated as a sprain. Examination reveals valgus deformity with painless, unrestricted passive motion of the ankle. He has grossly equal limb lengths. A radiograph of the affected ankle is shown in Figure 48a, and the contralateral ankle is shown in Figure 48b. Management should consist of


Explanation
Angular deformities of the ankle can occur following physeal injury. While an orthosis may be beneficial, the deformity is at the level of the ankle rather than the hindfoot. An epiphysiodesis or physeal bar resection would not be indicated as the growth plates are closed. Correction of the angular deformity should level the ankle joint and normalize the weight-bearing stresses on the ankle. This is most easily achieved with a closing wedge distal tibial osteotomy with or without concomitant osteotomy of the fibula. Thompson DM, Calhoun JH: Advanced techniques in foot and ankle reconstruction. Foot Ankle Clin 2000;5:417-442. Ting AJ, Tarr RR, Sarmiento A, Wagner K, Resnick C: The role of subtalar motion and ankle contact pressure changes from angular deformities of the tibia. Foot Ankle 1987;7:290-299.
Question 477
High Yield
A 27-year-old woman reports the acute atraumatic onset of burning pain in her right shoulder followed a week later by significant weakness and the inability to abduct her shoulder. One week prior to this incident she had recovered from a flu-like syndrome. Examination reveals full passive motion of the shoulder and the inability to actively raise the arm. Sensation in the right upper extremity is normal. Cervical spine examination is normal. Radiographs of the shoulder and cervical spine are normal. What is the most likely diagnosis?
Explanation
The patient has symptoms and examination findings of acute brachial neuritis which is often a diagnosis of exclusion. The recent viral flu-like symptoms have shown a correlation with the development of this disorder. The acute, severe shoulder weakness excludes calcific tendinitis, impingement, and poliomyelitis. A normal cervical spine examination makes cervical disk disease unlikely. Turner JW, Parsonage MJ: Neuralgic amyotrophy (paralytic brachial neuritis). Lancet 1957;2:209-212.
Question 478
High Yield
A toddler is brought in by his parents for evaluation of gait problems. Birth history and neurologic examination are unremarkable. After evaluating femoral torsion, tibial torsion, and foot contour, the diagnosis is excessive internal tibial torsion. The parents should be advised to expect which of the following outcomes?
Explanation
Excessive internal tibial torsion is a common cause of intoeing in toddlers. In most children, this resolves spontaneously by 3 to 4 years of age. Intoeing in elementary age children is usually the result of excessive femoral anteversion. Studies have shown that active intervention (casting, splinting, and shoe modifications) has no demonstrable effect on the natural history or resolution of tibial torsion. Surgery is rarely indicated in adolescents with severe internal tibial torsion that has not resolved and is resulting in cosmetic and functional problems. Canale ST, Beaty JH: Operative Pediatric Orthopaedics. St Louis, MO, Mosby Year Book, 1991, pp 357-385.
Question 479
High Yield
A 68-year-old woman with serologically proven rheumatoid arthritis underwent an open synovectomy and radial head resection 10 years ago. She now has severe pain that has failed to respond to nonsurgical management. Examination reveals a flexion arc of greater than 90 degrees. Radiographs are shown in Figures 15a and 15b. What is the most appropriate management?


Explanation
The radiographs reveal severe arthritic changes with no joint space, and the AP view shows a progressive malalignment secondary to the radial head resection. A prosthetic arthroplasty is indicated given the severe arthritis (Larsen grade III). Unconstrained arthroplasties have not performed as well as semiconstrained arthroplasties after previous radial head resections. However, both types of arthroplasties performed better in native elbows. Synovectomies should be reserved for less advanced disease states. Whaley A, Morrey BF, Adams R: Total elbow arthroplasty after previous resection of the radial head and synovectomy. J Bone Joint Surg Br 2005;87:47-53. Maenpaa HM, Kuusela PP, Kaarela KK, et al: Reoperation rate after elbow synovectomy in rheumatoid arthritis. J Shoulder Elbow Surg 2003;12:480-483.
Question 480
High Yield
A 20-year-old football player sustains a dorsiflexion external rotation injury to his right ankle. During sideline evaluation, which of the following findings best indicates a syndesmosis ankle sprain without diastasis?
Explanation
The inability to single leg hop is considered the best indicator of a syndesmosis ankle sprain without diastasis. Tenderness along the syndesmosis, the deltoid, or over the anterior talofibular ligament or anterior distal tibia/fibula may present later, following the initial injury. The squeeze test and tenderness with dorsiflexion and external rotation may be positive but often are not present initially. The best determinant for prediction of return to play is the amount of tenderness along the syndesmosis, measured from the distal fibula up the syndesmosis. Nussbaum ED, Hosea TM, et al: Prospective evaluation of syndesmosis ankle sprains without diastasis. Am J Sports Med 2001;29:31-35. Miller CD, Shelton WR, Barrett GR, et al: Deltoid and syndesmosis ligament injury of the ankle without fracture. Am J Sports Med 1985;23:746-750.
Question 481
High Yield
A 28-year-old professional dancer reports a 3-month history of progressive pain in the posterior aspect of the left ankle. Her symptoms are worse when she assumes the en pointe position. Examination reveals tenderness to palpation at the posterolateral aspect of the ankle posterior to the peroneal tendons which is made worse with passive plantar flexion. There is no nodularity, fluctuance, or tenderness of the Achilles tendon. The neurovascular examination is unremarkable. A lateral radiograph and MRI scan are shown in Figures 16a and 16b, respectively. Management should consist of

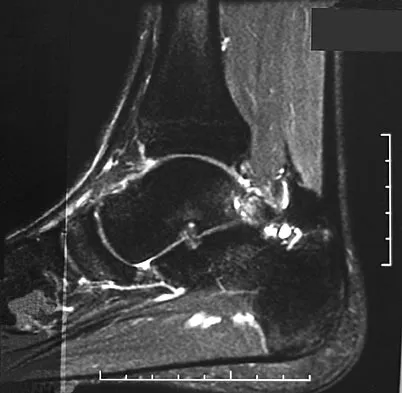
Explanation
The imaging studies reveal findings typical of the os trigonum syndrome. This condition results from inflammation between the os trigonum and the adjacent talus. The symptoms of posterior ankle pain are exacerbated by plantar flexion, which stresses the fibrous union between these two bones. Definitive management of the high-level athlete involves excision of the os trigonum from a medial approach, although arthroscopic excision has also been described. The os trigonum is not an intra-articular structure; therefore, ankle arthroscopy is neither diagnostic nor therapeutic. Abramowitz Y, Wollstein R, Barzilay Y, et al: Outcome of resection of a symptomatic os trigonum. J Bone Joint Surg Am 2003;85:1051-1057. Mouhsine E, Crevoisier X, Leyvraz P, et al: Post-traumatic overload or acute syndrome of the os trigonum: A possible cause of posterior ankle impingement. Knee Surg Sports Traumatol Arthrosc 2004;12:250-253.
Question 482
High Yield
Figure 11 shows the radiograph of an 18-year-old soccer player who reports recurrent lateral foot pain after sustaining an inversion injury. History reveals that 6 months ago he had been treated in a non-weight-bearing cast for a fifth metatarsal fracture. Management should consist of

Explanation
Fractures in this area of the fifth metatarsal have a high incidence of delayed union, nonunion, and recurrence with nonsurgical management. In an acute fracture, prolonged casting in a non-weight-bearing cast may allow for healing; however, in the presence of prolonged symptoms, recurrent fracture, and intermedullary sclerosis, surgical treatment is preferred. Surgery most commonly consists of intermedullary fixation or medullary curettage and bone grafting, followed by application of a non-weight-bearing cast. Torg JS, Balduini FC, Zelko RR, Pavlov H, Peff TC, Das M: Fractures of the base of the fifth metatarsal distal to the tuberosity: Classification and guidelines for nonsurgical and surgical management. J Bone Joint Surg Am 1984;66:209-214.
Question 483
High Yield
A 7-year-old child is unresponsive, tachycardic, and has a systolic blood pressure of 50 mm Hg after being struck by a car. The patient is intubated and venous access is obtained. The secondary survey reveals an unstable pelvis. Despite adequate resuscitation, the patient continues to be hemodynamically unstable. What is the best course of action?
Explanation
The patient is hemodynamically unstable, so any treatment should be aimed at stabilization. Airway, breathing, and circulation are the most important areas to control initially; the patient has been intubated and has adequate venous access. Despite fluid resuscitation, the child remains hypotensive, indicating continued blood loss. With an unstable pelvic fracture there can be significant hemorrhage. Decreasing the pelvic volume can decrease blood loss related to the pelvic fracture. This can be done in the emergency department by applying a pelvic sling. Other means of decreasing pelvic volume include a pelvic clamp, a simple anterior frame pelvic external fixator, or a simple sheet tied around the pelvis. These maneuvers may stabilize the patient so that further evaluation and treatment can be undertaken. All of the other choices will delay stabilization and should be postponed until the patient is stabilized. Torode I, Zieg D: Pelvic fractures in children. J Pediatr Orthop 1985;5:76-84. Eichelberger MR, Randolph JG: Pediatric trauma-initial resuscitation, in Moore EE, Eisman B, Van Way CE (eds): Critical Decisions in Trauma. St Louis, MO, CV Mosby, 1984, p 344.
Question 484
High Yield
A 10-year-old child reports acute leg pain after wrestling with his brother. AP and lateral radiographs are shown in Figures 21a and 21b. What is the best course of action?


Explanation
The radiographs show an eccentric metaphyseal lesion with a well-defined reactive rim of bone that is consistent with a nonossifying fibroma. Pathologic fractures through benign lesions should be treated as appropriate for the fracture, allowing the fracture to heal. Biopsy is not needed when the radiographic diagnosis is benign. MRI, in the presence of a fracture, is not particularly helpful because of the hematoma. If radiographic findings reveal that the lesion appears aggressive, a biopsy should be performed, obtaining tissue away from the fracture site. Marks KE, Bauer TW: Fibrous tumors of bone. Orthop Clin North Am 1989;20:377.
Question 485
High Yield
A 42-year-old athletic trainer has a persistent popping sensation about the lateral ankle associated with weakness and pain following a remote injury. Deficiency in what structure directly leads to this pathology?

Explanation
The patient has instability of the peroneal tendon. The superior peroneal retinaculum is the primary retaining structure preventing peroneal subluxation. It is a thickening of fascia that arises off the posterior margin of the distal 1 to 2 cm of the fibula and runs posteriorly to blend with the Achilles tendon sheath. The inferior peroneal retinaculum attaches to the peroneal tubercle of the calcaneus and is not involved in this pathology. A deficient groove in the posterior distal fibula may also be a contributing factor in the development of the condition.
Question 486
High Yield
A 43-year-old man reports a 3-year history of progressively worsening pain in the first metatarsophalangeal joint that is aggravated by activity. Larger shoes, intra-articular corticosteroid injections, and a Morton's extension pedorthic have failed to provide relief. Motion is limited to 10 degrees of dorsiflexion, and the "grind test" is positive. An AP radiograph is shown in Figure 39. What is the most appropriate surgical treatment?

Explanation
Stage III hallux rigidus comprises end-stage degenerative arthritis with loss of cartilage from the phalanx and metatarsal. Therefore, cheilectomy, osteotomy, and resection arthroplasty are inadequate. Resection arthroplasty results in diminished propulsion and transfer metatarsalgia. Resurfacing implant hemiarthroplasty remains unproven for earlier stages of hallux rigidus, but is not appropriate when there is cartilage loss from the base of the proximal phalanx. First metatarsophalangeal arthrodesis has proven to be a very reliable and functional treatment of end-stage hallux rigidus. Gibson JN, Thomson CE: Arthrodesis or total replacement arthroplasty for hallux rigidus: A randomized controlled trial. Foot Ankle Int 2005;26:680-690.
Question 487
High Yield
An 18-year-old woman sustains a twisting injury of the knee while skiing. Figures 7a and 7b show the radiograph and coronal MRI scan of the knee. In addition to the injury shown, what is the most likely associated injury?


Explanation
The MRI scan shows a Segond fracture, which is a small avulsion of the lateral joint capsule from the anterolateral aspect of the proximal tibia. It is almost always associated with anterior cruciate ligament rupture and often with a tear of either the medial or lateral meniscus. Goldman AB, Pavlov H, Rubenstein D: The Segond fracture of the proximal tibia: A small avulsion that reflects major ligamentous damage. Am J Roentgenol 1988;151:1163-1167. Sanders TG, Miller MD: A systematic approach to magnetic resonance imaging interpretation of sports medicine injuries of the knee. Am J Sports Med 2005;33:131-148.
Question 488
High Yield
During total shoulder replacement for rheumatoid arthritis, fracture of the humeral shaft occurs. An intraoperative radiograph shows a displaced short oblique fracture at the tip of the prosthesis. At this point, the surgeon should

Explanation
The risk of intraoperative fracture in osteopenic rheumatoid bone is significant. Fractures may occur with dislocation of the head and canal reaming, especially while extending and externally rotating the shoulder. If the fracture occurs at the distal tip of the prosthesis, the use of a long-stemmed prosthesis to bypass the fracture site and supplementation with wire cables has been reported with good results. Wright TW, Cofield RH: Humeral fractures after shoulder arthroplasty. J Bone Joint Surg Am 1995;77:1340-1346. Boyd AD Jr, Thornhill TS, Barnes CL: Fractures adjacent to humeral protheses. J Bone Joint Surg Am 1992;74:1498-1504.
Question 489
High Yield
A 27-year-old man has had pain in the right index finger for the past 9 months. The pain is completely relieved with ibuprofen. An AP radiograph and CT scan are shown in Figures 80a and 80b. What is the most likely diagnosis?

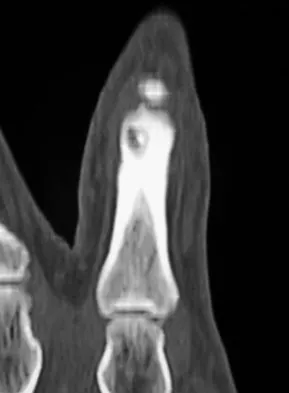
Explanation
Osteoid osteoma is a round or oval, well-circumscribed lesion with a radiolucent nidus. A small area of calcification may be present within the center of the nidus. The radiolucent nidus is surrounded by a thick rim of sclerotic bone. These diagnostic features are frequently better seen on CT. An increase in cyclooxygenase activity has been demonstrated within osteoid osteomas, which may explain why aspirin and other nonsteroidal anti-inflammatory drugs classically relieve the pain associated with these lesions. Kneisl JS, Simon MA: Medical management compared with operative treatment for osteoid-osteoma. J Bone Joint Surg Am 1992;74:179-185.
Question 490
High Yield
Figures 35a and 35b show the radiographs of a patient who underwent debridement of a chronically infected, fully constrained knee prosthesis and now reports pain and instability despite bracing. History reveals that the patient has had no drainage since undergoing the last debridement 6 months ago. A C-reactive protein level and aspiration are negative for infection. Treatment should now consist of


Explanation
The radiographs show a significant loss of the proximal anterior tibial cortex, consistent with an extensively damaged or deficient extensor mechanism. Such a deficit precludes insertion of another knee arthroplasty. Arthrodesis is the treatment of choice for this patient and is indicated for loss of the extensor mechanism and knee instability. A recent report on arthrodesis following removal of an infected prosthesis showed a union rate of 91% using a short intramedullary nail. Insertion of an antibiotic-impregnated PMMA spacer is not indicated because the rationale for using a spacer is to maintain a space for reinsertion of another prosthesis. Reconstruction of the extensor mechanism would not address the loss of the joint. Amputation is the final treatment option if the arthrodesis fails. Rand JA: Alternatives to reimplantation for salvage of the total knee arthroplasty complicated by infection. J Bone Joint Surg Am 1993;75:282-289. Lai KA, Shen WJ, Yang CY: Arthrodesis with a short Huckstep nail as a salvage procedure for failed total knee arthroplasty. J Bone Joint Surg Am 1998;80:380-388.
Question 491
High Yield
Which of the following aids in correction of patellar tracking after total knee arthroplasty (TKA)?

Explanation
Correct patellofemoral tracking has proven to be a crucial aspect in TKA because a large percent of problems after TKA are related to the patellofemoral articulation. External rotation of the femoral and tibial components has been shown to aid in tracking. Likewise, medialization of the patellar button aids in patellar tracking and prevention of lateral subluxations and dislocations. Attention to the distal femoral cut is critical in maintaining the joint line and preventing patella baja or alta. Tibial sizing, however, is not directly related to patellar tracking after TKA. Callaghan JJ, Rosenberg AG, Rubash HE, et al (eds): The Adult Knee. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 1245-1258.
Question 492
High Yield
Figure 12 shows the lumbar CT scan of a 24-year-old man who was injured in a snowmobile accident. What is the mechanism of injury?

Explanation
A true compression fracture is a single-column injury that does not create canal compromise. A burst fracture is a two- or three-column injury that disrupts the middle column and thereby narrows the spinal canal. This patient has a burst fracture. The mechanism of injury is usually vertical compression or flexion compression. Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 197-217.
Question 493
High Yield
Patients who have osteonecrosis of the humeral head and who have the best prognosis are those with which of the following conditions?
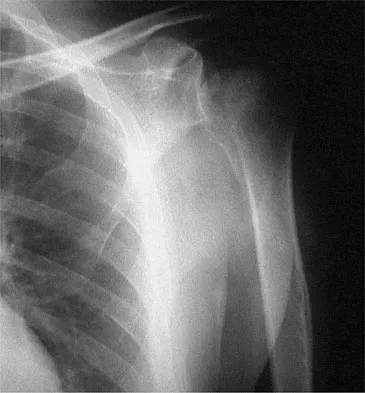
Explanation
The natural history of nontraumatic osteonecrosis varies greatly, so it is difficult to predict which patients will have severe arthrosis develop. Patients with sickle cell disease tend to have the most benign course. The most commonly reported cause of nontraumatic osteonecrosis is corticosteroid therapy. Fortunately, the incidence of osteonecrosis among patients treated with long-term systemic corticosteroids has fallen from more than 25% to less than 5% in recent years, owning to judicious steroid use and dosing. The interval between corticosteroid administration and the onset of shoulder symptoms is also variable, ranging from 6 to 18 months in one large series. This is comparable to the interval leading up to the onset of hip symptoms, which ranges from 6 months to 3 years or longer. The incidence of humeral head involvement has not been shown to vary with the underlying indication for steroid use. Hasan SS, Romeo AA: Nontraumatic osteonecrosis of the humeral head. J Shoulder Elbow Surg 2002;11:281-298.
Question 494
High Yield
A 14-year-old boy reports progressive right wrist pain. Radiographs are shown in Figure 3a, and a photomicrograph is shown in Figure 3b. What is the most likely diagnosis?

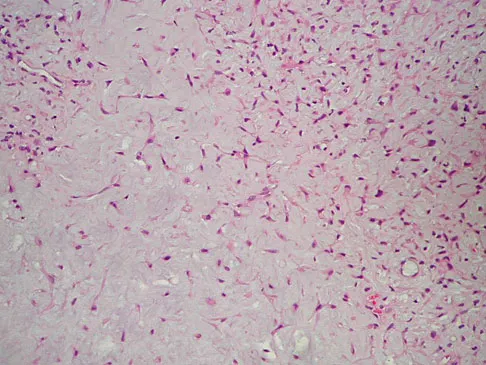
Explanation
The radiographs show a benign-appearing, well-defined lytic lesion with a thin rim of surrounding reactive bone. The photomicrograph shows spindle cells with a myxoid cartilaginous matrix. These findings are diagnostic of chondromyxoid fibroma. This is a rare, benign tumor that usually causes pain and can be locally aggressive. Lersundi A, Mankin HJ, Mourikis A, et al: Chondromyxoid fibroma: A rarely encountered and puzzling tumor. Clin Orthop Relat Res 2005;439:171-175.
Question 495
High Yield
Which of the following best describes the course of the median nerve at the elbow?
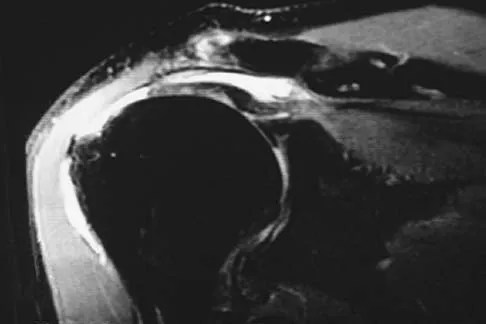
Explanation
The median nerve courses superficial to the ulnar artery, deep to the fibrous arch of the superficialis muscle, and deep to the superficial head of the pronator teres muscle. The median nerve lies within the interval between the flexor digitorum superficialis muscle and the flexor digitorium muscle as it progresses toward the wrist. Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics, ed 2. Philadelphia, PA, Lippincott-Raven, 1994, pp 118-131.
Question 496
High Yield
A 17-year-old boy who fell on a pitchfork in a barn 1 day ago now has a painful, swollen forearm. Examination reveals erythema, exquisite tenderness, and crepitus to palpation of the forearm. He has a pulse rate of 110/min and a blood pressure of 80/60 mm Hg. Radiographs show subcutaneous air and no fractures. Gram stain of wound drainage reveals a gram-positive bacillus. The next most appropriate step in management should consist of
Explanation
The successful treatment of necrotizing soft-tissue infections such as clostridial myonecrosis depends on prompt recognition and aggressive surgical debridement of all involved muscle, fascia, and soft tissue, resecting to a clearly normal healthy, viable margin. The effective antibiotic regimen for clostridial infection is high-dose penicillin; however, necrotizing infections are frequently polymicrobial so initially broad-spectrum antibiotics are indicated. Hyperbaric oxygen therapy may be used as an adjunct to surgical treatment but is insufficient as a primary therapy. Prolonged application of tourniquets and wound closure should be avoided. Pellegrini VD, Evarts CM: Complications, in Rockwood CA Jr, Green DP (eds): Fractures in Adults, ed 3. Philadelphia, PA, JB Lippincott, 1991, pp 365-370. Gerding DN, Peterson LR: Infections caused by anaerobic bacteria, in Shulman ST, Phair JP, Peterson LR, Warren JR (eds): Infectious Diseases, ed 5. Philadelphia, PA, WB Saunders, 1997, pp 416-417.
Question 497
High Yield
Figures 32a and 32b show the radiographs of an active 13-year-old boy who has persistent left thigh pain and a limp despite a trial of protected weight bearing. Management should consist of


Explanation
The plain radiographs show an eccentric metaphyseal lesion involving a long bone in a skeletally immature patient. The lesion is longer than it is wide, with distinctly lobular outer edges that are sclerotic. These findings are characteristic of a nonossifying fibroma. Small asymptomatic lesions may be followed clinically. Larger lesions that occupy greater than two thirds of the width of the shaft and are located in areas of high mechanical stress such as the femur are more prone to fracture than smaller lesions. Pain is often a sign of impending fracture or the presence of a small fracture that may not be apparent on radiographs. The natural history of the lesion is to resolve over a period of years. The procedure that would allow the patient to return to contact sports is curettage and bone grafting. Intralesional steroid injection has been advocated in the treatment of unicameral bone cysts and eosinophilic granuloma but not nonossifying fibromas. En block resection is not indicated for a benign lesion. Low-dose radiation therapy has been used for eosinophilic granuloma but not for nonossifying fibromas. Walker RN, Green NE, Spindler KP: Stress fractures in skeletally immature patients. J Pediatr Orthop 1996;16:578-584.
Question 498
High Yield
A 20-year-old male lacrosse player sustains an anterior dislocation of the shoulder. He is extremely concerned about recurrent dislocations. Which of the following treatments has been shown to reduce the risk of recurrent dislocation?
Explanation
Recent evidence has shown that the position of immobilization of the shoulder after a dislocation influences the reduction of the Bankart lesion. In an MRI study in patients who sustained an anterior dislocation, the Bankart lesion was reduced to the glenoid anatomically with the arm in 30 degrees of external rotation. Subsequently, a clinical follow-up study has shown a reduction in recurrence rates when the arm is immobilized in external rotation compared to internal rotation. Itoi E, Hatakeyama Y, Kido T, et al: A new method of immobilization after traumatic anterior dislocation of the shoulder: A preliminary study. J Shoulder Elbow Surg 2003;12:413-415.
Question 499
High Yield
Figures 8a through 8d show the radiographs and CT scans of a 14-year-old girl who has a painful, rigid planovalgus foot. Management consisting of arch supports and anti-inflammatory drugs failed to provide relief. A below-knee walking cast resulted in pain resolution, but she now reports that the pain has recurred. Management should now consist of



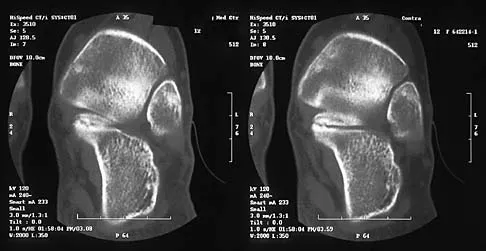
Explanation
Tarsal coalitions commonly present in the preadolescent age group as a rigid, planovalgus foot. Small coalitions of the calcaneonavicular joint or the middle facet of the talocalcaneal joint can be excised with interposition of fat or muscle tissue. Isolated calcaneocuboid joint coalitions are very rare. This patient has an associated large talocalcaneal coalition; therefore, resection is contraindicated. Surgery is warranted after failure of nonsurgical management, and because of the involvement of two joints, the only viable option for the severely symptomatic foot is triple arthrodesis. Vincent KA: Tarsal coalition and painful flatfoot. J Am Acad Orthop Surg 1998;6:274-281.
Question 500
High Yield
A 58-year-old woman has had a slowly progressing mass over the distal interphalangeal (DIP) joint of her dominant hand with a worsening deformity of her nail. She has no significant medical history but underwent bilateral knee arthroplasties 1 year ago. Radiographs reveal a small osteophyte at the DIP joint dorsally. A clinical photograph and a biopsy specimen are shown in Figures 76a and 76b. What is the most likely diagnosis?
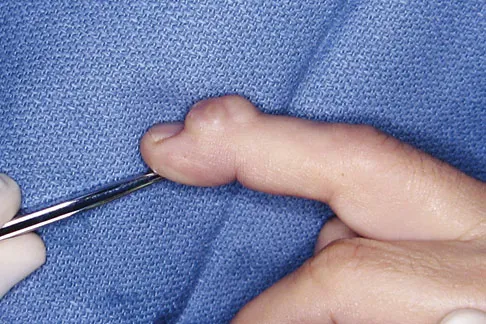

Explanation
A mucous cyst is thought to be a ganglion arising from the DIP joint in patients with osteoarthritis. They are frequently associated with nail deformities. Treatment involves removal of the cyst with debridement of DIP joint osteophytes. Fritz GR, Stern PJ, Dickey M: Complications following mucous cyst excision. J Hand Surg Br 1997;22:222-225.
