HY 2026
00:00
Start Quiz
Question 301
High Yield
An AP radiograph of the pelvis is shown in Figure 4. What muscle attaches to the avulsed fragment of bone identified by the arrow?

Explanation
The radiograph reveals an avulsion of the ischial apophysis, most likely the result of violent contraction of the attached hamstring tendons (semimembranosus, semitendinosus, and long head of the biceps femoris). The short head of the biceps femoris arises from the linea aspera on the posterior femur. The pectineus and adductor longus attach to the pubic portion of the pelvis. The piriformis runs from the sacrum to the femur. Woodburne RT (ed): Essentials of Human Anatomy. New York, NY, Oxford University Press, 1978, pp 542-545.
Question 302
High Yield
In hip arthroplasty, the location of the medial femoral circumflex artery is best described as
Explanation
The obturator artery lies closest to the transverse acetabular ligament. The femoral artery is closest to the anterior rim of the acetabulum. No named vessel lies within the substance of the gluteus minimus or superior to the piriformis tendon. The medial femoral circumflex artery lies medial or deep to the quadratus femoris muscle. Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach, ed 1. Philadelphia, PA, JB Lippincott, 1984, Figure 7-53, p 346.
Question 303
High Yield
Which of the following ligaments is most commonly involved in posterolateral rotatory instability of the elbow?
Explanation
Recurrent posterolateral rotatory instability of the elbow is difficult to diagnose. Such instability can be demonstrated only by the lateral pivot-shift test. The cause for this condition is laxity of the ulnar part of the lateral collateral ligament, which allows a transient rotatory subluxation of the ulnohumeral joint and a secondary dislocation of the radiohumeral joint. The annular ligament remains intact, so the radioulnar joint does not dislocate. Treatment consists of surgical reconstruction of the lax ulnar part of the lateral collateral ligament. The anterior band is the most important part of the medial collateral which is lax in valgus instability of the elbow. Morrey BF: Acute and chronic instability of the elbow. J Am Acad Orthop Surg 1996;4:117-128.
Question 304
High Yield
Figure 19 shows the radiograph of a 45-year-old woman who has a painful nonunion. Treatment should consist of

Explanation
The radiograph reveals a reverse obliquely subtrochanteric/intertrochanteric fracture. Open reduction and internal fixation should be accomplished with a 95-degree fixed angle device. An intramedullary nail with screw fixation into the head is another possible technique. Either method should correct the varus deformity. Exchange of a high-angled screw and plate device to a longer side plate and bone grafting does not afford any improvement in the mechanical stability. Hardware removal and retrograde intramedullary nailing is not indicated for this level of a proximal femoral injury. Placement of an implantable bone stimulator may change local biologic factors but would not enhance mechanical stability. The patient's femoral head is intact without signs of collapse; therefore, hardware removal, proximal femoral resection, and total hip arthroplasty are not warranted. Haidukewych GJ, Israel TA, Berry DJ: Reverse obliquity fractures of the intertrochanteric region of the femur. J Bone Joint Surg Am 2001;83:643-650.
Question 305
High Yield
Patients with tarsal tunnel syndrome are most likely to obtain a favorable outcome from decompression of the posterior tibial nerve if which of the following conditions is present?
Explanation
In one series, only 44% of patients demonstrated good results from tarsal tunnel decompression if they did not have a mass in the tarsal tunnel. Conditions that produce a traction neuropathy of the posterior tibial nerve are unlikely to respond to neurolysis. The most favorable condition associated with a good response to decompression is when a compressing anatomic structure can be removed from the tarsal tunnel. Frey C, Kerr R: Magnetic resonance imaging and the evaluation of tarsal tunnel syndrome. Foot Ankle 1993;14:159-164. Garrett AL: Poliomyelitis, in Nickel VL (ed): Orthopaedic Rehabilitation. New York, NY, Churchill Livingston, 1982, pp 449-458.
Question 306
High Yield
In a patient with a C5-6 herniation, the most likely sensory deficit will be in the
Explanation
A C5-6 herniation compresses the C6 root, which innervates the radial forearm, thumb, and index finger. The lateral shoulder is innervated by C5. The dorsal forearm and the middle finger typically are innervated by C7. The ulnar forearm, ring finger, and little finger are innervated by C8. There is no specific nerve associated with the volar forearm and palm.
Question 307
High Yield
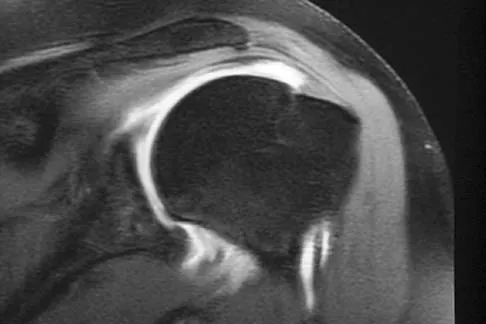
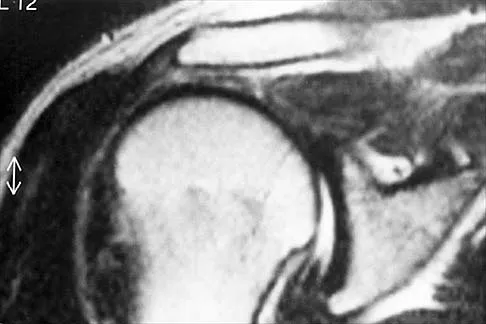
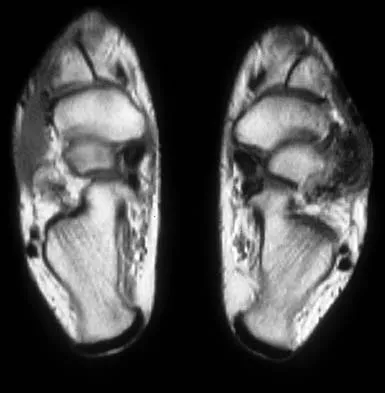
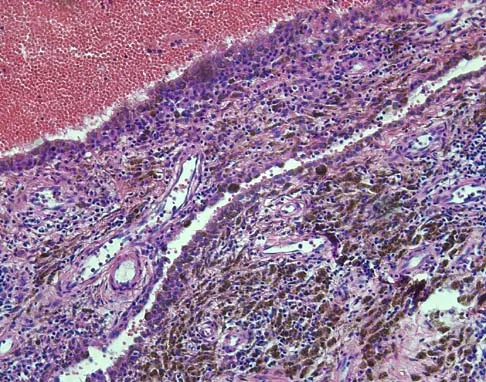
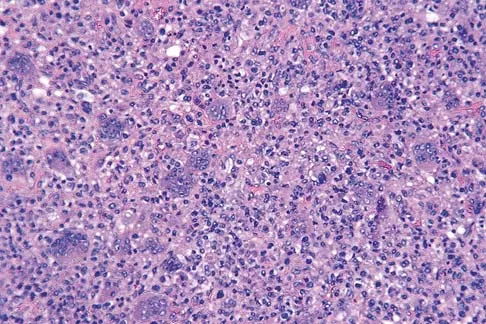
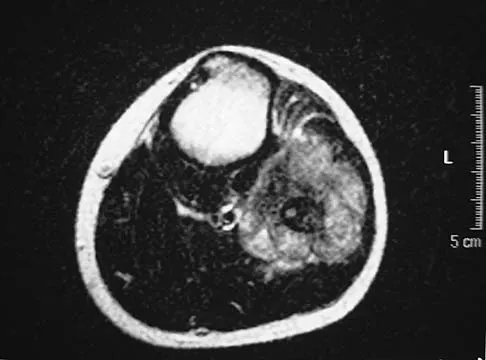
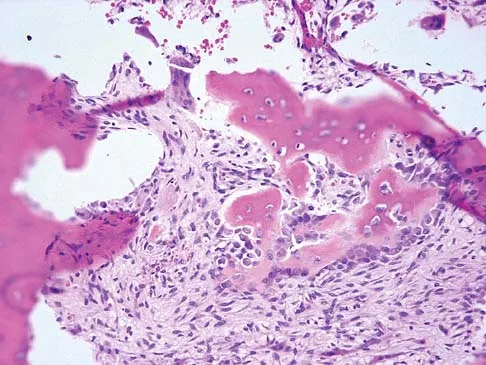
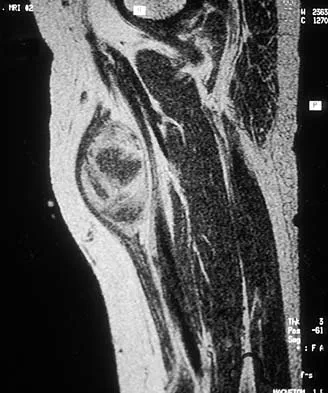
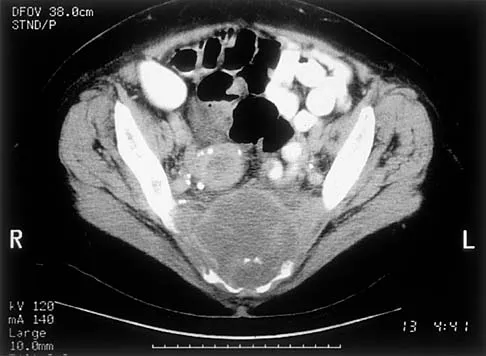
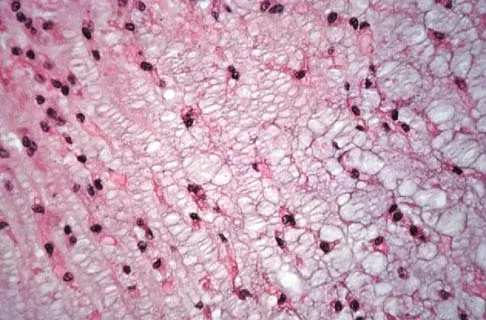
A 16-year-old girl has a painful foot mass. A radiograph, MRI scan, and biopsy specimens are shown in Figures 35a through 35d. What is the most likely diagnosis?

Explanation
Synovial sarcoma should always be considered in the differential diagnosis of a foot mass; however, the histopathology shows a typical example of PVNS, with hemosiderin, giant cells, and synovium. Synovial chondromatosis would have metaplastic cartilage in the synovium. The radiograph shows subtle erosion of the lateral cortex of the cuboid, and the MRI scan shows a soft-tissue mass. Ghert MA, Scully SP, Harrelson JM: Pigmented villonodular synovitis of the foot and ankle: A review of six cases. Foot Ankle Int 1999;20:326-330. Jones BC, Sundaram M, Kransdorf MJ: Synovial sarcoma: MR imaging findings in 34 patients. Am J Roentgenol 1993;161:827-830. Sartoris DJ, Resnick D: Magnetic resonance imaging of pediatric foot and ankle disorders. J Foot Surg 1990;29:489-494.
Question 308
High Yield
The rate of complications after in situ pinning of a chronic slipped capital femoral epiphysis is highest with placement of the screw in what quadrant of the femoral head?
Explanation
The rate of complications increases as the pin moves farther from the ideal position, which is the center of the head. This is the strongest argument for the use of a single pin. The highest rate of complications, primarily osteonecrosis and pin penetration, is associated with pin placement in the anterior superior quadrant. Raney EM, Ogden JA: Slipped capital femoral epiphysis. Current Ortho 1995;9:111-116.
Question 309
High Yield
A 28-year-old man sustained a fracture-dislocation of T8 in a motor vehicle accident 1 week ago. The injury resulted in complete paraplegia. Management should consist of

Explanation
With a complete injury in the thoracic spinal cord, the likelihood of neurologic recovery is small. If possible, treatment should be planned to allow rapid mobilization and rehabilitation without the use of braces and their associated skin problems. The use of long segment fixation provides for rapid mobilization without having to use braces postoperatively. The use of steroid protocol is controversial and should be considered only if it can be started within 8 hours of the injury. Laminectomy is contraindicated because it will increase instability.
Question 310
High Yield
A 68-year-old man with no significant medical history underwent a total knee arthroplasty 4 years ago. A radiograph is shown in Figure 55. He reports that he had no problems with the knee until 6 weeks ago when he noted the gradual onset of pain following a colonoscopy. Examination reveals a painful, swollen knee. Knee aspiration reveals a WBC count of 40,000/mm3. Management should consist of

Explanation
The treatment of choice for a late hematogenous infection is two-stage resection arthroplasty and reimplantation, with parenteral antibiotics prior to reimplantation. This is particularly true when septic loosening has occurred as in this patient. Open irrigation and debridement with polyethylene exchange has been used successfully when the duration of symptoms is 3 weeks or less. Long-term suppressive antibiotics are most commonly used when the patient's medical condition precludes further surgery. Delayed reimplantation has been shown to be superior to immediate reimplantation in multiple studies. Little data support the use of arthroscopic irrigation and debridement. Swanson KC, Windsor RE: Diagnosis of infection after total knee arthroplasty, in Callaghan JJ, Rosenberg AG, Rubash HE, et al (eds): The Adult Knee. Philadelphia, PA, JB Lippincott, 2003, vol 2, pp 1485-1491.
Question 311
High Yield
A 26-year-old rugby player injured his foot when tackled from behind. Radiographs are seen in Figures 35a through 35c. What is the most appropriate treatment?



Explanation
The patient has a ligamentous Lisfranc injury. Diastasis seen between the bases of the second metatarsal and medial cuneiform is pathognomonic for a rupture of the Lisfranc's ligament. This injury is best treated surgically with either open reduction and internal fixation or possibly closed manipulation and percutaneous screw fixation if anatomic alignment can be achieved closed. Pin fixation has been shown to be inferior to screw fixation due to the length of time that fixation is required for adequate ligament healing. Chiodo CP, Myerson MS: Developments and advances in the diagnosis and treatment of injuries of the tarsometatarsal joint. Orthop Clin North Am 2001;32:11-20.
Question 312
High Yield
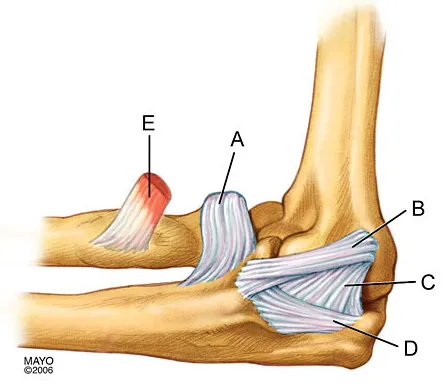
In Figure 2, which of the following structures is the primary stabilizer in preventing valgus instability of the elbow?
Explanation
The anterior bundle of the medial collateral ligament is the prime stabilizer of the medial aspect of the elbow and is indicated by "B" in the figure. When intact, this anterior bundle of the medial collateral ligament is a restraint to valgus instability of the elbow. The posterior bundle is regarded as a secondary stabilizer of the medial elbow (C). The transverse bundle (D), annular ligament (A), and biceps tendon (E) do not play a role in valgus stability of the elbow. Jobe F, Elattrache N: Diagnosis and treatment of ulnar collateral ligament injuries in athletes, in Morrey B (ed): The Elbow and Its Disorders. Philadelphia, PA, WB Saunders, 1993, p 566.
Question 313
High Yield
The Lisfranc ligament connects the base of the

Explanation
The Lisfranc ligament arises from the lateral surface of the first (medial) cuneiform and is directed obliquely outward and slightly downward to insert on the medial surface of the second metatarsal base. It is the strongest of the tarsometatarsal interosseous ligaments. Sarrafian SK: Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993.
Question 314
High Yield
In the initial evaluation of acute low back pain (duration of less than 4 weeks), plain radiographs are recommended in which of the following situations?

Explanation
Prolonged use of steroids is associated with compression fractures with minimal trauma. Indications for radiography with acute low back pain include possible tumor, fracture, infection, or cauda equina syndrome. Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, Appendix A15.
Question 315
High Yield
A 42-year-old woman has cervical stenosis and radicular deficits at the C5-6 and C6-7 levels. History reveals that she has smoked one pack of cigarettes a day for 25 years. Because nonsurgical management has failed to provide relief, she is now seeking surgical treatment. After preoperative counseling, it becomes clear that she is not likely to stop smoking. Which of the following surgical procedures should be used?
Explanation
In a review of 190 anterior cervical fusions, Hilibrand and associates reported that only 20 of 40 patients who smoked had solid fusion at all levels, whereas 64 of 91 nonsmokers had solid fusions at all levels when treated with multilevel interbody technique (Smith-Robinson). When fused with strut grafts, 14 of 15 smokers and 41 of 44 nonsmokers had solid fusions with a fusion rate of 93% in the same series. Multilevel allografts have a lower fusion rate than autografts, and diskectomy without fusion has an increased rate of residual neck pain. Hilibrand AS, Fye MA, Emery SE, et al: Impact of smoking on the outcome of anterior cervical arthrodesis with interbody or strut-grafting. J Bone Joint Surg Am 2001;83:668-673.
Question 316
High Yield
What is the single most important nutritional factor affecting athletic performance?
Explanation
Maintenance of adequate hydration is the single most important factor affecting athletic performance. While carbohydrate loading may be beneficial for some endurance athletes, the consumption of carbohydrates during exercise does not appear to be beneficial for athletes engaged in events that last less than 1 hour. In general, athletes consuming a balanced diet do not need electrolyte supplementation. Maughan RJ, Noakes TD: Fluid replacement and exercise stress: A brief review of studies on fluid replacement and some guidelines for the athlete. Sports Med 1991;12:16-31.
Question 317
High Yield
Which of the following prophylactic regimens for the prevention of deep venous thrombosis after knee arthroplasty has received a grade 1A recommendation in favor of its use from the American College of Chest Physicians (ACCP) in the 2004 guidelines?
Explanation
In the 2004 ACCP guidelines, there were three prophylactic regimens that received a grade 1A favorable recommendation. These included low-molecular-weight heparin, warfarin, or fondaparinux, as long as they are used for at least 10 days. If warfarin is used, the target INR should be 2.0 to 3.0, according to the guidelines. Pneumatic compression sleeves have gained popularity in the orthopaedic community but have not received a grade 1A rating from the ACCP at this time. Use of aspirin by itself is discouraged by the ACCP.
Question 318
High Yield
Osteoporotic vertebral compression fractures are associated with

Explanation
Osteoporotic vertebral compression fractures are associated with neurologic complications in less than 1% of patients. After the initial fracture however, patients have a 20% risk of further fractures. The mortality rate of patients with vertebral fractures exceeds that of patients with hip fractures when they are followed beyond 6 months. Gass M, Dawson-Hughs B: Preventing osteoporosis-related fractures: An overview. Am J Med 2006;119:S3-S11. Lindsay R, Silverman SL, Cooper C, et al: Risk of new vertebral fracture in the year following a fracture. JAMA 2001;285:320-323.
Question 319
High Yield
A 23-year-old woman sustains an injury to her right hand after falling off her snowboard. Examination reveals that she has difficulty moving her fingers. A radiograph and a clinical photograph are shown in Figures 8a and Figure 8b. Management should consist of


Explanation
The radiograph reveals oblique fractures of the third and fourth metacarpals. The rotational component of the fracture displacement is well visualized on the clinical photograph, which shows scissoring of the middle finger over the ring finger. The fracture obliquity results in rotational deformity that cannot be adequately maintained and held by closed treatment. The treatment of choice is open reduction and internal fixation. Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC (eds): Green's Operative Hand Surgery, ed 4. Philadelphia, PA, 1999, pp 711-771. Freeland AE, Benoist LA, Melancon KP: Parallel miniature screw fixation of spiral and long oblique hand phalangeal fractures. Orthopedics 1994;17:199-200.
Question 320
High Yield
In the first dorsal compartment of the wrist, what tendon most frequently contains multiple slips?
Explanation
The first extensor compartment of the wrist typically contains a single extensor pollicis brevis tendon and the abductor pollicis longus tendon that nearly always has multiple tendon slips. The extensor pollicis brevis tendon is frequently found to be separated from the slips of the abductor pollicis longus tendon by an intracompartmental septum. During surgery, this septum must be divided to complete the release of the compartment. Jackson WT, Viegas SF, Coon TM, Stimpson KD, Frogameni AD, Simpson JM: Anatomical variations in the first extensor compartment of the wrist: A clinical and anatomical study. J Bone Joint Surg Am 1986;68:923-926.
Question 321
High Yield
The so-called high ankle sprain from an external rotation mechanism of injury typically involves injury to which of the following structures?
Explanation
Ankle sprains most commonly involve injury to the lateral collateral ligaments of the ankle (anterior talofibular, posterior talofibular, and calcaneofibular) from an inversion mechanism of injury. A different entity has been more recently described that involves an external rotation mechanism of injury that widens the ankle mortise and disrupts the anterior inferior tibiofibular ligament. Deltoid ligament and extensor retinaculum injuries do occur, although infrequently, and involve eversion and extreme plantar flexion mechanisms, respectively. Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, p 182. Kaye RA: Stabilization of ankle syndesmosis injuries with a syndesmosis screw. Foot Ankle 1989;9:290-293. Baxter DE: The Foot and Ankle in Sports. St Louis, MO, Mosby-Year Book, 1995, p 30.
Question 322
High Yield
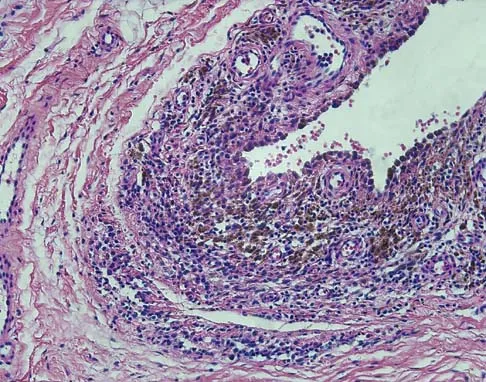
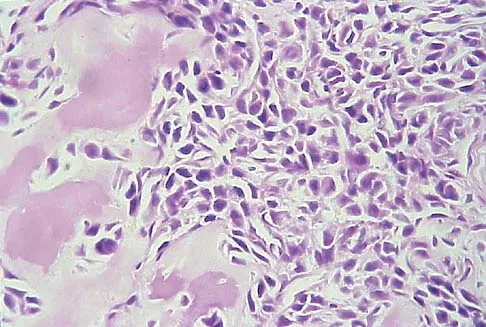
A 44-year-old man has right hip pain. Radiographs reveal a radiolucent lesion of the femoral head and neck. An MRI scan shows no extraosseous tumor extension. A histopathologic photomicrograph of the biopsy specimen is shown in Figure 5. The chance of metastatic disease developing from this lesion is approximately what percent?
Explanation
The risk of pulmonary metastasis from a benign giant cell tumor is estimated to be 5%.
Question 323
High Yield
An otherwise healthy 45-year-old woman reports the onset of severe right leg pain. Figure 20a shows an axial MRI scan of the L4-5 level, and Figure 20b shows a sagittal view with the arrow at the L4-5 level. What nerve root is the most likely source of her pain?


Explanation
The scans show a disk herniation in the far lateral region of the disk. In particular, the sagittal view shows the herniation adjacent to the exiting L4 nerve root. Disk herniations in this area that cause symptoms are more likely to compress the nerve exiting at the same level rather than the next most caudal level. McCulloch JA: Microdiscectomy, in Frymoyer JW (ed): The Adult Spine: Principles and Practice. New York, NY, Raven Press, 1991, vol 2, pp 1765-1783.
Question 324
High Yield
An 18-year-old man underwent open reduction and internal fixation of a tibial spine avulsion and a posterolateral corner repair. Two years later, he underwent lateral collateral ligament (LCL) and posterolateral corner reconstruction because of instability. Examination reveals a pronounced lateral varus knee thrust when ambulating. Varus stress in 30 degrees of flexion produces a 10-mm opening that is eliminated in extension. The Lachman's test is 2 mm with a firm end point, and the posterior drawer test is negative. Standing radiographs show widening of the lateral joint space and a 5-degree mechanical varus alignment. What is the most effective course of treatment?
Explanation
The patient has chronic posterolateral instability with a varus knee alignment; therefore, the most effective treatment is a valgus-producing HTO. A repeat soft-tissue reconstruction without correction of the varus alignment will most likely fail. An ACL reconstruction is not indicated with a normal Lachman's test. Physical therapy and bracing will have little effect. Naudie DD, Amendola A, Fowler PJ: Opening wedge high tibial osteotomy for symptomatic hyperextension-varus thrust. Am J Sports Med 2004;32:60-70.
Question 325
High Yield
A 68-year-old woman underwent a successful total right hip arthroplasty with a metal-on-metal articulation and cementless porous-coated components. Three months later, she underwent identical surgery on the left hip. Three months after surgery on the left hip, she reports groin pain on ambulation. Examination reveals significant groin discomfort with passive hip motion, particularly at the extremes of motion. Radiographs are shown in Figures 21a and 21b. Laboratory studies show an erythrocyte sedimentation rate of 35 mm/h and a C-reactive protein of 0.9. Aspiration yields scant growth of Staphylococcus epidermidis in the broth only, with no evidence of loosening on arthrography. A second aspiration yields scant growth of Staphylococcus epidermidis in the broth only. What is the most likely cause of the patient's pain?


Explanation
The difference in the clinical results combined with the laboratory findings points to infection. While there is a significant risk of false-positive findings with aspiration, the fact that two successive aspirations grew the same organism strongly suggests infection. The radiograph shows that there is more radiolucency around the left acetabular component than the right component. White RE: Evaluation of the painful total hip arthroplasty, in Callaghan JJ, Rosenberg AG, Rubash HE (eds): The Adult Hip. Philadelphia, PA, Lippincott-Raven, 1998, vol 2, pp 1377-1385.
Question 326
High Yield
A 19-year-old man was struck by a car and is seen in the emergency department with a grade IIIC open distal tibia and fibula fracture. Examination reveals that the toes are cool and dusky with a sluggish capillary refill. Angiography reveals a lesion in the posterior tibial artery amenable to repair. There is no sensation on the plantar aspect of the foot, and he is unable to flex his toes. A clinical photograph and radiograph are shown in Figures 2a and 2b. What is the next most appropriate step in management?


Explanation
In the past, loss of plantar sensation in this grade IIIC tibial fracture would have been an indication for below-knee amputation regardless of the potential for vascular repair. However the 2002 LEAP study divided 55 patients with loss of plantar sensation into two groups, the insensate amputation group and the insensate limb salvage group, with 55% of patients in the insensate salvage group regaining normal sensation 2 years after injury. Furthermore, those in the salvage group who remained insensate after 2 years had equivalent outcomes to those in the amputation group. Because of these findings, limb salvage with vascular repair and external stabilization with delayed closure is deemed appropriate treatment. Immediate intramedullary fixation is not indicated. Because ischemia, contusion, and stretch can adversely affect the tibial nerve, the additional insult of exploration of the nerve is also not advisable given the soft-tissue compromise. Bosse MJ, McCarthy ML, Jones AL, et al: The insensate foot following severe lower extremity trauma: An indication for amputation? J Bone Joint Surg Am 2005;87:2601-2608. Lange RH, Bach AW, Hansen ST Jr, et al: Open tibial fractures with associated vascular injuries: Prognosis for limb salvage. J Trauma 1985;25:203-208. Mackenzie EJ, Bosse MJ, Kellam JF, et al: Factors influencing the decision to amputate or reconstruct after high-energy lower extremity trauma. J Trauma 2002;52:641-649.
Question 327
High Yield
What is the most common MRI appearance of a malignant soft-tissue sarcoma?

Explanation
The classic MRI appearance of a soft-tissue sarcoma is a well-defined heterogeneous mass deep to the fascia. MRI has greatly enhanced our ability to identify and characterize soft-tissue masses. In many patients, MRI is diagnostic and may obviate the need for biopsy. In other patients, it may indicate with high probability that the mass is malignant and consideration for referral can be made. A common misconception is that sarcomas are infiltrative; therefore, physicians mistakenly exclude the diagnosis of a sarcoma based on a well-defined mass seen on MRI. However, sarcomas grow centrifugally with balloon-like expansion compressing surrounding normal tissue; as such, they appear well defined. Many benign soft-tissue masses such as lipomas are similarly well defined. However, MRI is especially useful in identifying fat. Lipomas appear to be homogeneous masses with fat signal characteristics on all sequences. Ill-defined soft-tissue masses include infection, trauma, and desmoid tumors. Heterogeneity is not unique to malignant tumors but is a characteristic of soft-tissue sarcomas. Bancroft LW, Peterson JJ, Kransdorf MJ, Nomikos GC, Murphey MD: Soft tissue tumors of the lower extremities. Radiol Clin North Am 2002;40:991-1011. Berquist TH, Ehman RL, King BF, et al: Value of MR imaging in differentiating benign from malignant soft-tissue masses: Study of 95 lesions. Am J Roentgenol 1990;155:1251-1255.
Question 328
High Yield
A 62-year-old patient is seen for routine follow-up after undergoing cementless total hip arthroplasty 2 years ago. The patient reports limited range of motion that severely affects daily activities. A radiograph is shown in Figure 51. Management should now consist of

Explanation
The patient has symptomatic postoperative heterotopic ossification after total hip arthroplasty. Postoperative prophylactic treatments include nonsteroidal anti-inflammatory drugs (usually indomethacin) or low-dose irradiation. The heterotopic ossification shown here is quite mature; therefore, nonsurgical management will not be successful. Surgical excision of grade III or IV heterotopic ossification should be followed with postoperative irradiation to minimize the chances of recurrence. Ayers DC, Evarts CM, Parkinson JR: The prevention of heterotopic ossification in high-risk patients by low-dose radiation therapy after total hip arthroplasty. J Bone Joint Surg Am 1986;68:1423-1430.
Question 329
High Yield
A 13-year-old girl sustained an isolated midshaft left femoral fracture in a motor vehicle accident. The fracture was treated with a rigid, antegrade intramedullary nail placed through the piriformis fossa. The fracture healed uneventfully, as shown in Figure 46a; however, at 12 months postoperatively she now reports left hip pain. A current AP radiograph and MRI scan are shown in Figures 46b and 46c. What complication occurred in this patient?



Explanation
The development of femoral head ischemic necrosis is the iatrogenically created complication in this skeletally immature patient. Placement of a rigid, antegrade intramedullary nail through the piriformis fossa is likely to damage the vascular supply to the femoral head as the vessels ascend the femoral neck on the way to the femoral head. The MRI scan reveals ischemic necrosis with early collapse of the femoral head. The joint space is preserved on the MRI scan, ruling out chondrolysis. Letts M, Jarvis J, Lawton L, et al: Complications of rigid intramedullary rodding of femoral shaft fractures in children. J Trauma 2002;52:504-516. Buckley SL: Current trends in the treatment of femoral shaft fractures in children and adolescents. Clin Orthop Relat Res 1997;338:60-73.
Question 330
High Yield
A 13-year-old patient has foot drop and lateral knee pain. AP and lateral radiographs and an MRI scan are shown in Figures 49a through 49c. A biopsy specimen is shown in Figure 49d. What is the preferred method of treatment?


Explanation
The "sunburst" radiographic appearance suggests an osteosarcoma, and the histologic findings confirm the diagnosis with malignant cells surrounded by pink osteoid. MRI scans are not particularly helpful in the diagnosis of osteosarcoma but are mandatory for surgical planning. Osteosarcomas are high-grade sarcomas that are best treated with chemotherapy and wide resection. Even though the peroneal nerve is involved, limb salvage is indicated. Survival after limb salvage is equivalent to amputation, with better function. Goorin AM, Abelson HT, Frei E: Osteosarcoma: Fifteen years later. N Engl J Med 1985;313:1637. Link MP, Goorin AM, Miser AW, et al: The effect of adjuvant chemotherapy on relapse-free survival in patients with osteosarcoma of the extremity. N Engl J Med 1986;314:1600.
Question 331
High Yield
Which of the following is NOT considered a risk factor for nonunion of a type II odontoid fracture?
Explanation
Although obesity can make brace or halo wear difficult, it has not been associated with an increased risk for nonunion. Carson GD, Heller JG, Abitbol JJ, et al: Odontoid fractures, in Levine AM, Eismont FJ, Garfin SR, et al (eds): Spine Trauma. Philadelphia, PA, WB Saunders, 1998, pp 235-238.
Question 332
High Yield
Figure 1 shows the radiograph of a 60-year-old woman who underwent a previous operation for great toe pain 20 years ago. She has had increasing pain over the past 5 years and now reports pain with any motion, swelling, and clicking. She also reports pain under the ball of foot. What is the most appropriate management to alleviate her metatarsalgia and great toe pain?

Explanation
The patient has a failed Silastic implant. Nonsurgical management will not work at this point. A Keller resection will only exacerbate her metatarsalgia. Implant removal with structural bone grafting and MTP fusion is the most appropriate choice because restoration of length is needed to alleviate the forefoot pain and bone grafting is required to fuse the MTP joint because there is an abundance of osteolysis. Total toe implants do not offer good long-term outcomes and are very difficult to fit into the large exploded-out cavity of the proximal phalanx. Hecht PJ, Gibbons MJ, Wapner KL, et al: Arthrodesis of the first metatarsophalangeal joint to salvage failed silicone implant arthroplasty. Foot Ankle Int 1997;18:383-390.
Question 333
High Yield
A farmer is seen in the emergency department after falling out of a hay loft onto the barn floor below. He is unable to bear weight. Exploration of a 0.5 cm laceration over the anterior tibia reveals bone. Radiographs reveal oblique displaced midshaft tibial and fibular fractures. Based on these findings, what is the most appropriate antibiotic prophylaxis?
Explanation
A farm injury is automatically considered a grade III (Gustillo classification) injury regardless of size, energy, or additional soft-tissue injury due to the likelihood of substantial contamination. Antibiotic recommendations for grade III injuries include a first- or second-generation cephalosporin with an aminoglycoside or fluoroquinolone within 3 hours of injury, with penicillin added for farm injuries. Okike K, Bhattacharyya T: Trends in the management of open fractures: A critical analysis. J Bone Joint Surg Am 2006;88:2739-2748.
Question 334
High Yield
A 7-year-old boy has a swollen and deformed right arm after falling off his bicycle. Radiographs reveal a completely displaced posterolateral supracondylar humeral fracture. Examination reveals a warm, pink hand and forearm but absent pulses. What is the next most appropriate step in management?

Explanation
The incidence of vascular injury in supracondylar humeral fractures is directly related to the degree and direction of displacement. Significant posterior lateral displacement tends to result in brachial artery and median nerve injuries, and posterior medial displacement may lead to radial nerve injury. The brachial artery is always injured at the level of the fracture; therefore, angiography or MRA will not assist in locating the injury. The treatment of choice is surgical reduction and stabilization of the fracture, followed by reassessment of the vascular status. If the hand is pink and warm or pulses can be detected with doppler, it is reasonable to follow the extremity closely after surgery. If the arm becomes pulseless and white, immediate anterior exploration of the arm is indicated. The artery is often entrapped in the fracture and once extricated, will provide adequate blood flow. If the artery is injured, a primary repair or vein graft is needed. Shaw BA: The role of angiography in assessing vascular injuries associated with supracondylar humerus fractures remains controversial. J Pediatr Orthop 1998;18:273. Sabharwal S, Tredwell SJ, Beauchamp RD, et al: Management of pulseless pink hand in pediatric supracondylar fractures of humerus. J Pediatr Orthop 1997;17:303-310.
Question 335
High Yield
A 32-year-old man notes increasing back pain and progressive paraparesis over the past few weeks. He is febrile, and laboratory studies show a WBC of 12,500/mm3. MRI scans are shown in Figures 6a and 6b. Management should consist of
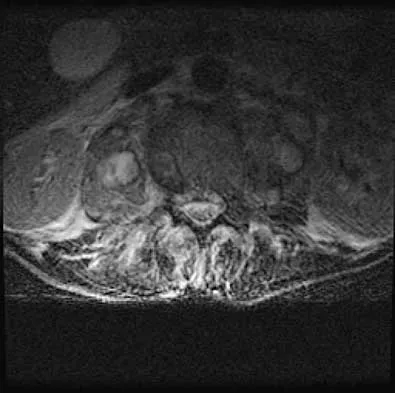

Explanation
Indications for surgery in spinal infections include progressive destruction despite antibiotic treatment, an abscess requiring drainage, neurologic deficit, need for diagnosis, and/or instability. This patient has a progressive neurologic deficit. Debridement performed at the site of the abscess should effect canal decompression. Once the debridement is complete back to viable bone, the defect can be reconstructed with a strut graft. Additional posterior stabilization is used as deemed necessary by the degree of anterior destruction. CT-guided needle aspiration, while occasionally useful in the earliest phases of an infection, produces frequent false-negative results and would provide little useful information in the management of this patient. Emery SE, Chan DP, Woodward HR: Treatment of hematogenous pyogenic vertebral osteomyelitis with anterior debridement and primary bone grafting. Spine 1989;14:284-291. Lifeso RM: Pyogenic spinal sepsis in adults. Spine 1990;15:1265-1271.
Question 336
High Yield
A 56-year-old man underwent right total shoulder arthroplasty 2 months ago. Recently while reaching with his shoulder in a flexed and adducted position, he noted shoulder pain and afterwards he could not externally rotate his arm. An axillary radiograph is shown in Figure 30. What is the most likely cause of this problem?

Explanation
Anteversion of the humeral component may result in anterior instability of the component. Posterior instability after total shoulder arthroplasty is usually the result of some combination of the following factors: untreated anterior soft-tissue contractures, excessive posterior capsular laxity, and excessive retroversion of the humeral and/or glenoid components. Cofield RH, Edgerton BC: Total shoulder arthroplasty: Complications and revision surgery. Instr Course Lect 1990;39:449-462.
Question 337
High Yield
An active 60-year-old man is evaluated 4 years following surgical correction of a hallux valgus deformity. The patient reports that a hallux varus deformity developed rapidly following his initial surgery. Conservative management consisting of wider shoes, toe strapping, and anti-inflammatory drugs has failed to provide relief. Examination reveals a hallux varus deformity with restricted painful motion of the metatarsophalangeal joint and callus formation under the second metatarsal head. What is the next most appropriate step in management?

Explanation
Hallux varus may occur as a complication following hallux valgus surgery, most commonly a modified McBride-type procedure. Conservative management is the initial treatment of choice; however, if unsuccessful, surgical options for reconstruction include soft-tissue reconstruction or metatarsophalangeal joint arthrodesis. The patient has evidence of joint arthrosis, making an arthrodesis the preferred method of reconstruction. Fascial arthroplasty, Silastic arthroplasty, and Keller resection arthroplasty will not correct the underlying deformity. Kitaoka HB, Patzer GL: Arthrodesis versus resection arthroplasty for failed hallux valgus operations. Clin Orthop 1998;347:208-214.
Question 338
High Yield
Antibiotic-loaded bone cement prostheses, such as that shown in Figure 8, are best created by using which of the following methods?

Explanation
In a review of the practical applications of antibiotic-loaded bone cement for the treatment of the infected total joint arthroplasties, Hanssen and Spangehl described commercially available antibiotic-loaded bone cement as low-dose antibiotic cements. These cements generally contained 0.5 g of either tobramycin or gentamicin per 40 g of cement. They are indicated for use in prophylaxis and not for treatment of infected total joint arthroplasties. High-dose antibiotic-loaded bone cements are described as those containing greater than 1.0 g of antibiotic per 40 g of cement. Effective elution levels have been documented with 3.6 g tobramycin and 1.0 g vancomycin per 40 g of bone cement. This was documented by Penner and associates. Furthermore, it was shown that the combination of the two antibiotics in the bone cement improved the elution of both antibiotics. Hanssen AD, Spangehl MJ: Practical applications of antibiotic-loaded bone cement for treatment of infected joint replacements. Clin Orthop 2004;427:79-85.
Question 339
High Yield
An 8-year-old girl injures her elbow playing soccer. After attempted reduction in the emergency department, radiographs of the elbow are shown in Figures 35a through 35c. What is the next most appropriate step in treatment?


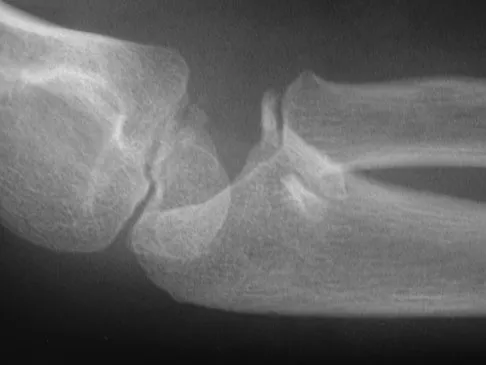
Explanation
Ninety percent of injuries to the proximal radius in children are radial neck fractures, and 50% of these fractures are through the metaphyseal bone. The remaining 50% are Salter-Harris type I or II fractures. These radiographs show a fracture of the radial head and subluxation of the radius anteriorly. Most congenital radial head dislocations are posterior lateral. Nonsurgical treatment modalities are unlikely to be successful due to the wide displacement of the fracture fragments, as well as dislocation of the radial head. Leung AG, Peterson HA: Fractures of the proximal radial head and neck in children with emphasis on those that involve the articular cartilage. J Pediatr Orthop 2000;20:7-14. Hashemi-Nejad A, Goddard NJ: Radial head fractures. Br J Hosp Med 1994;51:223-226.
Question 340
High Yield
When harvesting an iliac crest bone graft from the posterior approach, what anatomic structure is at greatest risk for injury if a Cobb elevator is directed too caudal?
Explanation
If a Cobb elevator is directed caudally while stripping the periosteum over the iliac wing, it will encounter the sciatic notch. Although this puts the sciatic nerve at risk, the first structure encountered is the superior gluteal artery. Because it is tethered at the superior edge of the notch, it is very vulnerable to injury and can then retract inside the pelvis, making it difficult to obtain hemostasis. The inferior gluteal artery exits the sciatic notch below the piriformis and is more protected. The cluneal nerves are at risk only if the incision extends too anteriorly, and the sacroiliac joint can be entered while harvesting the graft. Banwart JC, Asher MA, Hassanein RS: Iliac crest bone graft harvest donor site morbidity: A statistical evaluation. Spine 1995;20:1055-1060.
Question 341
High Yield
Which of the following acetabular cup designs has shown the greatest survivorship at 10 years in patients younger than age 60 years?
Explanation
Poor survivorship of cemented sockets in young patients has lead to the development of a variety of cementless designs. Of these, smooth metal-backed sockets have not performed as well as porous-coated designs. Threaded metal-backed sockets showed a 6% to 25% revision rate secondary to aseptic loosening at a mean follow-up of 4.5 to 6 years. Despite some early failed designs, cementless porous-coated metal-backed sockets have shown the best survivorship in long-term studies. Smith SE, Harris WH: Total hip arthroplasty performed with insertion of the femoral component with cement and the acetabular component without cement: Ten to thirteen-year study. J Bone Joint Surg Am 1997;79:1827-1833.
Question 342
High Yield
Preservation or reconstruction of which of the following structures is essential to minimize the risk of hallux valgus developing after removal of part or all of the medial sesamoid?
Explanation
Complications of medial sesamoidectomy include stiffness, claw toe, and hallux valgus. Each sesamoid sits within its respective head of the flexor hallucis brevis tendon. Excision of one sesamoid can result in slack in its flexor hallucis brevis tendon; therefore, it is imperative to preserve or repair the flexor hallucis brevis tendon when removing the medial sesamoid. Dedmond BT, Cory JW, McBryde A Jr: The hallucal sesamoid complex. J Am Acad Orthop Surg 2006;14:745-753.
Question 343
High Yield
A 40-year-old man has had hip pain with increased activity over the past year. Examination reveals restriction of motion and tenderness with combined hip flexion, adduction, and internal rotation. An AP radiograph is shown in Figure 34. What is the most likely diagnosis?

Explanation
Femoral acetabular impingement (FAI) is a pathologic entity leading to pain, reduced range of motion in flexion and internal rotation, and development of secondary arthritis of the hip. There are two types of FAI: cam impingement and pincher impingement. Cam impingement is seen when a nonspherical femoral head produces a cam effect when the prominent portion to the femoral head rotates into the joint. This mechanism produces shear forces that damage articular cartilage. Radiographs reveal early joint degeneration and flattening of the head neck junction (the so-called "pistol grip deformity") as seen in this image. The pincher type of impingement involves abnormal contact between the femoral head neck junction and the acetabulum, in the presence of a spherical femoral head. Beall DP, Sweet CF, Martin HD, et al: Imaging findings of femoraoacetabular impingement syndrome. Skeletal Radiol 2005;34:691-701.
Question 344
High Yield
In a retroperitoneal approach to the lumbar spine, what structure runs along the medial aspect of the psoas and along the lateral border of the spine?
Explanation
The sympathetic trunk runs longitudinally along the medial border of the psoas. The ilioinguinal nerve emerges along the upper lateral border of the psoas and travels to the quadratus lumborium, and the genitofemoral nerve lies more laterally on the psoas. The ureter is adherent to the posterior peritoneum and falls away from the psoas and the spine in the dissection, as does the aorta. Watkins RG (ed): Surgical Approaches to the Spine. New York, NY, Springer-Verlag, 1983, p 107.
Question 345
High Yield
What is the most common site of metastases from a soft-tissue sarcoma?

Explanation
The most common site of metastases from a soft-tissue sarcoma is the lungs and occurs in 40% to 60% of patients. The second most common site of metastases in soft-tissue sarcomas is the lymph nodes. Nodal metastases are seen with regularity in synovial sarcoma, epithelioid sarcoma, and rhabdosarcoma. The liver, brain, bone, and muscle are occasional sites of spread, but the occurrence is very rare. Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 219-276.
Question 346
High Yield
A 29-year-old patient sustains a closed, displaced joint depression intra-articular calcaneus fracture. In discussing potential complications of surgical intervention through an extensile lateral approach, which of the following is considered the most common complication following surgery?

Explanation
Delayed wound healing and wound dehiscence is the most common complication of surgical management of calcaneal fractures through an extensile lateral approach, occurring in up to 25% of patients. Most wounds ultimately heal with local treatment; the deep infection rate is approximately 1% to 4% in closed fractures. Posttraumatic arthritis may develop despite open reduction and internal fixation, but the percentages remain low. Peroneal tendinitis may occur from adhesions within the tendon sheath or from prominent hardware but is relatively uncommon. Nonunion of a calcaneal fracture is rare. Sanders RW, Clare MP: Fractures of the calcaneus, in Coughlin MJ, Mann RA, Saltzman CL (eds): Surgery of the Foot and Ankle, ed 8. Philadelphia, PA, Mosby-Elsevier, 2007, vol 2, pp 2017-2073.
Question 347
High Yield
The third plantar intrinsic muscle layer of the foot consists of which of the following structures?
Explanation
The plantar intrinsic muscles are divided into four layers with respect to depth from the plantar fascia. They are (from superficial to deep): 1) abductor hallucis, flexor digitorum brevis, abductor digiti minimi; 2) quadratus plantae, lumbricals; 3) flexor digiti minimi, flexor hallucis brevis, adductor hallucis brevis; and 4) dorsal and plantar interosseous muscles. The flexor hallucis brevis and adductor hallucis brevis originate from the midtarsal bones, encompass the sesamoids, and insert into the base of the proximal phalanx. The adductor hallucis brevis consists of two muscle bellies forming a conjoined tendon and inserting into the lateral portion of the proximal phalanx and the lateral sesamoid. The adductor hallucis brevis is stronger than the abductor hallucis brevis, which may contribute to hallux valgus. The flexor digitorum minimi travels under the fifth metatarsal, arising at the base and inserting into the lateral base of the fifth proximal phalanx.
Question 348
High Yield
On MRI, a nonsanguinous effusion has what appearance?

Explanation
Nonbloody effusions that are greater than 1 mL are readily detected by MRI. They appear black on T1-weighted images and white on T2-weighted images. A sanguinous effusion is seen as white on T1-weighted images and black on T2-weighted images. Resnick D, Kang HS: Synovial joints, in Resnick D, Kang HS (eds): Internal Derangements of Joints: Emphasis on MR Imaging. Philadelphia, PA, WB Saunders, 1997, pp 49-53.
Question 349
High Yield
Closed-chain exercise differs from open-chain exercise in which of the following ways?
Explanation
Closed-chain exercise requires the distal portion of the extremity to be fixed. It is more commonly used in lower extremity exercise, and movement is produced by co-contraction of muscles. Joint compression is increased, and multiple joints are involved with closed-chain exercise. In open-chain exercise, the distal portion of the extremity is free. Braddom RL (ed): Physical Medicine and Rehabilitation, ed 2. Philadelphia, PA, Saunders, 2000, pp 975-976.
Question 350
High Yield
A 12-year-old girl has painless bowing of the tibia. Radiographs and a biopsy specimen are shown in Figures 35a through 35c. What is the most likely diagnosis?


Explanation
The patient has osteofibrous dysplasia. The radiographic differential diagnosis includes osteofibrous dysplasia, fibrous dysplasia, and adamantinoma. Histology shows a fibro-osseous lesion with prominent osteoblastic rimming but a lack of epithelial nests. Adamantinoma is a low-grade malignancy that typically is located in the anterior tibial cortex and has a soap bubble appearance. Histologically, it is similar to osteofibrous dysplasia but includes epithelial nests of cells. Treatment requires resection. Fibrous dysplasia usually does not require biopsy; however, in this patient the radiographs do not distinguish it from adamantinoma. The radiographic findings are not typical of Ewing's sarcoma or osteosarcoma. Repeat biopsy should be considered if clinical or radiographic features change.
Question 351
High Yield
A 27-year-old man sustained a gunshot wound to the lumbar spine and undergoes an exploratory laparotomy. An injury to the cecum is identified and treated. Management should now include

Explanation
Gunshot wounds to the spine present relatively little risk of infection in most cases. When there has been an injury to the colon, the risk of infection can be minimized with a 7-day course of broad-spectrum antibiotics. Fragment removal is not indicated. Roffi RP, Waters RL, Adkins RH: Gunshot wounds to the spine associated with a perforated viscus. Spine 1989;14:808-811.
Question 352
High Yield
A 12-year-old girl has a 4-cm limb-length discrepancy following a fracture of the left distal femur 2 years ago. Examination reveals 18 degrees of genu valgum on the involved side, with 7 degrees of genu valgum on the opposite side. Radiographs show that the left distal femoral growth plate is now closed; however, the tibial growth plate is still open. Her bone age matches her chronologic age. Management should consist of
Explanation
The patient has a projected limb-length discrepancy of 7 cm. This includes the 4 cm she already has, plus 3 cm expected growth of the uninvolved distal femur during the 3 years of growth she has remaining. She also has moderate limb deformity. Femoral lengthening is considered the treatment of choice because it can address both the limb-length discrepancy and the deformity. Epiphyseodesis will not result in limb-length equality at maturity, with only approximately 1.8 cm of equalization expected from this procedure. Use of closed femoral shortening of 7 cm runs the risk of weakening the quadriceps on the normal side and will leave the patient with a remaining residual valgus deformity. Tibial lengthening will leave the knees at different levels. A shoe lift can be prescribed as a temporary measure but is not a good long-term solution. Westh RN, Menelaus MB: A simple calculation for the timing of epiphyseal arrest: A further report. J Bone Joint Surg Br 1981;63:117-119. Sasso RC, Urquhart BA, Cain TE: Closed femoral shortening. J Pediatr Orthop 1993;13:51-56.
Question 353
High Yield
Because the patient shown in Figure 27 can no longer fit in shoes, treatment of the deformity should consist of

Explanation
In local gigantism, a ray resection allows proper fitting of shoes. The ray resection narrows the foot and shortens the length. The foot may require further surgery with growth. Debulking, physeal arrest, and distal phalanx amputation are unlikely to be effective. Turra S, Santini S, Cagnoni G, Jacopetti T: Gigantism of the foot: Our experience in seven cases. J Pediatr Orthop 1998;18:337-345.
Question 354
High Yield
Which of the following staging studies should be obtained for an adult with an 8-cm deep, high-grade malignant fibrous histiocytoma of the extremity?
Explanation
MRI is the preferred imaging study to evaluate the local tumor extension for soft-tissue lesions, but CT can be used if MRI is contraindicated (eg, patients with pacemakers). CT of the chest is always recommended in patients with high-grade sarcomas because 80% of metastases occur in the lungs. CT of the abdomen and pelvis is indicated in patients with lower extremity liposarcoma because some patients also have synchronous retroperitoneal liposarcoma. Lymph node metastasis occurs in up to 5% of patients with soft-tissue sarcoma. If the nodes are clinically enlarged, biopsy is indicated. Routine sentinel node biopsy currently is not recommended. Bone scan is not used in the staging of soft-tissue sarcoma as it has not been shown to be cost-effective. Demetri GD, Pollock R, Baker L, Balcerzak S, Casper E, Conrad C, et al: NCCN sarcoma practice guidelines: National Comprehensive Cancer Network. Oncology (Huntingt) 1998;12:183-218.
Question 355
High Yield
What process is often found associated with other neoplasms?
Explanation
Aneurysmal bone cyst may be either a "pattern" or a "diagnosis." Therefore, aneurysmal bone cyst should be viewed as a diagnosis of exclusion. Hemorrhage into a variety of primary bone lesions (eg, giant cell tumor of bone, chondroblastoma, osteoblastoma, fibrous dysplasia, osteosarcoma, or vascular neoplasms) may result in intralesional, membrane-bone blood-filled cysts. Such secondary changes may be confused with aneurysmal bone cyst, resulting in inappropriate therapy because assessment should be focused on identifying the underlying primary process. The entire specimen should be examined histologically in an effort to locate an underlying primary bone tumor. Bonakdarpour A, Levy WM, Aegerter E: Primary and secondary aneurysmal bone cyst: A radiological study of 75 cases. Radiology 1978;126:75-83. Levy WM, Miller AS, Bonakdarpour A, Aegerter E: Aneurysmal bone cyst secondary to other osseous lesions: Report of 57 cases. Am J Clin Pathol 1975;63:1-8.
Question 356
High Yield
An 18-year-old girl with quadriplegic cerebral palsy underwent posterior spinal fusion from T2 to the pelvis 3 weeks ago. She now has a low-grade fever and mild midline erythema in a 1-cm area from which there is slight clear yellowish drainage. What is the next most appropriate step in management?

Explanation
The presence of drainage 3 weeks after surgery is a sign of wound infection. This infection most likely involves deep tissues until proven otherwise. Oral or IV antibiotics, in the absence of debridement, are not sufficient. Removal of the hardware would lead to rapid progression of the scoliosis in a spine that has been surgically destabilized by removal of the facet joints. The appropriate treatment is debridement with wound culture, IV antibiotics, and retention of hardware. The wound should be closed over drains. Theiss SM, Lonstein JE, Winter RB: Wound infections in reconstructive spine surgery. Orthop Clin North Am 1996;27:105-110.
Question 357
High Yield
What is the most appropriate orthotic management for the lesion shown in Figure 6?

Explanation
The figure shows an intractable plantar keratosis (IPK). The keratoma usually forms beneath a bony prominence. This can occur under the sesamoids, most commonly the tibial sesamoid, or under the fibular condyle of a prominent metatarsal head. The initial treatment of an IPK consists of paring down the callused lesion and placing a metatarsal pad proximal to the lesion to provide posting to unload the bony prominence.
Question 358
High Yield
An otherwise healthy 78-year-old woman has low back and buttock pain. Rectal examination reveals a large sacral mass. Figures 7a and 7b show a CT scan and a sagittal MRI scan of the lumbosacral spine. A biopsy specimen is shown in Figure 7c. What is the most likely diagnosis?

Explanation
A chordoma is a malignant neoplasm originating from remnants of the notochord. It is usually localized to the midline with 50% at the sacrococcygeal area, 35% at the skull base, and 15% at the mobile portion of the spine. Large vacuolated cells (physaliferous cells) are a characteristic of the tumor. Mindell ER: Chordoma. J Bone Joint Surg Am 1981;63:501-505.
Question 359
High Yield
What is the most likely cause of the lesion shown in Figures 35a and 35b?

Explanation
The most common cause of myositis ossificans is contusion. Certain regions, including the quadriceps and brachialis, are more commonly affected. The mechanisms of development have not been clearly established. Beiner JM, Jokl P: Muscle contusion injuries: Current treatment options. J Am Acad Orthop Surg 2001;9:227-237.
Question 360
High Yield
Which of the following statements regarding conus medullaris syndrome is most accurate?
Explanation
Conus medullaris syndrome most frequently occurs as a result of trauma or with a disk herniation at L1, resulting in a lower motor neuron syndrome but with a poor prognosis for recovery of bowel and bladder dysfunction. The conus region, as the termination of the spinal cord, contains the motor cell bodies of the sacral roots. The syndrome is usually a sacral level neural injury; therefore, lower extremity weakness is uncommon. Haher TR, Felmly WT, O'Brien M: Thoracic and lumbar fractures: Diagnosis and management, in Bridwell KH, Dewald RL, Hammerberg KW, et al (eds): The Textbook of Spinal Surgery, ed 2. New York, NY, Lippincott Williams & Wilkins, 1977, pp 1773-1778.
Question 361
High Yield
Which of the following findings is likely to be pathologic in a thin, well-conditioned endurance athlete?
Explanation
Left ventricular hypertrophy by voltage is a nonspecific diagnosis, especially in athletes with an asthenic body habitus. High vagal tone in endurance athletes may result in first degree or even type I second degree (ie, Wenckebach) AV block in endurance athletes. High vagal tone results in resting sinus bradycardia in many trained athletes. A I-II/IV systolic ejection murmur is occasionally found in healthy athletes; however, when the murmur increases in intensity with maneuvers that decrease ventricular filling, such as standing or the Valsalva maneuver, dynamic obstruction that is the result of hypertrophic obstructive cardiomyopathy should be suspected. Nonspecific STT wave changes in the lateral leads on ECG are not uncommon in highly trained athletes; thus, they are nonspecific for ischemic heart disease. Pelliccia A, Maron BJ, Culasso F, DiPaolo FM, et al: Clinical significance of abnormal electrocardiographic patterns in trained athletes. Circulation 2000;102:278-284.
Question 362
High Yield
Which of the following radiographic images is best for detecting anterior acetabular deficiency in the dysplastic hip?

Explanation
The false profile view of Lequesne and de Seze is obtained with the patient standing with the affected hip on the cassette, the ipsilateral foot parallel to the cassette, and the pelvis rotated 65 degrees from the plane of the cassette. This view best assesses anterior coverage of the femoral head. Garbuz DS, Masri BA, Haddad F, et al: Clinical and radiographic assessment the young adult with symptomatic dysplasia. Clin Orthop Relat Res 2004;418:18-22.
Question 363
High Yield
A 58-year-old man has had a 3-year history of recurrent ulcerations of the left ankle and instability despite multiple attempts at custom bracing, contact casting, and surgical debridement. He has an ankle-brachial index of 0.76. A clinical photograph and radiographs are shown in Figures 16a through 16c. Treatment should now consist of



Explanation
Nonsurgical management has failed to provide relief; therefore, the treatment of choice is arthrodesis with an intramedullary nail. Amputation may be indicated if the arthrodesis fails. The patient does have adequate circulation for an attempt at salvage. Total ankle arthroplasty is not indicated in a neuropathic patient. Pinzur MS, Kelikian A: Charcot ankle fusion with a retrograde locked intramedullary nail. Foot Ankle Int 1997;18:699-704.
Question 364
High Yield
The main advantage of surgical repair of an acute Achilles tendon rupture, when compared with nonsurgical management, is reduced

Explanation
The literature supports similar clinical outcomes after surgical and nonsurgical methods. The chief difference lies in the complications between the groups. Surgical patients experience more wound problems but a significantly lower rerupture rate. Although suturing the tendon allows earlier mobility, the tendon healing time is unchanged. Nonsurgical methods are less expensive to provide. Maffulli N: Rupture of the Achilles tendon. J Bone Joint Surg Am 1999;81:1019-1036. Cetti R, Christensen SE, Ejsted R, Jensen NM, Jorgensen U: Operative versus nonoperative treatment of Achilles tendon rupture: A prospective randomized study and review of the literature. Am J Sports Med 1993;21:791-799.
Question 365
High Yield
Which of the following is considered the treatment of choice for a chondroblastoma of the proximal tibial epiphysis without intra-articular extension?

Explanation
Curettage and bone grafting typically is the preferred method of treatment for chondroblastoma, with local recurrence rates of approximately 10%. Some clinicians advocate the addition of adjuvants such as phenol. Left alone, these lesions can destroy bone and invade the joint. Large intra-articular lesions may require major joint reconstruction. Wide local excision rarely is required to eradicate the tumor. Radiation therapy rarely is indicated and only for unresectable or multiply recurrent lesions. Springfield DS, Capanna R, Gherlinzoni F, Picci P, Campanacci M: Chondroblastoma: A review of seventy cases. J Bone Joint Surg Am 1985;67:748-755.
Question 366
High Yield
A 72-year-old woman who is right hand-dominant has severe pain in the right shoulder that has failed to respond to nonsurgical management. She reports night pain and significant disability. Examination reveals 30 degrees of active forward elevation. An AP radiograph is shown in Figure 27. Which of the following treatment options will provide the best functional improvement?

Explanation
The patient has end-stage rotator cuff tear arthropathy. The radiograph shows complete proximal humeral migration (acromiohumeral interval of 0 mm), severe glenohumeral arthritis, and acetabularization of the acromion. In addition, she has "pseudoparalysis" with active elevation of only 30 degrees. Reverse shoulder arthroplasty affords her the best opportunity for pain relief and functional improvement. The other procedures have mixed results but typically are better for pain relief than they are for functional gains. Frankle M, Siegal S, Pupello D, et al: The reverse shoulder prosthesis for glenohumeral arthritis associated with severe rotator cuff deficiency: A minimum two-year follow-up study of sixty patients. J Bone Joint Surg Am 2005;87:1697-1705.
Question 367
High Yield
A 12-year-old girl falls in gymnastics and sustains comminuted midshaft radius and ulna fractures. Closed reduction and cast immobilization are attempted but fracture redisplacement with 20 degrees of angulation occurs. Surgical treatment includes closed reduction and intramedullary fixation of both bones. What is the most common long-term complication for this fracture?
Explanation
Healing of forearm fractures in skeletally immature patients is the usual outcome. The use of intramedullary fixation has been reported to result in a lower frequency of refractures when compared to plate osteosynthesis due to the absence of diaphyseal holes after plate removal, which are considered stress risers. Regardless of implant technique, malunion and infection are infrequent. Loss of forearm pronation and supination is a common occurrence in surgically treated fractures due to the higher degree of soft-tissue injury, and periosteal stripping leads to fracture site instability and fracture comminution. Luhmann SJ, Gordon JE, Schoenecker PL: Intramedullary fixation of unstable both-bone forearm fractures in children. J Pediatr Orthop 1998;18:451-456.
Question 368
High Yield
Figure 42 is a transverse MRI scan of the left shoulder. The arrow points to which of the following structures?

Explanation
The figure shows an axial image of the shoulder immediately inferior to the coracoid process. The subscapularis tendon, which can be traced from the myotendinous junction, is torn and detached from its lesser tuberosity attachment on the humerus. Lateral to the lesser tuberosity, the bicipital groove is empty. The arrow points to the subluxated biceps tendon. Superficial fibers of the subscapularis tendon are contiguous with the biceps retinaculum, which covers the bicipital groove and hold the biceps tendon in place. The vast majority of subscapularis tendon tears result in disruption of the biceps retinaculum with resultant subluxation of the tendon. Resnick D, Kang HS (eds): Internal Derangement of Joints: Emphasis on MR Imaging. Philadelphia, PA, WB Saunders, 1997, pp 308-317.
Question 369
High Yield
What is the most likely late complication associated with cementless total knee replacement?
Explanation
In cementless total knee replacement, the risk of osteolysis is 30% if both components are placed without cement and screws are used for tibial fixation. The risk is 10% when a cemented tibial component is used, and the risk is 0% when both components are cemented. Loss of motion, patellofemoral pain, heterotopic bone formation, and patellar clunk are complications that can occur after cemented or cementless components are placed.
Question 370
High Yield
Figures 9a and 9b show the radiographs of a 75-year-old man who underwent a revision total knee arthroplasty with a long-stemmed tibial component. In rehabilitation, he reports fullness and tenderness in the proximal medial leg (at the knee). The strategy that would best limit this postoperative problem is use of


Explanation
The problem with this reconstruction is the medial protrusion of the base plate. The use of a base plate with an offset stem can prevent the protrusion and thus the impingement and pain. Allograft bone or smoothing the outline with cement would be just as prominent and likely to cause pain. An ingrowth surface may improve soft-tissue attachment but would still leave the implant protruding medially and likely to cause pain. A nonstemmed tibial base plate would lead to less medial protrusion but at the expense of a smaller area for load carriage on the proximal tibia.
Question 371
High Yield
A newborn has an anterolateral bow of the tibia and a duplication of the great toe. Which of the following conditions will develop as the infant grows?
Explanation
Anterolateral bowing of the tibia is normally associated with congenital pseudarthrosis of the tibia. This, in turn, is associated with neurofibromatosis. Posterior bowing is more benign and usually corrects spontaneously. However, anterolateral bowing also corrects spontaneously, and the limb-length discrepancy may be the only remaining sequela when associated with duplication of the great toe. Lisch nodules and axillary freckling are pathognomonic findings in neurofibromatosis but would not be expected in this patient because this type of tibial deformity is not associated with neurofibromatosis.
Question 372
High Yield
Figures 28a and 28b show the radiographs of a 79-year-old man who has constant knee pain. Prior to performing elective knee replacement surgery, management should include


Explanation
The radiographs show established Paget's disease. Bony expansion is evident, with thickened trabeculae consistent with the disordered bone remodeling process. A reduction of the serum alkaline phosphatase level to 50% of the pretreatment level may reduce pain from Paget's disease, and it is recommended prior to consideration of joint replacement. In elective cases, treatment of Paget's disease should begin at least 6 weeks prior to surgery. The other modalities are not related to the treatment of Paget's disease. Kaplan FS, Singer FS: Paget's disease of bone: Pathophysiology, diagnosis, and management. J Am Acad Orthop Surg 1995;3:336-344. Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 129-184.
Question 373
High Yield
In girls with idiopathic scoliosis, peak height velocity (PHV) typically occurs at what point?

Explanation
PHV generally occurs while girls are still Risser 0; menarche typically occurs before Risser 1, which has a wide variation in its timing. The curve magnitude at the PHV is the best prognostic indicator available. Most untreated patients with curves greater than 30 degrees at PHV require surgery, while patients with smaller curves at that stage typically do not require surgery. Little DG, Song KM, Katz D, Herring JA: Relationship of peak height velocity to other maturity indicators in idiopathic scoliosis in girls. J Bone Joint Surg Am 2000;82:685-693.
Question 374
High Yield
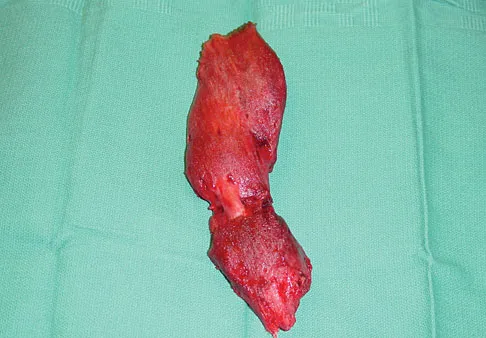
A 56-year-old woman has a painful mass on the bottom of her left foot, and orthotic management has failed to provide relief. Examination reveals that the mass is contiguous with the plantar fascia. An MRI scan shows a homogenous nodule within the plantar fascia. Resection of the tumor is shown in the clinical photograph in Figure 39. What type of cell is most likely responsible for the formation of this tumor?
Explanation
The history, examination, and surgical findings are most consistent with plantar fibromatosis. Plantar fibromatosis is a benign tumor of the plantar fascia that consists chiefly of fibromyoblasts. These cells produce excessive collagen and are similar to the cells found in the palmar fascia of patients with Dupuytren's contracture of the hand. The myocyte, synovial cell, and osteocyte all produce their respective individual tissue types but do not contribute to the formation of a plantar fibromatosis. The T-cell is an important immunologic cell that is most affected in patients with HIV.
Question 375
High Yield
In displaced calcaneal fractures, what fragment is the only one that remains in its anatomic position?
Explanation
The sustentaculum tali remains in its anatomic position because of its supporting ligamentous structures. This provides the key to the reconstruction of the calcaneus. The posterior facet is reduced to the sustentaculum tali and then fixed to it for stability. All of the other components of the calcaneus are then reduced to this complex. Sanders R: Displaced intra-articular fractures of the calcaneus. J Bone Joint Surg Am 2000;82:225-250. Eastwood DM, Gregg PJ, Atkins RM: Intra-articular fractures of the calcaneum: Part I. Pathological anatomy and classification. J Bone Joint Surg Br 1993;75:183-188.
Question 376
High Yield
The dorsal digital cutaneous nerve of the great toe shown in Figure 8 is a branch of what nerve?
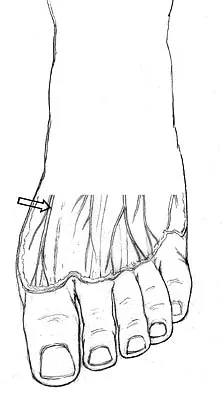
Explanation
The dorsal digital cutaneous nerve of the great toe is a branch of the medial branch of the superficial peroneal nerve. The deep peroneal nerve supplies the first web space. McMinn RMH, Hutchings RT, Logan BM: Color Atlas of Foot and Ankle Anatomy. Weert, Netherlands, Wolfe Medical Publications, 1982, p 50.
Question 377
High Yield
Which of the following body positions is associated with the highest intradiskal pressure?
Explanation
Intradiskal pressure is lowest when the patient is in the supine position. Sitting is associated with higher intradiskal pressures than standing. Flexion also increases intradiskal pressure. The combination of flexion and sitting produces the highest intradiskal pressure. Nachemson and Morris found that intradiskal pressure increases as position changes from lying supine, lying prone, standing, leaning forward, sitting, and sitting leaning forward. Twisting or straining in positions of relatively high intradiskal pressure may predispose patients to herniation of the intervertebral disk. Patients with a herniated disk may also notice their pain worsens with activities that increase the disk pressure, including the positions mentioned, or activities that increase intra-abdominal pressure (coughing, sneezing, straining). Nachemson A, Morris JM: In vivo measurements of intradiscal pressure. J Bone Joint Surg Am 1964;46:1077-1092.
Question 378
High Yield
Figure 28 shows an AP radiograph of a 54-year-old woman who underwent lumbar laminectomy and fusion at the L4 and L5 levels with placement of a bone stimulator 8 years ago. She also underwent a left total hip arthroplasty 2 years ago; aspiration of that joint now reveals that it is infected with a gram-positive cocci organism. History is also significant for IV drug use and human immunodeficiency virus (HIV). The patient reports fever, chills, and left flank and abdominal pain. Examination reveals significant pain with resisted left hip flexion and passive hip extension. She also has lumbar hyperlordosis. Which of the following studies would best identify the underlying cause of her infection?

Explanation
The patient's clinical signs (fever and flank, hip, and abdominal pain) suggest a primary iliopsoas abscess. With an increased patient population who abuse drugs and/or who are HIV-positive, iliopsoas abscess may be more prevalent because of systemic bacterial seeding and may be potentially unrecognized. Diagnostic imaging studies provide a better understanding of the anatomic magnitude of the infection, give concrete confirmation of the diagnosis, and may suggest an underlying cause. Neither standard abdominal radiographs nor ultrasound studies are sensitive enough to be diagnostic of this disease process. CT has been established as the standard study for identifying the underlying cause of this abscess. The hip infection has most likely developed as a result of hematogenous spread from an infected skin lesion from the patient's IV drug use. Santaella RO, Fishman EK, Lipsett PA: Primary vs secondary iliopsoas abscess: Presentation, microbiology, and treatment. Arch Surg 1995;130:1309-1313.
Question 379
High Yield
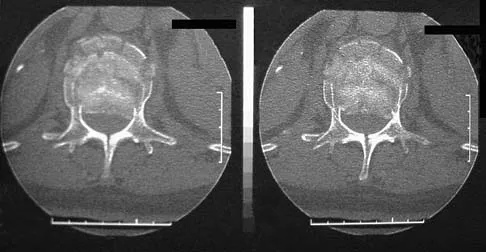
A 42-year-old man sustained a burst fracture at L2 in a motor vehicle accident. Examination reveals that he is neurologically intact. Figure 18 shows a cross-sectional CT scan through the fracture. If the fracture is managed nonsurgically for the next 2 years, the retained fragments can be expected to

Explanation
Numerous articles have reported that both surgical and nonsurgical management of burst fractures are associated with resolution of impingement at long-term follow-up. If the patient is neurologically intact and appropriately treated at the time of injury, neurologic deterioration is not expected nor is there a risk of injury to the dural sac. The retained fragments can be expected to gradually resorb and widen the spinal canal. Mumford J, Weinstein JN, Spratt KF, et al: Thoracolumbar burst fractures: The clinical efficacy and outcome of nonoperative management. Spine 1993;18:955-970.
Question 380
High Yield
A 25-year-old woman with a healed proximal tibiofibular fracture treated with an intramedullary nail 2 years ago is currently wearing an ankle-foot orthosis (AFO) and reports a persistent foot drop. She is unhappy with the AFO and has not seen any functional improvement despite months of physical therapy. Serial electromyograms (EMG) show no recent change over the past year. Examination and EMG findings are consistent with a tibialis anterior 1/5, extensor hallucis longus 2/5, extensor digitorum longus 2/5, posterior tibial tendon (PTT) 5/5, peroneals 3/5, flexor hallucis longus 5/5, and gastrocsoleus 5/5. No discrete nerve lesion was identified. The patient has a flexible equinovarus contracture. What is the most appropriate management?

Explanation
This pattern of injury is consistent with an unrecognized compartment syndrome of the anterior and lateral compartments. Transfer of the PTT through a long incision in the interosseous membrane corrects the foot drop deformity, and allows adequate dorsiflexion provided that the tendon to be transferred has a strength of 5/5. Muscles/tendons typically lose one grade of strength after transfer. Transfer into the tendons at the level of the ankle prevents overtensioning or pullout of a PTT tendon that is not long enough. Debridement of the scarred muscle in the anterior compartment decreases the risk of scarring down to the tendon transfer. Transfer of the peroneus longus is not preferred given its relative lack of strength and line of pull. Continued therapy and bracing are unlikely to lead to further improvement at 2 years after injury. An ankle fusion would correct the foot drop but would not address the tendon imbalances between the tibialis anterior and the peroneus longus, and the PTT and the peroneus brevis. Hansen ST Jr: Functional Reconstruction of the Foot and Ankle. Philadelphia, PA, Lippincott Williams & Wilkins, 2000, p 192. Atesalp AS, Yildiz C, Komurcu M, et al: Posterior tibial tendon transfer and tendo-Achilles lengthening for equinovarus foot deformity due to severe crush injury. Foot Ankle Int 2002;23:1103-1106. Scott AC, Scarborough N: The use of dynamic EMG in predicting the outcome of split posterior tibial tendon transfers in spastic hemiplegia. J Pediatr Orthop 2006;26:777-780.
Question 381
High Yield
What is the most common donor site complication following a free vascularized fibular graft for osteonecrosis of the femoral head?
Explanation
Urbaniak and Harvey reported donor site morbidity following free vascularized fibular graft in 198 consecutive patients. At a 5-year follow-up, they reported overall complications in 24% of the patients. The most common complication was a sensory deficit (11.8%), followed by motor weakness (2.7%), flexor hallucis longus contracture (2%), and deep venous thrombosis (less than 1%).
Question 382
High Yield
Figure 52 shows the MRI scan of a 28-year-old baseball pitcher. Examination will most likely reveal which of the following findings?

Explanation
A ganglion cyst compressing the suprascapular nerve results in poorly localized pain in the shoulder girdle. Sensation is intact, with weakness of external rotation and abduction. Supraspinatus and infraspinatus atrophy is often noted when viewed from behind. These cysts are typically associated with labral tears. Deltoid weakness is associated with an axillary nerve injury, and scapular winging results from injury to the long thoracic nerve. Piatt BE, Hawkins RJ, Fritz RC, et al: Clinical evaluation and treatment of spinoglenoid notch ganglion cysts. J Shoulder Elbow Surg 2002;11:600-604.
Question 383
High Yield
A 58-year-old woman sustained a ruptured Achilles tendon 1 year ago, and management consisted of an ankle-foot orthosis. She now reports increasing difficulty with ambulation and increasing pain. An MRI scan shows a 6-cm defect in the right Achilles tendon. Management should now consist of
Explanation
With a gap of less than 4 cm, a V-Y repair would be appropriate without a tendon transfer. For gaps greater than 5 cm, a lengthening with augmentation is the most appropriate treatment. Therefore, the treatment of choice is an Achilles tendon turndown with flexor hallucis longus tendon transfer. The plantaris tendon is not a strong enough repair, and direct repair is not possible given the large defect in the Achilles tendon. Continued use of the ankle-foot orthosis will not provide adequate relief for this patient.
Question 384
High Yield
Osteonecrosis of the femoral head after intramedullary nailing in children is thought to be the result of injury to the
Explanation
All of these are possible explanations for the development of osteonecrosis following intramedullary nailing in children. However, the lateral ascending cervical artery, which supplies the epiphysis, is much more vulnerable to injury in children because it lies in the trochanteric fossa. Buckley SL: Current trends in the treatment of femoral shaft fractures in children and adolescents. Clin Orthop 1997;338:60-73.
Question 385
High Yield
The dose of the chemotherapeutic agent doxorubicin (Adriamycin) is limited by which of the following factors?
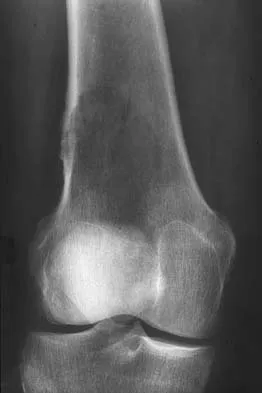
Explanation
Doxorubicin is a chemotherapeutic agent that is best known for dose-limiting cardiotoxicity. This is related not only to the cumulative dose, but also the rate of infusion.
Question 386
High Yield
An otherwise healthy 37-year-old man fell off the flatbed of a delivery truck and landed directly on his dominant left hand. Surgical stabilization of a distal radius fracture is performed. An intraoperative radiograph is shown in Figure 22. What is the next most appropriate step in management?

Explanation
The intraoperative radiograph reveals a scapholunate ligament disruption. Repair of the stout dorsal scapholunate interosseous ligaments is required. Interestingly, the results of scapholunate ligament injuries associated with distal radius fractures appear to be superior to those of isolated ligament injuries. Smith DW, Henry MK: Comprehensive management of soft-tissue injuries associated with distal radius fractures. J ASSH 2002;3:153-164.
Question 387
High Yield
Which of the following agents increases the risk for a nonunion following a posterior spinal fusion?
Explanation
Nonsteroidal anti-inflammatory drugs (NSAIDs) have been shown to increase the risk of pseudarthrosis. In a controlled rabbit study, nonunions were reported with the use of toradol and indomethacin. NSAIDs are commonly used medications with the potential to diminish osteogenesis. Studies clearly have demonstrated inhibition of spinal fusion following the postoperative administration of several NSAIDs, including ibuprofen. Cigarette smoking is another potent inhibitor of spinal fusion. Glassman SD, Rose SM, Dimar JR, et al: The effect of postoperative nonsteroidal anti-inflammatory drug administration on spinal fusion. Spine 1998;23:834-838.
Question 388
High Yield
Figures 47a and 47b show the CT scans of a patient who reports persistent pain in the sinus tarsi following a fall. The avulsion fracture fragment remains attached to what ligament?
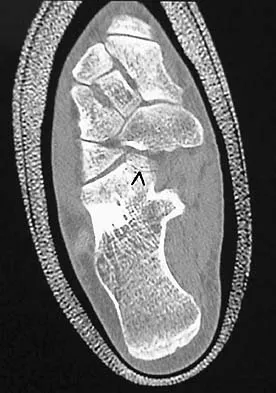

Explanation
The bifurcate ligament bifurcates to connect the dorsal aspect of the anterior process of the calcaneus to both the cuboid and the navicular. Inversion injuries on the side of the foot can result in avulsion fractures (arrow) of the anterior process of the calcaneus. Sarrafian SK: Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. New York, NY, Lippincott, 1993, p 192.
Question 389
High Yield
A 21-year-old man who was injured in a snowboarding accident 18 months ago now reports wrist pain. An MRI scan is shown in Figure 37. Based on the image findings, what is the most likely diagnosis?

Explanation
The coronal MRI scan of the wrist shows the scaphoid. There is a subtle fracture line with a step-off at the radial surface consistent with a nonunion. The signal intensity is markedly different between the two fragments of the scaphoid. This strongly suggests osteonecrosis. Preiser's disease is osteonecrosis typically involving most or all of the scaphoid. Kienbock's disease involves the lunate. Intraosseous ganglia are easily diagnosed on MRI but typically have a fluid-filled area surrounded by denser bone in the periphery. Scapholunate dissociation can be seen on MRI as an injury to the scapholunate ligament and widening of the scapholunate interval, neither of which is seen on this image.
Question 390
High Yield
A 72-year-old man injured his right shoulder after tripping over a chair leg. Radiographs obtained in the emergency department reveal an isolated anterior dislocation. After successful closed reduction, the patient has recurrent anterior instability and is unable to elevate the arm. What is the most likely cause of the recurrent instability?

Explanation
A rotator cuff tear is the most common cause of recurrent instability following a first-time dislocation in patients older than age 40 years. Dislocations occur through a posterior mechanism rather than by an isolated labral avulsion or a Bankart lesion as seen in younger patients. Nevaiser RJ, Nevaiser TJ: Recurrent instability of the shoulder after age 40. J Shoulder Elbow Surg 1995;4:416-418.
Question 391
High Yield
A baseball player has had diffuse scapular soreness for the past 8 weeks. He reports that it began insidiously over several days and gradually has become worse. He denies any history of trauma. Examination reveals drooping of the shoulder, with lateral winging of the scapula at rest. He is otherwise neurologically intact. What is the best course of action?
Explanation
Lateral scapular winging is characteristic of trapezius palsy, whereas medial scapular winging is characteristic of long thoracic nerve palsy. During sports activity, injury to the spinal accessory nerve is rare but may occur with blunt or stretching trauma. Patients often report an asymmetric neckline, drooping shoulder, winging of the scapula, and weakness of forward elevation. Evaluation should include a complete electrodiagnostic examination. Wiater JM, Bigliani LU: Spinal accessory nerve injury. Clin Orthop 1999;368:5-16. Wiater JM, Flatow EL: Long thoracic nerve injury. Clin Orthop 1999;368:17-27. Mariani PP, Santoriello P, Maresca G: Spontaneous accessory nerve palsy. J Shoulder Elbow Surg 1998;7:545-546. Porter P, Fernandez GN: Stretch-induced spinal accessory nerve palsy: A case report. J Shoulder Elbow Surg 2001;10:92-94.
Question 392
High Yield
Which of the following tumors is most likely to present with a pathologic fracture in a child?

Explanation
In nearly 50% of patients with a unicameral bone cyst, the lesion remains asymptomatic until a fracture occurs, usually as the result of relatively minor trauma. If the lesion expands, the bone is weakened and may cause pain. Fibrous cortical defects are usually an incidental finding and typically asymptomatic. Malignant bone tumors such as osteosarcoma and Ewing's sarcoma most commonly cause pain, and pathologic fracture occurs in less than 10% of patients. Giant cell tumors are uncommon in children and usually are painful. Wilkins RM: Unicameral bone cysts. J Am Acad Orthop Surg 2000;8:217-224. Dormans JP, Pill SG: Fractures through bone cysts: Unicameral bone cysts, aneurysmal bone cysts, fibrous cortical defects, and nonossifying fibromas. Instr Course Lect 2002;51:457-467.
Question 393
High Yield
The parents of a 13-year-old boy with Down syndrome report that he has an increasing limp and decreased endurance with activities. Lateral flexion-extension radiographs of the cervical spine show no evidence of instability. Examination reveals a right Trendelenburg limp and an obvious limb-length discrepancy. Hip motion is symmetric except for some decreased abduction on the right side. A standing AP radiograph is shown in Figure 20. Management should consist of

Explanation
Ligamentous laxity and muscle hypotonia seen in Down syndrome contribute to the incidence of hip subluxation and dislocation. These factors can be progressive and lead to degenerative arthritis in adults with Down syndrome. Because this patient has a progressive limp and decreased endurance, observation and a shoe lift are not options. Bracing may be an option in the younger child before significant bony changes occur. Surgical intervention is the treatment of choice in this patient; however, all components of the deformity need to be addressed. Because of the increased capsular laxity, there is a high likelihood of recurrence if capsulorrhaphy is not included with the pelvic and femoral osteotomies. Surgery in these patients is associated with a high rate of complications. Shaw ED, Beals RK: The hip joint in Down's syndrome: A study of its structure and associated disease. Clin Orthop 1992;278:101-107. Aprin H, Zinc WP, Hall JE: Management of dislocation of the hip in Down's syndrome. J Pediatr Orthop 1985;5:428-431.
Question 394
High Yield
Figure 13a shows the radiograph of a 9-year-old girl who sustained complete transverse fractures of the radial and ulnar shafts while in-line skating. A manipulative closed reduction is performed, and the result is seen in Figure 13b. What is the next most appropriate step in management?


Explanation
Bayonet apposition of the radius and ulnar shafts is quite acceptable, as long as the angulation is less than 10 degrees. The rotation must be acceptable as well. This patient went on to full healing, with full supination and pronation of the forearm and no cosmetic deformity. Price CT, Scott DS, Kurzner ME, Flynn JC: Malunited forearm fractures in children. J Pediatr Orthop 1990;10:705-712.
Question 395
High Yield
Figure 24 shows the radiograph of a 47-year-old woman who has severe right hip pain and a limp. Management should consist of

Explanation
Femoral shortening osteotomy for a Crowe type IV hip dislocation has been shown to provide superior results with minimal complications. Cementless fixation of the stem allows for modular implants that greatly simplify the reconstruction.
Question 396
High Yield
Figure 29a shows the clinical photograph of a 26-year-old woman who has had the leg deformity since birth. She reports difficulty with walking and weight bearing and notes increased discomfort and swelling when the leg is dependent. She denies any history of trauma or family history of a similar disorder. Examination reveals a fixed equinovarus deformity of the foot but no evidence of a limb-length discrepancy. No other cutaneous findings or soft-tissue masses are noted. Sagittal and axial T1- and T2-weighted MRI scans are shown in Figures 29b and 29c. What is the most likely diagnosis?


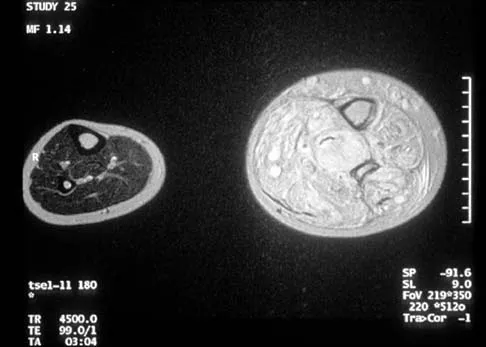
Explanation
Because the MRI scans show marked dilation and proliferation of lymphatic channels that completely involve all the leg muscles and the clinical photograph shows the severe swelling associated with this disease, the most likely diagnosis is lymphangiomatosis. Poliomyelitis affects the anterior horn cells and manifests as muscle atrophy. Neurofibromatosis can have a similar clinical appearance but usually is associated with other systemic and cutaneous findings. Congenital band syndrome results in amputated or shortened extremities. Chronic venous stasis disease usually is not associated with joint contractures, and typically it affects older individuals. Surgical excision is the only known treatment; this patient underwent an above-knee amputation. Berquist TH (ed): MRI of the Musculoskeletal System, ed 3. Philadelphia, PA, Lippincott Raven, 1997, p 771.
Question 397
High Yield
Figure 1 shows the radiograph of a 68-year-old man who underwent revision hip arthroplasty with impaction grafting of the femur and cementing of a tapered component into the graft 2 years ago. The patient remains symptom-free. Which of the following best describes the most likely histologic appearance of the proximal femur if a biopsy was performed?

Explanation
The radiograph shows three zones: an outer regenerated cortical layer, an interface zone consisting of viable trabecular bone and occasional particles of bone cement, and an inner layer of necrotic bone embedded in cement. No fibrous membrane is noted, and there is no direct contact of cement with native bone. Based on these findings, it is believed that the middle layer is the result of incorporation of the allograft with further remodeling. Nelissen RG, Bauer TW, Weidenhielm LR, LeGolvan DP, Mikhail WE: Revision hip arthroplasty with the use of cement and impaction grafting: Histological analysis of four cases. J Bone Joint Surg Am 1995;77:412-422.
Question 398
High Yield
A 52-year-old woman who underwent cheilectomy 1 year ago for hallux rigidus now reports continued pain in the first metatarsophalangeal joint. She did not have any incision healing problems, and has not had any fevers, erythema, or drainage. Which of the following procedures will provide the best combination of pain relief and function?

Explanation
All but the Moberg osteotomy are capable of providing pain relief; however, arthrodesis offers the best long-term results and restores weight bearing and propulsion function to the first ray. Machacek F Jr, Easley ME, Gruber F, et al: Salvage of a failed Keller resection arthroplasty. J Bone Joint Surg Am 2004;86:1131-1138.
Question 399
High Yield
Long bone fracture repair following intramedullary stabilization occurs primarily through which of the following healing mechanisms?

Explanation
The mechanical environment represents a major factor in the type of healing that occurs after a fracture. Intramedullary nail fixation allows for motion at the fracture site, which promotes bone formation both directly (intramembranous ossification) and through a cartilage intermediate (endochondral ossification). Absolute stability, as would be obtained with a compression plate, favors healing through the direct formation of bone without a cartilage intermediate (intramembranous ossification), or primary fracture repair. This type of healing would include the remodeling of the bone ends through the direct contact of bone, often referred to as contact healing or haversian remodeling. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 385-386.
Question 400
High Yield
A 12-year-old girl has had pain in her right knee for 1 month that started as activity-related and progressed to night pain. Radiographs are shown in Figures 16a and 16b, and a biopsy specimen is shown in Figure 16c. What is the recommended treatment?


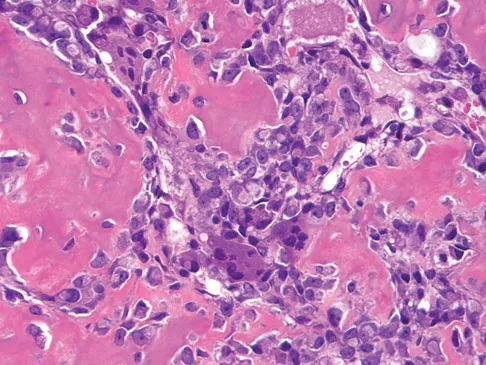
Explanation
This is a classic appearance for an osteosarcoma. The radiographs reveal a mixed osteolytic and osteoblastic lesion in a skeletally immature patient in the distal right femoral metaphysis. The pain pattern with progressive symptoms leading to the presence of night pain is also typical for this condition. The biopsy specimen reveals pleomorphic cells and the presence of osteoid. The current standard of care in the treatment of osteosarcoma is neoadjuvant chemotherapy followed by surgical resection or amputation followed by additional postoperative chemotherapy. Osteosarcoma is not radiosensitive. Wold LE, Adler CP, Sim FH, et al: Atlas of Orthopedic Pathology, ed 2. Philadelphia, PA, WB Saunders, 2003, p 179.
