HY 2026
00:00
Start Quiz
Question 201
High Yield
A 73-year-old man reports increasing back and lower extremity pain. A bone scan is shown in Figure 31. What is the most likely diagnosis?

Explanation
The bone scan reveals lesions throughout the skeleton. The patient's age, gender, and pain pattern are consistent with metastatic prostate cancer. Multiple myeloma typically does not have enough osteoblastic activity to produce this bone scan. The patient's age is not consistent with metastatic neuroblastoma (a pediatric disease). Polyostotic fibrous dysplasia may involve multiple active lesions in younger patients but does not have such a widespread distribution of lesions. Hodgkin's lymphoma can involve bone, but the widespread discrete appearance on this bone scan is most consistent with metastatic prostate cancer. In a patient with widespread bone metastases from prostate cancer, bisphosphonates may play a critical role in treatment by decreasing pain and the number of fractures. Roudier MP, Vesselle H, True LD, Higano CS, Ott SM, King SH, Vessella RL: Bone histology at autopsy and matched bone scintigraphy findings in patients with hormone refractory prostate cancer: The effect of bisphosphonate therapy on bone scintigraphy results. Clin Exp Metastasis 2003;20:171-180.
Question 202
High Yield
Where is the most common site for tuberculosis (TB) spondylitis in children?
Explanation
In children, the main route of infection in skeletal TB is through hematogenous spread from a primary source. The mycobacterium is deposited in the end arterials in the vertebral body adjacent to the anterior aspect of the vertebral end plate. Thus, the anterior portion of the vertebral body is most commonly involved. The lower thoracic region is the most common segment; next in decreasing order of frequency are the lumbar, upper thoracic, cervical, and sacral regions. Teo HE, Peh WC: Skeletal tuberculosis in children. Pediatric Radiol 2004;34:853-860.
Question 203
High Yield
Factors contributing to an increased risk of hip fracture include reduced bone mineral density of the femoral neck, cognitive status of the individual, and
Explanation
The etiology of hip fractures in the elderly is multifactorial, and intervention and prevention can occur at multiple points. Events leading to hip fracture from a fall include fall initiation (during which the individual's neuromuscular status, cognitive status, and vision come into play along with environmental hazards); fall descent (fall direction toward the side being the most influential, energy content of the fall, and fall height, along with muscle activity of the muscles of the thigh); impact (impact location, soft-tissue attenuation such as from trochanteric padding or from overlying fat, impact surface, and muscle activity); and the structural capacity of the femur (bone mineral density, bone geometry, and bone architecture). Hayes and Myers noted that striking the ground in a stiff state with the trunk muscles contracted actually increased the peak impact force, whereas falling in a relaxed state actually reduced peak impact force. Flexion of the trunk at impact had no bearing on the impact force. Direction of the fall was important; falls to the side, not forward, were associated with an increased risk of hip fracture. Increased muscle activity about the hip is thought to be associated with spontaneous fractures of the hip and may actually account for up to 25% of hip fractures; however, it is not related to fractures resulting from a fall.
Question 204
High Yield
Which of the following diagnostic studies best distinguishes Ewing's sarcoma from small cell osteosarcoma?

Explanation
Cytogenetics best demonstrates the 11;22 translocation characteristic of Ewing's sarcoma. The translocation also can be detected with polymerase chain reaction and fluorescent in situ hybridization. The Ewing antibody is used for immunostaining to check for cell membrane (surface) staining of a marker unrelated to the translocation; this could also help distinguish Ewing's sarcoma from small cell osteosarcoma. A bone scan will show increased uptake with both types of tumors. Although most Ewing's sarcoma tumors are diploid, some are polyploid as are most osteosarcomas. Flow cytometry is used to sort cells, sometimes based on antibody binding. LDH can be elevated in both Ewing's sarcoma and osteosarcoma and is a poor prognostic indicator when elevated. Lymph node metastases are uncommon in both of these tumors. Perotti D, Corletto V, Giardini R, Parafioriti A, Fossati-Bellani F, Luksch R: Retrospective analysis of ploidy in primary osseous and extraosseous Ewing family tumors in children. Tumori 1998;84:493-498. Riley RD, Burchill SA, Abrams KR, Heney D, Sutton AJ, Jones DR, et al: A systematic review of molecular and biological markers in tumours of the Ewing's sarcoma family. Eur J Cancer 2003;39:19-30.
Question 205
High Yield
A 23-year-old man is involved in a motor vehicle accident. An AP radiograph is shown in Figure 29a, and axial and sagittal CT scans are shown in Figures 29b and 29c. Neurologic examination shows 1/5 strength of his quadriceps and iliopsoas on the right, with 1/5 quadriceps function on the left. Definitive treatment of his injury should consist of


Explanation
The imaging studies show a fracture-dislocation. Surgical treatment of this injury consists of a decompression reduction, stabilization, and fusion. A posterolateral decompression can also be performed as necessary. An isolated anterior procedure in this type of injury is contraindicated. The anterior longitudinal ligament is most likely intact; therefore, an anterior procedure further destabilizes the spine. Reduction by an anterior approach would also be difficult. Nonsurgical management of the neurologic injury in this patient is not indicated. Theiss SM: Thoracolumbar and lumbar spine trauma, in Stannard JP, Schmidt AH, Kregor PJ (eds): Surgical Treatment of Orthopaedic Trauma. New York, NY, Thieme, 2007, pp 179-207.
Question 206
High Yield
A 58-year-old man has anterior knee pain after undergoing total knee arthroplasty for osteoarthritis 2 years ago. He denies any history of trauma. A Merchant view is shown in Figure 20. What is the most likely cause of his pain?
Explanation
The patient has a patellar stress fracture after resurfacing in a total knee arthroplasty. Several studies have shown that over-resection of the patella to less than 12 to 15 mm increases anterior patellar surface strains to a point where the risk of fracture is increased. Increasing the patellar thickness, positioning of the femoral component, lateral releases, and component types have not been clearly associated with increased fracture risk. Reuben JD, McDonald CL, Woodard PL, Hennington LJ: Effect of patella thickness on patella strain following total knee arthroplasty. J Arthroplasty 1991;6:251-258. Hsu HC, Luo ZP, Rand JA, An KN: Influence of patellar thickness on patellar tracking and patellofemoral contact characteristics after total knee arthroplasty. J Arthroplasty 1996;11:69-80.
Question 207
High Yield
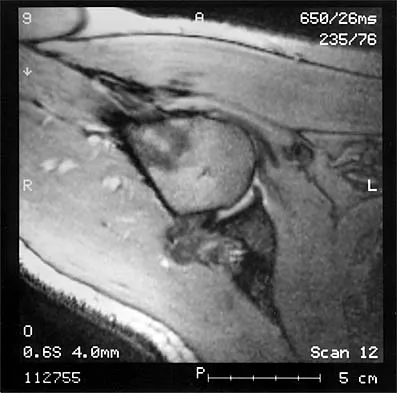
A 35-year-old patient has right hip pain. Figures 34a and 34b show the coronal MRI scan and the biopsy specimen. What is the most likely diagnosis?

Explanation
Alcohol abuse, steroids, Caisson disease, sickle cell disease, and radiation therapy are the leading causes of nontraumatic osteonecrosis of the femoral head. Arlet J: Nontraumatic avascular necrosis of the femoral head: Past, present, and future. Clin Orthop 1992;277:12-21.
Question 208
High Yield
Pain associated with a proximal medial tibial osteochondroma in a 10-year-old patient is most commonly the result of
Explanation
Pain secondary to an osteochondroma is usually from soft-tissue irritation and bursal formation. This is particularly common for proximal medial tibia osteochondromas that irritate the pes anserine tendons. Malignant degeneration into a chondrosarcoma rarely occurs, is usually associated with multiple hereditary exostoses, and usually occurs after skeletal maturity. Borges AM, Huvos AG, Smith J: Bursa formation and synovial chondrometaplasia associated with osteochondromas. Am J Clin Pathol 1981;75:648-653.
Question 209
High Yield
When conducted at near physiologic strain rates, tensile studies of the inferior glenohumeral ligament (IGHL) have shown that the
Explanation
Tensile testing of the inferior glenohumeral ligament at near physiologic strain rates has shown that the anterior band of the IGHL has the greatest stiffness of the three ligament regions and the glenoid insertion site shows greater strain than the ligament midsubstance. Bigliani LU, Pollock RG, Soslowsky LJ, Flatow EL, Pawluk RJ, Mow VC: Tensile properties of the inferior glenohumeral ligament. J Orthop Res 1992;10:187-197.
Question 210
High Yield
A patient with degenerative osteoarthritis of the sternoclavicular (SC) joint reports constant pain, discomfort, and marked prominence and instability of the SC joint following medial clavicle resection. Which of the following procedures is most likely to produce these signs and symptoms?
Explanation
Medial clavicle excision alone can be associated with postoperative instability of the clavicle. The clavicle should be stabilized to the first rib by reconstructing the costoclavicular ligament if it is torn or if the resection is lateral to its clavicular insertion. Therefore, care must be taken to resect only that part of the clavicle that is medial to the costoclavicular ligament. Adequate protection for vital structures that lie posterior to the medial end of the clavicle must be provided. Bremner RA: Nonarticular noninfected subacute arthritis of the sternoclavicular joint. J Bone Joint Surg Br 1959;41:749-753.
Question 211
High Yield
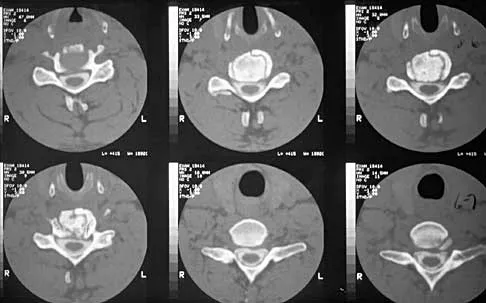
A 42-year-old woman is brought to the emergency department following a motor vehicle accident. She has sustained multiple injuries, and she is intubated and pharmacologically paralyzed. Sagittal cervical CT scans through the right cervical facets, the left cervical facets, and the midline are shown in Figures 12a through 12c, respectively. Definitive management of her cervical injury should consist of



Explanation
The CT scans reveal an occipital-cervical dissociation with subluxation of the occipitocervical joints bilaterally. Definitive management should consist of an occipital-cervical fusion with instrumentation. Immobilization in a Philadelphia collar is inadequate for this highly unstable injury, and halo immobilization, while affording adequate temporary immobilization, is not appropriate definitive management for this ligamentous injury. The patient does not have an injury at C4-C5 or C6-C7. Jackson RS, Banit DM, Rhyne AL III, et al: Upper cervical spine injuries. J Am Acad Orthop Surg 2002;10:271-280.
Question 212
High Yield
Which of the following is most commonly associated with an open clavicular fracture?

Explanation
Open clavicular fractures are rare and result from high-energy trauma. In a series of 20 patients with open clavicular fractures, 13 (65%) sustained a closed head injury. Fifteen (75%) had associated pulmonary injuries and 35% had a cervical or thoracic spine fracture. Only one demonstrated scapulothoracic dissociation. Screening for pulmonary and closed head injuries should be considered in the setting of traumatic open clavicular fractures.
Question 213
High Yield
A 43-year-old woman is referred after excisional biopsy of a cutaneous soft-tissue mass from her left shoulder. Based on the biopsy specimens shown in Figures 44a and 44b, what is the best course of action?
Explanation
Dermatofibrosarcoma protuberans (DFSP) is a rare superficial sarcoma that is frequently misdiagnosed at presentation. It is frequently excised prior to suspecting that the lesion is a sarcoma and if not appropriately treated with tumor bed resection to obtain wide margins, these lesions have a high incidence of local recurrence. It is recommended that the wide excision include the deep fascia and a 2.5- to 3-cm cuff of normal-appearing skin. Distant disease spread is rare and usually occurs in the face of a multiply recurrent lesion. Despite the apparent gross circumscription of these lesions, the tumor diffusely infiltrates the dermis and subcutaneous tissues. A characteristic histologic finding can be seen in the deep margins of the tumor where it intricately interdigitates with normal fat. Lindner NJ, Scarborough MT, Powell GJ, et al: Revision surgery in dermatofibrosarcoma protuberans of the trunk and extremities. Eur J Surg Oncol 1999;25:392-397.
Question 214
High Yield
A 67-year-old patient seen in the emergency department reports the acute onset of pain and is unable to ambulate. History reveals that the patient underwent surgical treatment for a periprosthetic femoral fracture 6 months ago. A radiograph is shown in Figure 41. What is the best treatment option at this time?

Explanation
The radiograph reveals a periprosthetic fracture at the tip of the stem with a stable cemented implant. This is classified as a Vancouver type B1 periprosthetic fracture. An attempt at internal fixation has already failed; therefore, the most predictable results would be achieved with distal fixation. After removal of the well-fixed cemented implant, the proximal bone may not be suitable for proximal fixation. Adequate bone stock is available such that an allograft prosthetic composite or a tumor prosthesis is not necessary. The best option is a long stem implant with distal fixation, which serves as an intramedullary device to restore alignment and increase the likelihood of union. Cortical onlay strut grafts are used as an adjunct to definitive fixation. Younger AS, Dunwoody I, Duncan CP: Periprosthetic hip and knee fractures: The scope of the problem. Inst Course Lect 1998;47:251-256.
Question 215
High Yield
The MRI scan shown in Figure 24 reveals a right-sided herniated nucleus pulposus at L4-5 in a patient with pain in the right leg. Administration of a caudal epidural steroid injection provides immediate relief. Over the next week he notes generalized weakness of the lower extremities and has one episode of urinary incontinence. What is the next most appropriate step in management?

Explanation
Whenever a patient's condition changes following a test or a procedure, the physician must determine the cause. A steroid flare reaction will not cause incontinence or weakness of the lower extremities. An L4-5 diskectomy may alleviate the problem if the right-sided L4-5 disk herniation is the etiology of the symptoms. However, it is unlikely that a right-sided disk herniation alone will cause a cauda equina syndrome. Possible etiologies include a further extrusion of a disk fragment at L4-5 that now obliterates the spinal canal, a disk herniation at another level, or an epidural abscess following injection of corticosteroids through a caudal approach. In the presence of a possible infection, myelography should not be performed from a lumbar puncture. The fastest and least invasive way to make an appropriate diagnosis is to obtain an MRI of the lumbar spine. In this patient, the MRI revealed an epidural abscess that was compressing the cauda equina. Because of the large dose of steroids that were injected, the patient did not manifest symptoms such as fevers and chills until late in the course. Knight JW, Cordingley JJ, Palazzo MG: Epidural abscess following epidural steroid and local anaesthetic injection. Anaesthesia 1997;52:576-578.
Question 216
High Yield
Talar compression syndrome in ballet dancers typically involves injury to which of the following structures?
Explanation
Talar compression syndrome is also known as os trigonum syndrome or posterior ankle impingement syndrome and occurs in activities involving extreme ankle plantar flexion. It involves pinching of the posterior talus (os trigonum or posterior process of the talus) between the calcaneus and tibia. The flexor hallucis longus also may be impinged. The other structures are not commonly injured in this syndrome. Brodsky AE, Khalil MA: Talar compression syndrome. Am J Sports Med 1986;14:472-476. Wredmark T, Carlstedt CA, Bauer H, Saartok T: Os trigonum syndrome: A clinical entity in ballet dancers. Foot Ankle 1991;11:404-406.
Question 217
High Yield
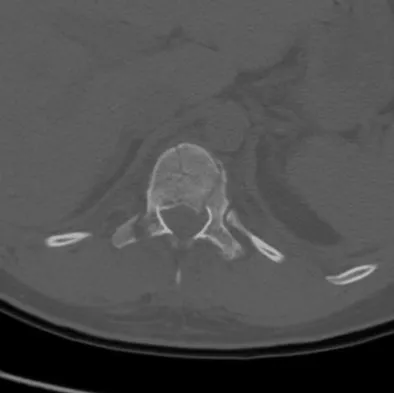
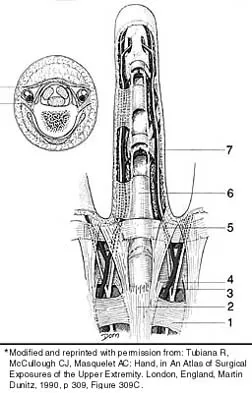
Figure 53 shows a thoracolumbar specimen as viewed from posterior to anterior following removal of all posterior elements. Which of the following structures does the red string pass under?
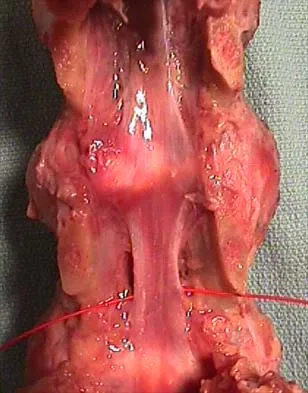
Explanation
The string passes under the ligamentum flavum as it runs from the posterior aspect of the vertebra above to the inferior aspect of the vertebra below in the sagittal midline. This is an important structure in diskectomy and in posterior approaches to the thoracolumbar spine and neural elements. It is rarely visualized in its entirety because typical exposures provide only a limited view.
Question 218
High Yield
A patient who was involved in a motor vehicle accident 2 weeks ago now reports neck pain. Work-up reveals no evidence of nerve root involvement or acute radiographic abnormality. The patient appears to have a hyperextension soft-tissue injury of the neck (whiplash). What is the best course of treatment at this time?

Explanation
Early mobilization and resumption of normal activities immediately after neck sprain has been shown to improve functional outcome and decrease subjective symptoms as measured 6 months after injury. Borchgrevink GE, Kaasa A, McDonagh D, Stiles TC, Haraldseth O, Lereim I: Acute treatment of whiplash neck injuries: A randomized trial during the first 14 days after a car accident. Spine 1998;23:25-31.
Question 219
High Yield
Which of the following design features of a femoral component used in a total knee arthroplasty best minimizes the patellar component contact stresses?
Explanation
Several studies have shown that design of the femoral component, especially the trochlear groove portion, largely influences patellar tracking and patellofemoral contact stresses. A deep, curved anatomic femoral trochlear groove has been shown to have the lowest contact stresses. Petersilge WJ, Oishi CS, Kaufman KR, Irby SE, Colwell CW Jr: The effect of trochlear design on patellofemoral shear and compressive forces in total knee arthroplasty. Clin Orthop 1994;309:124-130. Theiss SM, Kitziger KJ, Lotke PS, Lotke PA: Component design affecting patellofemoral complications after total knee arthroplasty. Clin Orthop 1996;326:183-187.
Question 220
High Yield
An infant is born with a mass that involves both the volar and dorsal compartments of the left arm. A clinical photograph and biopsy specimen are shown in Figures 41a and 41b. What is the best initial course of action?

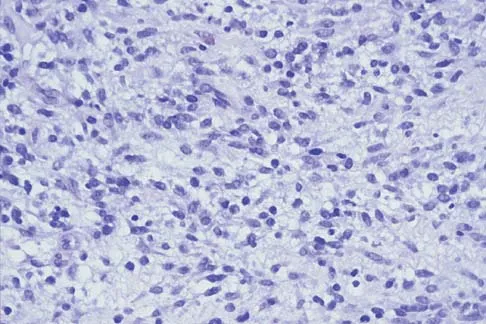
Explanation
The patient has infantile fibrosarcoma. For unresectable lesions, the treatment of choice is chemotherapy with vincristine, actinomycin-D, and cyclophosphamide, followed by excision if there is an adequate decrease in the size of the lesion.
Question 221
High Yield
A patient with a cobalt-chromium alloy (Co-Cr) femoral stem has a periprosthetic fracture that is to be fixed with a cable-plate device. The surgeon should make sure that the plate, screws, and cable, respectively, are made of
Explanation
Contact between metals in a biologic environment leads to galvanic corrosion. Reduction potentials of Co-Cr and stainless steel produce the worst combination of metals in commonly used implants. Because the fixation implants are not intended to contact the existing implant, it is not as great a consideration as the plate and the screws and cables that will directly contact each other. Miller MD (ed): Review of Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2000, pp 119-144.
Question 222
High Yield
During particle-induced osteolysis around implants, what cell secretes most of the interleukin-6 (IL-6)?
Explanation
During osteolysis, IL-6 is secreted by fibroblasts in the membrane surrounding the prosthesis. IL-6 also can be secreted by osteoblasts in other settings, but they are not the predominant source of IL-6 in particle-induced osteolysis. The remaining cells are not major sources of IL-6.
Question 223
High Yield
A patient who is an observant Jehovah's Witness requires major surgery for scoliosis that will likely result in significant blood loss. Which of the following might the patient consider allowing the surgical team to use?

Explanation
Jehovah's Witnesses will not accept the transfusion of blood or blood products such as packed red or white cells, platelets, or plasma. However, many Jehovah's Witnesses will accept the use of a cell saver in a "closed circuit." Jimenez R, Lewis VO (eds): Culturally Competent Care Guidebook. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2007.
Question 224
High Yield
Lumbar disk replacement has been shown to offer which of the following results?
Explanation
There is no clear evidence that disk replacement results in pain relief that is superior to fusion. Pain relief appears to be equivalent with these two procedures. No study has clearly demonstrated that normal segmental motion has been consistently restored. Preexisting facet arthropathy is considered to be a contraindication to disk replacement. Comparative long-term data demonstrating a reduced incidence of adjacent segment disease compared to fusion are not yet available. Geisler FH, Blumenthal SL, Guyer RD, et al: Neurological complications of lumbar artificial disc replacement and comparison of clinical results with those related to lumbar arthrodesis in the literature. J Neurosurg Spine 2004;1:143-154.
Question 225
High Yield
An intoxicated 68-year-old man fell at home. Examination reveals abrasions on his forehead, 2/5 weakness of his hand intrinsics and finger flexors, and 4/5 strength of the deltoid, biceps, and triceps bilaterally. Lower extremity motor function is 5/5. Sensory examination to pain and temperature is diminished in his hands but intact in his lower extremities. Deep tendon reflexes are depressed in all four extremities, but perianal sensation and rectal tone are intact. Foley catheterization yields 700 mL of urine. Radiographs of the cervical spine reveal multilevel spondylosis without fracture or subluxation. An MRI scan reveals high-intensity signal change within the cord substance at C5. What is the most likely diagnosis?

Explanation
Central cord syndrome is characterized by greater neurologic involvement of the upper extremities than the lower extremities. This is typically seen in older patients with cervical spondylosis without associated bony injury or joint subluxation. The prognosis for recovery is fair. Patients with Brown-Sequard syndrome have an ipsilateral motor deficit and contralateral loss of pain and temperature. Prognosis for recovery depends on the mechanism of injury, which is often of a penetrating nature. Anterior cord syndrome results from anterior compression such as occurs with a burst or teardrop fracture of the vertebral body; patients have bilateral motor loss, pain, and temperature loss with preservation of proprioception and vibratory sensation (posterior column function). The prognosis for recovery is generally poor. Posterior cord syndrome is rare and is associated with loss of posterior column function (proprioception and vibration). Northrup BE: Evaluation and early treatment of acute injuries to the spine and spinal cord, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott-Raven, 1998, pp 541-549.
Question 226
High Yield
A 9-year-old boy falls from a scooter and sustains the injury shown in the radiographs in Figure 26. After closed reduction and cast immobilization, what is the most likely complication that can result?

Explanation
The radiographs show a fracture of the distal radius and ulna physis. The most likely complication is growth arrest of the distal ulna. In contradistinction to physis fractures of the radius (growth arrest incidence of less than 5%), the incidence of growth arrest in the ulna is between 30% and 40%. Entrapment of the EPL tendon and cross union between the two bones is extremely rare. Vanheest A: Wrist deformities after fracture. Hand Clin 2006;22:113-120. Cannata G, De Maio F, Mancini F, et al: Physeal fractures of the distal radius and ulna: Long-term prognosis. J Orthop Trauma 2003;17:172-179. Ray TD, Tessler RH, Dell PC: Traumatic ulnar physeal arrest after distal forearm fractures in children. J Pediatr Orthop 1996;16:195-200.
Question 227
High Yield
A 10-year-old child with cerebral palsy undergoes bilateral hamstring lengthening for severe knee flexion contractures, and knee immobilizers are applied postoperatively. Examination at the initial postoperative check 2 hours after surgery reveals that she can dorsiflex her toes on the right foot, but not on the left foot. The physician should now
Explanation
Children with cerebral palsy are often difficult to examine. However, this patient clearly has a peroneal nerve deficit, most likely from the acute stretch after the hamstring lengthening. The nerve has the best chance of recovery if it is relaxed by flexing the knee. Once the nerve has recovered, gradual knee extension can be accomplished. Aspden RM, Porter RW: Nerve traction during correction of knee flexion deformity: A case report and calculation. J Bone Joint Surg Br 1994;76:471-473.
Question 228
High Yield
Figure 19 shows the radiograph of a 12-year-old boy who sustained an injury to his hand when another child fell on him. Management should consist of

Explanation
The patient has a Salter-Harris type III fracture of the proximal phalanx of the thumb. It is usually caused by an abduction injury where the ulnar collateral ligament avulses a fragment away from the proximal epiphysis and is the most common childhood gamekeeper's injury. If there is greater than 1 mm of separation or a significant articular step-off, an open reduction, performed through an extensor aponeurosis-splitting approach, is required to reestablish joint congruity and stability. Percutaneous or closed methods of reduction are usually ineffective. The dorsal approach avoids the volar neurovascular structures. Since the ulnar collateral ligament is still attached, this area does not need to be visualized. The major goal is to reestablish joint congruity and bony stability. This can be easily performed via the dorsal approach. Carey TP: Fracture and dislocations of the phalanges, in Letts RM (ed): Management of Pediatric Fractures. New York, NY, Churchill Livingstone, 1994, pp 435-436.
Question 229
High Yield
What is the optimum position of immobilization of the foot and ankle immediately after Achilles tendon repair to maximize skin perfusion?
Explanation
Achilles tendon tension is not affected by knee position when the ankle is in 20 degrees to 25 degrees of plantar flexion. Skin perfusion overlying the Achilles tendon is maximal in 20 degrees of plantar flexion and is reduced beyond 20 degrees of plantar flexion. Neutral flexion or any amount of dorsiflexion compromises the repair.
Question 230
High Yield
A teenager is undergoing a correction of deformity and lengthening of the femur. Distractions are proceeding as expected; however, during his 6-week follow-up examination, the patient reports that the distraction motors have become harder to turn over for the past 2 to 3 days. Figures 37a and 37b show current radiographs. What is the most likely complication being encountered?
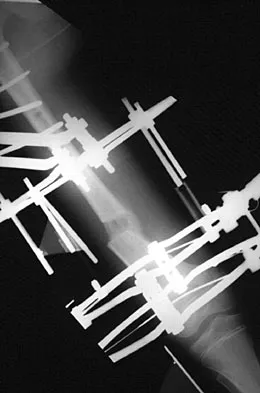
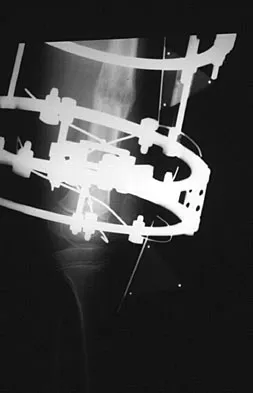
Explanation
Premature consolidation is a complication that is unique to gradual bone lengthening after corticotomy. Causes include excessive latency period, inadequate distraction rate, exuberant bone formation, patient compliance problems, and mechanical failure of the distraction apparatus. The femur and fibula are most commonly involved. This patient did not have an incomplete corticotomy, as initial distraction occurred before the distraction device was noted to seize up. The radiographs show bowing of the Ilizarov wires and mature regenerate bone, both suggestive of premature consolidation. No wire breakage or joint subluxation is seen on the radiographs. Treatment for premature consolidation includes continuing distraction until the consolidation bridge ruptures, or additional surgery may include closed rotational osteoclasis or repeat corticotomy. Paley D: Problems, obstacles and complications of limb lengthening, in Maiocchi AB, Aronson J (eds): Operative Principles of Ilizarov. Baltimore, MD, Williams & Wilkins, 1991, p 360.
Question 231
High Yield
A 32-year-old woman has an isolated left posterior wall acetabular fracture in which about 25% of the wall surface is involved. Which of the following criteria would indicate the need for surgical reduction and fixation?
Explanation
Fractures with a posterior wall fragment that makes up less than one third of the surface generally are stable. Conversely, fractures with a fragment making up more than 50% of the surface are unstable. Patients with an intermediate fracture fragment should undergo a fluoroscopic examination under sedation or anesthesia to determine if the fragment is truly stable. If so, the patient can be treated nonoperatively and safely mobilized. Tornetta P III: Non-operative management of acetabular fractures: The use of dynamic stress views. J Bone Joint Surg Br 1999;81:67-70.
Question 232
High Yield
Which of the following prognostic indicators is associated with the least favorable outcome for patients newly diagnosed with osteosarcoma?
Explanation
Distant bone metastasis is associated with an extremely poor prognosis for patients with osteosarcoma (5-year survival rate of less than 10%). Most osteosarcomas are high grade and extracompartmental, and approximately half are greater than 8 cm at presentation. The 5-year survival rate for these patients is approximately 70%. Patients with a solitary pulmonary metastasis have a prognosis worse than patients without detectable metastases but not as bad as those with bone metastases. Bielack SS, Kempf-Bielack B, Delling G, et al: Prognostic factors in high-grade osteosarcoma of the extremities or trunk: An analysis of 1,702 patients treated on neoadjuvant cooperative osteosarcoma study group protocols. J Clin Oncol 2002;20:776-790. Heck RK, Stacy GS, Flaherty MJ, et al: A comparison study of staging systems for bone sarcomas. Clin Orthop Relat Res 2003;415:64-71.
Question 233
High Yield
Which of the following conditions is transmitted by an autosomal dominant trait?
Explanation
Multiple hereditary exostosis is transmitted by an autosomal dominant trait. Li-Fraumeni syndrome and retinoblastoma are autosomal recessive or associated with autosomal recessive mutations. No genetic predisposition to Ollier's disease or Maffucci's syndrome has been identified. Mirra J (ed): Bone Tumors: Clinical, Radiologic and Pathologic Correlations. Philadelphia, PA, Lea and Febiger, 1989, p 1627.
Question 234
High Yield
Figures 10a and 10b show the radiographs of a 47-year-old man who reports pain in both shoulders. He has a history of leukemia that was treated with chemotherapy and high-dose cortisone. What is the most reliable treatment option for pain relief in this patient?


Explanation
The radiographs reveal osteonecrosis with collapse. The most reliable and durable treatment for osteonecrosis of the humeral head remains prosthetic shoulder arthroplasty. Osteonecrosis of the humeral head may be seen after the use of steroids, and there is an increasing demand for shoulder arthroplasty in young people because of the use of high-dose steroids in chemotherapy regimes for the treatment of malignant tumors. The indications for most shoulder arthrodeses today include posttraumatic brachial plexus injury, paralytic disorders in infancy, insufficiency of the deltoid muscle and rotator cuff, chronic infection, failed revision arthroplasty, severe refractory instability, and bone deficiency following resection of a tumor in the proximal aspect of the humerus. Clearly, the role of arthroscopy and related minimally invasive techniques in the treatment of humeral head osteonecrosis remains unknown. Hasan SS, Romeo AA: Nontraumatic osteonecrosis of the humeral head. J Shoulder Elbow Surg 2002;11:281-298. Hattrup SJ: Indications, technique, and results of shoulder arthroplasty in osteonecrosis. Orthop Clin North Am 1998;29:445-451.
Question 235
High Yield
What is the most important consideration in the preoperative evaluation of a child with polyarticular or systemic juvenile rheumatoid arthritis (JRA)?

Explanation
The cervical spine may be involved in a child with polyarticular or systemic JRA; fusion or instability can occur. Radiographic assessment of the cervical spine should include lateral flexion-extension views. The potential exists for spinal cord injury during intubation or positioning in the presence of an unstable cervical spine. Limitations of the TMJ and micrognathia may affect ease of intubation and administration of anesthesia via a mask. If the TMJ and jaw are involved, some patients may have dental findings such as dental caries and even abscesses which can affect surgery. Some children, particularly those with systemic arthritis, may be taking corticosteroids long-term and may need stress dosing with complex surgeries. Although it is important to routinely check for uveitis and iritis in children with JRA, this usually is not needed preoperatively. Uveitis and iritis are less likely in a child with systemic JRA. Cassity JT, Petty RE (eds): Textbook of Pediatric Rheumatology, ed 5. Philadelphia, PA, WB Saunders, 2005. Ilowite N: Current treatment of juvenile rheumatoid arthritis. Pediatrics 2002;109:109-115. Ruddy S, Harris ED, Sledge CB (eds): Kelley's Textbook of Rheumatology, ed 6. Philadelphia, PA, WB Saunders, 2001.
Question 236
High Yield
What is the most consistent finding regarding glenohumeral kinematics in patients with symptomatic tears of the rotator cuff?
Explanation
Normal glenohumeral kinematics are represented by ball-and-socket modeling when the rotator cuff is intact. This is true for motion that involves more than 30 degrees of abduction. In patients with shoulder pain and symptomatic rotator cuff tears, superior translation occurs with abduction beyond 30 degrees. This is quite evident in massive tears but is seen consistently to a lesser degree with smaller tears. Yamaguchi K, Sher JS, Anderson WK, et al: Glenohumeral motion in patients with rotator cuff tears: A comparison of asymptomatic and symptomatic shoulders. J Shoulder Elbow Surg 2000;9:6-11.
Question 237
High Yield
In surgically treating hand and finger infections in patients with diabetes mellitus, what factor is associated with higher amputation rates?
Explanation
Patients with diabetes mellitus are prone to infection, and surgical treatment of their infections frequently requires multiple procedures. The triad of poor wound healing, chronic neuropathy, and vascular disease contributes to the increased infection rate. Studies have demonstrated increased amputation rates in patients with diabetes mellitus who have renal failure or deep polymicrobial or gram-negative infections. Gonzalez MH, Bochar S, Novotny J, et al: Upper extremity infections in patients with diabetes mellitus. J Hand Surg Am 1999;24:682-686. Trumble TE (ed): Hand Surgery Update 3: Hand, Elbow, & Shoulder. Rosemont, IL, American Society for Surgery of the Hand, 2003, pp 433-457.
Question 238
High Yield
Following resection of malignant tumors, complications related to endoprosthetic reconstruction are most common in what anatomic location?
Explanation
It is generally accepted that reconstructions of the proximal tibia are associated with the highest incidence of failure, probably because of poor soft-tissue coverage, the need for extensor mechanism reconstruction, and other anatomic issues. It also may be related to the fact that patients with tumors of the proximal tibia, in general, have a better prognosis and better survival rates than patients with tumors located elsewhere in the body. Reconstructions of the proximal humerus may be more durable because they are not involved in weight-bearing activities.
Question 239
High Yield
A 45-year-old man underwent unipolar hemiarthroplasty reconstruction using cementless fixation for nontraumatic osteonecrosis of the femoral head 5 years ago. He now reports buttock and groin pain that is associated with loading activities. What is the most likely cause of his pain?
Explanation
One of the most common complications of hemiarthroplasty is acetabular cartilage degeneration, resulting in increasing pain. Conversion total hip arthroplasty generally is successful with placement of an acetabular cup. Additionally, many patients with osteonecrosis already have degenerative changes of the acetabular cartilage even though radiographic findings may appear normal. Steinberg ME, Corces A, Fallon M: Acetabular involvement in osteonecrosis of the femoral head. J Bone Joint Surg Am 1999;81:60-65.
Question 240
High Yield
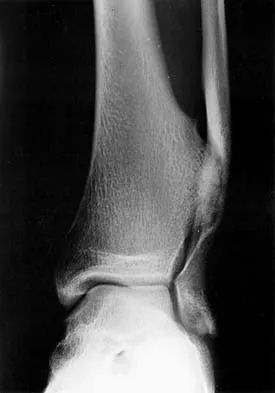
A 46-year-old man fell 20 feet and sustained the injury shown in Figure 3. The injury is closed; however, the soft tissues are swollen and ecchymotic with blisters. The most appropriate initial management should consist of

Explanation
Although this is a fracture of the medial and lateral malleoli, the degree of displacement and comminution of the medial dome indicate that this injury is similar to a pilon fracture. Initial management should consistent of stabilization to allow for soft-tissue healing. The use of temporizing spanning external fixation should be the initial step, followed by limited or more extensive open reduction and internal fixation when the soft-tissue status will allow. Initial placement in either a short or long leg cast does not provide the needed stability and does not allow for care and monitoring of soft tissues. In addition, maintaining reduction of the talus may be very difficult. Immediate open reduction and internal fixation through an injured soft-tissue envelope adds the risk of difficulties with incision healing and a higher risk of deep infection. In the acute setting, a primary ankle fusion through this soft-tissue envelope is not indicated. Marsh JL, Bonar S, Nepola JV, et al: Use of an articulated external fixator for fractures of the tibial plafond. J Bone Joint Surg Am 1995;77:1498-1509. Wyrsch B, McFerran MA, McAndrew M, et al: Operative treatment of fractures of the tibial plafond: A randomized, prospective study. J Bone Joint Surg Am 1996;78:1646-1657.
Question 241
High Yield
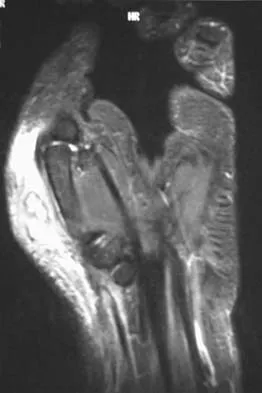
A 17-year-old girl who initially presented as a child with multiple skeletal lesions, café-au-lait spots, and precocious puberty now has bone pain. A recent bone scan reveals multiple areas of increased scintigraphic uptake, including bilateral proximal femurs. A radiograph is shown in Figure 19. Besides activity modification, what is the next best line of treatment for decreasing her pain?

Explanation
McCune-Albright syndrome is the combination of polyostotic fibrous dysplasia, café-au-lait lesions, and endocrine dysfunction. The most common endocrine presentation is precocious development of secondary sexual characteristics. Compared with bone lesions in patients without polyostotic disease, the skeletal lesions in patients with the syndrome tend to be larger, more persistent, and associated with more complications. Bisphosphonate therapy has been shown in several studies to decrease the pain associated with the skeletal lesions of fibrous dysplasia. DiCaprio MR, Enneking WF: Fibrous dysplasia: Pathophysiology, evaluation and treatment. J Bone Joint Surg Am 2005;87:1848-1864.
Question 242
High Yield
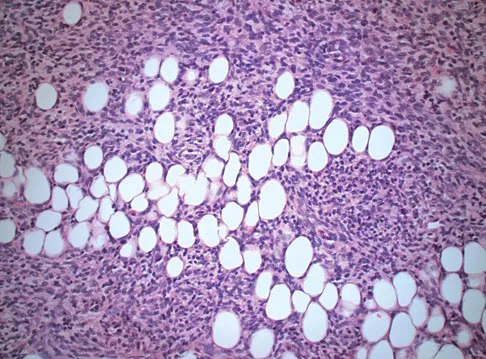
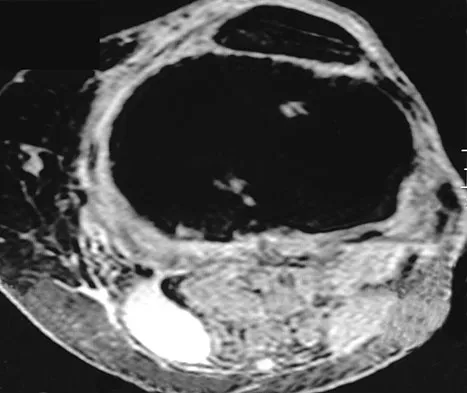
An 18-year-old man has had an enlarging mass in his hand for the past 3 months. Radiographs, an MRI scan, and biopsy specimens are shown in Figures 54a through 54d. What is the most likely diagnosis?

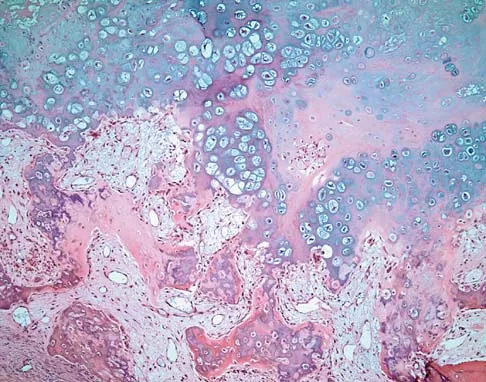
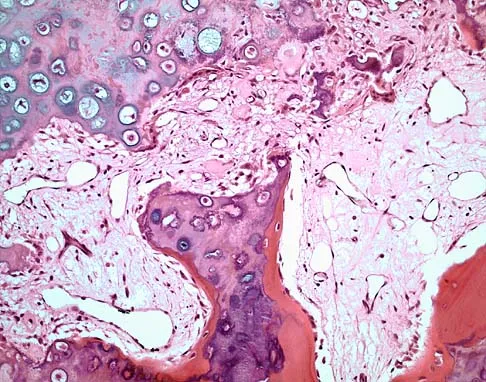
Explanation
Also known as Nora's lesion, BPOP is a benign osteocartilaginous tumor that almost always occurs in the hands and feet; one occurrence each in the femur and tibia has been reported. Although local recurrence is common after excision, metastases have not been reported. Abramovici L, Steiner GC: Bizarre parosteal osteochondromatous proliferation (Nora's lesion): A retrospective study of 12 cases, 2 arising in long bones. Hum Pathol 2002;33:1205-1210.
Question 243
High Yield
Following application of a short leg cast, a patient reports a complete foot drop. A compression injury of the peroneal nerve at the fibular neck is confirmed by electrical studies. Which of the following muscles is expected to be the last to recover function during the ensuing months?
Explanation
The recovery process from peroneal nerve palsy may take many months as axonal regrowth occurs. Of the muscles listed, the extensor hallucis is innervated most distally by the peroneal nerve. The flexor digitorum longus is innervated by the tibial nerve.
Question 244
High Yield
Use of prophylactic knee bracing in contact sports participants results in which of the following?

Explanation
Several studies have looked at the effects of knee bracing, and it appears to be effective in prophylactically decreasing the incidence of medial collateral ligament sprains. Najibi and Albright reported that although evidence is not conclusive, bracing appears to help decrease the incidence of medial collateral ligament injuries. Albright and associates showed similar findings. Prophylactic knee braces have been associated with an increased incidence of ankle injuries. Albright JP, Powell JW, Smith W, et al: Medial collateral ligament knee sprains in college football: Effectiveness of preventive braces. Am J Sports Med 1994;22:12-18.
Question 245
High Yield
What clinical finding is associated with the least favorable prognosis in an adolescent patient who has been diagnosed with a high-grade osteosarcoma of the distal femur?

Explanation
The presence of synchronous bone disease in young patients carries a dismal prognosis, one that is even worse than the presence of resectable pulmonary metastasis. Many osteosarcomas cross the physis; therefore, this has not been shown to be of prognostic importance. Similarly, the presence of the soft-tissue mass has less prognostic significance.
Question 246
High Yield
The management of a complex multifragmentary diaphyseal fracture of either the tibia or femur has changed during the last decade. Which of the following principles of treatment is now considered less important?

Explanation
Although the original concept of internal fixation was one of anatomic reduction and stable fixation, over the past 10 to 15 years there has been a change based on the advent of intramedullary nailing and bridge plating. It is now appreciated that in a multifragmentary diaphyseal fracture, particularly of the lower extremity, the achievement of axis alignment (mechanical and anatomic axis) is all that is required. Healing will occur by callus. Relatively stable fixation is achieved through intramedullary nailing or bridge plating, providing adequate pain relief for functional aftercare. Perren SM, Claes L: Biology and mechanics of fracture management, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 7-32. deBoer P: Diaphyseal fractures: Principles, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 93-104.
Question 247
High Yield
What bilateral surgical intervention is considered inappropriate based on the findings shown in the radiograph in Figure 52?

Explanation
The radiograph reveals osteonecrosis of both femoral heads with reasonably maintained joint surfaces. There may be some slight flattening of the femoral heads. Hip arthrodesis is difficult to perform because of the necrotic bone. Its use in patients with osteonecrotic hips is limited because of the 80% bilaterality; therefore, it is not an acceptable alternative. All the other options are acceptable interventions. Mont MA, Jones LC, Sotereanos DG, et al: Understanding and treating osteonecrosis of the femoral head. Instr Course Lect 2000;49:169-185.
Question 248
High Yield
A soccer player who sustained a twisting injury to the right ankle while making a cut is unable to bear weight and has diffuse tenderness over the anterior and lateral aspects of the ankle. Examination also shows a positive squeeze test. Plain radiographs and a stress radiograph are shown in Figures 26a through 26c. Radiographs of the leg and knee are normal. What is the most appropriate management?



Explanation
The mechanism of injury, physical examination, and radiographs indicate a "high" ankle sprain with disruption of the distal tibiofibular ligaments and interosseous membrane. These injuries typically involve pronation and external rotation forces. In addition, recovery is significantly delayed, often requiring 6 to 8 weeks to heal. Radiographs obtained months after recovery often show calcification within the distal syndesmosis, which is not typically symptomatic. This patient has gross instability, resulting in a high incidence of chronic diastasis and subluxation leading to impaired function. Treatment should consist of reduction and stabilization with a transsyndesmotic screw because this injury demonstrates a widened syndesmosis. Boytim MJ, Fisher DA, Neumann L: Syndesmotic ankle sprains. Am J Sports Med 1991;19:294-298.
Question 249
High Yield
Ewing's sarcoma of bone most commonly occurs in which of the following locations?
Explanation
Ewing's sarcoma typically occurs in the major long tubular bones, with the femur the most common location. The flat bones of the pelvis are the second most common location. Ewing's sarcoma occurs in the fibula but with a lower incidence than that seen in the major tubular bones. Ewing's sarcoma infrequently occurs in the metacarpals or the vertebral bodies. Simon M, Springfield D, et al: Ewing's Sarcoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 287.
Question 250
High Yield
Overgrowth of a limb in a patient with neurofibromatosis type 1 (NF1) is most likely associated with the presence of
Explanation
Plexiform neurofibromas are lesions found in patients with NF1. Clinical reports show the prevalence of plexiform neurofibroma to be 20% to 30% but increases to 40% when imaging studies are routinely obtained. The lesions are characterized by diffuse hypertrophy of the involved nerves but with preservation of the nerves' fascicular organization. The lesions may involve the dermis or may arise in the deeper structures. Palpation of a dermal lesion provokes an image of a "bag of worms." Plexiform neurofibromas may cause disfigurement and hyperpigmentation of the overlying skin. The lesions also can cause diffuse hypertrophy of the soft tissue and bone, with resultant changes ranging from a relatively minor limb-length discrepancy to gigantism of the entire extremity. Dural ectasia is frequently found in patients with NF1. Therefore, MRI should be obtained prior to planning spinal procedures in these patients; however, dural ectasia is not the cause of limb overgrowth. Lisch nodules are benign hamartomas of the iris. The lesions are uncommon during early childhood but are found in all adults with NF1. Juvenile xanthogranuloma has a low occurrence rate in patients with NF1; its presence is associated with juvenile chronic myeloid leukemia. Malignant peripheral nerve sheath tumors, formally called neurofibrosarcoma, result from malignant degeneration of a plexiform neurofibroma. This condition occurs in up to 4% of patients with NF1. Localized pain, an enlarging mass, or progressive neurologic symptoms suggest a malignant peripheral nerve sheath tumor in a patient with NF1. However, progressive neurologic symptoms also may occur with benign growth of a plexiform neurofibroma. Alman BA, Goldberg MJ: Syndromes of orthopaedic importance, in Morrissy RT, Weinstein SL (eds): Lovell and Winter's Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 287-338.
Question 251
High Yield
Which of the following properties primarily provides the excellent corrosion resistance of metallic alloys such as stainless steel and cobalt-chromium-molybdenum?
Explanation
All of the metals and metallic alloys used in orthopaedic surgery obtain their corrosion resistance from an adherent oxide layer. For stainless steel and cobalt alloy, the addition of chromium as an alloying element ensures the formation of a chromium oxide passive layer that forms on the surface and separates the bulk material from the corrosive body environment. Titanium alloy achieves the same result without chromium by forming an adherent passive layer of titanium oxide. Although these layers can indeed be hard, hardness does not in and of itself provide corrosion resistance. Adding nickel to both metallic alloys adds to strength but does not influence corrosion resistance appreciably. Galvanic potential can influence corrosion but does so by differences in potential between two contacting materials; for example, stainless steel and cobalt alloy have substantially different potentials, and if they were in contact within an aqueous environment, corrosion would commence with the stainless steel becoming the sacrificial anode. Metallic carbides are important in strengthening the alloys but have no role in providing corrosion resistance. Williams DF, Williams RL: Degradative effects of the biological environment on metal and ceramics, in Ratner BD, Hoffman AS, Shoen FJ, et al (eds): Biomaterials Science. San Diego, CA, Academic Press, 1996, pp 260-265. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 190-193.
Question 252
High Yield
When treating osteoporosis with alendronate, what is the most common side effect?
Explanation
Alendronate is a second-generation bisphosphonate, and it can cause epigastric distress in up to 30% of patients. This side effect can be minimized by gradually building up to therapeutic doses over a period of 4 to 8 weeks. Marshall JK, Rainsford KD, James C, et al: A randomized controlled trial to assess alendoronate-associated injury of the upper gastrointestinal tract. Aliment Pharmacol Ther 2000;14:1451-1457.
Question 253
High Yield
What is the best initial screening test for a patient with a limb-length discrepancy?

Explanation
With the patient standing, add blocks under the short leg until the pelvis is level, then measure the blocks to determine the discrepancy. This method is an accurate, simple, and inexpensive way to assess limb-length discrepancy. Differences of less than 2 cm need no treatment. Increasing discrepancy in a growing child should be followed clinically. Radiographic examination can include scanography, CT scanography, or a standing pelvic radiograph with the pelvis leveled. CT scanography is the most accurate diagnostic test when hip, knee, or ankle contractures are present. Herring JA: Tachdjian's Pediatric Orthopedics, ed 4. Philadelphia, PA, WB Saunders, 2002, pp 1041-1045. Schoenecker PL, Rich MM: The lower extremity, in Morrissy RT, Weinstein SL (eds): Lovell and Winter's Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 1120-1122. Stanitski DF: Limb-length inequality: Assessment and treatment options. J Am Acad Orthop Surg 1999;7:143-153.
Question 254
High Yield
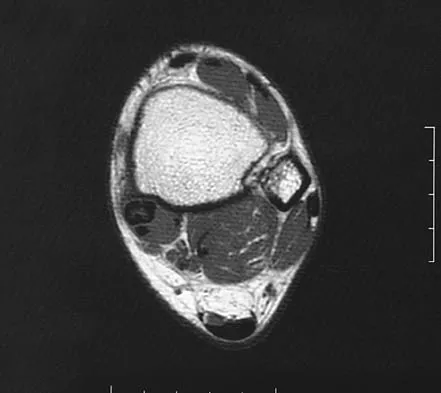
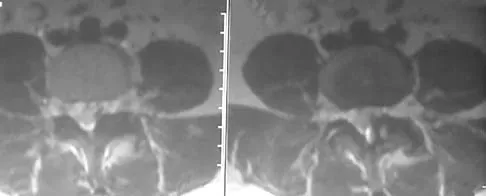
An 80-year-old woman notes a painless mass posterior to her left knee. MRI scans are shown in Figures 31a and 31b. What is the best course of action?
Explanation
The MRI scans show a popliteal cyst (Baker's cyst) in its most common location. The cyst emerges from the knee joint between the medial head of the gastrocnemius muscle and the tendon of the semimembranosus muscle. These images are diagnostic; therefore, no further work-up is indicated. Since the patient is asymptomatic, no treatment is necessary. Dlabach JA: Nontraumatic soft tissue disorders, in Canale ST (ed): Campbell's Operative Orthopaedics, ed 10. Philidelphia, PA, Mosby, 2003, vol 1, pp 885-969.
Question 255
High Yield
A 58-year-old man with type 1 diabetes mellitus is seen in the emergency department and he reports a 3-day history of a red swollen foot but no history of trauma. Examination reveals that the skin is intact, and the patient has discomfort with passive range of motion at the ankle, hindfoot, and midfoot joints. He denies any fever. Laboratory studies show a WBC count of 7,800/mm3, an erythrocyte sedimentation rate of 40 mm/h, a C-reactive protein level of 23, and a serum glucose of 100. A radiograph and MRI scans are shown in Figures 16a through 16c. What is the next most appropriate step in management?

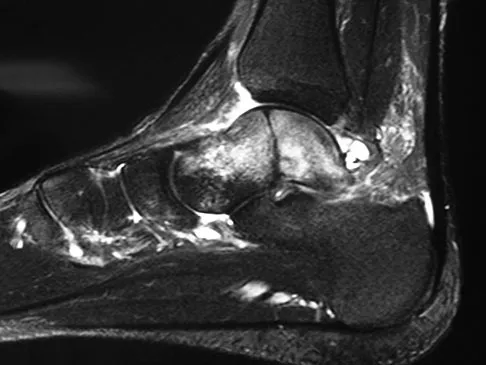
Explanation
Whereas it is difficult to distinguish between cellulitis, septic joint, osteomyelitis, and early Eichenholtz stage 1 Charcot, the presence of a fracture in the absence of ulcerations with a normal WBC count and serum glucose strongly indicates that the described symptoms are due to an early Charcot process alone. A technetium Tc 99m scan alone would not be helpful; however, the addition of a sulfur colloid marrow scan or indium In 111 scan may be more specific to rule out infection, though it is not warranted here. Total contact casting with non-weight-bearing or limited weight bearing during Eichenholtz stage 1 when the foot is warm, erythematous, and swollen is advised to help prevent deformity. Alternatively, stabilization with pneumatic bracing may also be considered. While some authors have proposed early fixation or arthrodesis for Eichenholtz stage 1, the gold standard is still total contact casting with no to limited weight bearing until the swelling resolves and evidence of consolidation is seen on radiographs. Trepman E, Nihal A, Pinzur MS: Current topics review: Charcot neuropathy of the foot and ankle. Foot Ankle Int 2005;26:46-63. Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2003, pp 123-134.
Question 256
High Yield
A 20-year-old man sustained a closed tibial fracture and is treated with a reamed intramedullary nail. What is the most common complication associated with this treatment?

Explanation
The most common complication is anterior knee pain (57%). The knee pain is activity related (92%) and exacerbated by kneeling (83%). Although knee pain is the most common complication, most patients rate it as mild to moderate and only 10% are unable to return to previous employment. Some authors report less knee pain with a peritendinous approach when compared to a tendon-splitting approach. In one study, nail removal resolved pain in 27%, improved it in 70%, and made it worse in 3%. The incidence of the other complications was: infection 0% to 3%, nonunion 0% to 6%, and malunion 2% to 13%. Compartment syndrome is rare after nailing. Court-Brown CM: Reamed intramedullary tibial nailing: An overview and analysis of 1106 cases. J Orthop Trauma 2004;18:96-101. McQueen MM, Gaston P, Court-Brown CM: Acute compartment syndrome: Who is at risk? J Bone Joint Surg Br 2000;82:200-203.
Question 257
High Yield
A 32-year-old man who works as a laborer has had left trapezius wasting and lateral scapular winging after injuring his shoulder when a cargo box fell onto his neck 8 months ago. He now reports posterior shoulder pain and fatigue, and he has difficulty shrugging his shoulder. Examination reveals marked scapular winging, impingement signs, and an asymmetrical appearance when the patient attempts a shoulder shrug. Primary scapular-trapezius winging is the result of damage to the

Explanation
The patient has primary scapular-trapezius winging. This condition can be caused by blunt trauma to the relatively superficial spinal accessory nerve that is located in the floor of the posterior cervical triangle in the subcutaneous tissue. Other causes of injury include penetrating trauma, traction, or surgical injury. With trapezius winging, the shoulder appears depressed and laterally translated because of an unopposed serratus anterior. This contrasts with primary serratus anterior winging, which is caused by injury to the long thoracic nerve. In this condition, the scapula assumes a position of superior elevation and medial translation, and the inferior angle is rotated medially. The thoracodorsal nerve supplies the latissimus dorsi and is not involved in primary scapular winging. Kuhn JE, Plancher KD, Hawkins RJ: Scapular winging. J Am Acad Orthop Surg 1995;3:319-325.
Question 258
High Yield
A 25-year-old man is unresponsive at the scene of a high-speed motor vehicle accident and remains obtunded. Initial evaluation in the emergency department reveals a left-sided femoral shaft fracture and a right-sided humeral shaft fracture. The cervical spine remains immobilized in a semi-rigid cervical collar, and the initial AP and lateral radiographs obtained in the emergency department are unremarkable. What is the most appropriate management at this time?
Explanation
Clearance of the cervical spine can be difficult in the obtunded or unresponsive patient. Various trauma series have been reported to detect up to 95% of cervical fractures but only when ideal imaging views have been obtained, which is not often possible in the unresponsive or uncooperative patient. Passively performed cervical flexion-extension under live fluoroscopy has been suggested but is not without inherent risk in the potentially unstable cervical spine. CT of the cervical spine has gained acceptance for the evaluation of these patients given the excellent evaluation of the osseous anatomy and for the common availability in most emergency departments. Sanchez and associates, using a protocol to evaluate for cervical spine injuries after blunt trauma, were able to detect 99% of cervical fractures with 100% specificity. Chiu WC, Haan JM, Cushing BM, et al: Ligamentous injuries of the cervical spine in unreliable blunt trauma patients: Incidence, evaluation, and outcome. J Trauma 2001;50:457-463. Sanchez B, Waxman K, Jones T, et al: Cervical spine clearance in blunt trauma: Evaluation of a computed tomography-based protocol. J Trauma 2005;59:179-183.
Question 259
High Yield
A 28-year-old man sustains the closed injury shown in Figures 3a through 3c after falling 8 feet while rock climbing. Management should consist of



Explanation
The radiographs show a comminuted talar body fracture. The goal of treatment is to minimize the risks of posttraumatic arthrosis of the ankle and subtalar joint and to maintain vascularity. Open reduction and internal fixation with an attempt at anatomic reduction will lead to improved outcomes. Attempting to repair this fracture via an arthrotomy only is extremely difficult, and the addition of a medial malleolar osteotomy is warranted. A limited anterior lateral arthrotomy with minimal soft-tissue stripping may assist with fixation of anterior-lateral and lateral fragments and allow better assessment of reduction of the major fracture line. Nonsurgical care would lead to inadequate reduction and increased risk of both ankle and hindfoot arthrosis. Talectomy and primary ankle and hindfoot arthrodesis should not be performed as primary surgical reconstructive options in this closed injury pattern. Sanders R: Fractures and fracture-dislocations of the talus, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1465-1518.
Question 260
High Yield
Which of the following findings is most prognostic for the ability of a young child with cerebral palsy to walk?

Explanation
Several studies have shown that sitting ability by age 2 years is highly prognostic of walking. Molnar and Gordon reported that children not sitting independently by age 2 years had a poor prognosis for walking. Wu and associates reported that children sitting without support by age 2 years had an odds ratio of 26:1 of walking compared with those unable to sit. This was far higher than the odds ratios for cerebral palsy location, motor dysfunction, crawling, creeping, scooting, or rolling. Molnar GE, Gordon SU: Cerebral palsy: Predictive value of selected clinical signs for early prognostication of motor function. Arch Phys Med Rehabil 1976;57:153-158.
Question 261
High Yield
A 55-year-old woman with a history of untreated idiopathic scoliosis has had neurogenic claudication for the past several months. MRI reveals spinal stenosis at L2-L3, L3-L4, and L4-L5. Radiographs show a 45-degree lumbar curve from T10 to L4, with a degenerative spondylolisthesis at L4-L5. Laminectomy at the stenotic levels and stabilization of the deformity are planned. Which of the following is NOT considered an absolute indication for extending the fusion to the sacrum, rather than stopping at L5?
Explanation
There are several indications for extending adult scoliosis fusions to the sacrum, rather than stopping in the lower lumbar spine. These indications include posterior column deficiencies at L5-S1, such as spondylolysis and laminectomy, and deformities extending to the sacrum, such as fixed tilt of L5-S1 or sagittal imbalance. MRI signal changes in the L5-S1 disk do not preclude stopping the fusion at L5. Some surgeons use diskography or diagnostic facet blocks to evaluate the integrity of the L5-S1 level prior to stopping the fusion at L5. Long scoliosis fusions stopping at L5 have a significant risk of failure, highlighting the importance of careful selection of fusion levels. Bradford DS, Tay BK, Hu SS: Adult scoliosis: Surgical indications, operative management, complications, and outcomes. Spine 1999;24:2617-2629. Bridwell KH: Where to stop the fusion distally in adult scoliosis: L4, L5, or the sacrum? Instr Course Lect 1996;45:101-107.
Question 262
High Yield
A 7-month-old girl has had a severe flatfoot deformity since birth. The talar head is prominent in the medial plantar arch of the foot. No other deformities of the spine or extremities are present. Motor and sensory examinations of the extremities are normal. Figures 37a through 37c show simulated weight-bearing AP and lateral radiographs and a planter flexion lateral view. What is the most likely diagnosis?



Explanation
Congenital vertical talus is a fixed dorsal dislocation of the talonavicular joint with equinus of the ankle joint. The AP radiograph shows valgus of the midfoot and an increased talocalcaneal angle; the lateral radiograph shows a vertically positioned talus and equinus of the ankle joint, and the plantar flexion lateral view shows that the talonavicular joint does not reduce. A line drawn through the long axis of the talus passes below the long axis of the first metatarsal. Initial management should consist of serial casting to stretch the dorsal soft-tissue structures; surgery eventually will be required to reduce the talonavicular joint. The differential diagnosis of congenital vertical talus includes pes calcaneovalgus, flexible pes planus, and peroneal spastic flatfoot. Pes calcaneovalgus, flexible pes planus, congenital short Achilles tendon, and peroneal spastic flatfoot would not show resistent dorsal dislocation of the navicular on the plantar flexion view. Kodros SA, Dias LS: Single-stage surgical correction of congenital vertical talus. J Pediatr Orthop 1999;19:42-48.
Question 263
High Yield
A 32-year-old construction worker reports a persistent burning, tingling sensation on the dorsum of his right foot and significant sensitivity on the plantar surface after a 500-lb steel beam dropped on it 8 weeks ago. Initial radiographs revealed no fractures, and the skin remained intact at the time of injury. Physical therapy, anti-inflammatory drugs, and a serotonin reuptake inhibitor have failed to provide relief. What is the next most appropriate step in management?
Explanation
Following failure of physical therapy and pharmacologic management in a patient with complex regional pain syndrome, the management of choice is sympathetic blocks. While continued physical therapy would be assistive, sympathetic blocks allow a more rapid relief of symptoms. Neurostimulation is not appropriate at this stage because of its invasive nature. Cepeda MS, Lau J, Carr DB: Defining the therapeutic role of local anesthetic sympathetic blockade in complex regional pain syndrome: A narrative and systematic review. Clin J Pain 2002;18:216-233. Perez RS, Kwakkel G, Zuurmond WW, et al: Treatment of reflex sympathetic dystrophy (CRPS type 1): A research synthesis of 21 randomized clinical trials. J Pain Symptom Manage 2001;21:511-526. Tran KM, Frank SM, Raja SN, et al: Lumbar sympathetic block for sympathetically maintained pain changes in cutaneous temperatures and pain perception. Anesth Analg 2000;90:1396-1401.
Question 264
High Yield
A patient underwent an anterior cervical diskectomy and interbody fusion for a C5-6 herniated nucleus pulposus and left C6 radiculopathy 8 months ago. He now reports new onset of severe neck pain and left C6 radicular pain, with wrist extension weakness. The radiograph and CT scan shown in Figures 26a and 26b reveal pseudarthrosis at C5-6. The next step in management should consist of

Explanation
Brodsky and associates reviewed 34 cases of cervical pseudarthrosis after anterior fusion. Seventeen were treated with revision anterior fusion and 17 with posterior foraminotomy and fusion. Good results were seen in 75% of patients who underwent revision anterior surgery, but better results (94%) were seen with posterior surgery, including foraminotomy and stabilization. Tribus and associates reported treatment of 16 patients with pseudarthrosis using revision anterior debridement of the fibrous tissue and fusion with autograft and plates. There was improvement of the neck in 75% of the patients, nonunion in 19%, continued weakness in 28%, and dysphagia in 5%. Farey and associates reported on 19 patients treated with posterior foraminotomy, stabilization, and fusion with a fusion rate of 100%, resolution of arm pain in 94%, resolution of weakness in 100%, and resolution of neck pain in 75%. It would appear that posterior foraminotomy is more effective for relieving arm pain and neurologic deficits associated with pseudarthrosis. Posterior fusion has the most reliable rate of arthrodesis in this setting. Dysphagia is reported in some patients undergoing more extensive anterior dissections required for applying plates. A neck brace is unlikely to aid in healing of pseudarthrosis in a patient who underwent surgery 8 months ago. A neck brace would be most effective within the first 3 months if a delayed union is identified. Brodsky AE, Khalil MA, Sassard WR, Neuman BP: Repair of symptomatic pseudarthrosis of anterior cervical fusion: Posterior versus anterior repair. Spine 1992;17:1137-1143. Tribus CB, Corteen DP, Zdeblick TA: The efficacy of anterior cervical plating in the management of symptomatic pseudarthrosis of the cervical spine. Spine 1999;24:860-864.
Question 265
High Yield
A 29-year-old man undergoes surgery for a grade I isthmic spondylolisthesis at L5. Following surgery, what type of brace will best immobilize the L5-S1 motion segment?
Explanation
The thoracolumbosacral orthosis with thigh extension best immobilizes the lumbosacral junction. Fidler and Plasmans have demonstrated increased motion at the lumbosacral junction with the standard chairback-type brace. Connolly PJ, Grob D: Bracing of patients after fusion for degenerative problems of the lumbar spine: Yes or no? Spine 1998;23:1426-1428.
Question 266
High Yield
What neurovascular structure is at greatest risk when creating a proximal anterolateral elbow arthroscopy portal?
Explanation
The radial nerve is 4 to 7 mm from the anterolateral portal, which is placed 1 cm anterior and 3 cm proximal to the lateral epicondyle. The posterior interosseous nerve can lie 1 to 14 mm from the portal site. Andrews JR, Carson WG: Arthroscopy of the elbow. Arthroscopy 1985;1:97-107.
Question 267
High Yield
What is the most frequent complication of percutaneous repair of an acute Achilles tendon rupture?

Explanation
Sural nerve entrapment is the major risk of percutaneous repair. A small mini-open technique with a suture guide can obviate that issue. Re-rupture rates after surgical repair are approximately 3%. Infection and wound problems are rarely encountered with percutaneous repair; they are issues with open repair. Aracil J, Pina A, Lozano JA, et al: Percutaneous suture of Achilles tendon ruptures. Foot Ankle 1992;13:350-351. Sutherland A, Maffulli N: A modified technique of percutaneous repair of the ruptured Achilles tendon. Oper Orthop Traumatol 1998;10:50-58.
Question 268
High Yield
Figures 3a and 3b show the current radiographs of a 59-year-old woman who has pain and deformity after undergoing bunion surgery 1 year ago. Nonsurgical management has failed to provide relief. Treatment should now consist of


Explanation
The hallux varus seen in this patient is most likely the result of a combination of causes. Based on the degenerative changes and the significant shortening of the first metatarsal relative to the second metatarsal, a metatarsophalangeal arthrodesis is the treatment of choice. The other surgical approaches are not expected to provide a satisfactory result. Coughlin MJ, Mann RA: Adult hallux valgus, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby-Year Book, 2000, pp 150-269.
Question 269
High Yield
Which of the following is considered the best measure of the adequacy of resuscitation in the first 6 hours after injury?
Explanation
The end point of resuscitation is adequate tissue perfusion and oxygenation. Blood lactate is the end point of anaerobic metabolism. The level of blood lactate reflects global hypoperfusion and is directly proportional to oxygen debt. Two separate prospective studies have verified a significant difference in mortality when blood lactate was used as a measure of resuscitation when compared to traditional parameters (mean arterial pressure, urine output, central venous pressure, and heart rate). Base deficit is a direct measure of metabolic acidosis and an indirect measure of blood lactate levels. It correlates well with organ dysfunction, mortality, and adequacy of resuscitation. It is easy to measure, can be obtained rapidly, and is an excellent assessment of the adequacy of resuscitation. Porter JM, Ivatury RR: In search of the optimal end points of resuscitation in trauma patients: A review. J Trauma 1998;44:908-914.
Question 270
High Yield
An active 55-year-old man who felt a sudden pop in the left heel while playing tennis 6 months ago was diagnosed with an ankle sprain around the time of injury. He now reports calf atrophy and severe weakness with running. Examination reveals a palpable defect in the Achilles tendon and only trace passive ankle flexion when the calf is squeezed. At the time of surgery, an Achilles tendon defect of 6 cm cannot be approximated. Surgical management of the Achilles tendon should include
Explanation
Chronic or neglected Achilles tendon ruptures can present a surgical problem. Ideally, end-to-end apposition of tendon should be attempted, but this should be accomplished without placing the foot in marked equinus. A defect of greater than 5 cm requires the use of a tendon transfer either alone or in combination with a V-Y advancement of the gastrocnemius. Because of its proximity to the Achilles tendon and its strength as a plantar flexor, the flexor hallucis longus is an ideal choice for this task. Studies have shown that early active range-of-motion exercises after an Achilles tendon repair is beneficial for tendon healing and improved clinical outcomes. Myerson M: Achilles tendon ruptures. Instr Course Lect 1999;48:219-230.
Question 271
High Yield
A patient undergoes hip arthroscopy, and the pathology is seen in Figure 18. What is the most likely diagnosis?

Explanation
The motorized shaver is adjacent to the acetabular labrum, which is torn. The femoral head and acetabulum are normal in appearance. Neither the fat pad nor a loose body is identified.
Question 272
High Yield
An otherwise healthy 57-year-old man has persistent, severe hip pain after undergoing total hip arthroplasty 3 months ago. What is the next most appropriate step in management?

Explanation
Any patient who is severely symptomatic this quickly after surgery must be evaluated for infection. Loosening is also a possible cause, but infection must be ruled-out. Bone scans are not helpful at this early postoperative stage. Normal laboratory values argue strongly against infection, but when abnormal, need to be supplemented with a hip aspiration. Aspiration remains the most selective and sensitive measure, especially when linked to a WBC count of the synovial tissues in the joint. There is no indication for an antiobiotic trial because it may make future culture sensitivity more difficult. Drancourt M, Stein A, Argenson JN, et al: Oral rifampin plus ofloxacin for treatment of staphylococcus-infected orthopedic implants. Antimicrob Agents Chemother 1993;37:1214-1218. Duncan CP, Beauchamp C: A temporary antibiotic-loaded joint replacement system for the management of complex infections involving the hip. Orthop Clin North Am 1993; 24: 751-759.
Question 273
High Yield
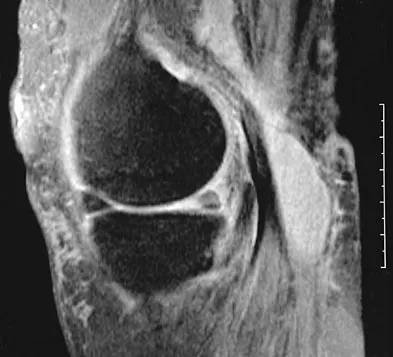
What is the principal advantage of surgical repair for the lesion shown in Figure 19?

Explanation
The MRI scan shows a rupture of the Achilles tendon. The substantiated advantages of repair are less risk of re-rupture and greater plantar flexion strength. Dorsiflexion strength is not influenced. Motion, pain, and period of recovery are not specifically improved as a consequence of surgery. Bhandari M, Guyatt GH, Siddiqui F, et al: Treatment of acute Achilles tendon ruptures: A systematic overview and meta-analysis. Clin Orthop 2002;400:190-200.
Question 274
High Yield
The diagnosis of an infection after total knee arthroplasty is most reliably proven based on what single study?
Explanation
In a study of 52 patients with infected total knee arthroplasties, Windsor and associates showed that the average leukocyte count was 8,300/mm3 and that aspirated knee fluid was positive in all patients except one. Knee radiographs can be unclear in showing infection, which may be present without radiographic signs of loosening. Technetium Tc 99m and gallium bone scans may not conclusively show the presence of infection, particularly in the first 3 years after knee arthroplasty. Windsor RE, Bono JV: Infected total knee replacements. J Am Acad Orthop Surg 1994;2:44-53.
Question 275
High Yield
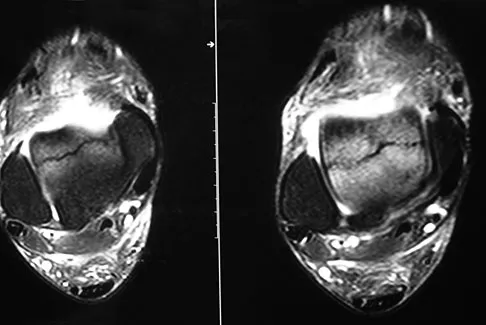
The MRI scan of the shoulder shown in Figure 2 was performed with the arm in abduction and external rotation. The image reveals what condition?
Explanation
Internal impingement of the shoulder is now a well-recognized cause of shoulder pain in the throwing athlete. First described by Walch and associates, it involves contact of the rotator cuff and labrum in the maximally externally rotated and abducted shoulder, such as in the late cocking phase of the throwing motion. Schickendantz and associates have shown this contact to be physiologic in most patients and becoming pathologic with repetitive overhead activity. Schickendantz MS, Ho CP, Keppler L, Shaw BD: MR imaging of the thrower's shoulder: Internal impingement, latissimus dorsi/subscapularis strains, and related injuries. Magn Reson Imaging Clin N Am 1999;7:39-49. Walch G, Boileau P, Noel E, et al: Impingement of the deep surface of the supraspinatus tendon on the posterosuperior glenoid rim: An arthroscopic study. J Shoulder Elbow Surg 1992;1:238-245.
Question 276
High Yield
While lifting weights, a patient feels a pop in his arm. He has the deformity shown in Figure 30. If left untreated, the patient will have the greatest deficiency in

Explanation
The patient has a distal biceps rupture. While the distal biceps contributes to elbow flexion, its main function is forearm supination. Baker BE, Bierwagen D: Rupture of the distal tendon of the biceps brachii: Operative versus non-operative treatment. J Bone Joint Surg Am 1985;67:414-417. D'Arco P, Sitler M, Kelly J, et al: Clinical, functional, and radiographic assessments of the conventional and modified Boyd-Anderson surgical procedures for repair of distal biceps tendon ruptures. Am J Sports Med 1998;26:254-261.
Question 277
High Yield
An 18-year-old football player sustains a contact injury to his right lower leg, and radiographs show a closed transverse fracture of the middle third of the tibia. Based on the clinical examination, a compartment syndrome is suspected. When measuring compartment pressures, the highest tissue pressure is recorded how many centimeters proximal or distal to the fracture site?
Explanation
Measurements of compartment pressures in patients with tibial fractures and compartment syndrome reveal that the highest tissue pressures are recorded at the level of the fracture or within 5 cm of the fracture. Tissue pressures show a statistically significant decrease when they are recorded at increasing distances proximal and distal to the site of the highest pressure recorded. To reliably determine the location of the highest tissue pressure in patients with tibial fractures, measurements should be obtained, at a minimum, in both the anterior and deep posterior compartments at the level of the fracture, as well as at locations proximal and distal. The highest tissue pressure recorded should serve as a basis for determining the need for fasciotomy. Heckman MM, Whitesides TE Jr, Grewe SR, Rooks MD: Compartment pressure in association with closed tibial fractures: The relationship between tissue pressure, compartment, and the distance from the site of the fracture. J Bone Joint Surg Am 1994;76:1285-1292.
Question 278
High Yield
Which of the following patients with cerebral palsy is considered the ideal candidate for a selective dorsal rhizotomy?
Explanation
The enthusiasm with which dorsal rhizotomy was received led to the broadening of selection criteria with poorer results. The ideal candidate is an ambulatory 4- to 8-year-old child with spastic diplegia who does not use assistive devices or have joint contractures. The child must be old enough to actively participate in the rigorous postoperative physical therapy program. The use of the procedure in an ambulatory 16-year-old patient is less desirable because joint contractures will most likely have developed to a varying degree. The hemiplegic child is best treated by orthopaedic interventions. Oppenheim WL: Selective posterior rhizotomy for spastic cerebral palsy: A review. Clin Orthop 1990;253:20-29. Renshaw TS, Green NE, Griffin PP, Root L: Cerebral palsy: Orthopaedic management. J Bone Joint Surg Am 1995;77:1590-1606.
Question 279
High Yield
A 14-year-old girl reports hip pain that is exacerbated by weight bearing. A radiograph and biopsy specimen are shown in Figures 16a and 16b. The best course of management should be

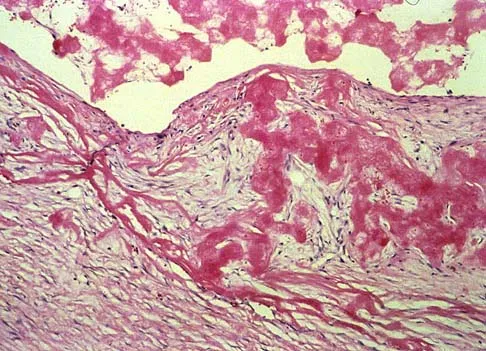
Explanation
The patient has a unicameral bone cyst. Because the subtrochanteric part of the femur is a high-stress region, the treatment of choice is bone curettage and grafting. Azouz EM, Karamitsos C, Reed MH, Baker L, Kozlowski K, Hoeffel JC: Types and complications of femoral neck fractures in children. Pediatr Radiol 1993;23:415-420.
Question 280
High Yield
Which of the following statements about hoarseness due to vocal cord paralysis after anterior cervical diskectomy and fusion is most accurate?
Explanation
It has been traditionally taught that a left-sided approach to the anterior cervical spine is associated with a lower incidence of injury compared to the right-sided approach. This is due in part to the anatomic differences in the path the recurrent laryngeal nerve (RLN) takes on the right as compared to the left. Both nerves ascend in the tracheoesophageal groove after branching off the vagus nerve in the upper thorax. The left-sided RLN loops around the aortic arch and stays relatively medial as compared to the right-sided RLN which loops around the right subclavian artery and is somewhat more lateral at this point, and therefore is theoretically more vulnerable as it ascends toward the larynx before becoming protected in the tracheoesophageal groove. Furthermore, the variant of a nonrecurrent inferior laryngeal nerve branching directly off the vagus nerve at the level of the midcervical spine is much more common on the right than the left. Despite this reasoning, there has been no clinical evidence to suggest that laterality of approach for anterior cervical surgery makes any difference in the incidence of vocal cord paralysis. Furthermore, two recent studies have shown that the incidence of RLN injury and vocal cord paralysis is equal with either side of approach. Beutler WJ, Sweeney CA, Connolly PJ: Recurrent laryngeal nerve injury with anterior cervical spine surgery risk with laterality of surgical approach. Spine 2001;26:1337-1342.
Question 281
High Yield
Figure 49 shows the radiograph of a 3-year-old child with progressive bowlegs. Laboratory studies show a calcium level of 9.5 mg/dL (normal 9.0 to 11.0 mg/dL), a phosphorus level of 4.2 mg/dL (normal 3 to 5.7 mg/dL), and an alkaline phosphatase level of 305 IU/L (normal 104 to 345 IU/L). What is the most likely diagnosis?

Explanation
The patient has bowlegs associated with very wide physes, particularly noted at the hips. The widening of the growth plates is a classic sign of rickets; however, the normal levels of calcium, phosphorus, and alkaline phosphatase rule out both nutritional and hypophosphatemic rickets. Patients with nutritional rickets or hypophosphatemic rickets have hypophosphatemia and increased alkaline phosphatase levels. Jansen metaphyseal dysostosis has very severe radiographic findings that are not found in this patient; however, these radiographic findings are classic for Schmid metaphyseal dysostosis. This disorder is caused by a mutation in the gene for type X collagen, which is found only in the growth plates of growing children. Lachman RS, Rimoin DL, Spranger J: Metaphyseal chondrodysplasia - Schmid type: Clinical and radiographic delineation with a review of the literature. Pediatr Radiol 1988;18:93-102.
Question 282
High Yield
Figures 35a and 35b show the radiographs of a 20-year-old man who is unable to rotate his dominant forearm. Examination reveals that the arm is fixed in supination. To regain motion, management should consist of


Explanation
The patient has a proximal synostosis; therefore, resection of the synostosis is considered the best option to regain motion. While forearm osteotomy can place the hand in a more functional position, rotation will not be restored. Proximal radial excision can provide forearm rotation; however, this procedure is reserved for patients who have a proximal radioulnar synostosis that is too extensive to allow a safe resection, involves the articular surface, and is associated with an anatomic deformity. Motion will not be restored with dynamic splinting. Kamineni S, Maritz NG, Morrey BF: Proximal radial resection for posttraumatic radioulnar synostosis: A new technique to improve forearm rotation. J Bone Joint Surg Am 2002;84:745-751.
Question 283
High Yield
Following a radial nerve neurapraxia at or above the elbow, return of muscle function can be expected to start at the brachioradialis and return along which of the following progressions?

Explanation
Following a radial nerve neurapraxia above the elbow, muscle recovery can be expected in a predictable pattern. Although variations will occur, the return of function or reinnervation usually occurs in the following order: brachioradialis, extensor carpi radialis longus, supinator, extensor carpi radialis brevis, extensor carpi ulnaris, extensor digitorum comminus, extensor digiti minimi, extensor indicis proprious, extensor pollicis longus, abductor pollicis longus, and extensor pollicis brevis. Netter F: The Ciba Collection of Medical Illustrations: The Musculoskeletal System. Part 1, Anatomy, Physiology and Metabolic Disorders. West Caldwell, NJ, Ciba-Geigy, 1991, vol 8, p 53.
Question 284
High Yield
A 35-year-old woman with type 1 diabetes mellitus has been treated for the past 2 years at a wound care center for persistent bilateral fifth metatarsal head ulcers. Management has consisted of shoe wear modifications, treatment with multiple enzymatic ointments, and a fifth metatarsal head resection on the left side. Physical examination reveals intact pulses, minimal ankle dorsiflexion, neutral hindfoot, and a persistent ulcer under the fifth metatarsal heads. What treatment will best help heal the ulcers?
Explanation
The patient likely has a significant Achilles contracture that causes her to always bear more weight on her forefoot. A gastrocnemius recession takes the ankle out of plantar flexion and she will be able to return to a normal gait and reduce the pressures on her forefoot. A forefoot amputation is a salvage option. The other choices are appropriate; however, the patient has had this problem for 2 years and she has already had multiple attempts at shoe wear modification. Laughlin RT, Calhoun JH, Mader JT: The diabetic foot. J Am Acad Orthop Surg 1995;3:218-225.
Question 285
High Yield
Following a fall from a height of 5 feet, a patient reports pain along the lateral border of the foot. The CT scan shown in Figure 54 indicates what pathology?

Explanation
The CT scan reveals an avulsion of the dorsal beak of the anterior process of the calcaneus. This common fracture is an avulsion of the origin of the bifurcate ligament, which runs from the anterior calcaneal process to both the cuboid and the lateral aspect of the navicular. An inversion mechanism is common, and the fracture is often missed in evaluation for a suspected ankle sprain. MRI may be useful in the diagnosis of these occult injuries, and suspicion should be present when tenderness exists over the superior portion of the anterior process of the calcaneus.
Question 286
High Yield
Nonsurgical management of pectoralis major tears is likely to result in weakness of glenohumeral
Explanation
Nonsurgical management is considered for proximal tears as well as partial tears in some individuals. Surgical management is often not appropriate in older or sedentary patients. However, patients treated nonsurgically will have a significant cosmetic defect, as well as weakness in adduction and internal rotation. Schepsis AA, Grafe MW, Jones HP, et al: Rupture of the pectoralis major muscle: Outcome or repair of acute and chronic injuries: Am J Sports Med 2000;28:9-15.
Question 287
High Yield
A 10-year-old boy with a history of retinoblastoma now reports right knee pain. AP and lateral radiographs are shown in Figures 3a and 3b. What is the most likely diagnosis?


Explanation
The radiographs show a bone-producing lesion in the femoral diaphysis. The radiographic appearance of small round cell tumors is more permeative with an elevated periosteum and no matrix production. The appearance of this lesion is most consistent with osteosarcoma. Patients who carry the Rb gene are predisposed to osteosarcoma. However, Ewing's sarcoma, primitive neuroectodermal tumor, and osteomyelitis can all occur in this location. Unni KK: Dahlin's Bone Tumors: General Aspects and Data on 11,087 Cases, ed 5. Philadelphia, PA, Lippincott-Raven, 1996, pp 143-160.
Question 288
High Yield
Based on the type of articulation shown in Figure 32, wear is not affected by which of the following factors?

Explanation
Wear in total hip arthroplasty is a very complex phenomenon. The radial mismatch of the femoral head to the acetabular component has been shown in multiple studies to be a significant factor in wear. The mismatch can neither be too small nor too large. When the mismatch is too small, seizing of the implants can occur. When the mismatch is too large, contact stresses increase and produce exceptionally high wear. The ideal radial mismatch should be approximately 50 microns. Surface roughness and ball sphericity are two items that are extremely important with respect to wear. High carbon content has been shown to decrease wear. This device has a very large head-to-neck ratio, so impingement-related wear is unlikely. Amstutz HC, Grigoris P: Metal on metal bearings in hip arthroplasty. Clin Orthop 1996;329:S11-S34. Amstutz HC, Campbell P, McKellop H, et al: Metal on metal total hip replacement workshop consensus document. Clin Orthop 1996;329:S297-S303.
Question 289
High Yield
Figure 35 shows the radiograph of a 12-year-old boy who fell off a snowmobile and landed on his left shoulder. He has a closed injury. Management should consist of

Explanation
Proximal humeral fractures in children are classified as metaphyseal or Salter-Harris type I or II fractures, and most of these fractures are treated with closed methods. Eighty percent of the growth of the humerus comes from the proximal physis; therefore, tremendous remodeling potential is present. Indications for open reduction include open fractures or severely displaced fractures in adolescents with minimal growth remaining. Acceptable limits of reduction in adolescent proximal humeral fractures include bayonet apposition and angulation of less than 35 degrees. Common blocks to reduction in adolescents include the biceps tendon and periosteum. For this fracture, use of a shoulder sling without reduction will lead to healing and an excellent result as the proximal humerus remodels. Kohler R, Trillaud JM: Fracture and fracture separation of the proximal humerus in children: Report of 136 cases. J Pediatr Orthop 1983;3:326-332. Beaty JH: Fractures of the proximal humerus and shaft in children. Instr Course Lect 1992;41:369-372. Dobbs MB, Luhmann SL, Gordon JE, et al: Severely displaced proximal humeral epiphyseal fractures. J Pediatr Orthop 2003;23:208-215. Beringer DC, Weiner DS, Noble JS, et al: Severely displaced proximal humeral epiphyseal fractures: A follow-up study. J Pediatr Orthop 1998;18:31-37.
Question 290
High Yield
A 30-year-old man falls off a 7-foot ladder and sustains the injury seen in the radiograph and the CT scan shown in Figures 39a and 39b. Medical history is negative. Management of this injury should include which of the following?

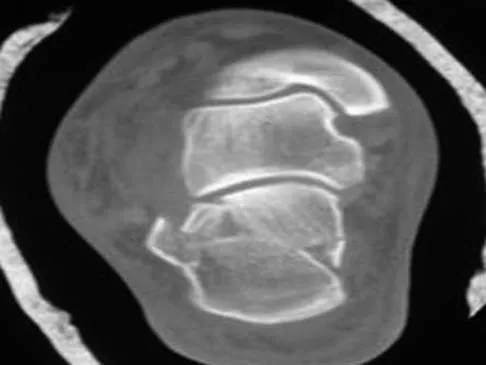
Explanation
A Sanders type 2 intra-articular calcaneus fracture in a young healthy nonsmoker is best treated with open reduction and internal fixation. Whereas nonsurgical management is an option, Buckley and associates have shown that these fractures have a better outcome with surgical care. Percutaneous fixation is reserved for tongue-type fractures and subtalar arthrodesis is used in some type 4 fractures. External fixation has not been shown to be advantageous in closed fractures. Buckley R, Tough S, McCormack R, et al: Operative compared with nonoperative treatment of displaced intra-articular calcaneal fractures: A prospective, randomized, controlled multicenter trial. J Bone Joint Surg Am 2002;84:1733-1744. Sanders R: Displaced intraarticular fractures of the calcaneus. J Bone Joint Surg Am 2000;82:225-250.
Question 291
High Yield
The medial collateral ligament complex of the elbow originates on what portion of the medial epicondyle?
Explanation
The medial collateral ligament complex of the elbow consists of three portions: the anterior bundle, the posterior bundle, and a transverse component that has little biomechanic significance. The origin of the ligament is from the central two thirds of the anteroinferior undersurface of the medial epicondyle.
Question 292
High Yield
Which of the following articulation couplings shows the lowest coefficient of friction as tested in the laboratory?

Explanation
Alumina ceramic is highly biocompatible when used as a biomaterial for joint arthroplasty implants. It has been shown to have good hardness, low roughness, and excellent wettability, therefore resulting in very low friction. However, it is expensive and limited reports have shown the problem of fracture on impact. The exact role for ceramic articulations is unknown at present. Cuckler JM, Bearcroft J, Asgian CM: Femoral head technologies to reduce polyethylene wear in total hip arthroplasty. Clin Orthop 1995;317:57-63.
Question 293
High Yield
A 15-year-old boy reports a 2-day history of progressive left buttock pain and severe limping. He denies any history of trauma or radiation of the pain. He has an oral temperature of 100.4 degrees F (38 degrees C). Examination reveals that the lumbar spine and left hip have unguarded motion. The abdomen is nontender. There is moderate tenderness of the left sacroiliac region with no palpable swelling. Pain is elicited when the left lower extremity is placed in the figure-4 position (FABER test). Laboratory studies show a peripheral WBC count of 11,500/mm3 (normal to 10,500/mm3) and an erythrocyte sedimentation rate of 38 mm/h (normal up to 20 mm/h). Radiographs of the pelvis, hips, and lumbar spine are normal. A nucleotide bone scan (posterior view) is shown in Figure 44. Initial management should consist of

Explanation
The symptoms, physical findings, and laboratory studies are most consistent with a diagnosis of infectious sacroiliitis, usually caused by Staphylococcus aureus. Initial radiographs will be normal, and the diagnosis of sacroiliitis is often delayed. A technetium Tc 99m bone scan will localize the problem in 90% of patients but may occasionally give a false-negative result in early cases. If suspicion is high, a gallium scan or MRI scan may help confirm the diagnosis of sacroiliitis. Needle aspiration of the sacroiliac joint is difficult; therefore, antibiotic selection is usually empiric or based on blood cultures. Sacroiliitis that is the result of connective tissue inflammatory disease is usually bilateral and without fever or leukocytosis. The lack of hip irritability, spinal rigidity, and abdominal tenderness helps to rule out other causes of limping with fever, such as psoas abscess, diskitis, and septic hip. Aprin H, Turen C: Pyogenic sacroiliitis in children. Clin Orthop 1993;287:98-106.
Question 294
High Yield
It has been shown that bisphosphonate-based supportive therapy (pamidronate or zoledronate) reduces skeletal events (onset or progression of osteolytic lesions) both in patients with multiple myeloma and in cancer patients with bone metastasis. The use of biphosphonate therapy has been associated with

Explanation
The use of bisphosphonates has been recently associated with the development of osteonecrosis of the jaw. Length of exposure seems to be the most important risk factor for this complication. The type of bisphosphonate may play a role and previous dental procedures may be a precipitating factor. Bisphosphonates are a class of therapeutic agents originally designed to treat loss of bone density (ie, alendronate). The primary mechanism of action of these drugs is inhibition of osteoclastic activity, and it has been shown that these drugs are useful in diseases with propensities toward osseous metastases. In particular, they are effective in diseases in which there is clear upregulation of osteoclastic or osteolytic activity, such as breast cancer and multiple myeloma, and have developed into a mainstay of treatment for individuals with these diseases. Although shown to reduce skeletal events, there has been no improvement in patient survival. Bamias A, Kastritis E, Bamia C, et al: Osteonecrosis of the jaw in cancer after treatment with bisphosphonates: Incidence and risk factors. J Clin Oncol 2005;23:8580-8587. Thakkar SG, Isada C, Smith J, et al: Jaw complications associated with bisphosphonate use in patients with plasma cell dyscrasias. Med Oncol 2006;23:51-56.
Question 295
High Yield
An otherwise healthy 13-year-old boy sustains the fracture shown in Figure 40 while throwing a fastball. Management should consist of

Explanation
Nonsurgical management such as a functional brace, hanging arm cast, or sugar tong splint is the treatment of choice for a fracture of the humeral shaft that is the result of throwing. The fracture surface typically is wide and the degree of displacement is not large; therefore, surgery is not indicated in most patients. Ogawa K, Yoshida A: Throwing fracture of the humeral shaft: An analysis of 90 patients. Am J Sports Med 1998;26:242-246.
Question 296
High Yield
A 20-year-old basketball player reports a 6-month history of right groin pain that radiates into his testicles with activities of daily living. He denies any history of trauma. Examination reveals tenderness about the groin, and he has full hip range of motion. The abdomen is soft. Radiographs are normal. Nonsurgical management has consisted of rest and physical therapy, but he continues to have pain. What is the next step in management?
Explanation
Sports hernias may be one of the most common causes of groin pain in athletes. Resisted hip adduction is painful in the case of groin disruption. Radiation of pain into the testicles and/or adductor region is often present. Sports hernias are associated with weakening of the posterior inguinal wall. In contrast with sports hernias, traditional or classic hernias can be readily detected on physical examination. Diagnostic imaging studies are not helpful and only serve to help exclude other diagnoses. Systemic high-dose steroids or sacroiliac joint injections have no role in treatment. High success rates have been reported for laparoscopic hernia repair in athletes. Kluin J, den Hoed PT, van Linschoten R, et al: Endoscopic evaluation and treatment of groin pain in the athlete. Am J Sports Med 2004;32:944-949. Genitsaris M, Goulimaris I, Sikas N: Laparoscopic repair of groin pain in athletes. Am J Sports Med 2004;32:1238-1242.
Question 297
High Yield
A 28-year-old man has had a 2-year history of progressive lateral ankle pain. History reveals that he underwent a triple arthrodesis at age 13 for a tarsal coalition. The pain has been refractory to braces, custom inserts, and nonsteroidal anti-inflammatory drugs. Weight-bearing radiographs of the ankle and foot are shown in Figures 3a through 3d. Surgical management should include which of the following?




Explanation
The patient has a valgus-supination triple arthrodesis malunion. Weight-bearing radiographs show excessive residual valgus through the subtalar joint, producing lateral subfibular impingement, and residual forefoot abduction and midfoot supination through the talonavicular joint, lateralizing the weight-bearing forces through the foot. The deformity is best managed with a medial displacement calcaneal osteotomy and transverse tarsal derotational osteotomy. Ankle arthroscopy and lateral ligament reconstruction are indicated in the event of ligament instability. Tendon transfer, lateral column lengthening, and heel cord lengthening are used for treatment of adult flatfoot from posterior tibial tendon insufficiency. Ankle arthrodesis and ankle arthroplasty are not indicated in this patient because the lateral ankle symptoms are the result of the underlying deformity in the hindfoot, the patient is young, and the ankle joint is relatively normal. Haddad SL, Myerson MS, Pell RF IV: Clinical and radiographic outcome of revision surgery for failed triple arthrodesis. Foot Ankle Int 1997;18:489-499.
Question 298
High Yield
A patient who was involved in a motor vehicle accident 2 days ago now reports neck pain. He denies any other symptoms. Radiographs reveal a type II odontoid fracture that is 2 mm anteriorly displaced. Management consists of halo vest immobilization in extension, and repeat radiographs reveal that the fracture is completely reduced. The patient is discharged to home, but later that evening he notes difficulty swallowing while trying to eat dinner. What is the most likely cause of this difficulty?

Explanation
If the neck is immobilized in excessive extension, it can be difficult for the patient to swallow. If the patient had injured the recurrent or superior laryngeal nerve at the time of the accident, it is likely to have manifested itself earlier on. Esophageal trauma or retropharyngeal edema or hematoma from the fracture also should have manifested itself earlier. Because the fracture was completely reduced, it is unlikely that moving the small fragment posteriorly would have injured the esophagus. Garfin SR, Botte MJ, Waters RL, Nickel VL: Complications in the use of halo fixation device. J Bone Joint Surg Am 1986;68:320-325.
Question 299
High Yield
A patient with diabetic peripheral neuropathy undergoes a partial first ray amputation for a chronic ulcer beneath the first metatarsal head. The insertion of the anterior tibialis is preserved. The patient has 10 degrees of passive dorsiflexion at the ankle and no other foot deformities or ulcers. Which of the following is considered appropriate shoe wear for this patient?
Explanation
The steel shank is a flat 1-inch steel strip placed between layers of the shoe to extend the foot lever and prevent deformity at the toe break seen following a partial first ray amputation. A rocker sole may be added as well to facilitate transition from foot flat to the toe-off phase of gait. Proper shoe fit is important, but "snug" fitting shoes in a patient with peripheral neuropathy and likely fluctuations in volume from intermittent swelling are to be avoided. A custom shoe is an unnecessary expense. The patient has at least 10 degrees of dorsiflexion at the ankle with an intact anterior tibialis muscle; therefore, catching the sole on carpeting should not be a problem. Philbin TM, Leyes M, Sferra JJ, et al: Orthotic and prosthetic devices in partial foot amputations. Foot Ankle Clin 2001;6:215-228.
Question 300
High Yield
Compared to eumenorrheic athletes, amenorrheic athletes have more frequent occurrences of
Explanation
In secondary amenorrhea, women do not receive the estrogen needed to maintain adequate bone mineralization. This hypoestrogenic state affects bone density, and there is evidence that stress fractures are more frequent in amenorrheic than eumenorrheic athletes. The other conditions are not seen with increased frequency in amenorrheic athletes. Warren MP: Health issues for women athletes: Exercise-induced amenorrhea. J Clin Endocrinol Metab 1999;84:1892-1896.
