HY 2026
00:00
Start Quiz
Question 101
High Yield
The dorsal (Thompson) approach to the proximal forearm uses which of the following intermuscular intervals?

Explanation
The Thompson posterior approach is used in treatment of fractures of the proximal radius. Dissection is carried out through the interval between the extensor carpi radialis brevis (radial nerve) and the extensor digitorum communis (posterior interosseous nerve). To identify this interval, the forearm is pronated and the mobile lateral wad of muscles (the ulnar-most belly is the extensor carpi radialis brevis) is grasped with the thumb and finger and pulled from the much less mobile mass of the extensor digitorum communis. The furrow created is marked with a skin marker for subsequent skin incision. The skin incision follows a line from the lateral epicondyle of the humerus to a point corresponding to the middle of the posterior aspect of the wrist. Distally, the intermuscular plane is between the extensor carpi radialis brevis and the extensor pollicis longus. Crenshaw AH Jr: Surgical techniques and approaches, in Canale ST (ed): Campbell's Operative Orthopaedics, ed 9. St Louis, MO, Mosby-Year Book, 1998, vol 1, pp 128-129. Hoppenfeld S, deBoer P: Posterior approach to the radius, in Surgical Exposures in Orthopaedics: The Anatomic Approach, ed 2. Philadelphia, PA, Lippincott-Raven, 1992, pp 136-146.
Question 102
High Yield
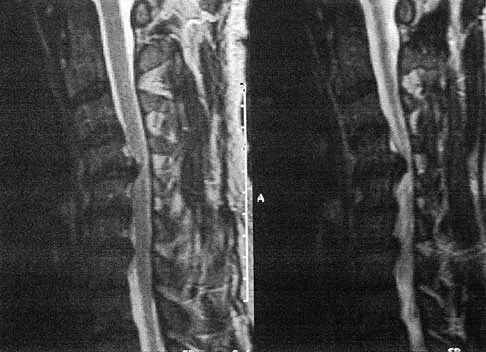
A 53-year-old man has had a long history of multiple joint symptoms, and he notes that the worst pain is from his left shoulder. A radiograph and MRI scan are shown in Figures 13a and 13b. Prior to surgical treatment of the shoulder, what is the most appropriate work-up?

Explanation
Rheumatoid arthritis is sometimes associated with radiographic evidence of instability of the cervical spine. In a study by Grauer and associates, radiographs of the cervical spine of patients with rheumatoid arthritis who had undergone total joint arthroplasty over a 5-year period were retrospectively reviewed. Nearly one half of the patients had radiographic evidence of cervical instability on the basis of traditional measurements. While radiographic evidence of cervical instability was not infrequent in this population of patients who underwent total joint arthroplasty for rheumatoid arthritis, radiographic predictors of paralysis were much less common. MRI prior to surgery may also be a consideration if the radiographic appearance of the rotator cuff alters the consideration of surgical treatment. In a series of patients undergoing prosthetic arthroplasty for a variety of shoulder disorders, the presence of a rotator cuff tear has been shown to be associated with a less favorable outcome. Most often, the presence of a rotator cuff tear was associated with a diagnosis of rheumatoid or other inflammatory arthritis and the tears were large and generally irreparable. Some case series demonstrated a higher prevalence of loosening of the glenoid component in patients with a large rotator cuff tear associated with superior migration of the humeral head. However, obtaining an MRI scan of the shoulder is not considered the best response since failure to determine cervical instability may result in anesthetic death. Whereas MRI may be helpful in planning reconstruction, it would be a less important priority. Grauer JN, Tingstad EM, Rand N, et al: Predictors of paralysis in the rheumatoid cervical spine in patients undergoing total joint arthroplasty. J Bone Joint Surg Am 2004;86:1420-1424.
Question 103
High Yield
Sudden cardiac death in the young athlete is most frequently caused by

Explanation
Hypertrophic cardiomyopathy is the leading cause of sudden cardiac death in athletes, accounting for 40% of reported cases. Most athletes have no previous symptoms, and sudden death may be the first clinical manifestation. The prevalence of hypertrophic cardiomyopathy in the general population is 1 in 500, with a mortality rate of 2% to 4% in young adults. Athletes with active myocarditis should not engage in sports for up to 6 months, and although they may be at risk for the development of chronic cardiomyopathy, it is rarely a cause of sudden cardiac death. Mitral valve prolapse with an accompanying systolic murmur is common in the general population, but infrequently a cause of sudden cardiac death. Weakening of the aortic wall associated with Marfan syndrome can result in abrupt rupture of the aorta. This accounts for 3% of sudden cardiac deaths in young athletes. Marfan syndrome usually can be detected on preparticipation screenings by its skeletal and ocular manifestations. Atherosclerotic coronary artery disease is the most common cause of sudden cardiac death in older athletes, accounting for 75% of reported cases. However, it is much less common in the young competitive athlete. Burke AP, Farb A, Virmani R, Goodin J, Smialek JE: Sports-related and non-sports-related sudden cardiac death in young adults. Am Heart J 1991;121:568-575.
Question 104
High Yield
What is the most common adverse postoperative complication of laminoplasty for multilevel cervical spondylotic myelopathy?

Explanation
A 30% to 50% loss of cervical range of motion is reported postoperatively in most patients following cervical laminoplasty. Inadvertent closure of the laminoplasty does occur but is rare. Laminoplasty is advocated in lieu of laminectomy to prevent progressive kyphosis and can effectively decompress the spinal cord. C5 nerve root palsies are a poorly understood but rare complication of surgical decompression for cervical spondylotic myelopathy. Emery SE: Cervical spondylotic myelopathy: Diagnosis and treatment. J Am Acad Orthop Surg 2001;9:376-388.
Question 105
High Yield
During a left-sided transforaminal lumbar interbody fusion at the L4-5 level, the surgeon notes a significant amount of bleeding that cannot be controlled while using a pituitary rongeur. What anatomic structure has been injured?
Explanation
The surgeon perforated the anterior longitudinal ligament and injured the common iliac artery. Bingol and associates described injuries to the vascular structures during lumbar disk surgery. The common iliac artery was most commonly affected and constituted 76.9% of injuries.
Question 106
High Yield
Figure 38 shows the radiograph of a 40-year-old woman who reports severe groin pain and lack of motion of the right hip. History reveals that the patient underwent a femoral osteotomy for hip dysplasia approximately 30 years ago. Treatment should include

Explanation
Although the patient is young, a total hip arthroplasty will provide pain relief and improve her range of motion. The arthritis is too advanced for the patient to benefit from an osteotomy. In addition, periacetabular osteotomy and hip arthrodesis do not improve range of motion of the hip. It has not been established that patients with severe osteoarthritis will benefit from arthroscopic debridement of the hip.
Question 107
High Yield
A 17-year-old high school football player reports wrist pain after being tackled. Radiographs are shown in Figures 22a through 22c. What is the recommended intervention?



Explanation
The patient has an acute fracture of the proximal pole. A 100% healing rate has been reported for open reduction and internal fixation of proximal pole fractures via a dorsal approach. This allows for direct viewing of the fracture line, facilitates reduction, and bone grafting can be done through the same incision if necessary. A vascularized or corticocancellous graft is reserved for nonunions. Proximal fractures are very slow to heal with a cast, if they heal at all. As a small fragment, percutaneous fixation is very difficult and has been reported for waist fractures. Rettig ME, Raskin KB: Retrograde compression screw fixation of acute proximal pole scaphoid fractures. J Hand Surg Am 1999;24:1206-1210.
Question 108
High Yield
A collegiate rower reports the sudden onset of right chest pain while rowing. The athlete states that the pain is worse with deep inspiration and coughing. Examination reveals localized tenderness over the posterolateral corner of the eighth rib. What is the most likely diagnosis?

Explanation
A rib stress fracture, the most common injury to the thorax in rowing athletes, generally occurs during periods of intense training with a low stroke rate and heavy loads. It is characterized by the sudden onset of sharp, localized chest pain while rowing. The fifth through the ninth rib is generally affected, and the diagnosis is best established with a bone scan. An intercostal muscle strain generally has an insidious onset and may be poorly localized. Costochondritis affects the anterior costochondral junction. A pneumothorax and an empyema can cause nonlocalized chest pain but are associated with respiratory distress and systemic physical findings. Karlson KA: Rib stress fractures in elite rowers. Am J Sports Med 1998;26:516-520.
Question 109
High Yield
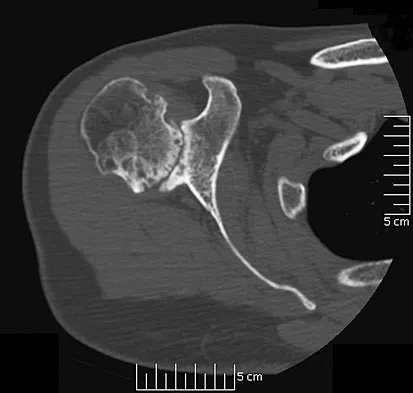
A 28-year-old man reports knee stiffness, swelling, and a constant ache that is worse with activity. Examination reveals an effusion, global tenderness, and warmth to the touch. Flexion is limited to 110 degrees. Figures 48a through 48d show sagittal T1-weighted, sagittal T2-weighted, axial T1-weighted fat-saturated gadolinium, and axial gradient echo MRI scans. Based on these findings, what is the most likely diagnosis?
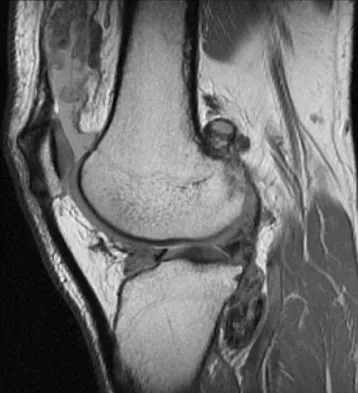
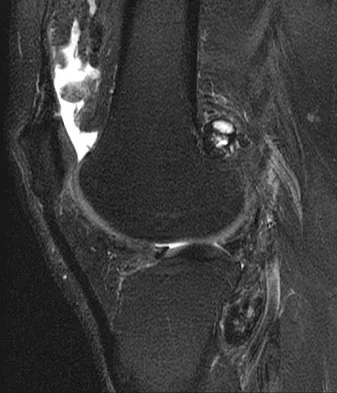
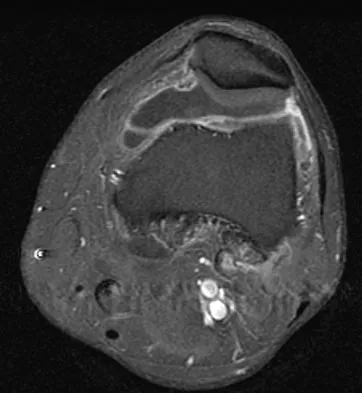

Explanation
The MRI scans show multiple low-signal intensity lesions scattered throughout the knee, extending posteriorly inferior to the tibial plateau. The low-signal intensity on both the T1- and T2-weighted images, the modest vascularity noted on the gadolinium image, and the "blooming" noted on the gradient echo image (ferrous-laden tissue) are all strongly suggestive of diffuse PVNS. Whereas synovial chondromatosis can present as diffuse masses in the knee, they present as nodule masses that have low T1- and high T2-weighted signal characteristics. Resnick D (ed): Diagnosis of Bone and Joint Disorders. Philadelphia, PA, WB Saunders, 2002, pp 4241-4252.
Question 110
High Yield
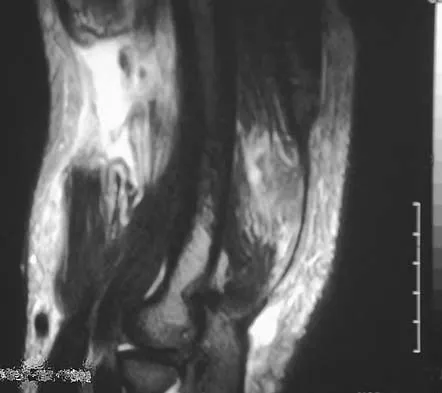
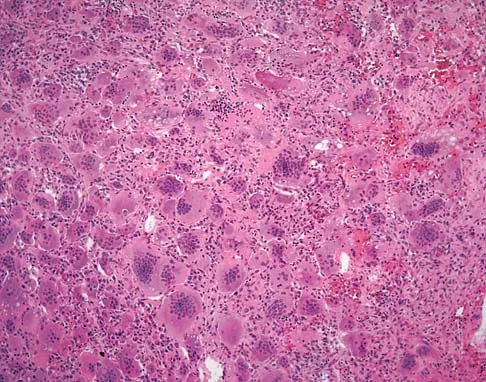
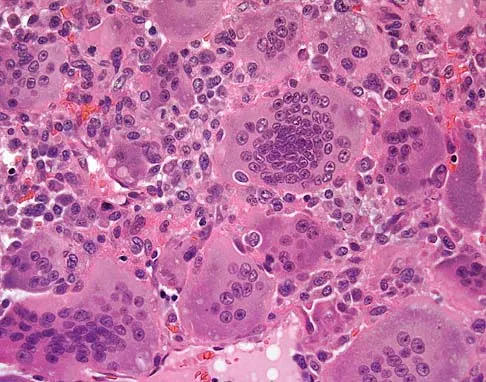
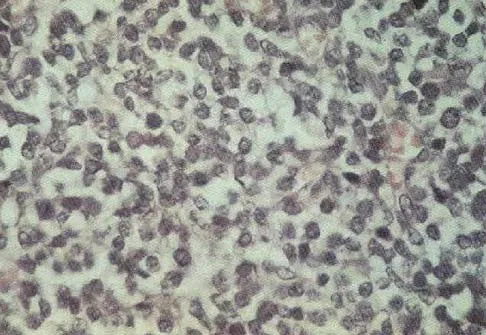
A 40-year-old man has a painless mass around his left ankle. He notes minimal growth over the past year. An MRI scan is shown in Figure 73a, and biopsy specimens are shown in Figures 73b and 73c. What is the most likely diagnosis?

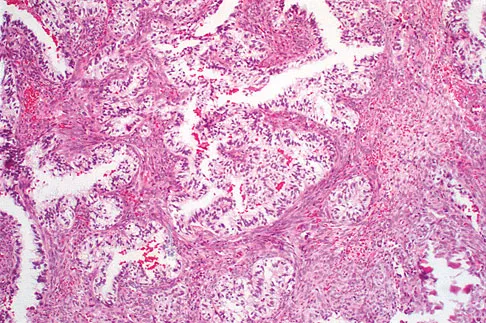
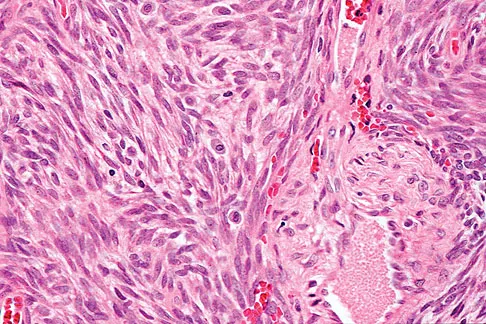
Explanation
The biopsy specimen is a low-power view of a soft-tissue sarcoma with a biphasic pattern of epithelial cells and fibrous spindle cells that are typical of a synovial sarcoma. A deep, painless soft-tissue mass greater than 5 cm in size is suspicious for a sarcoma. The imaging in this patient is indeterminate and the patient requires a biopsy for an accurate diagnosis. The biopsy reveals a tumor with a biphasic appearance consistent with a synovial sarcoma. These tumors are slow growing, occur primarily in the lower extremities, and are found in a younger demographic population compared to malignant fibrous histiocytoma and liposarcoma. They can occur in a biphasic pattern with clumps of epithelial cells and fibrous spindle cells or in a monophasic pattern. Synovial sarcomas stain positively for keratin. Keratin is positive in nearly all biphasic types and in many tumors of the monophasic fibrous type. Sixty percent of these tumors are found in the lower extremity. The area around the knee is the most common location, followed by the ankle and foot. Epithelioid and clear cell sarcomas are found associated with tendon sheaths of the hand and feet and are generally smaller in size. Epithelioid sarcoma may resemble granulomatous inflammation histologically; clear cell sarcoma is composed of nests of clear cells with occasional multinucleated giant cells. Pigmented villonodular synovitis is found within the synovium and is characterized by a villous histologic appearance with hemosiderin-laden macrophages. Malignant fibrous histiocytoma has a storiform histologic pattern with an abundance of pleomorphic cells. Enzinger FM, Weiss SW: Soft Tissue Tumors, ed 3. St Louis, MO, Mosby, 1995, p 757.
Question 111
High Yield
A 20-year-old man sustained an injury to his arm during a tug-of-war contest. An MRI scan is shown in Figure 18. What is the most likely diagnosis?
Explanation
The MRI scan reveals a transection of the biceps muscle. The underlying brachialis is intact. This injury can occur as a result of a cord wrapped around the upper arm. Care should be taken to ensure that there is no concurrent vascular injury. A posterior subcutaneous lipoma appears as a well-encapsulated mass on T2-weighted images. Heckman JD, Levine MI: Traumatic closed transection of the biceps brachii in the military parachutist. J Bone Joint Surg Am 1978;60:369-372.
Question 112
High Yield
During treatment of rupture of the subscapularis tendon with associated biceps instability, treatment of the biceps tendon should include which of the following?
Explanation
With subscapularis tendon ruptures that have biceps tendon pathology, treatment with tenodesis or tenotomy has improved clinical results. Subluxation or dislocation of the biceps tendon is common with subscapularis rupture. Dislocation of the biceps can occur either beneath the tendon, within the tendon, or extra-articularly. In all cases, the restraints to medial translations of the biceps have been disrupted. Attempts at recentering the biceps have not been successful, and clinical results appear to be improved when tenodesis or tenotomy is employed in the treatment of the unstable biceps associated with subscapularis tears. Edwards TB, Walch G, Sirvenaux F, et al: Repair of tears of the subscapularis: Surgical technique. J Bone Joint Surg Am 2006;88:1-10. Deutsch A, Altchek DW, Veltri DM, et al: Traumatic tears of the subscapularis tendon: Clinical diagnosis, magnetic resonance imaging findings, and operative treatment. Am J Sports Med 1997;25:13-22.
Question 113
High Yield
A 21-year-old woman with Marfan syndrome is seeking evaluation of her scoliosis. She reports no back or leg pain, and the neurologic examination is normal. Lateral and bending radiographs are shown in Figures 7a through 7e. Management should consist of





Explanation
Because the patient's thoracolumbar scoliosis is of a large enough magnitude, observation or bracing is not recommended. The thoracolumbar curve is flexible enough and L4 corrects well enough to the pelvis to consider anterior spinal fusion from T10 to L4. Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 161-171. Turi M, Johnston CE II, Richards BS: Anterior correction of idiopathic scoliosis using TSRH instrumentation. Spine 1993;18:417-422.
Question 114
High Yield
A 17-year-old man sustained a 5-mm laceration on the lateral aspect of the hindfoot while working on a farm. Examination in the emergency department revealed no fractures. Twenty-four hours later, he returns to the emergency department with increasing foot pain. Thin brown drainage is seen emanating from the wound. He has a temperature of 102.0 degrees F (38.9 degrees C), a pulse rate of 120, and a blood pressure of 80/40 mm Hg. Examination of the foot reveals diffuse swelling, ecchymosis, tenderness, and crepitus with palpation. Current radiographs are shown in Figures 40a and 40b. Management should now consist of


Explanation
The mechanism and environment in which the injury occurred, the clinical picture, and the radiographic findings of gas in the tissues suggest an anaerobic Gram-positive bacterial infection. This can be a life- and limb-threatening infection. Treatment should consist of wide debridement of all devitalized tissue, and intravenous antibiotics should be started. Wounds should be left open to allow bacterial effluent and increase oxygen tension in the wound. Hyperbaric oxygen may be used as an adjuvant but is no substitute for debridement. Pellegrini VD, Reid JS, Evarts CM: Complications, in Rockwood CA, Green DP, Bucholz RW, et al (eds): Rockwood and Green's Fractures in Adults, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 1, pp 458-463.
Question 115
High Yield
The husband of a 22-year-old woman has hypophosphatemic rickets. The woman has no orthopaedic abnormalities, but she is concerned about her chances of having a child with the same disease. What should they be told regarding this disorder?
Explanation
Hypophosphatemia is a rare genetic disease usually inherited as an X-linked dominant trait. The fact that the woman has no skeletal manifestations would indicate that the husband has the X-linked mutation. The disease is more severe in boys than it is in girls. The husband will not transmit the disease to his sons. However, all of their daughters will be affected either with the disease or as carriers. If the woman has the disease or the trait, there is a 50% chance that her sons will inherit the disease and a 50% chance that her daughters will be carriers or have a milder form of the disease. Parents should be advised to have genetic counseling so they can be informed when deciding whether to have children. Herring JA: Metabolic and endocrine bone diseases, in Tachdjian's Pediatric Orthopaedics, ed 3. New York, NY, WB Saunders, 2002, pp 1685-1743. Sillence DO: Disorders of bone density, volume, and mineralization, in Rimoin DL, Conner JM, Pyerite RE, et al (eds): Principles and Practice of Medical Genetics, ed 4. New York, NY, Churchill Livingstone, 2002.
Question 116
High Yield
A 73-year-old man is scheduled to have mature heterotopic bone resected from around his left total hip arthroplasty. The optimal management for prophylaxis against the return of heterotopic bone postoperatively is radiation therapy that consists of

Explanation
Patients require prophylaxis for heterotopic bone after resection to prevent recurrence. The optimal management has been found to be a dose of 700 cGy in one dose delivered either pre- or postoperatively. A dose of 2,000 to 3,000 cGy is considered excessive. Radiation therapy consisting of 1,000 cGy in five doses is an acceptable prophylaxis; however, it will require an extended hospital stay of 3 to 4 days and is more problematic for the patient who must be transported for radiation therapy for 5 days. A dose of 400 cGy is not as effective in prophylaxis for heterotopic bone formation. Healy WL, Lo TC, DeSimone AA, Rask B, Pfeifer BA: Single-dose irradiation for the prevention of heterotopic ossification after total hip arthroplasty: A comparison of doses of five hundred and fifty and seven hundred centigray. J Bone Joint Surg Am 1995;77:590-595. Pelligrini VD Jr, Gregoritch SJ: Preoperative irradiation for the prevention of heterotopic ossification following total hip arthroplasty. J Bone Joint Surg Am 1996;78:870-881.
Question 117
High Yield
Which of the following statements best describes the location of the nerve that is at risk in a direct posterior approach to the Achilles tendon?
Explanation
The sural nerve lies lateral to the Achilles tendon at the level of the foot but follows an oblique course proximally to lie directly over the tendon as it heads to the popliteal fossa. It is at risk with any proximal dissection from a direct posterior approach and in particular with procedures done at the musculotendinous junction. The nerve crosses over the lateral border of the Achilles tendon at an average of 9.8 cm above its insertion. Webb J, Moorjani N, Radford M: Anatomy of the sural nerve and its relation to the Achilles tendon. Foot Ankle Int 2000;21:475-477.
Question 118
High Yield
A 38-year-old woman has a lesion on her left foot that has increased in size over the past 6 months. The clinical photograph is shown in Figure 17a, and a photomicrograph of the biopsy specimen is shown in Figure 17b. What is the most likely diagnosis?

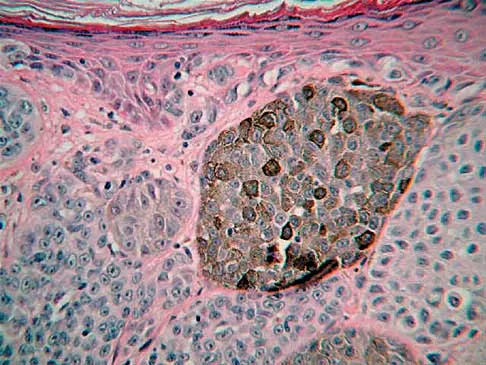
Explanation
Melanoma comprises 25% of lower extremity lesions and is the most common malignant tumor of the foot. The preferred treatment is wide resection. Hughes LE, Horgan K, Taylor BA, Laidler P: Malignant melanoma of the hand and foot: Diagnosis and management. Br J Surg 1985;72:811-815.
Question 119
High Yield
When compared to patients with osteoarthritis, patients with ankylosing spondylitis undergoing total hip arthroplasty can expect a
Explanation
Joshi and associates reported a 96% incidence of pain relief in 181 total hip arthroplasties in patients with ankylosing spondylitis. Only 65% of patients had good to excellent functional results, primarily the result of associated systemic diseases and spinal deformity. The incidence of infection was slightly higher, and the incidence of heterotopic ossification was higher in this group of patients.
Question 120
High Yield
A 45-year-old woman with stage II posterior tibial tendinitis has failed to respond to nonsurgical management. Recommended treatment now includes posterior tibial tendon debridement and medial calcaneal displacement osteotomy along with transfer of what tendon?
Explanation
The flexor digitorium longus is the commonly accepted tendon transfer for posterior tibial tendon insufficiency. The flexor hallucis longus has to be carefully rerouted to avoid crossing the neurovascular bundle and has not been shown clinically to provide superior results to flexor digitorum longus transfer. Use of the peroneus longus results in loss of plantar flexion strength of the first metatarsal, contributing to the flatfoot deformity. The anterior tibial tendon is in the anterior compartment and fires out of phase with the posterior tibial tendon. Sitler DF, Bell SJ: Soft tissue procedures. Foot Ankle Clin 2003;8:503-520.
Question 121
High Yield
What is the main benefit of using metal-backed tibial components in total knee arthroplasty?

Explanation
In a normal knee, the hard subchondral bone helps to distribute loads across the joint surface. A metal-backed tibial component in total knee arthroplasty decreases the compressive stresses on the underlying, softer cancellous bone by distributing the load over a larger surface area, particularly when one condyle is loaded. Although metallic base plates also increase the tensile forces on the other condyle when one is loaded and may decrease the thickness of the polyethylene tray, these are not benefits. Compressive forces on the polyethylene tray are increased with metal backing. The conformity of the articular surfaces is not affected by metal backing of the tibial component.
Question 122
High Yield
Based on the MR arthrogram of the elbow shown in Figure 8, which of the following structures is torn?

Explanation
Based on the MR arthrogram in which gadolinium (bright on T1-weighted images) was injected into the joint space prior to imaging, the study shows a tear of the anterior band of the ulnar collateral ligament (UCL). The disruption in the distal end of the UCL is outlined by contrast. A small collection of contrast extravasation into the flexor musculature further confirms the presence of a tear. The UCL has a broad-based attachment on the medial epicondyle and has a pointed or tapered attachment distally on the ulna. Most UCL tears occur distally at the ulnar (coronoid) attachment. MR arthrography provides improved sensitivity compared to conventional MRI, without contrast, for the detection of UCL pathology, particularly in the subacute or chronic setting. After the soft-tissue edema and joint fluid associated with the injury have resolved, the torn end of the ligament may lie in contact with its adjacent attachment and create a false-negative appearance. In this patient, a noncontrasted MR arthrogram showed no tear, yet the tear is apparent with intra-articular contrast and distention. MR arthrography of the elbow also may be useful in detecting intra-articular bodies or in evaluation for loose osteochondral fragments or flaps. Morrey BF: Acute and chronic instability of the elbow. J Am Acad Orthop Surg 1996;4:117-128.
Question 123
High Yield
Which of the following best describes the function of the notochord?
Explanation
The notochord is the anatomic structure that defines the phylum Chordata. The notochord plays a fundamental role in the development of the skeleton, and it exists only for a short period of time. During its temporary existence, the notochord serves as a transient axis of support, provides for the initial axis of orientation of the developing embryo, and most importantly, plays a vital role in the induction of the tissues that eventually form the vertebral column.
Question 124
High Yield
A 7-year-old girl who sustained a type III posteromedial extension supracondylar fracture underwent a closed reduction at the time of injury. Figure 27a shows the position of the fracture fragments prior to percutaneous medial and lateral pin fixation. Following surgery, healing was uneventful and the patient regained a full painless range of motion. Fifteen months after the injury, she now reports loss of elbow motion and moderate pain with activity. A current AP radiograph is shown in Figure 27b. What is the most likely cause of her symptoms?


Explanation
The patient sustained a very distal supracondylar fracture of the humerus. Fractures in this area can disrupt the blood vessels supplying the lateral ossification center of the trochlea. With disturbance of the blood supply in this area, local osteonecrosis occurs and disrupts the support for the overlying articular surface, producing joint incongruity and localized degenerative arthritis. Haraldsson S: The interosseous vasculature of the distal end of the humerus with special reference to the capitellum. Acta Orthop Scand 1957;27:81-93.
Question 125
High Yield
A 32-year-old man has a Glasgow Coma Scale score of 8 and an open pelvic fracture. The patient's family reports that he is a Jehovah's Witness. Initial hemodynamic instability has resolved. In the operating room during a washout, the patient's blood pressure becomes unstable. What is the most appropriate action?
Explanation
Certain medical procedures involving blood are specifically prohibited in the belief system of a Jehovah's Witness whereas others are not doctrinally prohibited. For procedures where there is no specific doctrinal prohibition, a Jehovah's Witness should obtain the details from medical personnel and make his or her own decision. Transfusions of allogeneic whole blood or its constituents or preoperative donated autologous blood are prohibited. Other procedures, while not doctrinally prohibited, are not promoted such as hemodilution, intraoperative cell salvage, use of a heart-lung machine, dialysis, epidural blood patch, plasmapheresis, white blood cell scans (labeling or tagging of removed blood returned to the patient), platelet gel, erythropoietin, or blood substitutes. The patient should not be given blood. Plasma expanders should be used first to restore hemodynamic stability. Cell saver blood from an open would is not recommended nor would there likely be enough from an open tibial fracture to salvage. The patient's family may be expressing their own beliefs rather than the patient's beliefs and it would be better to ask the patient when he or she is more alert to determine what procedures they would allow. A consult with the ethics committee will unnecessarily delay an intervention that should restore hemodynamic stability. Jimenez R, Lewis VO (eds): Culturally Competent Care Guidebook. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2007.
Question 126
High Yield
A 45-year-old woman with a long-standing history of diabetes mellitus has a large draining plantar ulcer of the right foot. Examination reveals some local cellulitis and erythema surrounding the ulcer. A clinical photograph is shown in Figure 7. Based on these findings, what is the most appropriate antibiotic?

Explanation
Combination drugs with activity against both aerobic and anaerobic organisms have been determined to be the best approach. The first-generation cephalosporins do not provide adequate coverage for gram-negative and anaerobic organisms. Gentamicin alone would not provide adequate activity against anaerobes, and there is the risk of renal and auditory toxicity. Pinzur MS, Slovenkai MD, Trepman E: Guidelines for diabetic foot care. Foot Ankle Int 1999;20:695-702.
Question 127
High Yield
Varus deformity after talar fractures is often seen due to collapse of the medial cortex. What artery supplies this portion of the talus?
Explanation
The artery of the tarsal canal is a branch of the posterior tibial artery. Among the branches of the artery of the tarsal canal is the deltoid artery. This arterial complex supplies the medial one third of the talar body. Disruption of this artery may lead to osteonecrosis of the medial body and subsequent collapse into varus. This is most commonly seen with talar body fractures but may be seen in Hawkins type 3 talar neck fractures. The artery of the tarsal sinus arises from the dorsalis pedis, lateral malleolar, and perforating peroneal arteries. The peroneal artery anastomoses with the calcaneal branches of the posterior tibial artery to form a plexus of vessels that supplies the posterior tubercle of the talus. Disruption of this artery would not result in collapse of the medial body, and thus would not lead to a varus deformity. Halibruton RA, Sullivan CR, Kelly PJ, et al: The extra-osseous and intra-osseous blood supply of the talus. J Bone Joint Surg Am 1958;40:1115.
Question 128
High Yield
A 35-year-old woman reports worsening pain after undergoing a neurectomy in the third interspace for a Morton's neuroma 12 months ago. She states that the pain is sharp and electrical, worse than before her surgery, and prevents her from participating in her usual work and exercise activities. Use of wider shoes and pads used before her surgery have failed to provide relief. Examination does not reveal any deformity or inflammation. Tenderness along with neuritic pain occurs with compression of the plantar aspect of the foot between the third and fourth metatarsal head area. To most reliably alleviate her pain, management should consist of

Explanation
Most patients with a significant recurrent neuroma will not obtain relief with conservative methods. Pain results from a stump neuroma at the weight-bearing area from too short of a resection of the nerve or from regrowth of the remaining nerve end. Although steroid injection may be helpful in localizing symptoms or providing temporary relief, it rarely cures a stump neuroma. Orthotics with a metatarsal pad will likely increase pressure and pain at the neuroma site. Physical therapy could temporize the symptoms but will not address the underlying problem. Similarly, bone decompression alone will not alter the location of the neuroma stump. Revision of the nerve to a more proximal level off of the weight-bearing area is the most likely method to succeed. A plantar approach facilitates identification and ability to revise the nerve to a more proximal level. Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 101-111. Johnson JE, Johnson KA, Unni KK: Persistent pain after excision of an interdigital neuroma: Results of reoperation. J Bone Joint Surg Am 1988;70:651-657. Beskin JL, Baxter DE: Recurrent pain following interdigital neurectomy: A plantar approach. Foot Ankle 1988;9:34-39.
Question 129
High Yield
A 13-year-old girl with Down syndrome has bilateral chronic patellar dislocations. She denies knee pain. She is able to straighten her knees and walks with a symmetric but awkward gait. She does not flex her knees in midstance. Examination reveals that the patellae cannot be brought into a reduced position. Management should consist of

Explanation
Chronic dislocation of the patella is occasionally seen in patients with Down syndrome. In early childhood, patellar realignment may restore stability of the patellae. In later childhood, bony changes in the patellar groove interfere with stability, even if surgical realignment is performed. Realignment can also lead to increased knee pain postoperatively. In asymptomatic patients who are able to extend their knees, continued observation is the management of choice. Dugdale TW, Renshaw TS: Instability of the patellofemoral joint in Down syndrome. J Bone Joint Surg Am 1986;68:405-413.
Question 130
High Yield
A 16-year-old female swimmer reports several episodes of atraumatic glenohumeral instability that occur with different arm positions. Examination reveals generalized ligamentous laxity and a positive sulcus sign, and her shoulder can be subluxated both anteriorly and posteriorly. Initial management should consist of

Explanation
The patient has multidirectional instability (MDI). It has been reported that a high percentage of patients with MDI respond to a properly structured exercise program that is continued for at least 3 to 6 months. If nonsurgical management fails to provide relief, stabilization with an inferior capsular shift procedure has been effective in a high percentage of patients. Unidirectional repairs, such as the Putti-Platt procedure, are unsuitable for correcting MDI. Thermal capsulorrhaphy has been reported to have a very high failure rate (greater than 50%) for treating MDI. Burkhead WZ Jr, Rockwood CA Jr: Treatment of instability of the shoulder with an exercise program. J Bone Joint Surg Am 1992;74:890-896. Neer CS II, Foster CR: Inferior capsular shift for involuntary inferior and multidirectional instability of the shoulder: A preliminary report. J Bone Joint Surg Am 1980;62:897-908. Pollock RG, Owens JM, Flatow EL, et al: Operative results of the inferior capsular shift procedure for multidirectional instability of the shoulder. J Bone Joint Surg Am 2000;82:919-928.
Question 131
High Yield
A 70-year-old woman reports anterior knee pain after undergoing an uncomplicated total knee arthroplasty 6 months ago. Examination reveals prepatellar tenderness, with no extensor lag. The radiographs shown in Figures 25a through 25c reveal a well-fixed patellar component. Management should consist of



Explanation
Patellar fractures that occur after a total knee arthroplasty are usually stress fractures. Integrity of the extensor mechanism precludes the need for surgical repair or internal fixation, while stability and fixation of the patellar component determine whether revision is indicated. A cylindrical cast and full weight bearing for 6 weeks is recommended for transverse fractures with an intact extensor mechanism and a stable component. A similar fracture, if vertical, may be treated with earlier motion. Rorabeck CH, Angliss RD, Lewis PL: Fractures of the femur, tibia, and patella after total knee arthroplasty: Decision making and principles of management, in Cannon WD Jr (ed): Instructional Course Lectures 47. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 449-458. Hozack WJ, Goll SR, Lotke PA, Rothman RH, Booth RE Jr: The treatment of patellar fractures after total knee arthroplasty. Clin Orthop 1988;236:123-127.
Question 132
High Yield
Initial postoperative management after repair of an acute rotator cuff tear includes
Explanation
In the immediate postoperative period following repair of an acute rotator cuff tear, passive forward elevation and external rotation should be performed within the safe zone determined at surgery. Early active range of motion (prior to tendon healing), internal rotation behind the back, and resistive exercises increase the risk of rupture of the repair. Iannotti JP: Full-thickness rotator cuff tear: Factors affecting surgical outcome. J Am Acad Orthop Surg 1994;2:87-95.
Question 133
High Yield
A 24-year-old professional basketball player reports the gradual onset of pain that is poorly localized to the left midfoot for the past 2 months. Examination reveals diffuse tenderness to palpation, full range of motion of the ankle and subtalar joint, and a normal neurovascular examination to the foot. An AP radiograph is shown in Figure 10. Definitive treatment should include

Explanation
The imaging studies reveal a navicular stress fracture. This condition is secondary to chronic overuse (often running on hard surfaces) and results in vague, ill-defined pain in the midfoot. These fractures can be missed on radiographs but are well-defined on CT or MRI. Tarsal navicular fractures are typically oriented in the sagittal plane. Surgery is typically indicated for the high-level athlete because of the high risk for nonunion and persistent symptoms following nonsurgical management. Internal fixation is the treatment of choice. Torg JS, Pavlov H, Cooley JH, et al: Stress fractures of the tarsal navicular. J Bone Joint Surg Am 1982;64:700-712.
Question 134
High Yield
A quarterback sustains a rough tackle after which he appears confused, has a dazed look on his face and an unsteady gait on standing. He denies loss of consciousness. Reexamination within 10 minutes is normal, the patient is lucid, and he wants to return to play. The coach and the player should be advised that he may
Explanation
The patient has a grade I (mild) concussion that can result in confusion and disorientation, without loss of consciousness. This concussion syndrome is completely reversible, with no long-term sequelae. Athletes who sustain a grade I concussion may return to play after 15 minutes if there are no lingering symptoms, such as headache or vertigo. A grade II concussion is characterized by loss of consciousness of less than 5 minutes. With this type of injury, the athlete can return to play in 1 week, if asymptomatic. If a grade III (severe) concussion is sustained, the athlete should avoid contact for a minimum of 1 month before considering a return to competition. A grade III concussion is characterized by a loss of consciousness of greater than 5 minutes or posttraumatic amnesia of greater than 24 hours. A CT scan is not indicated in a grade I injury. An athlete who sustains three grade I or grade II concussions, or two grade III concussions may not return to play for the season. Torg JS, Gennarelli TA: Head and cervical spine injuries, in DeLee JC, Drez D Jr (eds): Orthopaedic Sports Medicine Principles & Practice. Philadelphia, PA, WB Saunders, 1994, vol 1, pp 417-462.
Question 135
High Yield
Which of the following has been associated with a decreased rate of glenoid component radiolucent lines?
Explanation
According to a recent study, cemented pegged glenoid components had fewer radiolucent lines initially and at 2-year follow-up when compared to a cemented keeled design. Curve-backed designs have also shown fewer radiolucent lines when compared to flat-backed designs. Oversizing the glenoid can lead to impaired rotator cuff function and decreased range of motion. An off-centered glenoid can lead to early loosening. Gartsman GM, Elkousy HA, Warnock KM, et al: Radiographic comparison of pegged and keeled glenoid components. J Shoulder Elbow Surg 2005;14:252-257. Szabo I, Buscayret F, Edwards TB, et al: Radiographic comparison of flat-back and convex-back glenoid components in total shoulder arthroplasty. J Shoulder Elbow Surg 2005;14:636-642.
Question 136
High Yield
Figures 43a and 43b show the T1- and T2-weighted MRI scans of a 78-year-old woman who reports the sudden atraumatic onset of well-localized medial knee pain. Pain is worse at night and also occurs with weight-bearing activity. What is the most likely diagnosis?


Explanation
Osteonecrosis of the tibial plateau occurs infrequently. The symptoms are similar to those of idiopathic osteonecrosis of the medial femoral condyle and include pain and tenderness of the medial aspect of the knee and a slight synovitis. The range of motion of the knee remains within normal limits, and no gross deformity is present. Osteonecrosis of the tibial plateau is easily misdiagnosed as degenerative meniscus or osteoarthritis of the compartment of the knee. Review of lateral radiographs may reveal an osteopenic area in the subchondral bone of the medial tibial plateau. The diagnosis is more easily established with a bone scan where increased uptake of radionucleides is shown over the medial tibial plateau. In osteoarthritic involvement of the medial compartment, uptake is over both the medial femoral condyle and the medial tibial plateau, whereas if osteoarthritis involves the entire knee, uptake is diffuse over the entire joint. Radiographic findings in complex regional pain syndrome are normal as opposed to the findings for osteonecrosis or osteoarthritis. Osteosarcoma has a characteristic radiographic appearance of a bone-forming tumor. Loose bodies can derive from osteochondral fractures; a history of trauma is usually elicited. Osteoarthritis usually presents with joint space narrowing accompanying the weight-bearing pain. Soucacos PN, Berris AE, Xenakis TH, et al: Knee osteonecrosis: Distinguishing features in differential diagnosis, in Urbanik JR, Jones JD (eds): Osteonecrosis. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 413-424.
Question 137
High Yield
Which of the following nerves is most commonly injured when obtaining a bone graft from the posterior ilium?

Explanation
Cutaneous sensation to the buttock is provided by the superior, middle, and inferior cluneal nerves. The superior cluneal nerves are the lateral branches of the dorsal rami of the upper three lumbar nerves and penetrate deep fascia just proximal to the iliac crest. They pass distally to the skin of the buttock and will be injured if the exposure extends more than 8 cm anterolateral to the posterior superior iliac spine. The lateral femoral cutaneous nerve can be injured in an anterior ilium bone graft. The superior gluteal nerve or even the sciatic nerve can be injured if bone is removed from the sciatic notch or dissection is not kept subperiosteal; however, the rate of injury is far less than cluneal nerve injury. The L5 and S1 nerve roots are anterior and can be injured if the inner table bone is harvested and the dissection is not kept subperiosteal or is too medial; however, the rate of injury still is far less than cluneal nerve injury. Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, pp 295-297. Hollinshead WH: Textbook of Anatomy, ed 3. Hagerstown, MD, Harper and Row, 1974, p 379. Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, p 23.
Question 138
High Yield
Which of the following conditions is considered a relative contraindication to interscalene nerve block for patients scheduled to undergo shoulder surgery?
Explanation
A common side effect of interscalene nerve block for shoulder surgery is the blockade of the ipsilateral phrenic nerve. This, in turn, results in paresis of the diaphragm and up to a 30% reduction in pulmonary function volumes. Therefore, interscalene nerve block generally is not recommended for patients whose respiratory function is compromised. Other relative and absolute contraindications for interscalene nerve blocks include allergy to local anesthetics, infection at the injection site, uncontrolled seizure disorder, coagulation abnormality, and preexisting neurologic injury. Chelly JE: Indications for upper extremity blocks, in Chelly JE (ed): Peripheral Nerve Blocks, ed 2. Philadelphia, PA, Lippincott Williams & Wilkins, 2004, pp 19-27.
Question 139
High Yield
A 66-year-old woman who requires a cane for ambulation now notes increasing difficulty in using the cane after undergoing total elbow arthroplasty 3 months ago. AP and lateral radiographs are shown in Figures 15a and 15b. What is the most likely diagnosis?


Explanation
The lateral radiograph reveals a triceps avulsion with a small portion of bone. Triceps weakness and insufficiency can be a symptomatic problem after total elbow arthroplasty and is probably underreported. Ulnar nerve neuritis, aseptic loosening, instability, and infection are all complications of total elbow arthroplasty but would not account for the radiographic findings. Koval K (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orhthopaedic Surgeons, 2002, pp 323-327.
Question 140
High Yield
A 16-year-old high school football player has diffuse pain with attempted digital flexion after injuring the ring finger of the dominant hand 1 week ago. Examination reveals that he is unable to flex the distal interphalangeal joint. Management should consist of
Explanation
The patient has an avulsion of the flexor digitorum profundus. Treatment should include surgical exploration and tendon reinsertion. This is not an avulsion of the flexor digitorum superficialis because the patient's deficiency is the inability to flex the distal interphalangeal joint, not the proximal interphalangeal joint. Surgical release of the anterior interosseous nerve is not indicated because the flexor digitorum profundus of the ring finger is innervated by the ulnar nerve. A median nerve contusion causes wrist pain and/or numbness and tingling in the median nerve distribution. Strickland JW: Flexor tendons: Acute injuries, in Green DP, Hotchkiss RN, Pederson WC (eds): Green's Operative Hand Surgery, ed 4. Philadelphia, PA, 1999, pp 1851-1897.
Question 141
High Yield
The most favorable outcomes from release of the tarsal tunnel are in patients who have which of the following findings?
Explanation
Numerous causes of tarsal tunnel syndrome have been reported. The most favorable outcomes from release of the tarsal tunnel are in patients who have a space-occupying lesion (eg, ganglion, lipoma, or neurilemoma). While electrodiagnostic studies may be abnormal preoperatively, there is a low correlation between clinical outcome and electromyographic findings. Intrinsic weakness is a late finding in long-standing nerve dysfunction. Beskin JL: Nerve entrapment syndromes of the foot and ankle. J Am Acad Orthop Surg 1997;5:261-269.
Question 142
High Yield
A 10-year-old boy has a painful, swollen knee after falling off his bicycle. Examination reveals that the knee is held in 45 degrees of flexion, and any attempt to actively or passively extend the knee produces pain and muscle spasms. A lateral radiograph is shown in Figure 4. What is the most likely diagnosis?

Explanation
This is a typical patellar sleeve fracture. The patellar tendon avulses a portion of the distal bony patella, along with the retinaculum and articular cartilage from the inferior pole of the patella. It is common in children between ages 8 and 10 years. Anatomic reduction and repair of the extensor mechanism are mandatory to reestablish full knee extension. Houghton GR, Ackroyd CE: Sleeve fractures of the patella in children: A report of three cases. J Bone Joint Surg Br 1979;61:165-168.
Question 143
High Yield
Portions of which of the following normal structures help compose the spiral cord seen in Dupuytren's contracture?
Explanation
The normal fascial components that become diseased and compose the spiral cord include the pretendinous band, spiral band, lateral digital sheet, and Grayson's ligament. Cleland's ligament lies dorsal and is not involved with spiral cord formation. The intrinsic muscle and tendon, the natatory ligament, and the intermetacarpal ligament are well proximal to the digit and are not involved in spiral cord formation. McGrouther D: Dupuytren's contracture, in Green DP, Hotchkiss RN, Pederson WC (eds): Green's Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, vol 1, pp 565-569.
Question 144
High Yield
A 19-year-old girl has had pain and swelling in the right ankle for the past 4 months. She denies any history of trauma. Examination reveals a small soft-tissue mass over the anterior aspect of the ankle and slight pain with range of motion of the ankle joint. The examination is otherwise unremarkable. A radiograph and MRI scan are shown in Figures 45a and 45b, and biopsy specimens are shown in Figures 45c and 45d. What is the most likely diagnosis?


Explanation
Giant cell tumors typically occur in a juxta-articular location involving the epiphysis and metaphysis of long bones, usually eccentric in the bone. The radiographs show a destructive process within the distal tibia and an associated soft-tissue mass. The histology shows multinucleated giant cells in a bland matrix with a few scattered mitoses. Osteosarcoma can have a similar destructive appearance but a very different histologic pattern with osteoid production. Ewing's sarcoma also can have a diffuse destructive process in the bone. The histologic pattern of Ewing's sarcoma is diffuse round blue cells. Aneurysmal bone cysts typically are seen as a fluid-filled lesion on imaging studies and have only a scant amount of giant cells histologically. Metastatic adenocarcinoma does not demonstrate the pattern shown in the patient's histology specimen. Wold LA, et al: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, pp 198-199.
Question 145
High Yield
A 62-year-old man has cervical myelopathy with no evidence of cervical radiculopathy. MRI reveals stenosis at C4-5 and C5-6 with severe cord compression. Examination will most likely reveal which of the following findings?

Explanation
Cervical myelopathy involves compression of the spinal cord and presents as an upper motor neuron disorder. Patients commonly have extremity spasticity and problems with ambulation and balance. Hoffman's sign is often present and is elicited by suddenly extending the distal interphalangeal joint of the middle finger; reflexive finger flexion represents a positive finding. The extremities are usually hyperreflexic with myelopathy. With cervical radiculopathy (lower motor neuron disorder), reflexes are hyporeflexic, and patients report pain along a dermatomal distribution. A hyperactive jaw jerk reflex indicates pathology above the foramen magnum or in some cases, systemic disease. Flaccid paraparesis suggests a lower motor neuron problem. Sachs BL: Differential diagnosis of neck pain, arm pain and myelopathy, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 741-742.
Question 146
High Yield
Increasing articular conformity of the tibial polyethylene insert of a fixed-bearing total knee arthroplasty (TKA) prosthesis will have which of the following biomechanical effects?

Explanation
Increasing articular conformity increases the surface area for contact between the polyethylene and the femoral component. Advantages of this include lower peak contact stress within the polyethylene and less risk of polyethylene fatigue failure. Patellofemoral tracking is unchanged by increasing conformity unless gross component apposition is present. A potential disadvantage of increasing conformity includes some restriction in tibial rollback. Modest changes in conformity have not been shown to alter the rate of mechanical loosening. If conformity was increased to the extent of significant constraint, a potential increased risk of loosening would be expected, not a decrease. Design of modern TKAs includes a compromise in achieving enough constraint to lower polyethylene stress, without providing so much constraint as to limit kinematics and stress the fixation interfaces. D'Lima DD, Chen PC, Colwell CW Jr: Polyethylene contact stresses, articular congruity, and knee alignment. Clin Orthop 2001;392:232-238.
Question 147
High Yield
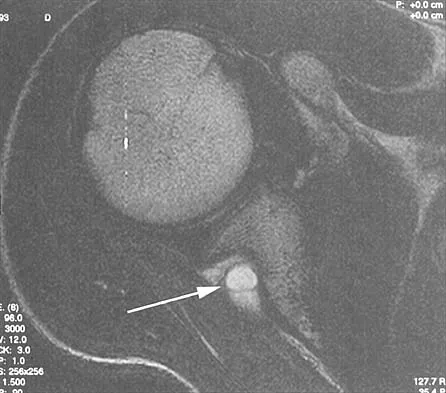
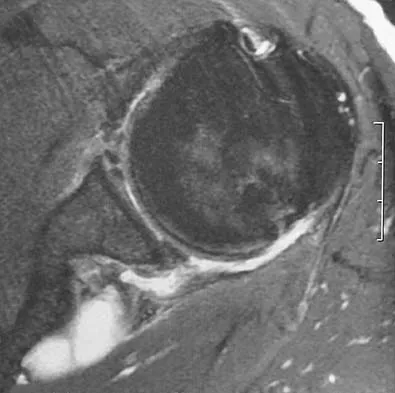
A coronal MRI scan through the shoulder joint is shown in Figure 26. The cyst indicated by the arrow will most likely cause compression of what nerve?
Explanation
The MRI scan shows a ganglion cyst in the region of the spinoglenoid notch. These are difficult to diagnose clinically but are readily apparent on MRI. They usually cause compression of the suprascapular nerve and weakness of the infraspinatus and supraspinatus muscles. Resnick D, Kang HS (eds): Internal Derangements of Joints: Emphasis on MR Imaging. Philadelphia, PA, WB Saunders, 1997, pp 306-309.
Question 148
High Yield
Figure 29 shows the radiograph of a 10-year-old boy who injured his knee playing football. What is the most appropriate initial treatment?

Explanation
Salter type I fractures of the distal femur are quite unstable; therefore, closed reduction and cast immobilization can be expected to result in high rates of redisplacement. Optimal treatment consists of open or closed reduction and smooth pin fixation, and supplemental casting is required to ensure fracture stability. Screw fixation may increase rates of growth plate injury. Blade plate or flexible nail fixation will be challenging to apply and is not necessary. Flynn JM, Skaggs DL, Sponseller PD, et al: The surgical management of pediatric fractures of the lower extremity. Instr Course Lect 2003;52:647-659. Thomson JD, Stricker SJ, Williams MM: Fractures of the distal femoral epiphyseal plate. J Pediatr Orthop 1995;15:474-478.
Question 149
High Yield
A 7-year-old girl has pain and a mass in the left scapula. A MRI scan and biopsy specimen are shown in Figures 30a and 30b. After staging studies, initial management should consist of
Explanation
The histology shows small round blue cells that are uniform in appearance; these findings are consistent with Ewing's sarcoma. The MRI scan shows infiltration of the marrow and a large surrounding soft-tissue mass. Based on these findings, the management of choice is systemic chemotherapy. Local control of the primary lesion is addressed by either surgical resection or radiation therapy or a combination of the two after the patient receives systemic chemotherapy. The clinical, radiographic, and histologic presentation of Ewing's sarcoma often can be confused with osteomyelitis. The histology shows an absence of inflammatory cells. Grier HE: The Ewing family of tumors: Ewing's sarcoma and primitive neuroectodermal tumors. Pediatr Clin North Am 1997;44:991-1004.
Question 150
High Yield
A 36-year-old man sustains a traumatic spondylolisthesis of L5 on S1. Surgical stabilization requires pedicular fixation into the sacrum. If the screw is placed in a medial to lateral direction and penetrates the sacral ala, what nerve root is at risk?
Explanation
The L5 nerve root lies directly over the superior and anterior alae. If the screw is directed approximately 20 degrees laterally and bicortical purchase is achieved, there is the risk of injuring the L5 nerve root. If the screw is directed medially into the body of S1, there is little risk of injury. The same root is at risk during placement of an iliosacral screw. Ebraheim NA, et al: Lumbosacral nerve and dorsal screw placement. Orthopedics 2000;23:245-247. Ebraheim NA, Mermer M, Xu R, Yeasting RA: Radiological evaluation of S1 dorsal screw placement. J Spinal Disord 1996;9:527-535.
Question 151
High Yield
Figure 12 shows the radiograph of a patient who has anterior knee pain. History reveals a femoral fracture at age 5 years. What is the most likely cause of the deformity?

Explanation
The radiograph shows a recurvatum deformity of the proximal tibia with growth arrest of the tibial tubercle apophysis. This deformity has been described in association with femoral shaft fractures in children and has been attributed to a clinically silent, concommitant injury to the proximal tibial physes and also to iatrogenic injury associated with a proximal tibial traction pin. Overlengthened hamstrings and rupture of the posterior cruciate ligament may lead to knee hyperextension; however, these problems should not cause bone deformity. Osgood-Schlatter disease occurs when growth is nearly complete and usually leads to prominence of the tibial tubercle. Patellar tendon rupture is rare in children and would not cause this deformity unless the repair was performed with screws across the apophysis. Hresko MT, Kasser JR: Physeal arrest about the knee associated with non-physeal injuries of the lower extremity. J Bone Joint Surg Am 1989;71:698-703.
Question 152
High Yield
Injury to which of the following structures has been reported following iliac crest bone graft harvest?
Explanation
Injury to the lateral femoral cutaneous nerve and the ilioinguinal nerve have both been described with an anterior iliac crest bone graft harvest. The lateral femoral cutaneous nerve may be injured from retraction after elevating the iliacus muscle or from direct injury when the nerve actually courses over the crest. A posterior crest harvest can injure the superior gluteal artery if a surgical instrument violates the sciatic notch. Injury to the inferior gluteal artery has not been described; it leaves the pelvis below the piriformis muscle belly and should not be at risk even with a violation of the sciatic notch. Injury to the ilioinguinal nerve has been reported from vigorous retraction of the iliacus muscle after exposing the inner table of the anterior ilium. Cluneal nerve injury may occur with posterior crest harvest, particularly if the skin incision is horizontal or extends more than 8 cm superolateral from the posterior superior iliac spine. Kurz LT, Garfin SR, Booth RE Jr: Iliac bone grafting: Techniques and complications of harvesting, in Garfin SR (ed): Complications of Spine Surgery. Baltimore, MD, Williams and Wilkins, 1989, pp 323-341.
Question 153
High Yield
A 55-year-old man sustained an isolated closed fracture of the humerus. Initial neurologic examination reveals no active wrist or finger extension. Radiographs are shown in Figures 28a and 28b. Management should consist of


Explanation
The patient has an isolated closed injury involving the humeral diaphysis. The lack of wrist and finger extension indicates injury to the radial nerve. Based on these findings, ongoing observation of the nerve is warranted with delayed exploration after 3 to 4 months if there are no signs of progressive return of nerve function. Treatment of the fracture should include external immobilization and fracture bracing. An indication for nerve exploration and surgical stabilization would be an open fracture. Zuckerman JD, Kovil KJ: Fractures of the shaft of the humerus, in Rockwood CA Jr, Green DP, Bucholz RW, Heckman JD (eds): Rockwood and Green's Fractures in Adults, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 1025-1053.
Question 154
High Yield
To avoid damage to the ascending branch of the anterior humeral circumflex artery during open reduction and internal fixation of a proximal humeral fracture, the blade plate should be placed in what position?
Explanation
The pectoralis major tendon inserts lateral to the biceps tendon, which runs in the bicipital groove. The primary vascular supply of the articular surface of the humeral head is derived from the anterior circumflex humeral artery, which continues into the arcuate artery once it enters the bone. The entry point is on the anterolateral aspect of the humerus just medial to the greater tuberosity within the bicipital groove. To avoid compromising circulation, the blade plate should be placed lateral to the bicipital groove and pectoralis major tendon insertion. Loebenberg M, Plate AM, Zuckerman J: Osteonecrosis of the humeral head. Instr Course Lect 1999;48:349-357.
Question 155
High Yield
A 22-year-old woman reports a 4-year history of worsening low back and left lower extremity pain following a motor vehicle accident. Management consisting of physical therapy, chiropractic manipulation, and interventional pain management, including sacroiliac joint injections and epidural steroid injections, has failed to provide relief. A sagittal T2-weighted MRI scan is shown in Figure 8. No nerve root compression is seen on axial images. She is currently working and lives with her fiancé. She smokes half a pack of cigarettes per day and reports depression on her health history. She is being maintained on narcotic analgesics and is having increasing difficulty performing her activities of daily living secondary to pain. What is the most appropriate management at this time?

Explanation
The MRI scan reveals a rudimentary disk at the L5-S1 level, suggesting transitional anatomy. There is a posterior disk bulge at L3-4. At L4-5, there is disk desiccation and loss of disk height, with a posterior disk bulge and a high intensity zone in the posterior annulus, suggesting an annular tear. While these and similar radiographic findings have been associated with the severity of a patient's pain, they are also commonly found in cross-sectional studies of asymptomatic subjects. Carragee and associates found 59% of symptomatic patients undergoing diskography have high intensity zones as compared to 25% of asymptomatic subjects of a similar patient profile. Diskographic injections provoked pain in disks with high intensity zones approximately 70% of the time whether the individual was previously symptomatic or not. This patient's non-specific pain pattern does not require further work-up as she is not a surgical candidate. Carragee EJ, Paragioudakis SJ, Khurana S: 2000 Volvo Award winner in clinical studies: Lumbar high-intensity zone and discography in subjects without low back problems. Spine 2000;25:2987-2992. Pneumaticos SG, Reitman CA, Lindsey RW: Diskography in the evaluation of low back pain. J Am Acad Orthop Surg 2006;14:46-55. Brox JI, Sorensen R, Friis A, et al: Randomized clinical trial of lumbar instrumented fusion and cognitive intervention and exercises in patients with chronic low back pain and disc degeneration. Spine 2003;28:1913-1921.
Question 156
High Yield
A 14-year-old boy sustained a 100% displaced distal radius Salter-Harris type II fracture. Neurologic examination demonstrates normal motor examination and two-point discrimination. He undergoes fracture reduction to the anatomic position with the application of a long arm cast. Postreduction he reports increasing hand and wrist pain with diminution of two-point discrimination to 10 mm over the index and middle fingers over the next several hours after surgery. The cast is bivalved and the padding released relieving all external pressure over the arm. Reevaluation reveals increasing sensory deficit over the affected area. What is the next most appropriate management intervention?
Explanation
The patient has an evolving acute carpal tunnel syndrome. Initial management for this injury is to relieve all external pressure that may elevate the neural compression. Surgical decompression of the median nerve at the carpal tunnel is the optimal intervention. Further nonsurgical interventions (cast removal or further bivalving) are insufficient to alleviate the neural compression. Waters PM, Mih AD: Fractures of the distal radius and ulna, in Beaty JH, Kasser JR (eds): Fractures in Children, ed 6. Philadelphia, PA, Lippincott, 2006, p 361.
Question 157
High Yield
Which of the following characteristics is seen in patients with osteochondritis dissecans of the elbow?
Explanation
Osteochondritis dissecans occurs in the older child or adolescent (typically older than age 13 years). It involves the lateral compartment. The etiology is felt to be microtraumatic vascular insufficiency from repetitive rotatory and compressive forces. MRI typically shows separation of cartilage from the capitellum and chondral fissuring. Panner's disease is usually seen in children younger than age 10 years, involves the entire capitellar ossific nucleus, and resolves typically with no residual deformity or late sequelae. There is no evidence of ligamentous injury. Defelice GS, Meunier MJ, Paletta GA: Elbow injury in the adolescent athlete, in Altchek DW, Andrews JR (eds): The Athlete's Elbow. New York, NY, Lippincott Williams & Wilkins, 2001, pp 231-248.
Question 158
High Yield
An 11-year-old boy has had a fever and pain and swelling over the lateral aspect of his right ankle for the past 3 days. Examination reveals warmth, swelling, and tenderness over the lateral malleolus, and he has a temperature of 103.2 degrees F (39.5 degrees C). Laboratory studies show a WBC count of 13,200/mm3 with 61% neutrophils, an erythocyte sedimentation rate of 112 mm/h, and a C-reactive protein of 15.7. Radiographs and a T2-weighted MRI scan are shown in Figures 13a through 13c. Aspiration yields 1 mL of purulent fluid. Management should now consist of



Explanation
The initial signs and symptoms of acute hematogenous osteomyelitis vary widely but usually include fever, bone pain, and impaired use of the involved extremity. In lower extremity infections, the child may limp or refuse to walk. Examination often reveals bone tenderness. In more advanced cases, erythema, warmth, and swelling may be present. The WBC and neutrophil counts are not always elevated, but the erythocyte sedimentation rate will be abnormal in more than 90% of patients. When the infection is diagnosed early, before a subperiosteal abscess has formed, antibiotics alone may be adequate to treat the infection. This patient has a more advanced infection, however, with the MRI scan revealing a subperiosteal abscess that was confirmed by aspiration. When an abscess is present, surgical drainage is generally indicated to remove devitalized tissue and to enhance the efficacy of the antibiotics. Further studies, such as bone or indium scans, are not necessary and will delay definitive treatment. Scott RJ, Christofersen MR, Robertson WW Jr, et al: Acute osteomyelitis in children: A review of 116 cases. J Pediatr Orthop 1990;10:649-652.
Question 159
High Yield
A 38-year-old man who is an avid tennis player has had persistent pain over the medial aspect of his knee for the past 6 years. He notes that the pain occurs on a daily basis with any significant activity. Nonsteroidal anti-inflammatory drugs have failed to provide relief. Radiographs are shown in Figures 22a and 22b. What is the best course of action?


Explanation
In a relatively young patient who is an avid tennis player, the treatment of choice is a joint preserving procedure. The radiographs reveal varus alignment with loading of the medial compartment. After all nonsurgical management options have been used, the best treatment option is a medial opening wedge osteotomy. A lateral closing wedge osteotomy of the proximal tibia is also a reasonable option, but it is not one of the choices. A unicompartmental arthroplasty or a total knee arthroplasty would place significant restrictions in this patient. A unispacer may be a temporizing procedure but is controversial and without substantial data in the literature. The knee arthroscopy will not address the medial compartment osteoarthritis. Nagel A, Insall JN, Scuderi GR: Proximal tibial osteotomy: A subjective outcome study. J Bone Joint Surg Am 1996;78:1353-1358. Rinonapoli E, Mancini GB, Corvaglia A, et al: Tibial osteotomy for varus gonarthrosis: A 10- to 21-year followup study. Clin Orthop 1998;353:185-193.
Question 160
High Yield
A 47-year-old woman underwent a distal chevron bunionectomy 2 months ago. Her postoperative recovery had been uneventful until 1 week ago. She now has new onset pain and dorsal swelling in the area of the third metatarsal. A radiograph is shown in Figure 27. What is the most likely diagnosis?

Explanation
Based on findings of a sudden increase in pain with associated swelling, the most likely diagnosis is a stress fracture. The initial radiographic findings usually will be negative. Morton's neuroma and transfer metatarsalgia are not associated with swelling. Metatarsophalangeal synovitis usually involves the second metatarsophalangeal joint. Freiberg's infraction is seen clearly on a radiograph.
Question 161
High Yield
A 15-year-old girl reports popping and clicking at the sternoclavicular joint and an intermittent asymmetrical prominence of the medial head of the clavicle. She denies any history of trauma or other symptoms. Management should consist of
Explanation
Atraumatic subluxation or dislocation of the sternoclavicular joint typically occurs in individuals with generalized ligamentous laxity. It is generally not painful, has no long-term sequelae, and needs no treatment. In fact, it is more likely to be painful following surgery than if managed nonsurgically. Rockwood CA Jr, Odor JM: Spontaneous atraumatic anterior subluxation of the sternoclavicular joint. J Bone Joint Surg Am 1989;71:1280-1288.
Question 162
High Yield
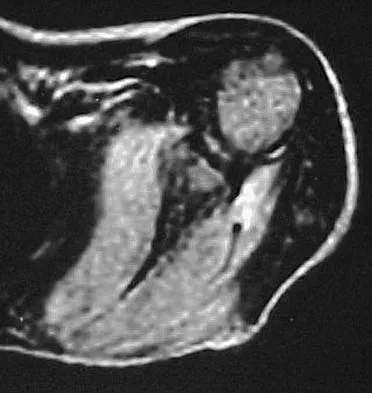
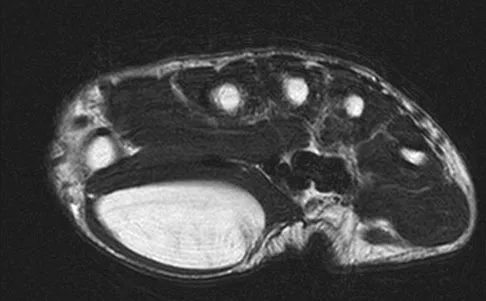
When performing surgical excision of the lesion shown in the MRI scan in Figure 3, what nerve is most likely at risk?
Explanation
The MRI scan shows a large mass (lipoma) in the thenar muscles of the palm. The recurrent motor branch of the median nerve innervates the thenar muscles. The anterior interosseous nerve (AIN) in the proximal forearm innervates the flexor pollicis longus, pronator quadratus, and flexor digitorum pollicis to the index and frequently the middle finger. The terminal branch of the AIN innervates only the wrist capsule. The palmar cutaneous branch of the ulnar nerve is a sensory structure to the hypothenar area. There is no commonly described recurrent branch of the ulnar nerve.
Question 163
High Yield
A patient who underwent primary total hip arthroplasty 7 years ago that resulted in excellent pain relief and a normal gait now reports pain and a limp. Postoperative and current AP radiographs are shown in Figures 2a and 2b. What is the most likely cause of the pathology seen?


Explanation
Osteolysis in the trochanteric bed can result in weakening of the bone and fracture. Nonsurgical management will provide reasonable clinical and radiographic results in patients with limited fracture displacement. Claus MC, Hopper RH, Engh CA: Fractures of the greater trochanter induced by osteolysis with the anatomic medullary locking prosthesis. J Arthroplasty 2002;17:706-712.
Question 164
High Yield
In the treatment of acetabular dysplasia, what type of pelvic osteotomy leaves the "teardrop" in its original position and redirects the acetabulum?

Explanation
The dial or spherical osteotomy leaves the medial wall or teardrop in its original position and, as a result, is intra-articular. The other pelvic osteotomies (except Chiari) redirect the acetabulum, including the medial wall. The Chiari osteotomy improves coverage without redirecting the acetabulum within the pelvis, and it leaves the teardrop in the same place. Lack W, Windhager R, Kutschera HP, Engel A: Chiari pelvic osteotomy for osteoarthritis secondary to hip dysplasia: Indications and long-term results. J Bone Joint Surg Br 1991;73:229-234. Ganz R, Klaue K, Vinh TS, Mast JW: A new periacetabular osteotomy for the treatment of hip dysplasias: Technique and preliminary results. Clin Orthop 1988;232:26-36.
Question 165
High Yield
A 23-year-old baseball pitcher reports pain in the posterior aspect of his dominant shoulder during the late cocking phase of throwing. With the dominant shoulder positioned in 90 degrees of abduction from the body and with the scapula stabilized, examination reveals 135 degrees of external rotation and 20 degrees of internal rotation. Examination of the opposite shoulder reveals 100 degrees of external rotation and 75 degrees of internal rotation. Both shoulders are stable on examination. Radiographs and MRI scans are unremarkable. What is the primary cause of his pain?
Explanation
Internal impingement of the shoulder is a leading cause of shoulder pain in the throwing athlete. The primary lesion in pathologic internal impingement is excessive tightening of the posterior band of the inferior glenohumeral ligament complex. To obtain an accurate assessment of true glenohumeral rotation, the scapula is stabilized during examination. A loss of 20 degrees or more of internal rotation, as measured with the shoulder positioned in 90 degrees of abduction, indicates excessive tightness of the posterior band of the inferior glenohumeral ligament complex. Burkhart SS, Morgan CD, Kibler WB: The disabled throwing shoulder: Spectrum of pathology. Part I: Pathoanatomy and biomechanics. Arthroscopy 2003;19:404-420.
Question 166
High Yield
A 15-year-old baseball pitcher who reports increasing pain in his right shoulder over the past 3 weeks states that the pain increases the more he pitches. Radiographs of both shoulders are shown in Figures 35a and 35b. What is the next most appropriate step in management?


Explanation
The patient has a rotational stress fracture of the proximal humeral physis (Little Leaguer's shoulder). The symptoms of increasing pain with activity and relief with rest are typical of a stress injury. Treatment should consist of cessation of throwing activity but rehabilitation of the shoulder girdle muscles. The pitching technique should be evaluated as well. Barnett LS: Little League shoulder syndrome: Proximal humeral epiphyseolysis in the adolescent baseball pitchers: A case report. J Bone Joint Surg Am 1985;67:495-496.
Question 167
High Yield
During an anterior approach to the shoulder, excessive traction on the conjoined tendon is most likely to result in loss of
Explanation
The musculocutaneous nerve travels through the conjoined tendon approximately 8 cm distal to the tip of the acromion. The musculocutaneous nerve innervates the biceps muscle and the bracialis muscle, both of which are responsible for elbow flexion. Shoulder flexion is facilitated by the anterior fibers of the deltoid muscle (axillary nerve) and the supraspinatus muscle (suprascapular nerve). The subscapular muscle facilitates internal rotation of the shoulder (upper and lower subscapularis nerve). Shoulder abduction is performed by the deltoid muscle (axillary nerve), and forearm pronation is facilitated by the pronator teres (median nerve). Hollinshead WH: Anatomy for Surgeons: The Back and Limbs, ed 3. Philadelphia, PA, Harper and Row, 1982, pp 391-393.
Question 168
High Yield
What range of motion parameters are required for a patient with posttraumatic elbow stiffness to accomplish all the normal activities of daily living?
Explanation
Activities of daily living such as dressing, eating, and bathing can all be performed with elbow motion through a 100 degrees arc of flexion and extension (30 degrees to 130 degrees) and a 100 degrees arc of forearm rotation (50 degrees pronation, 50 degrees supination). Some patients can accomplish these activities of daily living with 10 degrees less motion at each end point. This is referred to as the functional arc of motion. Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 283-294.
Question 169
High Yield
Figure 44 shows the radiograph of a 65-year-old man who underwent a revision arthroplasty to remove a loose, cemented femoral stem. When planning the postoperative restrictions, the surgeon should be aware that

Explanation
The transfemoral approach, also known as the extended trochanteric osteotomy, is an important technique to master for revision hip surgery. When performed correctly, it allows excellent exposure of the femoral canal and aids in exposure of the acetabulum. As demonstrated in the study cited, however, it markedly reduces the torque that the composite can withstand without failure. This type of basic science study is important to guide postoperative rehabilitation.
Question 170
High Yield
Familial (Leiden) thrombophilia is of importance in joint arthroplasty because of an abnormality in the clotting cascade. Which of the following statements best describes the condition?
Explanation
Factor V Leiden is a disease caused by an abnormality of factor V in which a single amino acid substitution of glutamine for arginine in the protein C cleavage region leads to decreased inactivation of factor V and thus a greater tendency to form clots. More than half of all individuals with Factor V Leiden will develop deep venous thrombosis in the presence of a single additional risk factor such as long bone fracture or total joint arthroplasty.
Question 171
High Yield
A 37-year-old electrician is diagnosed with a frozen shoulder after sustaining an electrical injury at work 2 weeks ago. Examination reveals that he cannot actively or passively externally rotate or abduct the arm. The glenohumeral joint and scapula move in a 1:1 ratio. Radiographs are shown in Figures 15a and 15b. The best course of action should be


Explanation
The patient's history, examination, and radiographs are classic for locked posterior dislocation of the glenohumeral joint. Posterior dislocation of the shoulder remains the most commonly missed dislocation of a major joint. Up to 80% are missed on initial presentation. The primary cause for failure to accurately diagnose this injury is inadequate radiographic evaluation. The typical presentation is a shoulder locked in internal rotation with loss of abduction. An axillary view not only will make the definitive diagnosis but will help assess the size of the articular surface defect and help plan treatment. This view can be done expediently as part of every trauma series. The AP view is suspicious for a posteriorly dislocated humerus with loss of the humeral neck profile, a vacant glenoid sign, and an anterior humeral head compression fracture (reverse Hill-Sachs lesion). Hawkins RJ, Neer CS II, Pianta RM, Mendoza FX: Locked posterior dislocation of the shoulder. J Bone Joint Surg Am 1987;69:9-18. Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow. Rosement, IL, American Academy of Orthopaedic Surgeons, 1997, pp 181-189.
Question 172
High Yield
What is the most important stabilizing mechanism in the midrange of motion of the glenohumeral joint?
Explanation
Concavity compression is a stabilizing mechanism by which muscular compression of the humeral head into the glenoid fossa stabilizes the glenohumeral joint against shear forces. This is dependent on the depth of the concavity and the magnitude of the compressive force. Lee SB, Kim KJ, O'Driscoll SW, et al: Dynamic glenohumeral stability provided by the rotator cuff muscles in the mid-range and end-range of motion: A study in cadavera. J Bone Joint Surg Am 2000;82:849-857.
Question 173
High Yield
A 13-year-old boy sustains a valgus stress injury to the knee while playing football, and he is unable to bear weight after the injury. Examination reveals tenderness medially superior to the joint line. The knee is held in flexion, and he has a large effusion and localized medial swelling. Plain radiographs show no obvious fracture. What is the next diagnostic step?
Explanation
In the skeletally mature individual, this mechanism of injury will often result in a sprain of the medial collateral ligament. In skeletally immature patients, the same mechanism can cause a fracture of the distal femoral physis. If the fracture is nondisplaced, the plain radiographs may show only soft-tissue swelling or effusion. While the MRI scan may show edema in the soft tissues on the medial side of the knee and even an abnormality of the physis, stress radiographs provide a quicker and less expensive means of making the diagnosis. Arthroscopy and arthrography would not be helpful in making the diagnosis. Arthroscopy may result in further displacement of the injury. Smith L: Concealed injury to the knee. J Bone Joint Surg Am 1962;44:1659-1660.
Question 174
High Yield
What is the primary intracellular signaling mediator for bone morphogenetic protein (BMP) activity?
Explanation
BMPs signal through the activation of a transmembrane serine/threonine kinase receptor that leads to the activation of intracellular signaling molecules called SMADs. There are currently eight known SMADs, and the activation of different SMADs within a cell leads to different cellular responses. The other mediators are not believed to be directly involved with BMP signaling. Lieberman J, Daluiski A, Einhorn TA: The role of growth factors in the repair of bone: Biology and clinical applications. J Bone Joint Surg Am 2002;84:1032-1044. Li J, Sandell LJ: Transcriptional regulation of cartilage-specific genes, in Rosier RN, Evans C (eds): Molecular Biology in Orthoapedics, Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 21-24.
Question 175
High Yield
A 39-year-old man has had persistent right shoulder pain for the past 6 months. A formal physical therapy program has failed to provide relief, and an injection several months ago provided only short-term relief. Examination reveals a positive Neer and Hawkins test. There is no instability and the neurovascular examination is normal. Arthroscopy reveals a partial rotator cuff tear on the bursal side measuring 60% of the tendon thickness. What is the next most appropriate step in management?

Explanation
Although arthroscopic debridement with or without subacromial decompression is a reasonable response, the patient has positive impingement signs. Several recent studies regarding the surgical treatment of partial rotator cuff tears have demonstrated good to excellent results after repair of tears involving more than 50% of the tendon thickness. This was shown specifically for bursal-sided tears and joint-side tears. Biceps tenotomy is not indicated in a young patient. Matava MJ, Purcell DB, Rudzki JR: Partial-thickness rotator cuff tears. Am J Sports Med 2005;33:1405-1417.
Question 176
High Yield
Acetaminophen is an antipyretic medication. It exerts its pharmacologic effects by inhibiting which of the following enzymes?
Explanation
Acetaminophen inhibits prostaglandin E2 production via IL-1 B, without affecting cyclooxygenase-2 enzymatic activity. The therapeutic concentrations of acetaminophen induce an inhibition of IL-1 B-dependent NF-kappa B nuclear translocation. The selectivity of this effect suggests the existence of an acetaminophen-specific activity at the transcriptional level that may be one of the mechanisms through which the drug exerts its pharmacologic effects. Acetaminophen does not affect any of the other enzymes named above.
Question 177
High Yield
After excising a mass from the thigh that was thought to be a lipoma, the pathology reveals that the mass is a high-grade sarcoma. Subsequent treatment should include

Explanation
Following excision of a suspected benign soft-tissue tumor that proves to be malignant, repeat excision of the tumor bed is recommended. The initial surgical margins are inadequate after an intralesional or marginal excision, necessitating additional surgery for more definitive local control. While radiation therapy and/or chemotherapy may help to reduce the risk of local recurrence in patients with microscopic residual disease, local control is improved following repeat excision. Radiation therapy alone is inadequate to address poor surgical margins, and would likely be given postoperatively. Bisphosphonates have no current role in the treatment of soft-tissue sarcoma. Noria S, Davis A, Kandel R, et al: Residual disease following unplanned excision of soft-tissue sarcoma of an extremity. J Bone Joint Surg Am 1996;78:650-655.
Question 178
High Yield
Figure 48 shows an MRI scan of the knee. The arrow is pointing to what structure?

Explanation
The arrow points to the biceps femoris, which is inserted onto the fibula. The biceps femoris lies at the posterolateral aspect of the thigh. The semimembranosus and the semitendinous lie at the posterior medial aspect of the thigh. Gray H: Anatomy of the Human Body. Philadelphia, PA, Lea and Febiger, 1918, 2000.
Question 179
High Yield
Figure 16 shows the radiograph of a 23-year-old man who has severe right shoulder pain after his motorcyle hit a bridge guardrail. He is neurologically intact. Nonsurgical management will most likely result in

Explanation
Internal fixation of the clavicle, glenoid, or both has been recommended for fractures of the clavicle and glenoid neck (floating shoulders). Recently, the inherent instability of these dual fractures has been questioned in a biomechanical model without further disruption of the coracoclavicular or acromioclavicular ligamentous structures. Nonsurgical management of the majority of combined scapular/glenoid fractures in patients with less than 10 mm of displacement has resulted in excellent shoulder function and will most likely achieve an excellent result in this patient. Egol KA, Connor PM, Karunakar MA, Sims SH, Bosse MJ, Kellam JF: The floating shoulder: Clinical and functional results. J Bone Joint Surg Am 2001;83:1188-1194. Williams GR Jr, Naranja J, Klimkiewicz J, et al: The floating shoulder: A biomechanical basis for classification and management. J Bone Joint Surg Am 2001;83:1182-1187.
Question 180
High Yield
A 34-year-old man underwent a transtibial amputation as the result of a work-related injury. The amputation was performed at the inferior level of the tibial tubercle. The residual limb has a soft-tissue envelope composed of gastrocnemius muscle that is used as soft-tissue cushioning for the distal tibia. Despite undergoing several prosthetic fittings, he continues to report pain and instability. Examination reveals that the prosthesis appears to fit well with no apparent pressure points or areas of skin breakdown. He is not willing to have any further surgery. Which of the following modifications will most likely provide relief?
Explanation
While transtibial amputees can be fitted with a prosthesis with a residual limb as short as 5 cm, or with retention of the insertion of the patellar tendon, this patient has an unstable gait because of the limited ability of the prosthetic socket to maintain a snug and stable fit. While cumbersome and bulky, double metal uprights and a corset is the only predictable method of gaining stability. The other methods attempt to add an element of stability; however, they are unlikely to be successful. Bowker JH, Goldberg B, Poonekar PD: Transtibial amputation: Surgical procedures and postsurgical management, in Bowker JH, Michael JW (eds): Atlas of Limb Prosthetics. St Louis, MO, Mosby Year Book, 1992, pp 429-452.
Question 181
High Yield
An otherwise healthy 32-year-old man who underwent an uneventful L5-S1 lumbar microdiskectomy 6 weeks ago now reports increasing and severe back pain that awakens him from sleep. Examination reveals a benign-appearing wound, and the neurologic examination is normal. Laboratory studies show an erythrocyte sedimentation rate (ESR) of 90 mm/h and a WBC of 9,000/mm3. Plain radiographs are normal. What is the next most appropriate step in management?
Explanation
The patient's history and laboratory studies are very suspicious for a postoperative diskitis. The predominant symptom often is back pain. An ESR of 90 mm/h is considered significantly elevated and normally would be expected to return to near baseline by 2 weeks postoperatively. A normal WBC result is not unusual with postoperative diskitis. Management should consist of an MRI with gadolinium to confirm the diagnosis, followed by a biopsy percutaneously to obtain tissues for pathology and microbiology. Surgical debridement is reserved for patients whose percutaneous biopsy results are negative and a high index of suspicion for diskitis remains, or when management consisting of IV antibiotics, bed rest, and spinal immobilization fails to provide relief. Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 257-271.
Question 182
High Yield
Figure 55 shows the radiograph of a 30-year-old man who sustained a closed comminuted fracture of the right clavicle. Examination reveals decreased sensation in the radial nerve distribution. Weakness is noted with shoulder abduction, internal rotation, and wrist extension. A displaced bone fragment is most likely pressing on what portion of the brachial plexus?

Explanation
Clavicular fractures are occasionally complicated by injury to the brachial plexus. A displaced bone fragment pressing on the posterior cord proximal to the upper subscapularis nerve would account for these findings. Jobe CM, Coen MJ: Gross anatomy of the shoulder, in Rockwood CA, Matsen FA, Wirth MA, et al (eds): The Shoulder. Philadelphia, PA, WB Saunders, 2004, vol 2, pp 1078-1079.
Question 183
High Yield
Figures 30a and 30b show the MRI scans of a 51-year-old woman who has had an enlarging soft-tissue mass in her right thigh for the past 18 months. Examination reveals no inguinal adenopathy. Results of a biopsy show a high-grade sarcoma. A bone scan is unremarkable, and a CT scan of the chest shows no evidence of pulmonary metastasis. According to the Musculoskeletal Tumor Society (MSTS) staging system, the tumor should be classified as what stage?
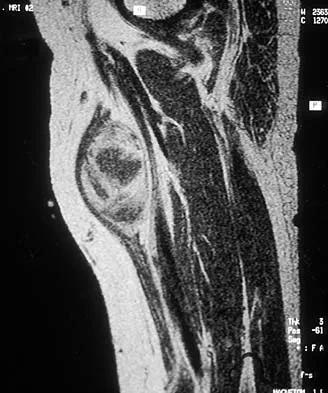
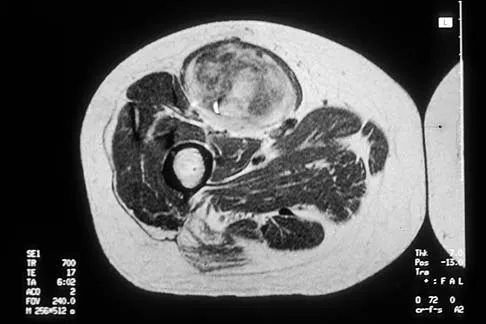
Explanation
According to the MSTS staging system, soft-tissue sarcomas are staged according to the following factors: grade, site, and metastasis. Roman numerals are used to designate malignant tumors, and Arabic numerals are used for benign tumors. Low-grade malignant tumors are staged as I while intermediate- and high-grade tumors are staged as II. Site is defined as intracompartmental (A) or extracompartmental (B). Any metastasis is staged as III. This patient has a high-grade tumor (II), and the MRI scans show that it is confined to a single compartment; therefore, it is staged as IIA. There is no evidence of metastatic disease. Enneking WF, Spanier SS, Goodman MA: A system for the surgical staging of musculoskeletal sarcoma. Clin Orthop 1980;153:106-120. Peabody TD, Monson D, Montag A, Schell MJ, Finn H, Simon MA: A comparison of the prognoses for deep and subcutaneous sarcomas of the extremities. J Bone Joint Surg Am 1994;76:1167-1173. Pisters PW, Leung DH, Woodruff J, Shi W, Brennan MF: Analysis of prognostic factors in 1,041 patients with localized soft tissue sarcomas of the extremities. J Clin Oncol 1996;14:1679-1689.
Question 184
High Yield
Anterior subluxation in a throwing athlete is most commonly the result of

Explanation
Subtle anterior subluxation in the throwing athlete most frequently results from excessive capsular laxity because of repetitive microtrauma. Avulsion of the inferior glenohumeral ligament from the glenoid, or more rarely from the humerus, occurs with macrotrauma. A large Hill-Sachs lesion and a glenoid rim fracture also may result from a traumatic anterior dislocation. Kvitne RS, Jobe FW: The diagnosis and treatment of anterior instability in the throwing athlete. Clin Orthop 1993;291:107-123.
Question 185
High Yield
A 20-year-old man reports painless snapping about the lateral aspect of the right hip. He denies any history of trauma. Examination reveals no limp or tenderness. Hip range of motion is full, and there is good strength. Radiographs are normal. What anatomic structure is most likely causing these symptoms?
Explanation
Coxa saltans (snapping hip syndrome) can occur in two forms: external/lateral or interior/medial/anterior. This patient has the external/lateral form. The external/lateral form involves the iliotibial band, tensor fascia, or gluteus medius, which snaps over the greater trochanter. The external form usually can be treated with physical therapy alone; however, several recent studies report satisfactory results with surgical treatment. Faraj and associates reported good results from surgical Z-plasty in a series of 10 patients. White and associates reported good results in a series of 16 patients with 17 hips who underwent surgical release of an external snapping hip. The interior/medial/anterior form can involve the iliopsoas tendon, acetabular labrum, subluxation of the hip, and loose bodies. White RA, Hughes MS, Burd T, et al: A new operative approach in the correction of external coxa saltans: The snapping hip. Am J Sports Med 2004;32:1504-1508. Faraj AA, Moulton A, Sirivastava VM: Snapping iliotibial band: Report of ten cases and review of the literature. Acta Orthop Belg 2001;67:19-23.
Question 186
High Yield
A 7-year-old boy has had chronic left leg pain that is worse at night but is not activity related. Use of nonsteroidal anti-inflammatory drugs for the past 6 months has failed to provide relief. A CBC count with differential, erythrocyte sedimentation rate, and C-reactive protein are within normal limits. Radiographs and a CT scan are shown in Figures 31a through 31c. Management should consist of


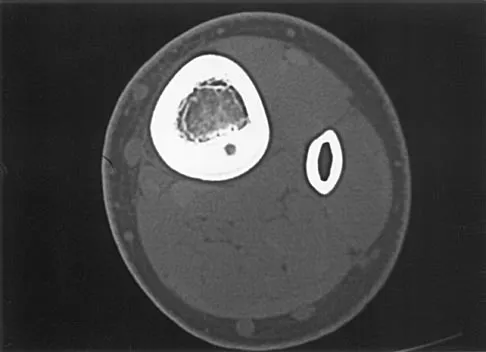
Explanation
Osteoid osteomas are painful bone lesions, with radiographs revealing a dense sclerotic cortex surrounding a small radiolucency or nidus. Symptoms often are worse at night but usually are not activity related. While treatment in the past has consisted of open en bloc excision, current means of removal include percutaneous drilling under CT guidance and percutaneous radiofrequency coagulation. Success rates of percutaneous treatment are comparable to those seen following open procedures. The characteristic radiographic appearance of this lesion usually obviates the need for biopsy. Because the lesion is not caused by pyogenic organisms, antibiotics are not indicated. Donahue F, Ahmad A, Mnaymneh W, Pevsner NH: Osteoid osteoma: Computed tomography guided percutaneous excision. Clin Orthop 1999;366:191-196.
Question 187
High Yield
A 24-year-old female soccer player has had lateral joint line pain and a recurrent effusion in the left knee after sustaining a twisting injury 6 weeks ago. She reports that symptoms worsen with athletic activities. MRI scans are shown in Figures 2a through 2c. What is the most likely diagnosis?

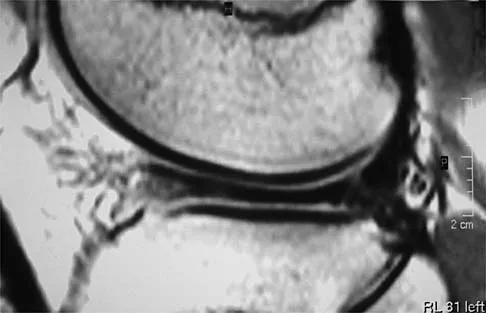
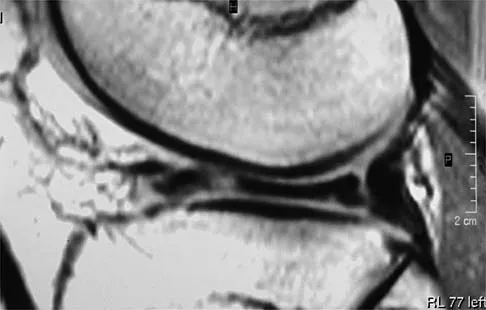
Explanation
The MRI scans show the typical findings of a torn discoid lateral meniscus. The average transverse diameter of the lateral meniscus is 11 or 12 mm. A discoid lateral meniscus is suggested when three or more contiguous 5-mm sagittal sections on the MRI scan show continuity of the menicus between the anterior and posterior horns, or when two adjacent peripheral sagittal 5-mm sections show equal meniscal height. Normally the black "bow tie" would be seen on two contiguous sagittal sections. The presence of a discoid meniscus can be further confirmed if coronal views reveal increased width. Jordan MR: Lateral meniscal variants: Evaluation and treatment. J Am Acad Orthop Surg 1996;4:191-200.
Question 188
High Yield
Creatine is currently being used by athletes as a dietary supplement in an attempt to enhance performance. What is the physiologic basis for its use?
Explanation
Creatine is currently used as a nutritional supplement in an attempt to enhance athletic performance. The physiologic basis for its use is based on its conversion by CK to PCr, which acts as an energy reservoir in muscle cells for the production of ATP. A number of studies that examined the effect of creatine supplementation on performance concluded that while creatine does not increase peak force production, it can increase the amount of work done in the first few anaerobic short duration, maximal effort trials. The mechanism for this enhancement of work is unknown, but it is most likely secondary to the increase in the available PCr pool. Greenhaff PL: Creatine and its application as an ergogenic aid. Int J Sport Nutr 1995;5:S100-S110. Greenhaff PL, Casey A, Short AH, Harris R, Soderlund K, Hultman E: Influence of oral creatine supplementation on muscle torque during repeated bouts of maximal voluntary exercise in man. Clin Sci 1993;84:565-571. Trump ME, Heigenhauser GJ, Putman CT, Spriet LL: Importance of muscle phosphocreatine during intermittent maximal cycling. J Appl Physiol 1996;80:1574-1580.
Question 189
High Yield
A 25-year-old man sustained the closed injury shown in Figures 22a and 22b. Examination reveals that this is an isolated injury, and he is hemodynamically stable. Treatment should consist of


Explanation
The treatment of choice for closed diaphyseal femoral fractures in adults is reamed intramedullary nailing with static interlocking. Reaming allows placement of a larger, stronger implant and offers better healing rates than unreamed nailing. Static interlocking ensures that there is no loss of reduction because of underappreciated fracture lines or comminution. Brumback RJ, Virkus WW: Intramedullary nailing of the femur: Reamed versus nonreamed. J Am Acad Orthop Surg 2000;8:83-90.
Question 190
High Yield
Failure of high tibial osteotomy (HTO) is most closely associated with which of the following factors?
Explanation
Long-term survivorship studies have attempted to clarify patient factors related to good outcomes in HTO. One particular study showed that a patient age of less than 50 years was related to good outcomes in those who had good preoperative knee flexion. The same study found no relation between HTO failure and the presence of postoperative infection or deep venous thrombosis. The presence of a lateral tibial thrust is a contraindication to performing this surgery. As expected, good patient selection is critical to obtaining good long-term results with HTO. Naudie D, Borne RB, Rorabeck CH, Bourne TJ: Survivorship of the high tibial valgus osteotomy: A 10- to 22-year followup study. Clin Orthop 1999;367:18-27. Rinonapoli E, Mancini GB, Corvaglia A, Musiello S: Tibial osteotomy for varus gonarthrosis: A 10- to 21-year followup study. Clin Orthop 1998;353:185-193.
Question 191
High Yield
Bleeding is encountered while developing the internervous plane between the tensor fascia lata and the sartorius during the anterior approach to the hip. The most likely cause is injury to what artery?
Explanation
The ascending branch of the lateral femoral circumflex artery crosses the gap between the tensor fascia lata and the sartorious and must be identified and ligated or coagulated. The other vessels are out of the field of dissection. Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, p 312.
Question 192
High Yield
A 25-year-old man injured his dominant shoulder after falling on his outstretched arm 4 months ago. Examination reveals that he cannot lift his arm above 90 degrees, and he has pronounced medial scapular winging. Management should consist of

Explanation
Serratus anterior palsy or long thoracic nerve palsy is usually caused by traction injury to the nerve, blunt injury, or iatrogenic injury. The palsy results in winging of the scapula and medial rotation of the inferior pole of the scapula. A patient with this injury will usually recover in 12 to 18 months. Initial treatment should include observation and shoulder strengthening exercises. Nerve exploration with repair has not proven beneficial in changing the outcome. Many orthopaedic surgeons favor using a split pectoralis major transfer for symptomatic patients. Electrodiagnostic studies are helpful in confirming the diagnosis. Post M: Pectoralis major transfer for winging of the scapula. J Shoulder Elbow Surg 1995;4:1-9.
Question 193
High Yield
A 65-year-old man has a painful mass of the middle finger. A clinical photograph, lateral radiograph, coronal MRI scan, and biopsy specimen are seen in Figures 20a through 20d. What is the most likely diagnosis?



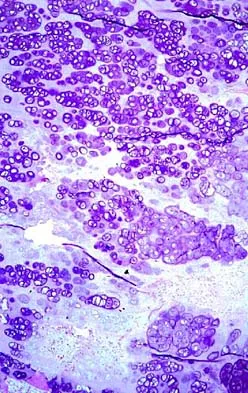
Explanation
Although the degeneration of an isolated benign cartilaginous lesion into a chondrosarcoma is rare, it occurs in roughly 10% of patients with Ollier's disease. Pain is the most common symptom of chondrosarcoma. The treatment of low-grade chondrosarcoma ranges from intralesional excision to wide amputation. The intent of the surgery is to remove all the disease to decrease the chance of local recurrence. Lee FY, Mankin HJ, Fondren G, et al: Chondrosarcoma of bone: An assessment of outcome. J Bone Joint Surg Am 1999;81:326-338.
Question 194
High Yield
A 37-year-old man who works in a factory has isolated, lateral unicompartmental pain about his knee with activities. Nonsurgical management has failed to provide relief. The radiograph shown in Figure 45 reveals a tibiofemoral angle of approximately 15 degrees which is clinically correctable to neutral. What is the best surgical option in this patient?

Explanation
Patients with a valgus alignment about the knee can have lateral compartment arthritis. Similar to a high tibial osteotomy, a supracondylar femoral osteotomy is indicated in younger patients who have a more active lifestyle and isolated unicompartmental disease. In this young patient who works in a factory and has a valgus knee, a medial closing wedge supracondylar femoral osteotomy is the treatment of choice. The role of arthroplasty is limited in younger patients. Mathews J, Cobb AG, Richardson S, et al: Distal femoral osteotomy for lateral compartment osteoarthritis of the knee. Orthopedics 1998;21:437-440.
Question 195
High Yield
A 42 year-old-woman who underwent surgery for lumbar scoliosis 2 years ago now has fixed sagittal plane imbalance and severe back pain. Which of the following is considered a contraindication to isolated pedicle subtraction osteotomy for the treatment of iatrogenic flatback syndrome in this patient?
Explanation
Pedicle subtraction osteotomy is the preferred osteotomy technique for the treatment of many patients with iatrogenic flatback syndrome. In the presence of an anterior pseudarthrosis, however, it must be done in conjunction with an anterior procedure. Prior laminectomy is not a contraindication. Significant correction, usually averaging about 30 degrees, can be obtained through each osteotomy. Osteotomies should be performed at L2 or below in the presence of kyphosis at the thoracolumbar junction. The pedicle subtraction technique is preferred with vascular calcifications because it does not lengthen the anterior column, which could risk vascular injury. Potter BK, Lenke LG, Kuklo TR: Prevention and management of iatrogenic flatback deformity. J Bone Joint Surg Am 2004;86:1793-1808.
Question 196
High Yield
What is the major difference in outcome following open reduction and internal fixation (ORIF) of the tibial plafond at 2 to 5 days versus 10 to 20 days?
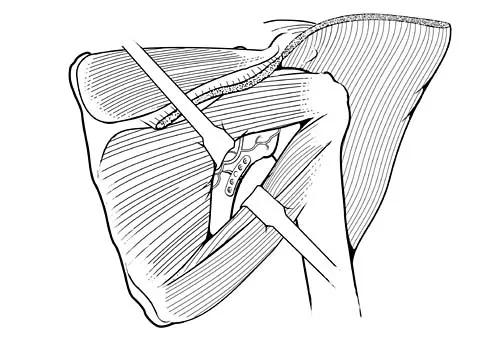
Explanation
Long-term outcomes following tibial plafond fractures treated with ORIF are satisfactory in most patients despite a high incidence of posttraumatic osteoarthritis. If ORIF is delayed until 10 to 20 days following injury, the major difference in outcomes is fewer complications associated with wound healing. Ankle strength, pain, range of motion, and the development of arthritis are equal regardless of the time until fixation. Sirkin M, Sanders R, DePasquale T, et al: A staged protocol for soft tissue management in the treatment of complex pilon fractures. J Orthop Trauma 1999;13:78-84.
Question 197
High Yield
According to the Third National Acute Spinal Cord Injury Study (NASCIS 3), what is the recommended protocol for a patient who sustained a spinal cord injury 7 hours ago?
Explanation
NASCIS 2 established the recommended doses of methylprednisolone for spinal cord injury. This included an initial bolus of 30 mg/kg over 1 hour, followed by an infusion of 5.4 mg/kg/h for an additional 23 hours. If the injury was more than 8 hours old, the methylprednisolone was not recommended. NASCIS 3 changed the dosing schedule based on the time from injury. If the time from injury to treatment was less than 3 hours, the standard protocol was followed (30 mg/kg bolus followed by 5.4 mg/kg/h for 23 hours). If the time from injury to treatment was between 3 and 8 hours, the infusion was continued at 5.4 mg/kg for an additional 23 hours (48 hours total). In this situation with a time of injury 7 hours ago, treatment should consist of a bolus and further steroid therapy for 48 hours. Bracken MB, Shepard MJ, Holford TR, et al: Administration of methylprednisolone for 24 or 48 hours or tirilazad mesylate for 48 hours in the treatment of acute spinal cord injury: Results of the Third National Acute Spinal Cord Injury Randomized Controlled Trial. National Acute Spinal Cord Injury Study. JAMA 1997;277:1597-1604.
Question 198
High Yield
A 21-year-old woman sustained a minimally displaced traumatic spondylolisthesis of C2 (Hangman's fracture) after striking the windshield with her forehead during a motor vehicle accident. Management should consist of
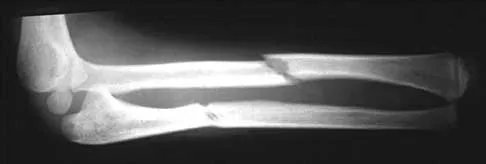
Explanation
According to the classification of Levine and Edwards, a type I Hangman's fracture is minimally displaced without angulation and represents a stable injury. Good clinical success has been achieved with nonsurgical management consisting of use of a rigid collar until the patient reports pain relief, followed by quick mobilization.
Question 199
High Yield
The cervical disk herniation shown in the MRI scans in Figures 30a and 30b will most likely create which of the following constellations of symptoms?

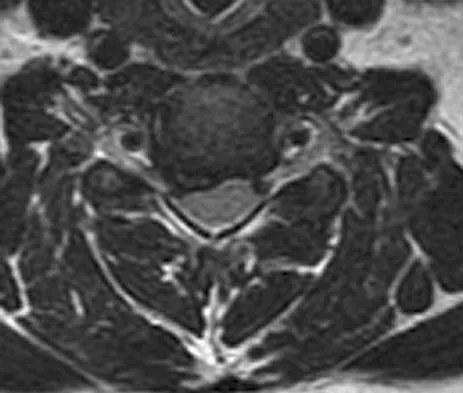
Explanation
The MRI scans reveal a right-sided C5-6 herniated nucleus pulposus. A disk herniation in this region encroaches on the C6 root and is accompanied by a sensory change along the thumb and index finger, alterations in the brachioradialis reflex, and possible wrist extension weakness. Although the nerve root associated with the vertebral body passes above the pedicles such that the C6 root passes above the C6 pedicle, it is still the C6 root that is encroached on because the herniation affects the exiting root rather than the traversing root as seen in the lumbar spine. Klein JD, Garfin SR: Clinical evaluation of patients with suspected spine problems, in Frymoyer JW (ed): Adult Spine: Principles and Practice, ed 2. Philadephia, PA, Lippincott-Raven, 1997, pp 319-330.
Question 200
High Yield
A corset-type brace may help reduce symptoms during an episode of acute low back pain as the result of
Explanation
Although there is no significant alteration in motion with a corset, studies have shown a decrease in intradiskal pressure. Nachemson A, Morris JM: In vivo measurements of intradiscal pressure: Discometry, a method for determination of pressure in the low lumbar disc. J Bone Joint Surg Am 1964;46:1077-1092.
