HY 2026
00:00
Start Quiz
Question 1
High Yield
A construction worker sustained a comminuted calcaneus fracture 2 years ago. He now reports progressive hindfoot pain with the recent onset of anterior ankle pain. A lateral hindfoot radiograph is shown in Figure 31. Treatment should consist of

Explanation
The patient has subtalar arthrosis, a loss of heel height with anterior ankle impingement. The mechanics of the ankle are impaired, and dorsiflexion is painful and limited. The talar declination angle is measured by drawing a line through the longitudinal axis of the talus and the plane of support of the foot on a weight-bearing lateral radiograph. Anterior impingement is suggested with any value below 20°. By performing a distraction arthrodesis through the subtalar joint, the normal declination of the talus is reestablished, eliminating the anterior ankle impingement. Tibiotalocalaneal fusion would be inappropriate because the patient does not have arthritic symptoms in the ankle. Ankle arthroscopy or in situ arthrodesis would not reestablish appropriate ankle mechanics, and the osteophytes would be prone to redevelop. Lateral wall ostectomy may help with impingement at the level of the fibula or the lateral ankle but would provide no benefit to anterior ankle impingement. Carr JB, Hansen ST, Benirschke SK: Subtalar distraction bone block fusion for late complications of os calcis fractures. Foot Ankle 1988;9:81-86.
Question 2
High Yield
An 18-year-old man sustains an injury to the right brachial plexus after falling off his bicycle. Examination reveals no rhomboideus major or minor muscle function. This finding most likely indicates a preganglionic injury to which of the following nerve roots?
Explanation
The rhomboideus major and minor muscles are innervated by the dorsal scapular nerve, which is supplied entirely by the C5 nerve root. The dorsal scapular nerve arises just distal to the dorsal root ganglion of the C5 nerve root. A functioning rhomboid muscle indicates that an injury involving C5 nerve root fibers must be postganglionic or distal to the C5 dorsal root ganglion. Woodburne RT, Crelin ES, Kaplan FS, Dingle RV (eds): The Ciba Collection of Medical Illustrations. Summit, NJ, Ciba-Geigy Corporation, 1987, vol 8, pp 23-28.
Question 3
High Yield
Acute redislocation of the glenohumeral joint is a complication that occurs following a first-time dislocation. This is most often seen with
Explanation
Redislocation following acute dislocation occurs in approximately 3% of patients. This redislocation tends to occur in middle-aged and elderly patients. A higher incidence of redislocation occurs when there are accompanying fractures of the glenoid rim and the greater tuberosity. Robinson CM, Kelly M, Wakefield AE: Redislocation of the shoulder during the first six weeks after a primary anterior dislocation: Risk factors and results of treatment. J Bone Joint Surg Am 2002;84:1552-1559.
Question 4
High Yield
A 24-year-old dancer reports posterior ankle pain when in the "en pointe" position. Examination reveals posteromedial tenderness, no pain reproduction with passive forced planter flexion, and pain with motion of the hallux. What is the most likely diagnosis?
Explanation
Flexor hallucis longus tendinitis is a common cause of posterior ankle pain in dancers. It tends to be more posteromedial and is characterized by a clicking or catching sensation posteromedially with motion of the great toe. A painful os trigonum typically causes more posterolateral ankle pain and may occur after an ankle sprain or plantar flexion injury where there may be a fracture of the os trigonum. Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 249-261.
Question 5
High Yield
A 35-year-old male laborer with isolated posttraumatic degenerative arthritis of the right hip undergoes the procedure shown in Figure 8. What is the most appropriate position of the right lower extremity?

Explanation
The primary indication for hip arthrodesis is isolated unilateral hip disease in a young, active patient. Avoiding abductor damage and preserving proximal femoral anatomy are imperative to allow conversion to a future total hip arthroplasty. Optimal positioning is 30 degrees of flexion to allow swing-through. Neutral abduction and adduction and slight external rotation allow the most efficient gait while allowing sufficient support in stance. A small degree of adduction is acceptable for a successful hip arthrodesis. Callaghan JJ, Brand RA, Pedersen DR: Hip arthrodesis: A long term follow-up. J Bone Joint Surg Am 1985;67:1328-1335.
Question 6
High Yield
A 66-year-old woman was a restrained passenger in an automobile accident. She sustained a direct blow to her nondominant left hand as the airbag in her automobile deployed and she now reports pain, swelling, and difficulty moving her fingers. Radiographs are shown in Figures 58a and 58b. Appropriate definitive treatment should consist of


Explanation
While most isolated metacarpal fractures can be treated nonsurgically, multiple metacarpal fractures are inherently unstable due to the loss of support that an intact adjacent metacarpal provides; therefore, treatment should consist of surgical fixation of all three metacarpal fractures. Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC, et al (eds): Green's Operative Hand Surgery, ed 5. Philadelphia, PA, Elsevier, 2005, p 286.
Question 7
High Yield
The use of a screw between the clavicle and the coracoid process to maintain the clavicle and acromioclavicular (AC) joint in a reduced position is a treatment option for AC joint separations. Screw removal is generally recommended after soft-tissue healing. What effect does this rigid coracoclavicular fixation have on shoulder kinematics?
Explanation
This issue has been debated since Inman published his classic study on clavicular rotation in 1944. Subsequently, it has been shown by several authors that the clinical evaluation of patients with either coracoclavicular screws in place or with arthrodesis of the coracoclavicular reveals little to no loss of shoulder motion. This is most likely the result of synchronous motion of the scapula and clavicle in shoulder movements. Flatow EL: The biomechanics of the acromioclavicular, sternoclavicular, and scapulothoracic joints. Instr Course Lect 1993;42:237-245. Kenedy JC, Cameron H: Complete dislocation of the acromioclavicular joint. J Bone Joint Surg Br 1954;36:202-208. Rockwood CA Jr, Williams GR, Young CD: Disorders of the acromioclavicular joint, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1998, vol 1, pp 483-553.
Question 8
High Yield
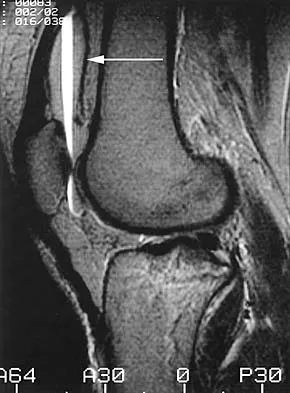
The cortical injury to the posterolateral distal fibula shown in Figure 25 indicates involvement of which of the following structures?

Explanation
The patient has a rim avulsion fracture that is the result of a forceful twisting injury as the superior peroneal retinaculum is avulsed from its fibular attachment along with a small rim of bone. Injuries to the anterior talofibular ligament or calcaneal fibular ligament would show cortical avulsions more anteriorly or distally at the fibular tip. Deltoid ligament injuries would reveal medial radiographic changes. In a true injury to the syndesmosis, if osseous structures do show avulsion, it would be more directly posterior or anterior on the distal fibula or would occur on the tibial surface. Murr S: Dislocation of the peroneal tendons with marginal fracture of the lateral malleolus. J Bone Joint Surg Br 1961;43:563-565.
Question 9
High Yield
Figures 15a through 15c show the radiographs of a 23-year-old football player who was injured when another player fell on his flexed and planted foot. He reports severe pain in the midfoot with a feeling of numbness on the dorsum of the foot, and he is unable to bear weight on the limb. Examination reveals mild swelling. Management should consist of



Explanation
Myerson and associates studied the outcomes of 19 patients with tarsometatarsal joint injuries during athletic activity. Injuries were classified as first- or second-degree sprains of the tarsometatarsal joint or a third-degree sprain with diastasis between the metatarsals or cuneiforms. Poor functional results were seen in those with a delay in diagnosis and with inadequate treatment. For patients with third-degree sprains, poor results were obtained with nonsurgical management. These patients required open reduction and internal fixation for optimal return to function. The anatomic reduction is critical to the outcome; therefore, open reduction is preferred. Baxter DE: The Foot and Ankle in Sport, ed 1. St Louis, MO, Mosby, 1995, pp 107-123. Curtis MJ, Myerson M, Szura B: Tarsometatarsal joint injuries in the athlete. Am J Sports Med 1993;21:497-502. Kuo RS, Tejwani NC, DiGiovanni CW, et al: Outcome after open reduction and internal fixation of Lisfranc joint injuries. J Bone Joint Surg Am 2000;82:1609-1618.
Question 10
High Yield
A 58-year-old woman with rheumatoid arthritis and a severe hindfoot valgus deformity now reports recurrent lateral ankle pain. Examination reveals pain over the fibula and sinus tarsi, with a valgus hindfoot that is passively correctable. Despite the use of an ankle-foot orthosis, this is the second time this problem has occurred. Radiographs and a clinical photograph are shown in Figures 28a through 28c. What is the next most appropriate step in treatment?



Explanation
Excessive hindfoot valgus can lead to abutment between the calcaneus and fibula. This valgus force can lead to a stress fracture of the distal fibula. Surgery may be required if an insufficiency fracture recurs despite orthotic management. Of the choices listed, a subtalar arthrodesis is most likely to achieve rebalancing of the foot at the level of the deformity. Stephens HM, Walling AK, Solmen JD, Tankson CJ: Subtalar repositional arthrodesis for adult acquired flatfoot. Clin Orthop 1999;365:69-73
Question 11
High Yield
A baseball pitcher has intractable posterior and superior shoulder pain. The arthroscopic view seen in Figure 25 shows no Bankart or Hill-Sachs lesion and a negative drive-through sign. There are no signs of ligamentous laxity, but active compression and anterior slide tests are positive. Treatment should consist of
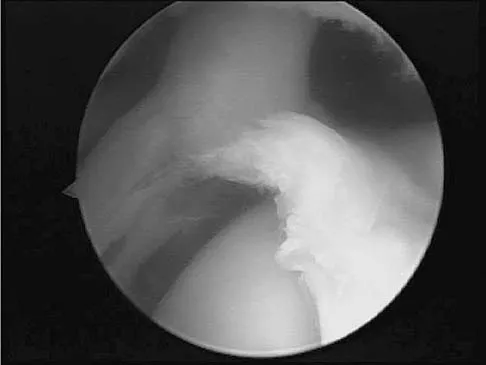
Explanation
According to Morgan and associates, a type II SLAP lesion can create or is associated with a superior instability pattern. They suggest that this can exist without a co-existing anteroinferior instability pattern. They reported that repair of the SLAP lesion alone resulted in satisfactory outcomes in 90% of patients and a return to throwing in more than 90% of pitchers. The arthroscopic findings in this patient do not support a diagnosis of anteroinferior laxity or instability; therefore, thermal capsular shift or capsular placation is not necessary. Morgan CD, Burkhart SS, Palmeri M, et al: Type II SLAP lesions: Three subtypes and their relationships to superior instability and rotator cuff tears. Arthroscopy 1998;14:553-565. Mileski RA, Snyder RJ: Superior labral lesions in the shoulder: Pathoanatomy and surgical management. J Am Acad Orthop Surg 1998;6:121-131.
Question 12
High Yield
A patient with Charcot-Marie-Tooth disease has a progressively rigid cavovarus foot deformity. The patient states that the pain is restricted to the forefoot, where rigid claw toe deformities have developed. Which of the following structures is primarily involved in creation of a claw toe deformity?

Explanation
Diseases such as Charcot-Marie-Tooth result in spasticity to the extrinsic flexor tendons. This results in hyperflexion of the proximal and distal interphalangeal joints of the involved toe, as well as hyperextension at the metatarsophalangeal joint. The tendon often becomes contracted with progressive equinus of the ankle. Correction of ankle equinus exaggerates the claw toe deformity. The interosseous tendon plays no role in the etiology of a claw toe but may become contracted in later stages of the disease. Laxity of the volar plate may precipitate a claw toe deformity in a nonspastic situation. In patients with a head injury, claw toe deformities are generally the result of overactivity of the extensor tendons. Keenan MA, Gorai AP, Smith CW, Garland DE: Intrinsic toe flexion deformity following correction of spastic equinovarus deformity in adults. Foot Ankle 1987;7:333-337. Pichney GA, Derner R, Lauf E: Digital "V" arthrodesis. J Foot Ankle Surg 1993;32:473-479.
Question 13
High Yield
Figures 5a and 5b show the radiographs of a 56-year-old man who was seen in the emergency department following a twisting injury to his left ankle. Examination in your office 3 days later reveals marked swelling and diffuse tenderness to palpation about the ankle and leg. What is the next most appropriate step in management?


Explanation
The radiographs show an isolated posterior malleolus fracture which, given the injury mechanism, is highly suspicious for a Maisonneuve injury. As with any suspected extremity injury, radiographs including the joints above and below the level of injury are acutely indicated. Although MRI may reveal a ligamentous injury to the ankle and CT may show asymmetry of the ankle mortise or syndesmosis, both studies are considerably more costly and are not indicated in the absence of a complete radiographic work-up. Technetium bone scan is nonspecific and would be of limited value in this instance, as would repeat radiographs of the ankle. Walling AK, Sanders RW: Ankle fractures, in Coughlin MJ, Mann RA, Saltzman CL (eds): Surgery of the Foot and Ankle, ed 8. Philadelphia, PA, Mosby-Elsevier, 2007, vol 2, pp 1973-2016.
Question 14
High Yield
A 45-year-old man who smokes reports the rapid onset of color changes and coolness in the fingers. Examination shows an abnormal Allen test. Plain radiographs of the hand and wrist are normal. Which of the following studies will best aid in diagnosis?

Explanation
The patient has symptoms typical of Raynaud's phenomenon secondary to underlying vascular disease. The next most appropriate step in the management of this patient should be to perform contrast angiography on the involved upper extremity to look for proximal or distal arterial lesions or insufficiencies. MRI and contrast CT are not as specific as angiography for the identification of vascular lesions of the upper extremity. Although patients with primary Raynaud's vasospastic disease can have normal angiographic findings, they typically are younger than age 40 years, are female, and have normal results on an Allen test. Green DP, Hotchkiss RN, Pederson WC (eds): Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, pp 2288-2290.
Question 15
High Yield
The scoring system for impending pathologic fractures devised by Mirels involves assessment of which of the following factors?

Explanation
The scoring system published by Mirels in 1989 is based on the following characteristics: the location of the lesion, the amount of pain the patient is experiencing, the type of lesion (either lucent, mixed, or blastic), and the lesion size. The tumor is scored from 1 to 3 in each category and a total score is obtained that correlates to fracture risk. Prophylactic fixation is advised for lesions with scores of higher than 8, and consideration for stabilization should be strongly considered for scores of 8. The Mirels scoring system can be useful as an adjunct to clinical decision making. Mirels H: Metastatic disease in long bones: A proposed scoring system for diagnosing impending pathologic fractures. 1989. Clin Orthop Relat Res 2003;415:S4-S13.
Question 16
High Yield
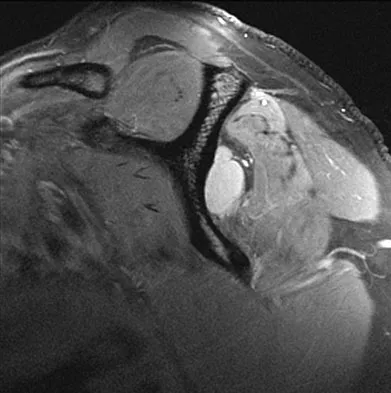
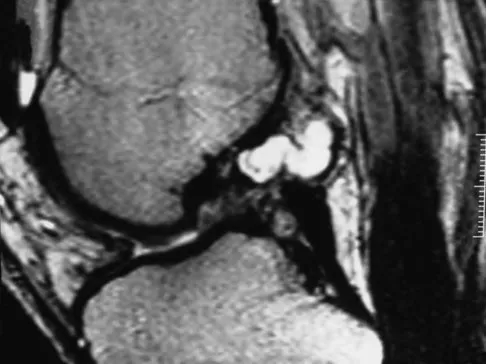
A 22-year-old volleyball player reports the insidious onset of superior and posterior shoulder pain. Radiographs are normal. An MRI scan is shown in Figure 25. What is the most specific physical examination finding?

Explanation
Overhead athletes are prone to a number of problems involving the shoulder. Pitchers and volleyball players are susceptible to posterior superior labral tears and internal impingement. These patients will have posterior superior shoulder pain, a positive relocation sign, and a positive active compression test. Occasionally, these posterior superior labral tears are associated with a spinoglenoid cyst as seen in the MRI scan. These cysts cause compression of the suprascapular nerve which manifests primarily as weakness of the infraspinatus, resulting in weakness of external rotation. Romeo AA, Rotenberg DD, Bach BR Jr: Suprascapular neuropathy. J Am Acad Orthop Surg 1999;7:358-367.
Question 17
High Yield
The peroneus tertius is a commonly used landmark for arthroscopic portal placement. What is the function of this tendon?

Explanation
The peroneus tertius, although absent in 10% of the population, originates on the distal third of the extensor surface of the fibula and inserts onto the base of the fifth metatarsal, possibly extending to the fascia over the fourth interosseous space. The muscle is located in the anterior compartment of the leg and is innervated by the deep peroneal nerve. The tendon produces dorsiflexion and eversion when walking and can be used as an insertion point during tendon transfers to assist dorsiflexion. This tendon is peculiar to humans and is a proximally migrated deep extensor of the fifth toe. Joshi SD, Joshi SS, Athavale SA: Morphology of the peroneus tertius muscle. Clin Anat 2006;19:611-614. Williams PL, Bannister LH, Berry MM, et al (eds): Gray's Anatomy, ed 38. London, Churchill Livingston, 1995, p 883.
Question 18
High Yield
Figures 36a and 36b show the radiographs of a 48-year-old woman who smokes cigarettes and sustained a segmental femoral shaft fracture in a motor vehicle accident 9 months ago. Initial management consisted of stabilization with a reamed statically locked intramedullary nail. She now reports lower leg pain that increases with activity. In addition to advising the patient to quit smoking, management should include


Explanation
The patient has an oligotrophic nonunion of the distal femoral fracture. Although the proximal fracture appears incompletely united, it was stable at exchange nailing. The treatment of choice is exchange reamed nailing to at least 2 mm above the nail in place. Bone grafting is debatable. Recent studies have shown a 70% to 75% success rate with exchange nailing only, so in nonhypertrophic nonunions, bone grafting can be considered. Nonsurgical management consisting of observation or external stimulation runs the risk of implant failure. Plate fixation is acceptable but is considered a second choice because of the need to consider stabilization of the proximal fracture until union is achieved. Also, plate fixation definitely requires bone grafting. Webb LX, Winquist RA, Hansen ST: Intramedullary nailing and reaming for delayed union or nonunion of the femoral shaft: A report of 105 consecutive cases. Clin Orthop 1986;212:133-141. Weresh MJ, Hakanson R, Stover MD, et al: Failure of exchange reamed intramedullary nailing for ununited femoral shaft fractures. J Orthop Trauma 2000;14:335-338.
Question 19
High Yield
A 20-year-old man sustains the injury shown in Figures 1a and 1b in a motorcycle accident. In addition to a prompt closed reduction, his outcome might be optimized by


Explanation
Lateral subtalar dislocations, which are less common than medial subtalar dislocations, are high-energy injuries that are frequently associated with small osteochondral fractures. It is generally recommended that large fragments be internally fixed, and small fragments entrapped within the joint be excised. Although arthrosis frequently occurs after this injury and is the most common long-term complication, primary subtalar arthrodesis is not indicated. A talar neck fracture is not evident on the radiographs, and lateral subtalar dislocation usually does not lead to instability.
Question 20
High Yield
What is the most important factor in determining recovery after surgical repair of a complete laceration of a nerve at the wrist?
Explanation
All other factors being equal, a patient's age is the most important factor in determining outcome after peripheral nerve injury. Repair of a nerve laceration within the first 2 weeks is generally considered appropriate. Fascicular repair may be of benefit in larger proximal nerves to reapproximate appropriate nerve bundles; distally perineural or epineural repair is sufficient. Use of a fibrin tissue sealant for nerve repair does not result in improved outcomes over suture repair. Nerve conduits have shown promise in digital nerves but do not have proven benefit in larger caliber nerves. Sunderland S: Nerve Injuries and Their Repair: A Critical Appraisal. New York, NY, Churchill Livingstone, 1991. Wilgis ES, Brushart TM: Nerve repair and grafting, in Green DP, Hotchkiss RN (eds): Operative Hand Surgery, ed 3. New York, NY, Churchill Livingstone, 1993, p 1325. Narakas A: The use of fibrin glue in repair of peripheral nerves. Orthop Clin North Am 1988;19:187-199.
Question 21
High Yield
A 38-year-old man sustains a complete avulsion with retraction of the ischial attachment of the hamstring muscles in a fall while water skiing. He indicates that he is an aggressive athlete who participates regularly in multiple running and cutting-type sports, and he strongly desires to continue his athletic competition. Management should consist of
Explanation
Several studies have identified a complete proximal avulsion of the hamstring muscles as an injury that leads to significant long-term disability, with a high percentage of athletes who must permanently restrict their activities following nonsurgical management. Early surgical repair and prolonged rehabilitation have yielded consistently better results than nonsurgical management. Orava S, Kujala UM: Rupture of the ischial origin of the hamstring muscles. Am J Sports Med 1995;23:702-705.
Question 22
High Yield
What neurovascular structure is most at risk when performing an inside-out repair of the posterior horn of the medial meniscus?
Explanation
The saphenous nerve is located on the posterior medial aspect of the knee and must be protected when performing an inside-out repair of the medial meniscus. The peroneal nerve is most at risk with lateral meniscal repairs. The other structures usually are not at risk with meniscal repair. Cannon WD Jr, Morgan CD: Meniscal repair: Arthroscopic repair techniques. Instr Course Lect 1994;43:77-96.
Question 23
High Yield
Second impact syndrome (SIS) after head injury is characterized by which of the following?
Explanation
SIS is a devastating but preventable complication of head injury. It occurs when return to activities is allowed prior to complete resolution of the symptoms of the first head injury. A second, sometimes trivial, head injury can lead to a devastating series of events that can result in sudden death. The symptoms tend to progress rapidly and often involve the brain stem. The prognosis is poor. Cantu RC: Second-impact syndrome. Clin Sports Med 1998;17:37-44. Saunders RL, Harbaugh RE: Second impact in catastrophic contact-sports head trauma. JAMA 1984;252:538-539.
Question 24
High Yield
During a posterior approach to the right Achilles tendon, the surgeon encounters a nerve running with the small saphenous vein as shown in Figure 22. This nerve innervates what part of the foot?
Explanation
The sural nerve runs with the small saphenous vein on the posterior leg just lateral to the Achilles tendon. It is formed by contributions from both the tibial and common peroneal nerves and provides sensation on the dorso-lateral aspect of the foot. Aktan Ikiz ZA, Ucerler H, Bilge O: The anatomic features of the sural nerve with an emphasis on its clinical importance. Foot Ankle Int 2005;26:560-567.
Question 25
High Yield
Which of the following structures is most vulnerable during a medial sesamoidectomy of the hallux?
Explanation
The plantar-medial cutaneous nerve is at risk with the surgical approach to the medial sesamoid. It is found directly underlying an incision made at the junction of the glabrous skin of the hallux and must be identified before the approach can proceed. Transection will result in a painful neuroma that impinges on the plantar-medial surface of the toe and cause problems with shoe wear. The only other structure that lies near the surgical field is the abductor hallucis tendon which lies dorsal to the incision.
Question 26
High Yield
The spring ligament of the foot connects what two bones?
Explanation
The spring ligament is also known as the calcaneonavicular ligament and connects the calcaneus to the navicular. This ligament supports the talar head and is an important anatomic supporting structure of the medial longitudinal arch of the foot. Choi K, Lee S, Otis JC, et al: Anatomical reconstruction of the spring ligament using peroneus longus tendon graft. Foot Ankle Int 2003;24:430-436.
Question 27
High Yield
Figures 18a and 18b show the radiographs of a patient who has pain with walking. On careful questioning, it is determined that the discomfort occurs at push-off, or when the patient attempts to climb stairs. What nonsurgical option is most likely to ameliorate the symptoms?


Explanation
The patient has a malunion of an attempted open reduction of a Lisfranc dislocation. The pain occurs during the terminal stance phase of gait as load is being transferred from the hindfoot to the forefoot. The bending moment can be best neutralized with shoe modification with a cushioned heel and rocker sole, which best unloads the tarsal-metatarsal junction. Bono CM, Berberian WS: Orthotic devices: Degenerative disorders of the foot and ankle. Foot Ankle Clin 2001;6:329-340.
Question 28
High Yield
Figures 10a and 10b show the clinical photograph and MRI scan of a plantar foot lesion. If excisional biopsy is performed, what is the most likely complication?

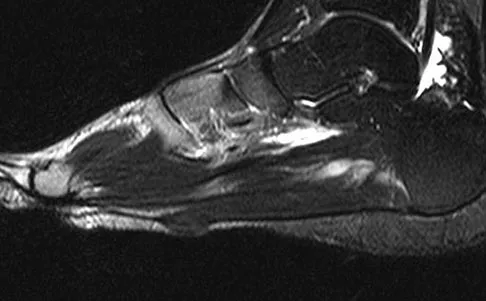
Explanation
The MRI scan shows plantar fibromatosis. The treatment is usually nonsurgical. If surgery is indicated, wide local excision with excision of the entire plantar fascia is usually indicated. The main problem with simple excision of the lesion is the high chance of recurrence. The other listed complications are those that are a result of the wide local excision. Aluisio FV, Mair SD, Hall RL: Plantar fibromatosis: Treatment of primary and recurrent lesions and factors associated with recurrence. Foot Ankle Int 1996;17:672-678.
Question 29
High Yield
Figure 2 shows the radiograph of a 72-year-old woman who reports pain after a fall. History includes several years of increasing thigh pain and limb shortening. Management consisting of an extensive work-up for infection reveals normal laboratory studies, a positive bone scan, and a negative hip aspiration. What is the most likely etiology of this complication?

Explanation
The patient has a midstem periprosthetic fracture, which commonly results in loosening of the prosthesis. Patients who have a large amount of bone loss may require an allograft with the surgical reconstruction. Although the patient reported a fall, her history is also consistent with preexisting loosening of the prosthesis. Chronic infection has been shown in up to 16% of these fractures; however, the patient's work-up revealed no infection. Garbuz DS, Masri BA, Duncan CP: Periprosthetic fractures of the femur: Principles of prevention and management, in Cannon WD Jr (ed): Instructional Course Lectures 47. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 237-242. Bethea JS III, DeAndrade JR, Fleming LL, Lindenbaum SD, Welch RB: Proximal femoral fractures following total hip arthroplasty. Clin Orthop 1982;170:95-106.
Question 30
High Yield
Which of the following changes of calcium metabolism accompany the loss of bone during menopause?
Explanation
There is a negative change of calcium balance with a decrease in intestinal absorption and an increase in urinary calcium loss. The reduction of intestinal absorption is accompanied by reduced circulating concentrations of total, but not free 1,25-dihydroxyvitamin D. However, estrogen may also directly regulate intestinal calcium resorption independent of vitamin D. Tubular resorption of calcium is higher in the presence of estrogen. Studies of the levels of PTH in the presence of estrogen are controversial. Oh KW, Rhee EJ, Lee WY, et al: The relationship between circulating osteoprotegerin levels and bone mineral metabolism in healthy women. Clin Endocrinol (Oxf) 2004;61:244-249.
Question 31
High Yield
A 6-year-old Little League pitcher has had pain in the right elbow for the past 2 weeks. Examination reveals mild lateral elbow joint tenderness with full range of motion and no effusion or collateral laxity. A radiograph is shown in Figure 38. Initial management should consist of

Explanation
The radiograph shows osteochondritis dissecans (OCD) of the capitellum, one manifestation of "pitcher's elbow." The lesion is nondisplaced, and healing is possible if the inciting throwing activities are curtailed. Long arm cast treatment may be reasonable for the noncompliant patient but should not exceed 6 weeks duration. Surgical treatment is indicated for loose bodies or cartilage flaps. Elbow OCD lesions are now being seen in younger children as more participate in organized sports, especially baseball and gymnastics. Bauer M, Jonsson K, Josefsson PO, et al: Osteochondritis dissecans of the elbow: A long-term follow-up study. Clin Orthop 1992;284:156-160. Takahara M, Ogino T, Sasaki I, et al: Long term outcome of osteochondritis dissecans of the humeral capitellum. Clin Orthop 1999;363:108-115.
Question 32
High Yield
What percent of patients initially diagnosed with classic, high-grade osteosarcoma of the extremity have visible evidence of pulmonary metastasis on CT of the chest?
Explanation
CT studies show that approximately 10% to 20% of patients with high-grade osteosarcoma have pulmonary metastases at diagnosis. Although not visible on current staging studies, it is believed that up to 80% of patients have micrometastatic disease that requires systemic chemotherapy. Because it is not possible to identify those patients who do not have disseminated micrometastatic disease, most patients are treated presumptively with chemotherapy. Kaste SC, Pratt CB, Cain AM, et al: Metastases detected at the time of diagnosis of primary pediatric extremity osteosarcoma at diagnosis: Imaging features. Cancer 1999;86:1602-1608.
Question 33
High Yield
A 17-year-old high school long distance runner is seeking advice before running a marathon for the first time. What advice should be given regarding his fluid, carbohydrate, and electrolyte intake around the time of the race?
Explanation
The goal of fluid replenishment should be to replace the sweat that has been lost. Sweat is mostly water, with a small concentration of salts and other electrolytes. Absorption is enhanced by solutions of low osmolality. Scientific research has also shown that adding carbohydrates to the drink improves athletic performance. Carbohydrates such as glucose and maltodextrins (glucose polymers) stimulate fluid absorption by the intestines. Fructose slows intestinal absorption of fluids. Drinks that are high in fructose, such as orange juice, can lead to gastrointestinal distress and osmotic diarrhea. Kirkendall D: Fluids and electrolytes, in The U.S. Soccer Sports Medicine Book. Baltimore, MD, Williams and Wilkins, 1996.
Question 34
High Yield
Which of the following best describes the mechanical response of the inferior glenohumeral ligament to repetitive subfailure strains?
Explanation
Repetitive subfailure strains have been shown to affect the mechanical behavior of the inferior glenohumeral ligament, producing dramatic declines in the peak load response and length increases that are largely unrecoverable. In another study, anteroinferior subluxation was found to result in nonrecoverable strain in the anteroinferior capsule, varying from 3% to 7% through a range of joint subluxation. Pollock RG, Wang VM, Bucchieri JS, et al: Effects of repetitive subfailure strains on the mechanical behavior of the inferior glenohumeral ligament. J Shoulder Elbow Surg 2000;9:427-435.
Question 35
High Yield
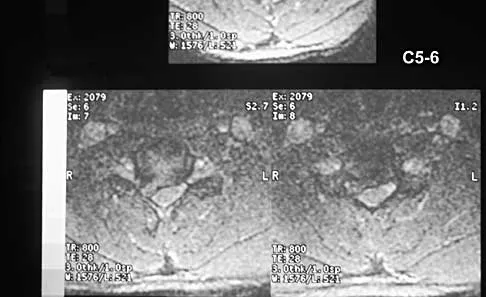
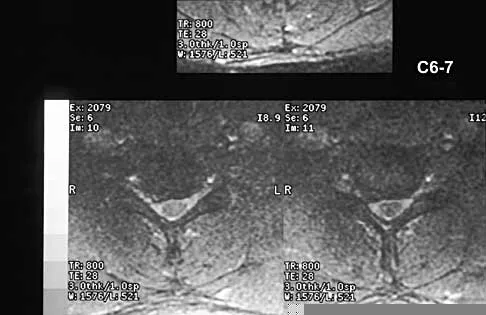
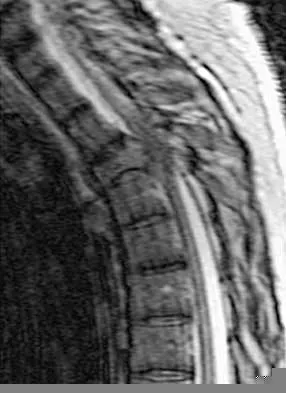
A 40-year-old carpenter has a 3-month history of right arm pain and neck pain that now leaves him unable to work. Examination reveals a positive Spurling test, weakness of the biceps, and a mildly positive Hoffman's sign on the right side. Electromyography and nerve conduction velocity studies show a right C6 deficit. Figures 27a through 27c show MRI scans that reveal two-level spondylotic disease at C5-6 and C6-7, a large herniated nucleus pulposus at C5-6, and a prominent ridge and hard disk at C6-7. Nonsurgical management fails to provide relief, so the patient elects surgical intervention. Which of the following surgical options would give the best long-term results?

Explanation
The patient has a single-level deficit by clinical examination but an adjacent level that may be pathologic. Hilibrand and associates, in a review of 374 patients with myeloradiculopathy treated with single-level or multilevel anterior cervical diskectomy and fusion, showed that 25% of patients had an occurrence of new radiculopathy or myelopathy at an adjacent level within 10 years after surgery. Reoperation rates were highest in those patients where the adjacent nonfused segment was C5-6 or C6-7. Those patients who had multilevel fusions had a lower incidence of adjacent segment disease. The authors recommended incorporating an adjacent level in the initial procedure in patients with myelopathy or radiculopathy when significant disease was noted. Posterior keyhole foraminotomy is an excellent procedure for single-level radiculopathy but is not effective in relieving myelopathy. Anterior cervical diskectomy without fusion has an increased incidence of hypermobility and neck pain on long-term follow-up. In a later review, these authors reported improved fusion rates and better clinical outcomes with the use of strut fusions instead of multilevel interbody grafts. Hilibrand AS, Carlson GD, Palumbo MA, Jones PK, Bohlman HH: Radiculopathy and myelopathy at segments adjacent to the site of a previous anterior cervical arthrodesis. J Bone Joint Surg Am 1999;81:519-528. Henderson CM, Hennessy RG, Shuey HM Jr, Shackelford EG: Posterior-lateral foraminotomy as an exclusive operative technique for cervical radiculopathy: A review of 846 consecutively operated cases. Neurosurgery 1983;13:504-512.
Question 36
High Yield
Figure 37 shows the radiograph of a 21-year-old collegiate basketball player who has had mild midfoot aching for the past 4 months. What is the best course of action?

Explanation
A stress fracture of the navicular is considered a high-risk injury because of the incidence of nonunion. If identified early, cast immobilization with no weight bearing is appropriate. However, this patient is a high-caliber athlete who has had symptoms for 4 months. Therefore, surgery is recommended to expedite recovery and optimize the chance of healing. Meyer SA, Saltaman CL, Albright JP: Stress fractures of the foot and ankle. Clin Sports Med 1993;12:395-413. Kahn JM, Fuller PJ, Burkner PD, et al: Outcome of conservative and surgical management of navicular stress fractures in athletes: Eighty-six cases proven with computerized tomography. Am J Sports Med 1992;20:657-666.
Question 37
High Yield
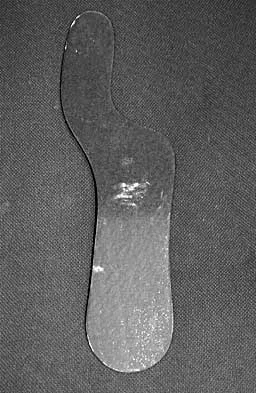
The orthosis shown in Figure 47 is commonly used for
Explanation
The orthosis shown is a carbon reinforced Morton's extension, and it is commonly used for hallux rigidus. It decreases motion of the first metatarsophalangeal joint and subsequently decreases pain.
Question 38
High Yield
A 68-year-old woman who underwent a right total hip arthroplasty 1 year ago has dislocated her hip five times since surgery. Radiographs show a retroverted acetabular component. What is the best treatment for this patient?
Explanation
The most common cause of recurrent dislocation following total hip arthroplasty continues to be component malposition. Component malposition should be addressed prior to any other treatment options, such as increasing soft-tissue tension with increased femoral offset or greater trochanteric advancement. A larger femoral head size may help, but correcting the component malposition should give more predictable results. A retroverted acetabular component should be revised to 15 degrees to 20 degrees of anteversion, matching the patient's anatomy with an abduction angle close to 45 degrees. Daly PJ, Morrey BF: Operative correction of an unstable total hip arthroplasty. J Bone Joint Surg Am 1992;74:1334-1343. Jolles BM, Zangger P, Leyvraz PF: Factors predisposing to dislocation after primary total hip arthroplasty: A multivariate analysis. J Arthroplasty 2002;17-282-288.
Question 39
High Yield
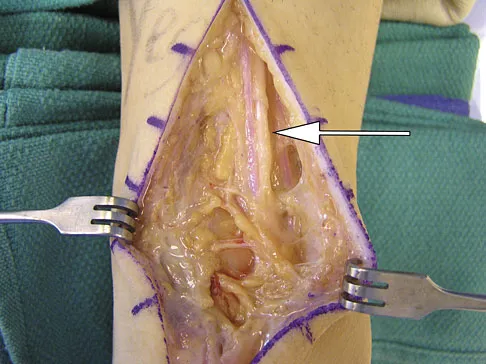
A 35-year-old man sustained a 1-inch stab incision in his proximal forearm while trying to use a screwdriver 2 weeks ago. The laceration was routinely closed, and no problems about the incision site were noted. He now reports that he has been unable to straighten his fingers or thumb completely since the injury. Clinical photographs shown in Figures 30a and 30b show the man passively flexing the wrist. What is the most appropriate management?


Explanation
The clinical photographs indicate that the tenodesis effect of digit flexion with passive wrist extension and digit extension with passive wrist flexion is intact, indicating no discontinuity of the extensor or flexor tendons. The most likely injury is a laceration of the posterior interosseous nerve.
Question 40
High Yield
Which of the following forms of nonsurgical management is considered best for acute low back pain without radiculopathy?
Explanation
Temporary bed rest (less than 4 days) with gradual resumption of activities can be efficacious. Epidural steroid injections may be indicated for acute low back pain with radiculopathy. Acupuncture, facet joint injections, or ligamentous (sclerosant) injections are not indicated. Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, Appendix A15.
Question 41
High Yield
What complication is most likely to develop after right total hip arthroplasty in the patient shown in Figure 5?

Explanation
The patient has hypertrophic arthritis, which is a strong risk factor for heterotopic bone formation. The remaining complications are possible but do not have the same significant risks. Goel A, Sharp DJ: Heterotopic bone formation after hip replacement: The influence of the type of osteoarthritis. J Bone Joint Surg Br 1991;73:255-257.
Question 42
High Yield
A 55-year-old man sustained an elbow dislocation in a fall. Postreduction radiographs are shown in Figures 40a and 40b. What is the best course of management?


Explanation
The radiographs show an elbow dislocation associated with a comminuted radial head fracture. In the setting of comminution and instability, factures of the radial head are best managed with an arthroplasty rather than open reduction and internal fixation. Resection of the radial head will worsen the instability and is not recommended. Silastic radial head replacements are contraindicated. Hildebrand KA, Patterson SD, King GJ: Acute elbow dislocations: Simple and complex. Orthop Clin North Am 1999;30:63-79.
Question 43
High Yield
Which of the following nerves is most commonly injured during ankle arthroscopy?
Explanation
The superficial peroneal nerve, which is adjacent to the location of the lateral arthroscopic portal is most commonly injured. Ferkel RD, Heath DD, Guhl JF: Neurological complications of ankle arthroscopy. Arthroscopy 1996;12:200-208.
Question 44
High Yield
A patient with a below-the-knee amputation is being evaluated for a new prosthesis. He wants to improve his ability to walk on uneven surfaces. What modification to the prosthesis can be made to accommodate this request?
Explanation
Changing from a solid keel to a keel with a sagittal split allows an amputee to navigate uneven terrain more easily. Changing the length of the keel affects the responsiveness of the prosthesis but does not address the surface conditions for ambulation. The SACH is not used as frequently anymore, because overload problems to the nonamputated foot have been observed. Koval K (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 31-45.
Question 45
High Yield
A 27-year-old man now reports dorsiflexion and inversion weakness after an automobile collision 6 months ago in which compartment syndrome developed isolated to the anterior and deep posterior compartments. Examination reveals the development of a progressive cavovarus deformity, but the ankle and hindfoot remain flexible. In addition to Achilles tendon lengthening, which of the following procedures is most likely to improve the motor balance of his foot and ankle?

Explanation
Compartment syndrome of the anterior and deep posterior compartments results in anterior tibialis and posterior tibialis tendon weakness, respectively. Furthermore, the long flexors to the hallux and lesser toes will be weak as well. The intact peroneus longus overpowers the weak anterior tibialis tendon, resulting in plantar flexion of the first metatarsal, cavus, and hindfoot varus. Therefore, transferring the peroneus longus to the dorsolateral midfoot reduces the first metatarsal plantar flexion torque, and possibly augments ankle dorsiflexion torque. Hansen ST: Functional Reconstruction of the Foot and Ankle. Philadelphia, PA, Lippincott, Williams & Wilkins, 2000, pp 433-435.
Question 46
High Yield
A 66-year-old man has a high-grade angiosarcoma of the right tibia. A radiograph is shown in Figure 43. Treatment should consist of
Explanation
Angiosarcoma is a locally aggressive sarcoma. The radiograph shows extensive multiple discontinuous lesions throughout the entire tibia. The extent of bone involvement precludes resection; therefore, the treatment of choice is amputation, either above the knee or through the knee. Radiation therapy is not needed after amputation, and chemotherapy remains investigational for soft-tissue sarcoma.
Question 47
High Yield
A 27-year-old woman has a bilateral C5-C6 facet dislocation and quadriparesis after being involved in a motor vehicle accident. Initial management consisted of reduction with traction, but she remains a Frankel A quadriplegic. To facilitate rehabilitation, surgical stabilization and fusion is planned. From a biomechanical point of view, which of the following techniques is the LEAST stable method of fixation?
Explanation
In two different biomechanical studies performed in both bovine and human cadaveric spines, all posterior techniques of stabilization were found to be superior to anterior plating in flexion-distraction injuries of the cervical spine. These injuries usually have an intact anterior longitudinal ligament that allows posterior fixation to function as a tension band. Anterior plating with grafting destroys this last remaining stabilizing structure and does not allow for a tension band effect because all of the posterior stabilizing structures have been destroyed with the injury. In clinical practice, however, anterior plating can be effective in the treatment of this injury with appropriate postoperative orthotic management. Sutterlin CE III, McAfee PC, Warden KE, et al: A biomechanical evaluation of cervical spine stabilization methods in a bovine model: Static and cyclical loading. Spine 1988;13:795-802.
Question 48
High Yield
If a surgeon inadvertently burrs through the midlateral wall of C5 during a anterior corpectomy, what structure is at greatest risk for injury?
Explanation
The vertebral artery is contained within the vertebral foramen and thus tethered alongside the vertebral body, making it vulnerable to injury if a drill penetrates the lateral wall. The C5 root passes over the C5 pedicle and is not in the vicinity. The C6 root passes under the C5 pedicle but is posterior to the vertebral artery and is only vulnerable at the very posterior-inferior corner. The carotid artery and the vagus nerve are both within the carotid sheath and well anterior. Pfeifer BA, Freidberg SR, Jewell ER: Repair of injured vertebral artery in anterior cervical procedures. Spine 1994;19:1471-1474.
Question 49
High Yield
A 42-year-old man has had left lower extremity pain in an L5 radicular pattern for the past 6 weeks. He denies significant axial low back pain. History reveals that he underwent an L4-5 diskectomy with successful relief of similar pain 5 years ago. Which of the following imaging studies would offer the greatest amount of information?
Explanation
MRI with gadolinium will best identify recurrent herniated nucleus pulposus or other root compression and distinguish scar from recurrent disk. CT is unable to distinguish scar from recurrent disk density, and the addition of myelogram dye can reveal compromise of the thecal sac but cannot distinguish the scar from recurrent disk as the source of compression. Although lateral flexion-extension radiographs may be important to rule out any instability, much of that information can be inferred from the associated disk and adjacent bony changes on MRI. Bone scan techniques may identify subtle stress fractures resulting from previous aggressive facet resection, but low back pain also would be expected. Mirowitz SA, Shady KL: Gadopentetate dimeglumine-enhanced MR imaging of the postoperative lumbar spine: Comparison of fat-suppressed and conventional T1-weighted images. Am J Roentgenol 1992;159:385-389.
Question 50
High Yield
A 3-year-old child has refused to walk for the past 2 days. Examination in the emergency department reveals a temperature of 102.2 degrees F (39 degrees C) and limited range of motion of the left hip. An AP pelvic radiograph is normal. Laboratory studies show a WBC count of 9,000/mm3, an erythrocyte sedimentation rate (ESR) of 65 mm/h, and a C-reactive protein level of 10.5 mg/L (normal < 0.4). What is the next most appropriate step in management?
Explanation
Examination reveals an irritable hip, creating a differential diagnosis of transient synovitis versus pyogenic hip arthritis. Kocher and associates described four criteria to help predict the presence of infection: inability to bear weight, fever, ESR of more than 40 mm/h, and a peripheral WBC count of more than 12,000/mm3. This patient meets three of the four criteria, with a positive predictive value of 73% to 93% for joint infection. Therefore, aspiration of the hip is warranted, with a high likelihood that emergent hip arthrotomy will be indicated. Ideally, intravenous antibiotics should be administered after culture material has been obtained from needle aspiration of the hip. An urgent bone scan is better indicated as a screening test for sacroiliitis or diskitis. If the arthrocentesis proves negative, CT or MRI of the pelvis may be indicated to rule out a pelvic or psoas abscess. Del Beccaro MA, Champoux AN, Bockers T, et al: Septic arthritis versus transient synovitis of the hip: The value of screening laboratory tests. Ann Emerg Med 1992;21:1418-1422. Kocher MS, Mandiga R, Zurakowski D, et al: Validation of a clinical prediction rule for the differentiation between septic arthritis and transient synovitis of the hip in children. J Bone Joint Surg Am 2004;86:1629-1635.
Question 51
High Yield
A 60-year-old woman with a history of breast cancer has progressive paraparesis. The MRI scan is shown in Figure 28. What form of management is most likely to restore or maintain ambulation?
Explanation
Surgical decompression and stabilization have been shown to be the most effective means of improving neurologic function. Decompression is most reliably done from the side of the compression, which is anterior in this patient. Harrington KD: Metastatic tumors of the spine: Diagnosis and treatment. J Am Acad Orthop Surg 1993;1:76-86.
Question 52
High Yield
A 14-year-old patient with an L3 myelomeningocele underwent anterior and posterior spinal fusion for a curve of 50 degrees. Follow-up examination 1 week after the procedure now reveals persistent drainage from the posterior wound. Results of laboratory cultures show Streptococcus viridans, Staphylococcus aureus, and Enterococcus. In addition to IV antibiotics, surgical irrigation, and debridement, management should include
Explanation
The rate of wound infections has dramatically decreased with the routine use of prophylactic antibiotics. Factors known to increase the risk of infection include instrumentation, prolonged surgical time, excessive blood loss, poor perioperative nutritional status, a history of surgery, and a history of infection. The use of allograft does not result in an increased rate of infection. Adequate treatment requires early diagnosis and intervention. Temperature elevation and persistent wound drainage are highly suspicious for infection. An erythrocyte sedimentation rate and a WBC are not useful in diagnosis unless serial examinations show rising levels. Patients should be taken to the operating room where the entire wound can be reopened, irrigated, and debrided. Bone graft can be washed and replaced. Hardware should not be removed. The wound should be closed over suction drains. IV antibiotics should be given for a period of at least 10 days, followed by 6 weeks orally. Leaving the wound open to granulate with dressing changes results in prolonged hospitalization, inadequate treatment of the infection, and a poor cosmetic result. Lonstein JE: Complications of treatment, in Bradford DS, Lonstein JE, Moe JH, et al (eds): Moe's Textbook of Scoliosis and Other Spinal Deformities, ed 2. Philadelphia, Pa, WB Saunders, 1987, p 476.
Question 53
High Yield
Figures 31a and 31b show the T1- and T2-weighted MRI scans of a patient's knee joint. What is the most likely diagnosis?

Explanation
The scans show a lipohemarthrosis. There is the characteristic layering of a superior zone containing fat (high signal intensity), a central zone containing serum (low signal intensity), and an inferior zone that contains red blood cells (low signal intensity). The most common cause of a lipohemarthrosis is an intra-articular fracture with leakage of marrow fat into the joint. Resnick D, Kang HS: Synovial joints, in Resnick D, Kang HS (eds): Internal Derangements of Joints: Emphasis on MR Imaging. Philadelphia, PA, WB Saunders, 1997, pp 49-53.
Question 54
High Yield
A previously healthy 65-year-old woman has a closed fracture of the right clavicle after falling down the basement stairs. Examination reveals good capillary refill in the digits of her right hand. Radial and ulnar pulses are 1+ at the right wrist compared with 2+ on the opposite side. In the arteriogram shown in Figure 36, the arrow is pointing at which of the following arteries?
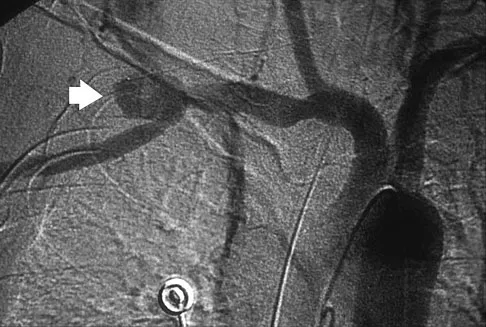
Explanation
The axillary artery commences at the first rib as a direct continuation of the subclavian artery and becomes the brachial artery at the lower border of the teres major. The arteriogram reveals a nonfilling defect in the third portion of the artery just distal to the subscapular artery. The complex arterial collateral circulation in this region often permits distal perfusion of the extremity despite injury.
Question 55
High Yield
A 48-year-old man has had pain and swelling of the hallux metatarsophalangeal joint for the past 9 months. A rocker bottom stiff-soled shoe has failed to provide relief; however, two cortisone injections have temporarily alleviated his symptoms. The radiographs shown in Figures 20a and 20b reveal diffuse arthritis of the entire hallux metatarsophalangeal joint. What is the most definitive surgical treatment?


Explanation
Because the radiographs demonstrate severe arthritis, hallux metatarsophalangeal arthrodesis is the treatment of choice. Cheilectomy alone will not relieve pain because the entire joint is degenerative. Joint replacement has not been shown to be a long-term solution. Keller resection arthroplasty is not indicated in younger active patients. Hallux valgus correction will not address arthritis of the joint and could stiffen the joint further. Smith RW, Joanis TL, Maxwell PD: Great toe metatarsophalangeal joint arthrodesis: A user-friendly technique. Foot Ankle 1992;13:367-377.
Question 56
High Yield
A 22-year-old college football player reports shortness of breath and dyspnea after a tackle. Examination reveals tachypnea, tachycardia, the trachea is shifted to the right, and there are decreased breath sounds on the left lung fields. The first line of treatment on the field should be
Explanation
The patient has a tension pneumothorax. This is a life-threatening emergency where air is trapped between the pleura and the lung, which prevents expansion of the lung. This causes hypoxia and cardiopulmonary compromise. The first line of treatment is to place a needle into the second intercostal space in the midclavicular line. The athlete should then be transported to the emergency department for chest tube placement. The athlete cannot return to play, and resuscitation is not necessary because he has not gone into cardiopulmonary arrest. Amaral JF: Thoracoabdominal injuries in the athlete. Clin Sports Med 1997;16:739-753.
Question 57
High Yield
Which of the following clinical scenarios represents an appropriate indication for convex hemiepiphysiodesis/hemiarthrodesis in the treatment of a child with a congenital spinal deformity?
Explanation
Convex hemiarthrodesis and hemiepiphysiodesis are procedures designed to gradually reduce curve magnitude in congenital scoliosis because of hemivertebrae. They are used to surgically create an anterior and posterior bar to arrest growth on the convexity of the existing deformity. Success of the technique is predicated on continued growth on the concave side of the deformity. Prerequisites for this procedure include curves of limited length (less than or equal to five vertebrae), curves of reasonable magnitude (less than 70 degrees), absence of kyphosis, concave growth potential, and appropriate age (younger than age 5 years).
Question 58
High Yield
Which of the following cardiac conditions is considered an absolute contraindication to vigorous exercise?

Explanation
Hypertrophic cardiomyopathy (HCM) accounts for up to 50% of cases of sudden death in young athletes. HCM phenotype becomes evident by age 13 to 14 years. Those at higher risk include individuals with cardiac symptoms, a family history of inherited cardiac disease, and those with a family history of premature sudden death. Echocardiography is useful for detecting structural heart disease, including the cardiomyopathies and valvular abnormalities. Trained adolescent athletes demonstrated greater absolute left ventricular wall thickness (LVWT) compared to controls. HCM should be considered in any trained adolescent male athlete with a LVWT of more than 12 mm (female of more than 11 mm) and a nondilated ventricle. Adolescent and adult athletes differ with respect to the range of LVWT measurements, as a manifestation of left ventricular hypertrophy (LVH). Differentiating LVH ("athlete's heart") from HCM involves looking at additional echocardiographic features. Sharma and associates reported that adolescents with HCM had a small or normal-sized left ventricle (less than 48 mm) chamber size, while those with LVH had a chamber size at the upper limits of normal (52 mm to 60 mm). Sharma S, Maron BJ, Whyte G, et al: Physiologic limits of left ventricular hypertrophy in elite junior athletes: Relevance to differential diagnosis of athlete's heart and hypertrophic cardiomyopathy. J Am College Cardiol 2002;40:1431-1436. Maron BJ, Spirito P, Wesley Y, et al: Development and progression of left ventricular hypertrophy in children with hypertrophic cardiomyopathy. N Engl J Med 1986;315:610-614.
Question 59
High Yield
Figures 61a and 61b show the CT and MRI scans of a 40-year-old man who has hip pain. He undergoes total hip arthroplasty and curettage and cementation of the lesion as shown in Figure 61c. Histopathologic photomicrographs of the curettage specimen are shown in Figures 61d and 61e. What is the best course of treatment?
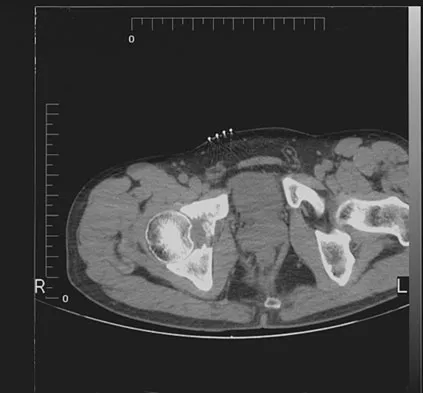
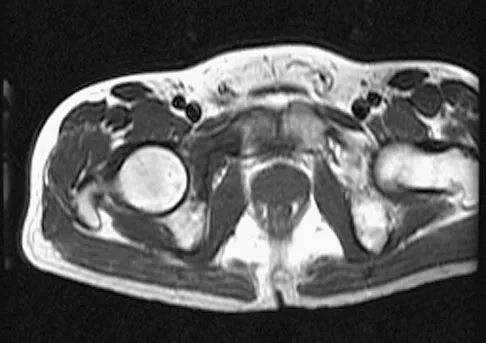

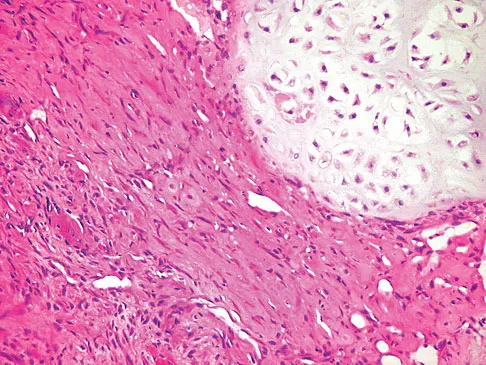
Explanation
The definitive surgery would be removal of the entire resection bed, and in this case of dedifferentiated chondrosarcoma, a hemipelvectomy was performed. The MRI and CT scans show an aggressive cartilage lesion. The histology, representative of a dedifferentiated chondrosarcoma, shows a bimorphic low-grade cartilage lesion with high-grade spindle cell sarcoma. The cartilage lesion is usually an enchondroma or low-grade chondrosarcoma. The dedifferentiated portion is typically a malignant fibrous histocytoma, osteosarcoma, or fibrosarcoma. Weber KL, Pring ME, Sim FH: Treatment and outcome of recurrent pelvic chondrosarcoma. Clin Orthop Relat Res 2002;397:19-28.
Question 60
High Yield
A 15-year-old boy reports feeling a pop and notes sudden giving way of the left knee while playing basketball. He has immediate pain and swelling in the knee. An AP radiograph is shown in Figure 32. A small avulsion fragment from the lateral tibial margin is the only finding. What is the most likely diagnosis?

Explanation
An avulsion fracture from the lateral tibial margin carries the eponym Segond fracture and is pathognomonic for an anterior cruciate ligament (ACL) tear. The fragment is located posterior to Gerdy's tubercle and is superior and anterior to the fibular head. It represents an avulsion of the lateral capsular ligament of the knee and is caused by the same mechanism that causes the ACL tear. The pes anserinus is the insertion point of the medial hamstrings and would not be affected in a lateral avulsion injury. The posterior cruciate ligament may be seen on a lateral view if associated with an avulsion fragment, but a tear of the PCL generally cannot be diagnosed on an AP view. The insertion of the iliotibial band is broad and is unlikely to produce an avulsion injury such as that seen in the radiograph. This view is not consistent with the appearance of a lateral collateral ligament injury. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 533-557.
Question 61
High Yield
Which of the following studies has the highest sensitivity and specificity in diagnosis of osteonecrosis of the femoral head?

Explanation
An MRI scan is both highly sensitive and specific for the evaluation of osteonecrosis. The measurement of increased intraosseous pressure can be technically difficult and the results have been variable. Plain radiographs can be normal early in the progression of osteonecrosis of the femoral head. The technetium Tc 99m bone scan is a very sensitive test. However, it is not specific; increased uptake can be noted in patients with arthritis, neoplastic disease, fracture, or sepsis. In addition, because of bilaterality, the frequency of false-negative scans is relatively high. Steinberg ME: Early diagnosis, evaluation, and staging of osteonecrosis, in Jackson DW (ed): Instructional Course Lectures 43. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 513-518.
Question 62
High Yield
A 52-year-old man has pain in the sternal area after landing on his right shoulder in a fall from his bicycle. In addition, he reports that he had difficulty swallowing and breathing immediately after the fall, but the symptoms resolved. A CT scan reveals a posterior sternoclavicular dislocation. Initial management should include
Explanation
Posterior sternoclavicular dislocations require rapid treatment because of the proximity of major neurovascular structures and the airway. Initial management should consist of closed reduction under general anesthesia in the operating room with a chest surgeon available. A successful closed reduction is usually stable. Internal fixation of sternoclavicular injuries should be avoided because of the likelihood of hardware migration and possible injury to the mediastinal structures. If closed reduction is unsuccessful, open reduction is indicated. Treatment following reduction of the sternoclavicular joint includes the application of a figure-of-8 splint and a sling for 6 weeks, followed by stretching and strengthening exercises. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont IL, American Academy of Orthopaedic Surgeons, 1999, pp 287-297.
Question 63
High Yield
A 27-year-old professional soccer player sustained an injury to his cervical spine in a collision with another player. Initially he was diagnosed with a right C6 radiculopathy that resolved with rest, anti-inflammatory medications, and physical therapy. Following a fall in a game, he noted a recurrence of neck pain without radicular signs or symptoms. Additional nonsurgical management over the past few months has failed to provide relief. A cervical MRI scan shows a right-sided C5-6 herniation without any evidence of disk disease at other cervical levels. The patient desires to continue his career as a professional soccer player. What treatment offers the best long-term option for return to play?
Explanation
The patient has chronic neck pain that is affecting his career as a professional soccer player. Although he had signs and symptoms of a right C6 radiculopathy, neck pain is his only current symptom. Therefore, procedures to address the relief of radiculopathy (keyhole foraminotomy and transforaminal epidural steroid injection) are likely to be ineffective. Although Watkins and others have described continuing nonsurgical management for symptomatic herniated disks and return to play only when asymptomatic, the patient has not found relief with these modalities. A single-level cervical fusion (either postoperative or congenital) generally is not considered a contraindication for return to play in collision or contact sports. Therefore, anterior cervical fusion at C5-6 offers the best long-term option for return to play. Watkins RG: Cervical spine injuries in athletes, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 373-386. Watkins RG: Neck injuries in football players. Clin Sports Med 1986;5:215-246. Morganti C, Sweeney CA, Albanese SA, et al: Return to play after cervical spine injury. Spine 2001;26:1131-1136.
Question 64
High Yield
An active 47-year-old woman with rheumatoid arthritis reports forefoot pain and deformity and has difficulty with shoe wear. Examination reveals hallux valgus and claw toes. A radiograph is shown in Figure 10. What is the most appropriate surgical treatment?

Explanation
Rheumatoid arthritis commonly affects the metatarsophalangeal joints, which become destabilized with time resulting in hallux valgus and dislocated lesser claw toes. The result is metatarsalgia as the dislocated claw toes "pull" the fat pad distally. Severe hallux valgus reduces first ray load, which compounds the metatarsalgia because the load is transferred to the lesser metatarsal heads. First metatarsophalangeal arthrodesis restores weight bearing medially and corrects the painful bunion. Metatarsal head resection slackens the toe tendons to allow correction of the claw toes by whatever means necessary and decreases plantar load over the forefoot. Rheumatoid arthritis in the first metatarsophalangeal joint will continue to progress if osteotomies or a Lapidus procedure are performed. Keller resection arthroplasty increases transfer metatarsalgia and reduces push-off power during gait. Flexor-to-extensor tendon transfer of the lesser toes does not address the metatarsalgia and does not correct the dislocation of the metatarsophalangeal joint. Coughlin MJ: Arthritides, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, p 572.
Question 65
High Yield
Figure 17 shows the radiograph of a 25-year-old professional football player who has superior shoulder pain that prevents him from sports participation. History reveals that he sustained a shoulder injury that was treated with closed reduction and temporary pinning 3 years ago. The best course of action should be
Explanation
The radiograph shows a complete acromioclavicular separation. Because the patient is a professional athlete who is unable to participate, surgery is indicated. Chronic separations, especially those with previous trauma from joint pinning, should be treated with resection of the distal clavicle and stabilization to the coracoid. Some type of biologic reconstruction of the coracoclavicular ligaments is generally recommended. Open repair of the ligaments is generally not possible in such a delayed fashion. Screw fixation alone will not provide a lasting solution as the screws usually need to be removed, leaving no fixation in place. Reconstruction using the coracoacromial ligament is generally recommended with coracoclavicular fixation to protect the repair while it heals. Nuber GW, Bowen MK: Disorders of the acromioclavicular joint: Pathophysiology, diagnosis and management, in Iannotti JP, Williams GR (eds): Disorders of the Shoulder: Diagnosis and Management. Philadelphia, PA, Lippincott Williams and Wilkins, 1999.
Question 66
High Yield
Human tendons are made up primarily of what collagen type (~95%)?
Explanation
Tendons are dense, primarily collagenous tissues that attach muscle to bone. Collagen content of the dry weight is slightly greater than that found in ligaments and is predominantly type I. Type III collagen makes up the remaining ~5% of total collagen content. Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 10-12. Garrett WE, Speer KP, Kirkendall DT (eds): Principles & Practice of Orthopaedic Sports Medicine. Philadelphia, PA, Lippincott Williams & Wilkins, 2000, pp 21-37.
Question 67
High Yield
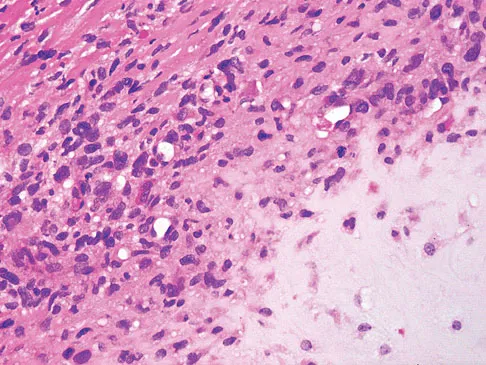
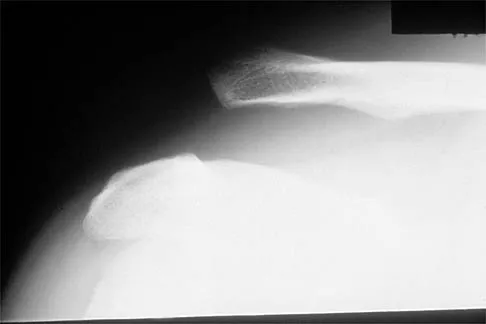
A 16-year-old boy has had left knee pain and swelling after sustaining a minor twisting injury while playing basketball 2 weeks ago. Figures 5a through 5e show the radiograph, MRI scans, and biopsy specimens. What is the most likely diagnosis?

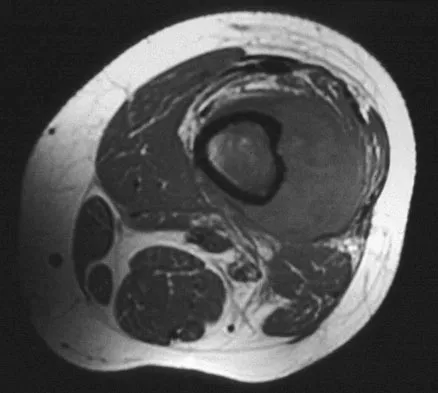

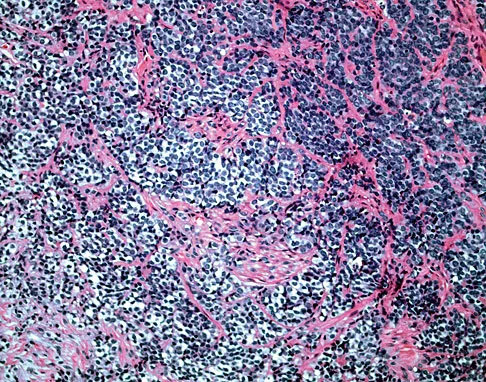
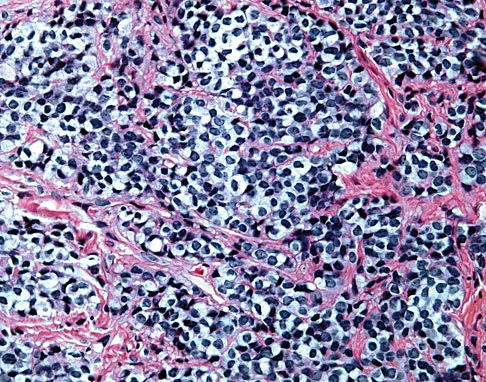
Explanation
The imaging studies and histology are most consistent with Ewing's sarcoma. Tuberculosis can show small round blue cells on histology (lymphocytes associated with chronic infection) but would more typically involve the knee joint and periarticular bone. Osteosarcoma and MFH do not have small round blue cells histologically. Sissons HA, Murray RO, Kemp HBS: Orthopaedic Diagnosis. Berlin, Springer-Verlag, 1984, pp 254-256.
Question 68
High Yield
The MRI findings shown in Figure 51 would most likely create which of the following signs and symptoms?
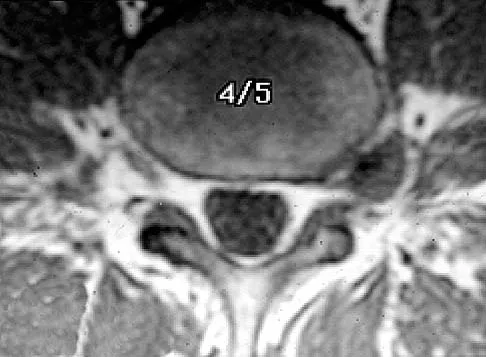
Explanation
The MRI scan shows a far lateral disk herniation. With the L4-5 disk, a far lateral herniation abuts the left L4 nerve root. The findings would be consistent with those of a left L4 radiculopathy and would include pain or a sensory deficit on the anteromedial aspect of the knee, diminished patellar tendon reflex, and quadriceps weakness, perhaps making it difficult to walk up and down stairs. Fardin DF, Garfin SR (eds): Orthopaedic Knowledge Update: Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 329.
Question 69
High Yield
A 30-year-old man has chronic pain, joint stiffness, and symmetrical polyarthropathy but no significant synovitis. Examination reveals enlargement of the second and third metatarsal heads. Radiographs show chondrocalcinosis of the ankles and bony enlargement of the midfoot; no marginal erosions are evident at the metatarsophalangeal level. What is the most likely diagnosis?
Explanation
The patient's clinical picture is considered the classic presentation for hemochromatosis. Osteoarthritis and pseudogout more commonly affect an older age group. Rheumatoid arthritis is more common in women and is not commonly associated with chondrocalcinosis. The radiographic appearance of the forefoot in Reiter's syndrome is one of a pencil in cup deformity of the metatarsophalangeal joint, not enlargement. Stevens FM, Edwards C: Recognizing and managing hemochromatosis and hemochromatosis arthropathy. J Musculoskeletal Med 2004;4:212-225.
Question 70
High Yield
Which of the following best describes the resultant forces on an increased offset stem when compared with a standard offset stem?

Explanation
The increased emphasis on restoring offset in total hip arthroplasty has implications for the forces applied to the components and the fixation interfaces. Static analysis has shown that with an increased affect, joint reaction force on the articulation is decreased. When the resultant load on the hip is "out of plane" (ie, directed anterior to posterior), there is increased torsion where the stem is turned into more retroversion. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 134-180. Hurwitz DE, Andriaacchi TP: Biomechanics of the hip, in Callaghan J, Rosenberg AG, Rubash HE (eds): The Adult Hip. Philadelphia, PA, Lippincott-Raven , 1998.
Question 71
High Yield
A 64-year-old man with a history of metastatic lung cancer reports increasing right hip pain over the period of several months. Radiographs are shown in Figures 3a and 3b. Initial management should consist of


Explanation
The patient has lung cancer metastatic to the right proximal femur. The lesion is large, has destroyed a portion of the cortex, and involves the peritrochanteric region. All of these findings put the patient at high risk for pathologic fracture. The lesion is amenable to intramedullary fixation in the form of some type of reconstruction nail. Chemotherapy alone will not restore the bone stock. Given the extent of the lesion, radiation therapy, chemotherapy, or embolization will not prevent fracture. A proximal femoral replacement would be indicated in patients with bone destruction extending into the femoral head and neck. Bisphosphonates may diminish the risk of subsequent lesions but are not sufficient to treat this high-risk lesion. Radiation therapy should be given postoperatively to prevent further bone destruction.
Question 72
High Yield
A 22-year-old woman injures her neck in a motor vehicle accident. Examination reveals no sensory or motor function below T8. Radiographs and an MRI scan show a burst fracture at T7. Forty-eight hours later, the bulbocavernosus reflex is present but there is no evidence of motor or sensory recovery in the lower extremities. What is the most likely diagnosis?

Explanation
Spinal shock typically ends after 48 hours with the return of reflexes, including the bulbocavernosus reflex. Lack of motor or sensory recovery in the lower extremities with the return of reflexes generally indicates a complete cord syndrome. Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 179-187.
Question 73
High Yield
Which of the following tendons is the primary antagonist of the posterior tibialis tendon?

Explanation
The primary action of the posterior tibialis tendon is inversion of the foot; secondarily, it plantar flexes the ankle. The anterior tibialis tendon also inverts the foot and only partially antagonizes the posterior tibialis tendon. The primary action of the peroneus longus is plantar flexion of the first ray. It secondarily everts the posterior tibialis tendon. The action of the flexor digitorum longus tendon is synergistic with the posterior tibialis tendon. The primary action of the peroneus brevis tendon is eversion; therefore, it is the primary antagonist of the posterior tibialis tendon. Sarrafian SK: Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993, pp 550-551.
Question 74
High Yield
Which of the following is a true statement regarding thoracic disk herniations?
Explanation
Symptomatic herniations of the thoracic spine are much less common than those of the cervical or lumbar region. They tend to occur most commonly during the third to fifth decades of life and although they can be found at all levels, they are most common in the lower third near the thoracolumbar region. Posterior laminectomy and disk excision has the highest rate of neurologic deterioration and is not recommended. Multiple studies have shown that herniated thoracic disks can be found at one or more levels in 40% of asymptomatic individuals. Shah RP, Grauer JN: Thoracoscopic excision of thoracic herniated disc, in Vaccaro AR, Bono CM (eds): Minimally Invasive Spine Surgery. New York, NY, Informa Healthcare, 2007, pp 73-80.
Question 75
High Yield
Figure 24 shows the radiograph of an otherwise healthy 56-year-old patient who reports hip pain after undergoing a primary cementless hip replacement 4 months ago. The next most appropriate step should consist of

Explanation
Periosteal new bone formation is a warning sign of prosthetic infection. Indomethacin may prevent heterotopic ossification if given early enough; however, it is irrelevant in this patient. A C-reactive protein and a sed rate are useful screening studies that add to the predictive value of the radiographs and may be performed routinely if sepsis is suspected. A bone scan obtained 4 months after surgery would show increased uptake in all cases. If results of a sed rate and C-reactive protein are normal, then a biopsy should be considered to rule out a neoplasm.
Question 76
High Yield
A 15-year-old boy has hindfoot pain and very limited subtalar motion. A CT scan reveals a talocalcaneal coalition involving 40% of the middle facet. He has no degeneration of the posterior subtalar facet. Following failure of nonsurgical management, treatment should consist of
Explanation
The CT scan is an important test to help determine the extent of involvement of the talocalcaneal facet in a talocalcaneal coalition. In a young patient with no arthritis and joint involvement of less than 50%, resection of the coalition and fat pad interposition has been shown to be successful. A calcaneal osteotomy does not address the coalition. Subtalar arthroereisis has been used for treatment of a flexible flatfoot; tarsal coalition patients have a rigid-type flatfoot deformity. Sullivan JA: The child's foot, in Morrissy RT, Weinstein SL (eds): Lovell and Winter's Pediatric Orthopaedics, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 2, pp 1077-1135.
Question 77
High Yield
Which of the following statements most accurately describes the layers of articular cartilage?
Explanation
Normal articular cartilage is composed of three zones that are based on the shape of the chondrocytes and the distribution of the type II collagen. The tangential zone has flattened chondrocytes, condensed collagen fibers, and sparse proteoglycan. The intermediate zone is the thickest layer with round chondrocytes oriented in perpendicular or vertical columns paralleling the collagen fibers. The basal layer is deepest with round chondrocytes. The tidemark is deep to the basal layer and separates the true articular cartilage from the deeper cartilage that is a remnant of the cartilage anlage, which participated in endochondral ossification during longitudinal growth in childhood. The tidemark divides the superficial uncalcified cartilage from the deeper calcified cartilage and also is the division between nutritional sources for the chondrocytes. The tidemark is the zone in which chondrocyte renewal took place in childhood. The tidemark is found only in joints and not in the cap of an enchondroma. It is seen most prominently in the adult, nongrowing joint.
Question 78
High Yield
When compared with a patient who has a subluxated hip, a patient with a dislocated hip who is undergoing acetabular reconstruction for developmental dysplasia of the hip will most likely have

Explanation
The rate of revision has been found to be significantly increased in patients with a dislocated hip preoperatively compared with patients with a subluxated hip. This may be the result of compromised acetabular bone stock. The rate of nerve palsy may be increased because of the greater degree of lengthening required to reduce the reconstructed hip. Numair J, Joshi AB, Murphy JC, Porter ML, Hardinge K: Total hip arthroplasty for congenital dysplasia or dislocation of the hip: Survivorship analysis and long-term results. J Bone Joint Surg Am 1997;79:1352-1360.
Question 79
High Yield
A 39-year-old woman fell onto her flexed elbow and sustained a comminuted displaced radial head and neck fracture. Radiographs confirm concentric reduction of the ulnohumeral joint. Examination reveals pain with compression of the radius and ulna at the wrist. What is the best treatment for the radial head fracture?
Explanation
Patients with comminuted radial neck and head fractures and associated wrist pain have a significant injury to the elbow and forearm. Nonsurgical management is an option, but initial casting will result in stiffness and early range of motion is likely to be unsuccessful secondary to pain. Surgical treatment with open reduction and internal fixation, although possible, is technically demanding and results are unpredictable with comminuted fractures. Excision alone in the face of wrist pain may lead to radial shortening. The treatment of choice is excision and metallic radial head arthroplasty. Silastic implants have been associated with synovitis and wear debris. Furry KL, Clinkscales CM: Comminuted fractures of the radial head: Arthroplasty versus internal fixation. Clin Orthop 1998;353:40-52.
Question 80
High Yield
A 45-year-old woman has idiopathic scoliosis. Surgery is to include an anterior thoracic release through an open left thoracotomy. The thoracotomy will have what effect on the patient's pulmonary function postoperatively?
Explanation
A thoracotomy in an adult with idiopathic scoliosis causes a reduction in pulmonary function that often does not return to preoperative levels. What pulmonary function that does recover, recovers over many months. Long-term improvement in pulmonary function, compared to preoperative function, is rarely seen. This should be considered in planning surgical intervention in adults with scoliosis. Graham EJ, Lenke LG, Lowe TG, et al: Prospective pulmonary function evaluation following open thoracotomy for anterior spinal fusion in adolescent idiopathic scoliosis. Spine 2000;25:2319-2325.
Question 81
High Yield
A 22-year-old wrestler who underwent an open anterior shoulder reconstruction to repair a dislocated shoulder 6 months ago now reports shoulder pain after attempting a takedown. Examination reveals external rotation that is 15 degrees greater than the contralateral side. He has pain associated with abduction and external rotation but no apprehension. Which of the following tests would most likely reveal positive findings?
Explanation
Postoperative subscapularis detachment can be identified with a positive lift-off test that reveals weakness in internal rotation. This complication does not necessarily compromise the anterior capsule repair. The load-and-sift maneuver and articular contrast studies may be normal. Supraspinatus tests for impingement and weakness should be negative. Gerber C, Krushell RJ: Isolated ruptures of the tendon of the subscapularis muscle: Clinical fractures in 16 cases. J Bone Joint Surg Br 1991;73:389-394.
Question 82
High Yield
What is the most common cause of mechanical failure of an orthopaedic biomaterial during clinical use?
Explanation
In most orthopaedic applications, the materials are strong enough to withstand a single cycle of loading in vivo. However, these loads may be large enough to initiate a small crack in the implant that can grow slowly over thousands or millions of cycles, eventually leading to gross failure. Such fatigue failure has occurred with virtually every type of implant, including stainless steel fracture plates and screws, bone cement in joint arthroplasty, and polyethylene inserts in total knee arthroplasty. Lewis G: Fatigue testing and performance of acrylic bone-cement materials: State-of-the-art review. J Biomed Mater Res Br 2003;66:457-486. Stolk J, Verdonschot N, Huiskes R: Stair climbing is more detrimental to the cement in hip replacement than walking. Clin Orthop 2002;405:294-305.
Question 83
High Yield
A 17-year-old high school soccer player sustains an anterior cruciate ligament (ACL) tear at the beginning of the season. An MRI scan confirms a complete ACL tear with no meniscal injuries. The patient plans an early return to play and would like to avoid surgery. Therefore, the patient and family should be advised that nonsurgical management consisting of rehabilitative exercises and the use of a functional knee brace will most likely result in

Explanation
While there are athletes who can function at a full level with an ACL tear, they are in the minority. As yet, there is no reliable way to predict the patients who will be able to compensate for the loss of the ACL. Studies have confirmed the risk of recurrent instability and meniscal injury in athletes with an ACL-deficient knee who participate in cutting sports. One study showed that only 12 of 43 patients who attempted rehabilitation and bracing were able to return successfully for the season. Another study showed that 17 of 31 athletes who were able to return to their sport sustained 23 meniscal tears because of recurrent instability. Shelton WR, Barrett GR, Dukes A: Early season anterior cruciate ligament tears: A treatment dilemma. Am J Sports Med 1997;25:656-658.
Question 84
High Yield
What normal tissue has a low signal intensity (appears black) on both T1- and T2-weighted images?
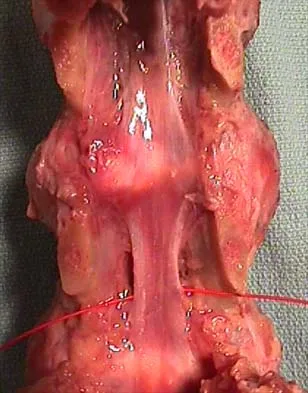
Explanation
Tendons, cortical bone, ligaments, menisci, and fibrous tissue will show low signal intensity (SI) on both T1- and T2-weighted images. Fat-containing tissues, such as subcutaneous fat and bone marrow, will show high SI on T1-weighted images and low SI on T2-weighted images. Tissues with high water content, such as joint fluid, intervertebral disk, and edema, will show low SI on T1-weighted images and high SI on T2-weighted images. Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 65-70.
Question 85
High Yield
Figure 17 shows the radiograph of a 2-year-old girl who sustained a fracture of the femur in a fall while walking with her parents. History reveals that this is her third long bone fracture, having sustained a humerus fracture 1 year ago and a fracture of the opposite femur 9 months ago. There is no family history of any similar problem. Examination reveals distinctly blue sclerae, normal appearing teeth, and no skin lesions. What is the most likely cause of this patient's disorder?

Explanation
Osteogenesis imperfecta (OI) is a genetically determined disorder of type I collagen synthesis that is characterized by bone fragility. This patient has had three fractures of the long bones by age 2 years, with the last one occurring after relatively minor trauma. The patient's history and clinical features are consistent with a diagnosis of Sillence type IA OI. Type I OI is the mildest and most common form. Inheritance is autosomal-dominant; however, as in this patient, new mutations are frequent. Type I is subclassified into the A type (absence of dentinogenesis imperfecta) and B type (presence of dentinogenesis imperfecta). The sclerae are blue, and the first fractures usually occur in the preschool years after walking has begun. Cells from individuals with type I OI largely demonstrate a quantitative defect of type I collagen; they synthesize and secrete about half the normal amount of type I procollagen. Qualitative mutations that lead to an abnormal type I procollagen molecule result in more severe types of the disorder. There are no indications that this child has been abused. Radiographs of the femur show no evidence of rickets, pyknodysostosis, or osteopetrosis. Morquio syndrome, characterized by excess excretion of keratin sulfate in the urine, is not associated with bone fragility. Kocher MS, Shapiro F: Osteogenesis imperfecta. J Am Acad Orthop Surg 1998;6:225-236. Sillence DO, Senn A, Danks DM: Osteogenesis imperfecta: An expanding panorama of variants. Clin Orthop 1981;159:11-25.
Question 86
High Yield
Figure 7 shows the radiograph of an otherwise healthy 65-year-old man who injured his right dominant shoulder while skiing 18 months ago. He did not seek treatment at the time of the injury. He now reports intermittent soreness when playing golf but has no other limitations. Examination reveals full range of motion and no tenderness, but he has slight pain with a crossed arm adduction stress test. He is neurologically intact. Initial management should consist of

Explanation
The radiograph shows a displaced type II distal clavicle fracture with nonunion. Because the patient's symptoms are minimal, the injury can be treated like a grade III acromioclavicular separation. Present management should consist of ice, anti-inflammatory drugs, activity modification, and perhaps physical therapy. If nonsurgical management fails to provide relief, the surgical options are varied with no uniformity in the literature regarding surgical treatment of this injury. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 271-286.
Question 87
High Yield
Atraumatic neuropathy of the suprascapular nerve usually occurs at what anatomic location?
Explanation
The suprascapular nerve passes through the suprascapular notch and the spinoglenoid notch before innervating the infraspinatus muscle. At both locations, the suprascapular nerve is prone to nerve compression, which often results from a ganglion cyst. The other anatomic locations are not associated with suprascapular nerve impingement. Romeo AA, Rotenberg DD, Bach BR: Suprascapular neuropathy. J Am Acad Orthop Surg 1999;7:358-367.
Question 88
High Yield
A 23-year-old woman has had vague left knee pain for the past 6 months. A radiograph and CT scan are shown in Figures 50a and 50b. What is the most likely diagnosis?

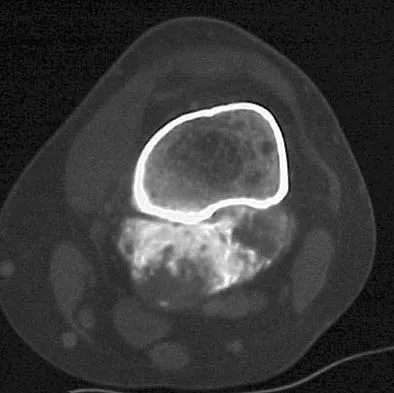
Explanation
The radiographic appearance of the lesion emanating from the posterior cortex of the left distal femur is consistent with a surface bone-producing lesion; therefore, the most likely diagnosis is a parosteal osteosarcoma. In an osteochondroma, the cortex and medullary cavity of the lesion are in continuity with that of the native bone. A dedifferentiated chondrosarcoma has histologic components of a high-grade sarcoma plus a benign or low-grade malignant cartilage tumor. Tumoral calcinosis is characterized by amorphous calcium in the soft tissues and does not emanate from the bone itself. While often confused with parosteal osteosarcoma, myositis ossificans is usually more mature at the periphery of the lesion rather than the center. In addition, myositis ossificans does not involve the underlying cortex but remains separate from the bone. Unni KK: Dahlin's Bone Tumors: General Aspects and Data on 11,087 Cases, ed 5. Philadelphia, PA, Lippincott-Raven, 1996, pp 185-196.
Question 89
High Yield
Osteoporosis is best diagnosed by
Explanation
Risk factors can suggest the existence of osteoporosis. However, definitive testing, based on the use of bone densitometry measurements, uses the T score in which an average score is taken from a normal population of young women. The presence of increased osteoid in lamellar bone is seen in osteomalacia but not osteoporosis. The presence of fractures is evidence of a risk factor for osteoporosis and can predict future fractures, but it does not definitively confirm the diagnosis. The Singh index is a radiographic finding that is not as accurate as bone mineral density scores.
Question 90
High Yield
A 45-year-old man has severe pain in both feet after his boots become wet while hunting. Examination 3 hours after the onset of symptoms reveals that his feet are cold to touch and the skin appears blanched. Management should consist of
Explanation
The patient has frostbite involving both feet. Rapid rewarming in a protected environment is the initial treatment. A footbath with water at 104.0 degrees F to 107.6 degrees F (40 degrees C to 42 degrees C) is ideal. This facilitates a uniform rewarming of the involved tissue. The other choices are less than ideal. Appliances such as heating pads provide uneven heating and may actually burn the skin. Pinzur MS: Frostbite: Prevention and treatment. Biomechanics 1997;4:14-21.
Question 91
High Yield
A 24-year-old man reports the development of a foot drop following a knee dislocation 1 year ago. The common peroneal nerve was found to be in continuity at the time of surgical reconstruction of the posterolateral corner of the knee joint. He would like to eliminate the need for an ankle-foot orthosis. What is the best option to achieve elimination of the orthosis?
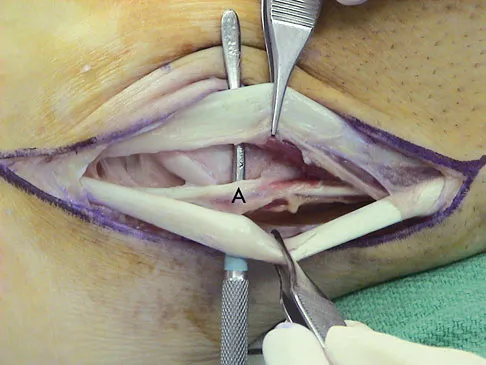
Explanation
The ankle dorsiflexor muscles have been denervated for too long a period to expect reinnervation to be successful. Even if the extensor hallucis longus tendon was functional, it is unlikely to have sufficient strength to achieve dynamic ankle dorsiflexion. The tibialis posterior tendon transfer has been shown to predictably achieve these goals in a high percentage of patients. Successful ankle fusion is likely to fail with time due to the development of forefoot equinus. Pinzur MS, Kett N, Trilla M: Combined anteroposterior tibial tendon transfer in post-traumatic peroneal palsy. Foot Ankle 1988;8:27l-275.
Question 92
High Yield
A 22-year-old college quarterback is tackled and sustains a reducible first carpometacarpal dislocation. What is the recommended treatment?
Explanation
When comparing closed reduction and pinning to ligament reconstruction, the reconstruction group had slightly better abduction and pinch strength. The volar oblique ligament usually tears off the first metacarpal in a subperiosteal fashion. In this young patient, motion-sparing procedures are preferred. Simonian PT, Trumble TE: Traumatic dislocation of the thumb carpometacarpal joint: Early ligamentous reconstruction versus closed reduction and pinning. J Hand Surg Am 1996;21;802-806.
Question 93
High Yield
What is the most common malignancy involving the hand?
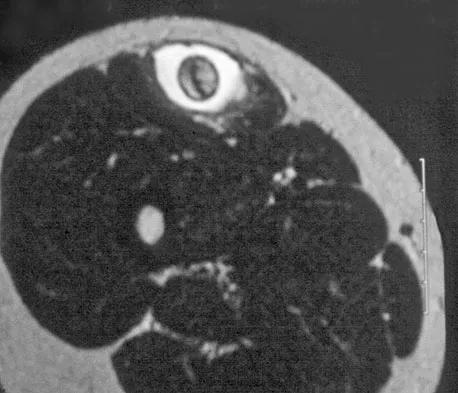
Explanation
Skin cancers far outnumber primary musculoskeletal malignancies of the hand and the most common of these is squamous cell carcinoma. Metatastic lung carcinoma, while classic for the carcinoma that metastasizes to the hand, does so at an extremely low rate. Fink JA, Akelman E: Nonmelanotic malignant skin tumors of the hand. Hand Clin 1995;11:255-264.
Question 94
High Yield
A 35-year-old woman who is a recreational runner reports posterior knee pain and tightness in the knee with flexion during running. She denies any history of trauma. Examination reveals normal patellar glide and tilt and no patellar apprehension. Range of motion is 5 degrees to 120 degrees, and quadriceps function and knee ligamentous examination are normal. Radiographs are normal. An MRI scan is shown in Figure 18. What is the most likely diagnosis?
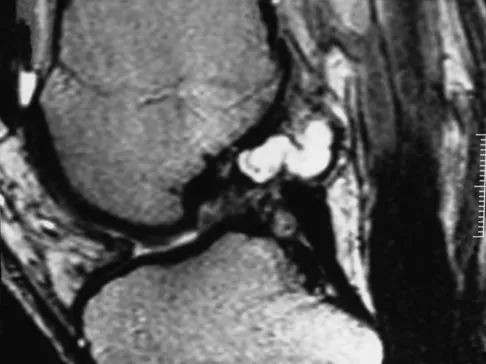
Explanation
Ganglia involving the cruciate ligaments have been recently reported as a cause of knee pain that interferes with knee flexion and extension. The symptoms are poorly localized in this patient and not along the medial joint line, making the diagnosis of a torn medial meniscus less likely. In addition, the MRI findings do not show a significant medial meniscal lesion. A Baker's cyst is usually posteromedial and extends posterior to the interval between the medial head of the gastrocnemius and semimembranosus. MRI scans show a fluid-filled lesion with an increased signal on T1- and T2-weighted images. A lipoma would be bright on the T1-weighted image only. Deutsch A, Veltri DM, Altchek DW, et al: Symptomatic intraarticular ganglia of the cruciate ligaments of the knee. Arthroscopy 1994;10:219-223.
Question 95
High Yield
What is a common clinical finding in patients with severe hypercalcemia secondary to bony metastasis?
Explanation
Increased levels of calcium are known to cause anorexia, nausea, vomiting, dehydration, muscle weakness, polyuria, and polydipsia. Treatment may include hydration, saline diuresis, and bisphosphonates.
Question 96
High Yield
A 14-year-old boy who is right handed reports right shoulder pain. Radiographs show a lucent lesion of the proximal humeral epiphysis with a narrow zone of transition. Results of an open biopsy confirm the presence of a chondroblastoma. Based on these findings, the next most appropriate step in management should consist of

Explanation
The patient has a chondroblastoma of the proximal humerus; therefore, the treatment of choice is curettage and bone grafting. Surgical resection of the proximal humerus is not indicated in the initial treatment of an intraosseous chondroblastoma. Mirra JM: Bone Tumors: Clinical, Radiologic, and Pathologic Correlations. Philadelphia, PA, Lea and Febiger, 1989, pp 589-623.
Question 97
High Yield
A 49-year-old woman noted pain in her right axilla 1 day after moving heavy furniture. Two weeks later, she now reports persistent numbness and paresthesias along the inner aspect of her upper arm radiating into the ulnar digits. Examination reveals full shoulder motion, tenderness over the first rib, and a decreased radial pulse with the shoulder placed overhead. What is the most likely diagnosis?

Explanation
Thoracic outlet syndrome is thought to be caused by compression of the neurovascular supply to the upper limb in the supraclavicular and axillary regions of the shoulder. While typically progressive in onset, thoracic outlet syndrome may develop after acute injury. Injury or weakness of the scapular muscles, especially the trapezius, may result in descent of the scapula and cause compression of the thoracic outlet. In general, most symptoms are the result of neural compression. Typical symptoms include pain in the neck or shoulder and numbness or tingling that predominantly involves the ulnar side of the arm and hand. Exacerbation of these symptoms is typical when the arm is abducted. Initial management should consist of postural exercises aimed at restoring proper scapular stability. Severe recalcitrant symptoms may warrant surgical decompression. Leffert RD: Thoracic outlet syndrome. J Am Acad Orthop Surg 1994;2:317-325.
Question 98
High Yield
A 21-year-old collegiate pitcher has had pain in his dominant shoulder for the past 3 months despite management consisting of rest, rehabilitation, and an analysis of throwing mechanics. An arthroscopic photograph from the posterior portal is shown in Figure 10. The biceps anchor to the bone was not detached to probing. Treatment of the lesion to the left of the cannula should consist of arthroscopic
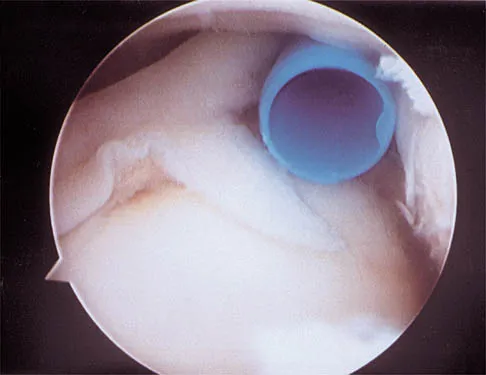
Explanation
The lesion is a variation of a type I superior labrum anterior and posterior lesion; therefore, appropriate treatment is simple debridement. Biceps tenodesis or release is not indicated because the biceps tendon and anchor are intact. There is no indication for labral repair or capsulorraphy. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 261-270.
Question 99
High Yield
What is the most common bacteria cultured from dog and cat bites to the upper extremity?
Explanation
To define bacteria responsible for dog and cat bite infections, a prospective study yielded a median of five bacterial isolates per culture. Pasteurella is most common from both dog bites (50%) and cat bites (75%). Pasteurella canis was the most frequent pathogen of dog bites, and Pasteurella multocida was the most common isolate of cat bites. Other common aerobes included streptococci, staphylococci, moraxella, and neisseria.
Question 100
High Yield
Free flap coverage for severe trauma to the upper extremity has the fewest complications when performed within what time period after injury?
Explanation
Flap necrosis and infection rates are lowest if free flap coverage is performed within 72 hours of injury. Delays beyond 72 hours are associated with a higher rate of complications. Godina M: Early microsurgical reconstruction of complex trauma of the extremities. Plast Reconstr Surg 1986;78:285-292.
