INTRODUCTION AND EVIDENCE-BASED PRINCIPLES
The operative management of full-thickness rotator cuff tears represents a cornerstone of modern orthopedic shoulder surgery. The primary objective of surgical intervention is to achieve a biomechanically stable, tension-free repair that restores the anatomical footprint of the rotator cuff, thereby optimizing the biological environment for tendon-to-bone healing.
Historically, the biologic healing of rotator cuff repairs has been a subject of intense academic scrutiny. Early arthroscopic techniques yielded variable results. As noted in foundational literature, Galatz et al. found less evidence of robust healing in arthroscopic procedures performed between 1997 and 2000, largely due to the biomechanical limitations of early anchor designs and single-row constructs that failed to adequately compress the tendon against the tuberosity. However, with the evolution of surgical techniques, instrumentation, and a deeper understanding of tear morphology, outcomes have improved dramatically. Boileau et al. subsequently demonstrated that modern arthroscopic repairs of full-thickness cuff tears do, in fact, heal reliably when meticulous attention is paid to footprint restoration, mechanical stability, and biological augmentation.
Clinical Pearl: The transition from older, high-failure-rate techniques to modern success is rooted in the recognition of tear patterns and the application of margin convergence. Restoring the biomechanical linkage of the rotator cable is paramount to preventing tension overload at the repair site.
PREOPERATIVE EVALUATION AND IMAGING
Clinical Assessment
Patients typically present with night pain, weakness in elevation and external rotation, and a positive impingement profile. A thorough clinical examination must assess the integrity of the supraspinatus (Jobe’s test), infraspinatus (resisted external rotation, lag signs), and subscapularis (lift-off, belly-press, bear-hug tests).
Advanced Imaging
Magnetic Resonance Imaging (MRI) without contrast is the gold standard for evaluating full-thickness tears. The surgeon must systematically evaluate:
* Tear Size and Retraction: Measured in both the coronal and sagittal planes (Patte classification).
* Muscle Atrophy and Fatty Infiltration: Graded using the Goutallier classification on T1-weighted sagittal oblique images. Grades 3 and 4 fatty infiltration are generally considered irreversible and portend a higher rate of structural failure post-repair.
* Tendon Quality: Assessing the thickness and signal intensity of the residual tendon stump.
SURGICAL ANATOMY AND TEAR PATTERN RECOGNITION
Recognizing the geometric configuration of the tear is the most critical step in arthroscopic rotator cuff repair. Failure to recognize the tear pattern leads to non-anatomic, high-tension repairs that are doomed to mechanical failure. Tears are rarely simple, two-dimensional avulsions; they are complex, three-dimensional structural failures that must be reduced along their specific axes of mobility.
Acute L-Shaped Tears
Acute L-shaped tears typically involve the supraspinatus (SS) and the rotator interval (RI). These tears have a longitudinal component (parallel to the tendon fibers) and a transverse component (avulsed from the greater tuberosity).
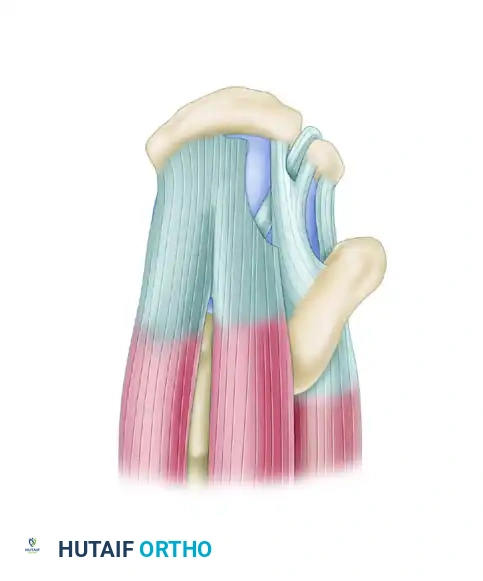
Superior view of an acute L-shaped rotator cuff tear involving the supraspinatus and rotator interval.
The biomechanical principle of repairing an L-shaped tear dictates that the longitudinal split must be addressed first. Attempting to pull the apex of the tear directly lateral to the tuberosity will result in excessive tension and dog-ear deformity.
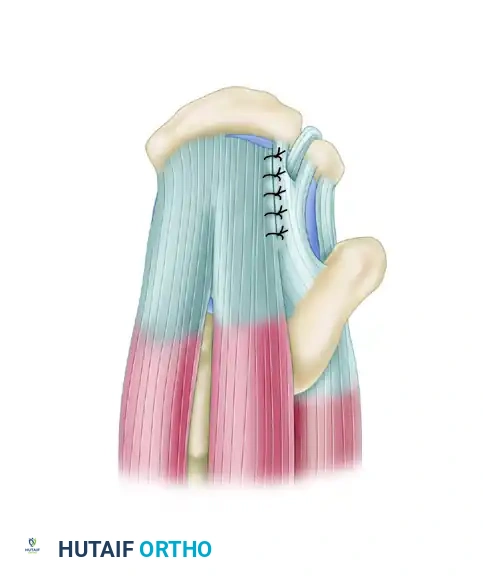
Tears should be initially repaired along the longitudinal split using side-to-side sutures.
Once the longitudinal split is closed, the tear is effectively converted into a smaller, crescent-shaped tear. This converged margin can then be repaired directly to the bone footprint with minimal tension.

The converged margin is finally repaired to the bone footprint.
Chronic L-Shaped and U-Shaped Tears
When an L-shaped tear is left untreated, chronic retraction and remodeling cause it to assume a U-shaped configuration.
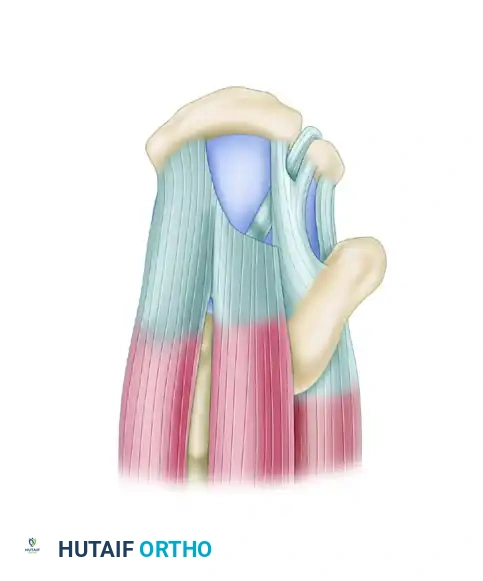
Superior view of a chronic L-shaped tear, which has retracted and assumed a U-shaped configuration.
Despite their retracted appearance, these tears often exhibit excellent mobility from an anterior-to-posterior direction. Typically, one tear margin (usually the posterior leaf involving the infraspinatus) is more mobile than the anterior leaf. The principle of margin convergence, popularized by Burkhart, is essential here.

Tears should be initially repaired using side-to-side sutures, applying the principle of margin convergence to reduce strain on the final bone repair.
By placing side-to-side sutures starting at the medial apex of the tear and working laterally, the surgeon zips the tear closed. This significantly reduces the strain on the free edge of the tendon.

The converged margin is then repaired to the bone in a tension-free manner.
Surgical Warning: Never attempt to pull a chronic U-shaped tear directly lateral to the tuberosity without first performing margin convergence. Doing so will exceed the ultimate tensile strength of the tendon, leading to immediate intraoperative suture pull-through or early postoperative failure.
EVIDENCE-BASED SURGICAL ALGORITHM
The decision to perform a single-row versus a double-row repair depends heavily on the size of the tear, the quality of the tendon, and the surgeon's technical proficiency. Both open and arthroscopic techniques are viable, though the all-arthroscopic approach is currently favored for its ability to preserve the deltoid origin and minimize postoperative morbidity.
Footprint coverage must be obtained under physiological tension. Furthermore, biomechanical studies have demonstrated that multiple suture passes through the tendon (e.g., three sutures instead of two per anchor) significantly increase the load-to-failure and provide superior contact pressure at the tendon-bone interface.
Based on current literature and biomechanical yield strengths, we utilize the following strict treatment algorithm for full-thickness tears:
1. Small Tears (1.0 cm)
- Construct: Single-row repair.
- Fixation: One suture anchor.
- Suture Configuration: Two simple sutures (or one mattress suture) passed through the tendon. This provides adequate compression for small, unretracted tears without overcrowding the footprint.
2. Medium Tears (1.5 cm)
- Construct: Single-row repair.
- Fixation: One suture anchor.
- Suture Configuration: Three sutures passed through the tendon. The addition of the third suture pass significantly increases the footprint contact area and biomechanical strength, which is necessary as the tear size increases.
3. Medium-to-Large Tears (> 1.5 cm to 3.0 cm)
- Construct: Single-row or equivalent repair.
- Fixation: Two suture anchors.
- Suture Configuration: Multiple passes (typically 4 to 6 suture limbs) to ensure broad coverage across the greater tuberosity.
4. Large Tears (> 3.0 cm)
- Construct: Double-row repair (or transosseous-equivalent/suture-bridge technique).
- Rationale: For tears larger than 3.0 cm, a double-row repair has been shown in several high-level studies to be biomechanically superior to single-row repairs. It maximizes footprint coverage, provides a pressurized seal against synovial fluid intrusion, and significantly lowers the re-tear rate in large defects.
MANAGEMENT OF MASSIVE ROTATOR CUFF TEARS
Massive rotator cuff tears (typically defined as involving two or more complete tendons or measuring > 5 cm) present a unique surgical challenge. These tears are often associated with significant retraction, capsular contracture, and altered glenohumeral kinematics.
Tendon Mobilization and Releases
Before any anchors are placed, extensive mobilization is mandatory.
1. Intra-articular Release: Release of the capsule from the undersurface of the rotator cuff.
2. Subacromial Release: Excision of the bursa and release of adhesions between the cuff and the acromion.
3. Coracohumeral Ligament (CHL) Release: The CHL is a primary restrictor to lateral excursion of the supraspinatus and infraspinatus. Releasing the CHL at the base of the coracoid process is often the key to achieving a tension-free repair.
Fixation Strategy for Massive Tears
If structural supplementation (e.g., dermal allograft or synthetic mesh) is not utilized, the repair relies heavily on margin convergence.
Pitfall: In massive, chronically retracted tears, attempting a double-row repair often over-tensions the construct.
For massive cuff tears, after releases and margin convergence are complete, fixation is usually performed as a single row just lateral to the articular surface. Medializing the footprint slightly prevents tension overload and failure at the muscle-tendon interface. The goal is to restore a balanced force couple (anterior subscapularis and posterior infraspinatus/teres minor) to stabilize the humeral head, even if complete lateral footprint coverage is impossible.
SURGICAL TECHNIQUE: STEP-BY-STEP
1. Patient Positioning and Setup
The procedure can be performed in either the beach-chair or lateral decubitus position, based on surgeon preference.
* Beach Chair: Offers excellent anatomical orientation and ease of conversion to an open procedure if necessary.
* Lateral Decubitus: Provides excellent visualization of the subacromial space and utilizes longitudinal traction to open the glenohumeral joint.
2. Diagnostic Arthroscopy and Footprint Preparation
A standard posterior viewing portal is established. An anterior portal is created through the rotator interval. The tear is assessed for size, pattern, and mobility. The greater tuberosity footprint is prepared using a motorized shaver and a radiofrequency wand to remove soft tissue remnants.
* Decortication: The cortical bone is lightly decorticated to a bleeding bed to stimulate marrow-derived mesenchymal stem cells. Aggressive burring should be avoided, as it removes the strong cortical bone necessary for anchor purchase.
3. Anchor Placement and Suture Passing
Anchors are placed at the articular margin (for single-row or medial row of a double-row construct). The angle of insertion should be approximately 45 degrees to the bone surface to maximize pullout strength. Sutures are passed through the tendon using an antegrade or retrograde suture-passing device, adhering to the algorithm detailed above (e.g., 3 passes for a 1.5 cm tear).
4. Knot Tying and Construct Completion
If margin convergence is required (for L- or U-shaped tears), side-to-side sutures are passed and tied first, working from medial to lateral. Once the tear is reduced to a crescent shape, the sutures from the bone anchors are tied. In a double-row transosseous-equivalent repair, the medial knots are tied, and the suture tails are brought laterally and secured with knotless anchors at the lateral edge of the tuberosity.
POSTOPERATIVE REHABILITATION PROTOCOL
Successful biological healing is heavily dependent on strict adherence to a phased postoperative rehabilitation protocol.
Phase I: Maximum Protection (Weeks 0-6)
- Immobilization: The patient is placed in an abduction sling to remove tension from the superior cuff.
- Range of Motion (ROM): Strictly passive ROM. Pendulum exercises, passive forward elevation, and external rotation within safe limits determined intraoperatively.
- Restrictions: No active motion, no lifting, no sudden movements.
Phase II: Active-Assisted to Active Motion (Weeks 6-12)
- Sling Weaning: The sling is gradually discontinued.
- ROM: Transition from active-assisted to full active ROM. Pulleys and wand exercises are initiated.
- Strengthening: Submaximal isometric exercises for the deltoid and intact cuff muscles.
Phase III: Strengthening and Return to Function (Weeks 12-24)
- Strengthening: Isotonic strengthening using resistance bands and light weights. Focus on scapular stabilizers and restoring the glenohumeral force couples.
- Return to Play/Work: Heavy lifting and overhead sports are generally restricted until 5 to 6 months postoperatively, pending clinical evaluation of strength and functional mechanics.
CONCLUSION
The successful operative management of full-thickness rotator cuff tears requires a synthesis of anatomical knowledge, biomechanical principles, and meticulous surgical execution. By accurately identifying tear patterns—specifically acute and chronic L-shaped configurations—and applying the principles of margin convergence, surgeons can reduce repair tension. Adhering to an evidence-based algorithm for anchor and suture configurations ensures that footprint coverage is optimized, ultimately leading to superior biological healing and excellent clinical outcomes.
