Management of Frostbite and High-Pressure Injection Injuries
Key Takeaway
Frostbite and high-pressure injection injuries represent severe orthopedic emergencies requiring distinct management protocols. Frostbite necessitates rapid, controlled rewarming and delayed surgical intervention to allow tissue demarcation. Conversely, high-pressure injection injuries demand emergent, aggressive surgical decompression and extensive débridement to prevent catastrophic ischemic necrosis and limb loss. This guide details the pathophysiology, classification, and evidence-based surgical strategies for both conditions, providing a framework for optimal limb salvage and functional recovery.
FROSTBITE INJURIES OF THE EXTREMITIES
Frostbite injuries predominantly afflict the appendicular skeleton, with the hands and feet accounting for approximately 90% of all documented cases. The management of these injuries requires a profound understanding of the underlying pathophysiology, which dictates a strictly phased approach to treatment. Unlike thermal burns, which often benefit from early excision and grafting, frostbite demands immense clinical patience, relying on delayed surgical intervention to maximize tissue preservation.
Pathophysiology and Biomechanics of Cold Injury
The tissue damage sustained in frostbite is biphasic, arising from both direct cellular toxicity and secondary microvascular collapse.
- Direct Cellular Death (Freezing Phase): As tissue temperatures plummet, extracellular ice crystals form, creating an osmotic gradient that draws water out of the cells. This leads to intracellular dehydration, protein denaturation, and eventual cell membrane lysis.
- Progressive Ischemia (Vascular Phase): Early in the exposure, profound vascular constriction occurs as a thermoregulatory mechanism to preserve core body temperature. As the tissue thaws, a reperfusion injury ensues. Research by Heggers and Robson has demonstrated a significant elevation of thromboxane A2 and prostaglandin F2-alpha metabolites within frostbite blister fluid. These potent mediators induce severe venular and arterial vasospasm, endothelial damage, and subsequent microvascular thrombosis, culminating in profound tissue anoxia.
In order of increasing severity, the clinical progression of tissue damage manifests as erythema, edema, vesiculation, full-thickness skin necrosis, deep soft-tissue necrosis, and ultimately, osteonecrosis.
Clinical Classification of Frostbite
While traditional paradigms categorized frostbite into four distinct degrees (akin to thermal burns), contemporary orthopedic practice favors a binary classification system of Superficial versus Deep injuries. This simplified designation, as outlined by McAdams et al., has proven vastly superior in guiding treatment algorithms and predicting prognostic outcomes.
Superficial Frostbite:
* First Degree: Characterized by partial skin freezing. Patients present with erythema, edema, and hyperemia. Blisters and necrosis are absent, though occasional skin desquamation may occur 5 to 10 days post-injury.
* Second Degree: Involves full-thickness skin freezing. Clinical hallmarks include substantial edema and the formation of vesicles filled with clear fluid. These blisters eventually desquamate, forming a blackened eschar.
Deep Frostbite:
* Third Degree: Encompasses full-thickness freezing of the skin and underlying subcutaneous tissue. Pathognomonic signs include violaceous or hemorrhagic blisters, skin necrosis, and a distinct blue-gray discoloration of the affected digits.
* Fourth Degree: The most severe form, involving full-thickness freezing of skin, subcutaneous tissue, muscle, tendon, and bone. Edema is paradoxically minimal. The tissue is initially mottled and deep red or cyanotic, eventually progressing to a dry, black, mummified state.
Prehospital and Emergency Resuscitation
Regardless of the depth of the cold injury, the initial treatment algorithm remains uniform.
Surgical Warning: The "Freeze-Thaw-Freeze" Phenomenon
In the prehospital setting, absolutely no attempt should be made to rewarm the affected extremity if there is any risk of refreezing during transport. A freeze-thaw-freeze cycle induces catastrophic, irreversible microvascular thrombosis and exponentially increases the rate of subsequent amputation.
The extremity must be carefully splinted to prevent mechanical trauma to the insensate tissue, and the patient should be promptly transferred to a definitive care facility.
Inpatient Management and Rewarming Protocols
Upon arrival at the hospital, immediate and controlled rewarming is the cornerstone of initial therapy. A widely accepted treatment protocol, originally developed by McCauley and subsequently modified by Su, Lohman, and Gottlieb, dictates the following phased approach:
- Controlled Hydrotherapy: The patient's affected extremity is placed in a Hubbard tank, tub, or whirlpool bath with an initial water temperature of approximately 38ºC. The temperature is meticulously and slowly increased to a maximum of 40ºC. The clinical objective is to restore normal skin temperature within 15 to 20 minutes.
- Systemic Resuscitation: Intravenous fluid resuscitation is critical to support peripheral circulation and mitigate the systemic acidosis that frequently accompanies the return of cold, acidotic blood from the extremities to the central circulation. Intravenous sodium bicarbonate should be administered as dictated by arterial blood gas analysis.
- Medical Adjuncts: Tetanus prophylaxis is mandatory. A regimen of Ibuprofen (12 mg/kg PO per day) is initiated to inhibit the arachidonic acid cascade, specifically targeting the deleterious effects of thromboxane. Appropriate analgesia and prophylactic penicillin are also administered.
Local Wound Care and Blister Management
Following the initial rewarming phase, the extremity must be washed daily, with a Hubbard tank providing an optimal environment for gentle hydrotherapy.
The management of frostbite blisters requires clinical nuance:
* Clear Vesicles: These may be aspirated or carefully débrided if they rupture spontaneously, become excessively tight and painful, or exhibit signs of clinical infection.
* Hemorrhagic Blisters: These indicate deeper structural damage to the subdermal plexus. They should generally be left intact to prevent desiccation of the underlying deep tissues. Topical aloe vera is applied every 6 hours to inhibit local thromboxane production.
Active range-of-motion exercises must be encouraged immediately to prevent joint contractures and tendon adhesions. The extremity should remain elevated and splinted in a functional position between therapy sessions.
Surgical Decision-Making and Delayed Amputation
Clinical Pearl: "Freeze in January, Amputate in July"
In stark contrast to the management of thermal burns, there is absolutely no role for early excision and grafting in the treatment of frostbite. Premature surgical intervention invariably sacrifices viable tissue.
Amputation must be strictly delayed until a definitive line of demarcation becomes clinically evident. This process of auto-amputation and demarcation may require several weeks to several months.
To assist in predicting tissue viability and planning eventual surgical margins, advanced imaging modalities are highly valuable. A triple-phase technetium-99m methylene diphosphonate bone scan, performed at 48 hours and repeated at 5 days post-injury, is the gold standard.
* Superficial Injury: Normal blood and bone pool images.
* Deep Injury: Little or no flow in either blood or bone pool images.
If extensive tissue loss occurs, complex reconstructive coverage may be required, including split-thickness skin grafts, pedicled skin flaps, or free tissue transfer, provided the patient is a candidate for limb salvage.
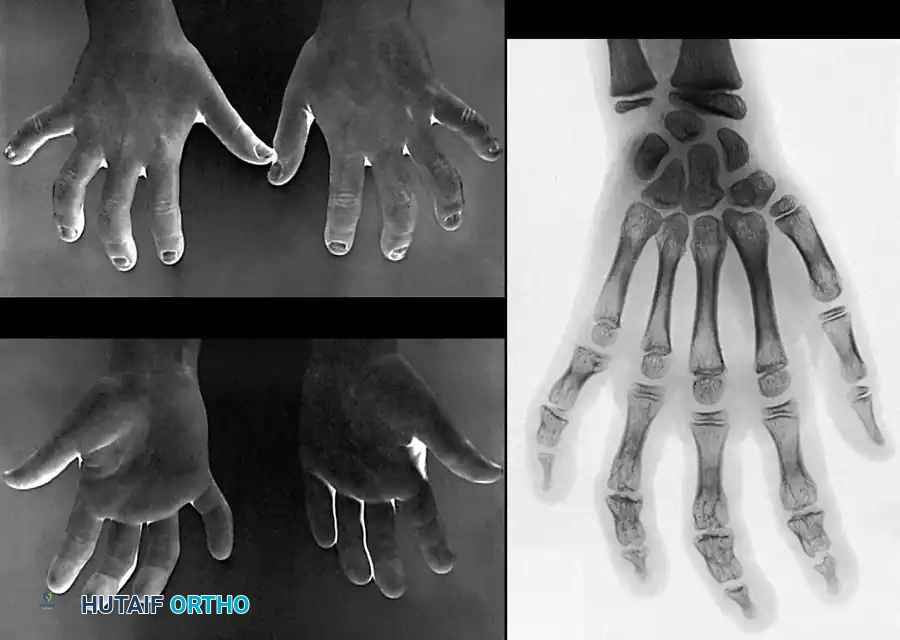
Pediatric Considerations: Physeal Arrest
Children sustaining severe frostbite injuries face the unique and devastating complication of premature physeal arrest. As reported by Bigelow and Ritchie, the cartilaginous growth plates are highly susceptible to cold-induced chondrocyte necrosis.
The index and little fingers are statistically involved more frequently than the middle and ring fingers, while the thumb is typically spared due to its robust vascular supply and protected anatomical position. The disturbance in longitudinal growth develops insidiously over years. Later in life, corrective osteotomies or lengthening procedures may be required to address severe angular deformities; however, these interventions should be delayed as long as possible to allow for maximal skeletal maturation.
HIGH-PRESSURE INJECTION INJURIES OF THE HAND
High-pressure injection injuries represent one of the most deceptive and devastating surgical emergencies in hand surgery. Fluids accidentally injected into the hand through industrial high-pressure equipment include lubricating grease, diesel fuel, brake fluid, dry cleaning solvents (hydrocarbons, methoxypropanol, and dichlorofluoroethane), insecticides, paint, turpentine, cement, molten metal, and liquid plastics.
Mechanism of Injury and Pathophysiology
The nozzle pressure in industrial paint and grease guns can easily exceed 5,000 psi. The vast majority of these injuries occur when a worker attempts to wipe the jet opening of a high-pressure gun with their index fingertip.
The stream of fluid strikes the digit with such immense kinetic energy that it effortlessly penetrates the dermal barrier. Once introduced into the closed compartments of the hand, the fluid spreads rapidly along the planes of least resistance—specifically, the neurovascular bundles, fascial planes, and synovial flexor tendon sheaths.
The resulting tissue destruction is multifactorial:
1. Mechanical Distention: The sheer volume of injected fluid balloons the soft tissues, causing immediate compartment syndrome and profound mechanical ischemia.
2. Chemical Toxicity: The injected substances induce a severe, necrotizing inflammatory reaction. Oil-based substances are particularly hazardous. Paints are generally more toxic than grease, and oil-based paints are significantly more destructive than latex-based variants. Dry cleaning solvents cause rapid, direct cellular necrosis due to extreme local toxicity.
3. Secondary Infection: The introduction of foreign material and necrotic debris creates an optimal nidus for deep space infections.
Clinical Presentation and Evaluation
The initial presentation of a high-pressure injection injury is notoriously benign, often leading to a dangerous delay in treatment. The entry wound may appear as a mere pinpoint puncture, and the patient may report only mild discomfort.
However, within hours, the digit becomes exquisitely tender, tensely swollen, and pale. As the inflammatory cascade accelerates, the patient will develop severe throbbing pain, fever, and leukocytosis.

The image above demonstrates the rapid progression of flexor tenosynovitis with accompanying dorsal cellulitis, presenting just 3 days after the injection of grease into the palmar aspect of the right index finger. The profound swelling and erythema are indicative of the severe chemical irritation and secondary ischemic necrosis occurring within the closed flexor sheath.
Emergent Surgical Management: Step-by-Step Approach
Stark, Ashworth, and Boyes established the foundational doctrine for these injuries: immediate, aggressive incision and drainage under general anesthesia is mandatory. Delaying surgical decompression invariably results in catastrophic tissue loss and amputation.
Surgical Warning: Anesthesia and Tourniquet Use
Digital blocks are strictly contraindicated. The introduction of local anesthetic volume into an already distended, ischemic digit will precipitate immediate vascular collapse. General anesthesia or a proximal brachial plexus block is required. A pneumatic arm tourniquet should be utilized to ensure a bloodless field, but the extremity should not be exsanguinated with an Esmarch bandage, as this may force the injected material further proximally into the forearm.
Surgical Technique:
1. Incision Planning: Bold, extensive incisions are required. For digital involvement, mid-lateral or wide Bruner (zigzag) incisions are utilized to expose the entire flexor tendon sheath. The incisions must extend proximally until completely normal, unadulterated tissue is encountered.
2. Decompression and Exploration: The subcutaneous tissues are carefully elevated. The neurovascular bundles must be identified and protected; they are often encased in the injected material.
3. Flexor Sheath Management: If the material has entered the flexor tendon sheath, the sheath must be opened. The A1 pulley is typically released, while the A2 and A4 pulleys are preserved if possible to prevent tendon bowstringing. However, if the pulleys are heavily infiltrated and necrotic, they must be sacrificed.
4. Radical Débridement: All foreign material, necrotic fat, and devitalized fascia must be meticulously excised. Paint and grease often adhere tenaciously to the paratenon and epineurium, requiring tedious micro-surgical débridement under loupe magnification.
5. Irrigation: Copious pulsatile lavage with normal saline is employed to mechanically flush out remaining particulate matter.
Open Wound Management and Postoperative Protocol
Primary closure of a high-pressure injection injury is absolutely contraindicated. The incisions must be left open to allow for continued drainage, decompression, and serial evaluations.

As demonstrated in the clinical photographs above, the open wound treatment plan requires wide débridement, extensive drainage, and open packing. The wounds are packed loosely with saline-moistened gauze or a non-adherent dressing.
Postoperative Care:
* The hand is immobilized in a bulky, non-compressive dressing and splinted in the intrinsic-plus position (wrist extended 30 degrees, metacarpophalangeal joints flexed 70-90 degrees, interphalangeal joints fully extended).
* Strict elevation is maintained to minimize postoperative edema.
* Broad-spectrum intravenous antibiotics are administered empirically and tailored based on intraoperative cultures.
* The patient is returned to the operating room at 48 to 72 hours for a planned "second-look" débridement. Serial débridements are performed until the wound bed is entirely clean and viable.
* Delayed primary closure, skin grafting, or healing by secondary intention is subsequently employed.
Prognosis and Amputation Rates
Despite aggressive surgical management, the prognosis for high-pressure injection injuries remains guarded. Historically, amputation rates have ranged from 16% to 49%, heavily dependent on the type of fluid injected, the pressure of the injection, and the time elapsed from injury to surgical decompression.
Using the rigorous open wound treatment plan described above, Pinto et al. demonstrated that wide débridement, drainage, open packing, and delayed closure successfully salvaged 84% of affected hands and fingers. However, even in this optimized cohort, 16% of patients (specifically those presenting 3 to 8 days post-injury) ultimately required digital amputation due to irreversible ischemic necrosis and overwhelming infection. Early recognition and emergent surgical intervention remain the most critical determinants of limb salvage.
You Might Also Like


