Fibular Groove Deepening, Superior Retinaculum Repair, and Management of Os Peroneum Syndrome
Key Takeaway
Chronic peroneal tendon subluxation often requires surgical intervention to restore the stabilizing function of the superior peroneal retinaculum and deepen the retromalleolar fibular groove. The Raikin technique utilizes a pants-over-vest retinacular repair combined with osseous deepening to prevent recurrent dislocation. Concurrently, painful os peroneum syndrome may necessitate excision and tenodesis. This guide details the biomechanics, step-by-step surgical approaches, and evidence-based postoperative protocols for these complex lateral ankle pathologies.
INTRODUCTION TO PERONEAL TENDON INSTABILITY AND PATHOLOGY
Disorders of the peroneal tendons encompass a broad spectrum of pathologies, ranging from acute tenosynovitis to chronic tendinopathy, longitudinal split tears, and frank instability. The stability of the peroneus longus and peroneus brevis tendons within the retromalleolar groove is primarily dependent on the integrity of the superior peroneal retinaculum (SPR) and the osseous morphology of the posterior distal fibula.
When conservative measures fail, chronic subluxation or dislocation of the peroneal tendons necessitates surgical intervention. The primary goals of operative management are to restore the anatomical fibro-osseous tunnel, repair or reconstruct the incompetent SPR, and address any concomitant intra-substance tendon pathology. Furthermore, distal pathology involving the peroneus longus as it traverses the cuboid tunnel—specifically Painful Os Peroneum Syndrome (POPS)—requires a nuanced understanding of midfoot biomechanics to execute appropriate surgical debridement and tenodesis.
This comprehensive guide details the Raikin technique for fibular groove deepening and SPR repair, advanced reconstruction options for chronic instability, and the definitive management of POPS.
FIBULAR GROOVE DEEPENING AND REPAIR OF THE SUPERIOR RETINACULUM (RAIKIN)
Although numerous techniques have been described for the treatment of chronic subluxation of the peroneal tendons—including bone block procedures, tissue transfers, and tendon rerouting—anatomical repair of the superior peroneal retinaculum to the posterolateral fibula, combined with a deepening procedure of the posterior fibular sulcus, remains the gold standard. This combined approach reliably restores the anatomical constraints of the retromalleolar space and is highly satisfactory in preventing recurrent dislocation.
Pathoanatomy and Biomechanics
The posterior surface of the distal fibula is highly variable. Cadaveric studies demonstrate that the retromalleolar groove is concave in approximately 82% of individuals, flat in 11%, and convex in 7%. Patients with a flat or convex fibular morphology are biomechanically predisposed to peroneal tendon instability.
The SPR is the primary restraint to peroneal tendon subluxation. It originates from the posterolateral ridge of the distal fibula and inserts onto the lateral calcaneus. In cases of acute trauma (typically forced dorsiflexion with sudden reflex contraction of the peroneal muscles), the SPR can be avulsed from its fibular attachment, often taking a thin fleck of cortical bone with it (the "fleck sign" on radiographs). If left untreated, the SPR heals in a lax, redundant position, creating a false pouch over the lateral malleolus into which the tendons subluxate.
Clinical Pearl: Always evaluate for concomitant longitudinal split tears of the peroneus brevis tendon. The mechanical attrition of the tendon subluxating over the sharp posterolateral ridge of the fibula frequently results in a "salami-slicer" effect, leading to longitudinal attrition and tearing.
Indications and Preoperative Evaluation
Indications for Surgery:
* Chronic, symptomatic subluxation or dislocation of the peroneal tendons.
* Failure of conservative management (immobilization, taping, physical therapy, NSAIDs).
* Concomitant symptomatic peroneal tendon tears requiring debridement and tubularization.
Preoperative Evaluation:
* Clinical Examination: Palpation of the retromalleolar groove may reveal tenderness or a palpable defect in the SPR. The apprehension test (active dorsiflexion and eversion against resistance) often reproduces the subluxation.
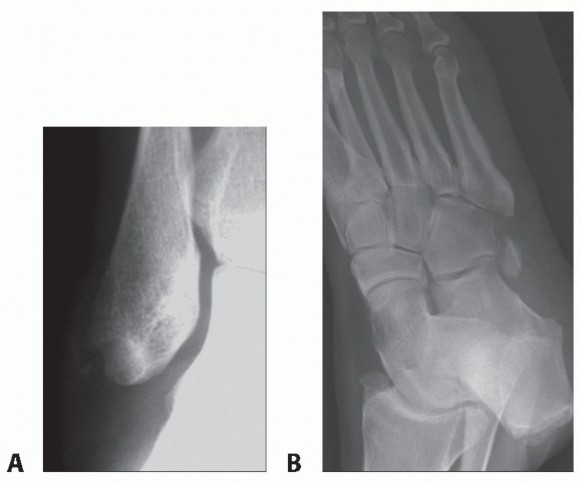
* Imaging: Weight-bearing radiographs of the ankle to rule out fractures and assess for the "fleck sign." Magnetic Resonance Imaging (MRI) is the modality of choice to evaluate the integrity of the SPR, the morphology of the fibular groove, and the presence of intra-substance tendon tears. Ultrasound can be utilized dynamically to visualize real-time subluxation.
Surgical Technique: The Raikin Procedure
The Raikin technique emphasizes a robust, anatomical repair of the SPR utilizing a "pants-over-vest" suture configuration, combined with osseous deepening of the fibular groove to create a secure fibro-osseous sheath.
1. Patient Positioning and Anesthesia
The patient is placed in the lateral decubitus position, or supine with a large bump under the ipsilateral hip to allow internal rotation of the leg, providing unimpeded access to the lateral ankle. A thigh tourniquet is applied. Regional anesthesia (popliteal block) combined with general anesthesia or sedation is preferred.
2. Surgical Approach
* A longitudinal incision is made along the posterior border of the distal fibula, extending from 5 cm proximal to the tip of the lateral malleolus down to the peroneal tubercle of the calcaneus.
* Careful subcutaneous dissection is performed to identify and protect the sural nerve and the lesser saphenous vein, which typically cross the surgical field distally.
3. Identification and Mobilization of the SPR
* The superficial fascia is incised, and the redundant or avulsed SPR is identified.
* The SPR is incised longitudinally, leaving a small cuff of tissue attached to the fibula if present, or elevated directly off the false pouch.
* The peroneus longus and brevis tendons are inspected. Any tenosynovitis is debrided. If a longitudinal split tear of the peroneus brevis is identified, it is debrided and tubularized using a running 4-0 non-absorbable suture.
4. Fibular Groove Deepening
* The periosteum over the posterior fibula is elevated.
* Using a high-speed burr or an osteotome, a cortical window is created, or the posterior fibula is directly decorticated to deepen the sulcus.
* Alternative (Indirect Deepening): A trapdoor of posterior cortical bone is hinged laterally, the underlying cancellous bone is impacted or curetted, and the cortical trapdoor is tamped back into the defect, creating a smooth, deepened concave groove without exposing raw cancellous bone to the tendons.
5. Pants-over-Vest Retinacular Repair
* The peroneal tendons are reduced into the newly deepened fibular groove.
* The SPR is repaired using a pants-over-vest technique. Suture anchors (typically 2.5 mm to 3.0 mm) are placed along the posterolateral ridge of the fibula.
* The sutures are passed through the SPR, drawing the retinaculum under the deep anterior surface of the groove, effectively imbricating the tissue and eliminating the false pouch.
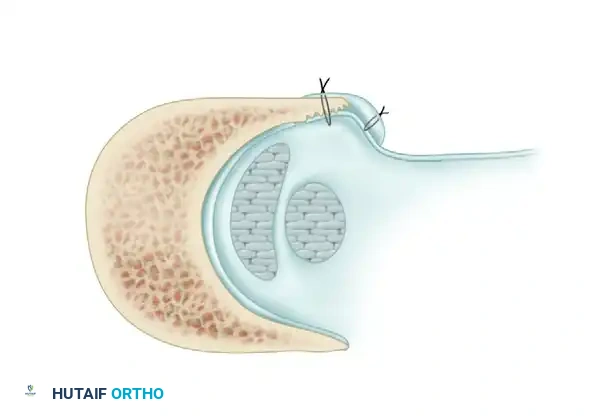
Axial cross-section demonstrating the deepened fibular groove. The peroneus brevis and longus tendons are reduced. Note the superior peroneal retinaculum being drawn tightly against the fibula using the pants-over-vest suture repair, eliminating the lateral false pouch.
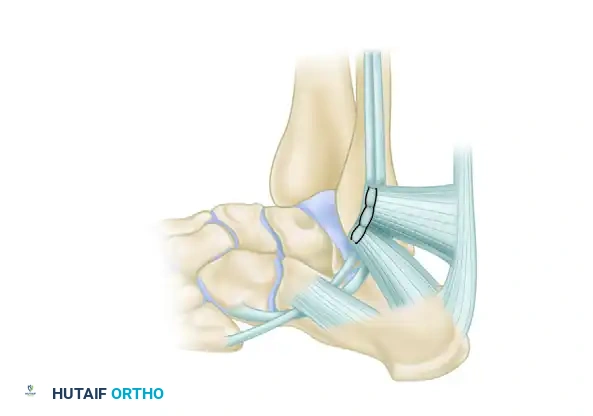
Lateral view of the completed repair. The repaired peroneal retinaculum is securely attached under the deep anterior surface of the groove, restoring the anatomical fibro-osseous sheath.
Surgical Warning: Do not over-tighten the SPR. While eliminating laxity is crucial, excessive tension can lead to stenosis of the fibro-osseous sheath, resulting in postoperative tendon tethering, restricted excursion, and chronic pain. Ensure the tendons glide freely within the deepened groove prior to final knot tying.
Complex Reconstructions and Salvage Options
In cases of severe chronicity, multiple prior failed surgeries, or complete attenuation of the SPR, primary repair may be impossible. In such scenarios, alternative reconstruction options must be employed:
- Achilles Tendon Slip Harvest: A distally based slip of the Achilles tendon (approximately 4-5 mm wide) can be harvested, routed anteriorly, and utilized to reconstruct the superior peroneal retinaculum. The graft is sutured to the posterolateral fibula using suture anchors, creating a robust biological restraint.
- Modified Chrisman-Snook Procedure: In the setting of a chronic, irreparable split tear of the peroneus brevis tendon combined with instability, the anterior half of the split tendon can be utilized for reconstruction. The anterior limb is detached proximally, rerouted through a drill hole in the distal fibula (anterior to posterior), passed over the remaining intact peroneal tendons to act as a restraining sling, and finally attached to the lateral aspect of the calcaneus. This effectively reconstructs both the SPR and the calcaneofibular ligament (CFL).
Postoperative Care and Rehabilitation
Postoperative care following fibular groove deepening and SPR repair is critical to ensure tissue healing while preventing stiffness. The protocol is identical to that of primary repair of the peroneal tendons:
- Weeks 0-2: The patient is placed in a non-weight-bearing short leg cast or rigid splint with the ankle in slight plantarflexion and eversion to minimize tension on the repair.
- Weeks 2-6: Sutures are removed. The patient is transitioned to a controlled ankle motion (CAM) boot. Weight-bearing is gradually advanced as tolerated. Active range of motion (ROM) exercises are initiated, focusing on dorsiflexion and plantarflexion. Inversion is strictly avoided.
- Weeks 6-12: Transition to a supportive lace-up ankle brace. Physical therapy focuses on peroneal strengthening, proprioception, and balance training.
- Months 3-4: Gradual return to sports and high-impact activities, contingent upon the restoration of full strength and pain-free ROM.
Clinical Outcomes and Evidence
The combination of groove deepening and anatomical SPR repair yields excellent clinical results.
* Porter et al. reported on 13 athletes who underwent fibular groove deepening and retinacular reconstruction. The study demonstrated zero cases of recurrent subluxation or dislocation, with all athletes successfully returning to competitive sports by 3 months postoperatively.
* Maffulli et al. described the anatomical reattachment of the retinaculum utilizing soft tissue anchors in 14 patients. All 14 patients returned to their normal daily and athletic activities with no further episodes of tendon subluxation, highlighting the reliability of modern suture anchor fixation in this anatomical region.
DISTAL PERONEAL LONGUS TENDINITIS ASSOCIATED WITH OS PERONEUM: THE PAINFUL OS PERONEUM SYNDROME (POPS)
While retromalleolar pathology is common, the peroneus longus tendon is also susceptible to injury further distally, specifically as it curves around the cuboid. The os peroneum is a sesamoid bone located within the substance of the peroneus longus tendon, typically articulating with the lateral aspect of the cuboid.
Patients occasionally develop localized inflammation, tendinitis, or frank rupture of the peroneus longus tendon at this anatomical fulcrum, a condition known as Painful Os Peroneum Syndrome (POPS).
Anatomy and Pathomechanics
The peroneus longus tendon courses distally from the retromalleolar groove, passes inferior to the peroneal tubercle of the calcaneus, and enters the cuboid tunnel. As it makes a sharp medial turn to traverse the plantar aspect of the midfoot (inserting onto the base of the first metatarsal and medial cuneiform), it is subjected to significant mechanical stress.
The os peroneum acts as a fulcrum to improve the mechanical advantage of the tendon. However, during repetitive loading or acute trauma, the sesamoid can become inflamed, hypertrophic, or fractured. Furthermore, the tendon can undergo attritional tearing or complete rupture as it is compressed between the os peroneum and the cuboid—a "nutcracker" effect.
Clinical Presentation and Diagnosis
Symptoms and Signs:
* Patients present with localized pain, swelling, and reproducible tenderness directly over the plantar-lateral aspect of the midfoot, specifically in the region of the cuboid tunnel.
* Pain is exacerbated by resisted plantarflexion of the first ray or resisted eversion of the foot.
* A palpable mass or thickening may be present at the lateral border of the cuboid.
Imaging Modalities:
* Plain Radiographs: Oblique and lateral views of the foot are essential. The os peroneum may appear sclerotic, fragmented, or enlarged.
* The Migration Sign: A critical radiographic finding is the proximal migration of the os peroneum. If the sesamoid is displaced proximally from its normal position (which is lateral and plantar to the cuboid articulation), it is highly indicative of a complete rupture of the peroneus longus tendon distal to the os peroneum.
* Bone Scans: Technetium-99m bone scans are highly sensitive and helpful in confirming the diagnosis of POPS. Increased focal bony uptake is usually present within the os peroneum.
* MRI: Magnetic Resonance Imaging is the definitive modality for evaluating the soft tissue integrity. It can clearly delineate tenosynovitis, partial-thickness tears, or complete rupture of the peroneus longus tendon, as well as bone marrow edema within the os peroneum and adjacent cuboid.
Clinical Pearl: Do not mistake a bipartite os peroneum for a fracture. A bipartite sesamoid will typically have smooth, well-corticated margins, whereas an acute fracture will exhibit irregular, sharp radiolucent lines. However, both can become symptomatic and lead to POPS.
Conservative Management
Initial treatment for POPS should always be non-operative, focusing on reducing inflammation and offloading the tendon:
* Immobilization: Prolonged immobilization in a short leg walking cast or CAM boot for 4 to 6 weeks to rest the tendon.
* Pharmacotherapy: Oral non-steroidal anti-inflammatory drugs (NSAIDs) to manage acute inflammation.
* Injections: A carefully administered local corticosteroid injection into the tendon sheath (avoiding intra-tendinous injection) in the region of the cuboid tunnel can provide significant diagnostic and therapeutic relief.
* Orthotics: Custom foot orthotics with a lateral wedge or a first ray cutout can alter midfoot biomechanics and reduce tension on the peroneus longus.
Surgical Technique: Os Peroneum Excision and Tenodesis
Chronic, reproducible tenderness in the plantar-lateral aspect of the midfoot despite exhaustive conservative treatment is a strict indication for surgical intervention.
1. Approach and Exploration
* A lateral longitudinal incision is made over the cuboid, following the course of the peroneus longus tendon.
* The inferior peroneal retinaculum is incised, and the tendon sheath is opened.
* The peroneus longus tendon is meticulously inspected for tears, tendinosis, and the condition of the os peroneum.
2. Debridement and Excision
* If the os peroneum is fragmented, enlarged, or associated with severe tendinosis, it is carefully shelled out of the tendon substance using a scalpel.
* The remaining tendon is debrided of all degenerative tissue. If the tendon defect following excision is small, it can be tubularized.
3. Tenodesis (If Indicated)
* If the excision of the os peroneum leaves a massive defect, or if there is a complete rupture of the peroneus longus tendon distal to the cuboid tunnel (evidenced by proximal migration), primary repair is often impossible due to tendon retraction and poor tissue quality.
* In these cases, a tenodesis of the proximal stump of the peroneus longus to the intact peroneus brevis tendon is performed.
* The peroneus longus is tensioned appropriately and sutured side-to-side to the peroneus brevis using multiple interrupted non-absorbable sutures (e.g., #0 or 2-0 FiberWire) just proximal to the base of the fifth metatarsal.
* The distal stump of the peroneus longus within the plantar vault is typically left in situ, as it rarely causes symptoms once tension is removed.
Postoperative Care for POPS Surgery
- Weeks 0-2: Non-weight-bearing in a splint to protect the tenodesis and skin incisions.
- Weeks 2-6: Transition to a CAM boot. Weight-bearing is initiated and advanced. Gentle active ROM is permitted.
- Weeks 6-12: Wean from the boot into a supportive shoe. Physical therapy commences, focusing on evertor strengthening and midfoot stabilization. Full recovery and return to high-impact activities may take 4 to 6 months depending on the extent of the tenodesis and preoperative chronicity.
You Might Also Like