Comprehensive Management of Lower Extremity Nonunions: Fibula, Patella, and Femur

Key Takeaway
Nonunions of the lower extremity present complex biomechanical challenges requiring meticulous surgical strategy. While fibular and patellar nonunions are relatively rare and often managed conservatively or with targeted excision, femoral nonunions demand robust intervention. Modern treatments emphasize reamed exchange intramedullary nailing, locked plating, and biological augmentation. This guide details the indications, operative techniques, and postoperative protocols essential for achieving successful osseous consolidation in complex lower extremity nonunions.
INTRODUCTION TO LOWER EXTREMITY NONUNIONS
The management of lower extremity nonunions requires a profound understanding of local biomechanics, vascularity, and the mechanical environment of the fracture site. While the advent of modern osteosynthesis—particularly locked intramedullary nailing and anatomically contoured locking plates—has drastically reduced the incidence of nonunions, they remain a formidable challenge when they occur. This comprehensive guide delineates the evidence-based protocols for managing nonunions of the fibula, patella, and femur, ranging from conservative observation to complex Ilizarov bone transport and subperiosteal decortication.
MANAGEMENT OF FIBULAR NONUNIONS
Lateral Malleolus Nonunions
Nonunions of the lateral malleolus are exceedingly rare and, when present, rarely necessitate surgical intervention. From a biomechanical standpoint, the lateral malleolus acts as a lateral buttress for the talus. Nonunions without displacement are typically asymptomatic, and a significant proportion will eventually undergo spontaneous osseous consolidation.
Crucially, isolated nonunion of the lateral malleolus has not been correlated with the development of post-traumatic tibiotalar arthritis or other significant long-term functional abnormalities, provided the syndesmosis remains intact and the talus is anatomically reduced within the mortise. Therefore, the presence of a lateral malleolar nonunion does not inherently compromise the final clinical outcome of an ankle fracture.
Fibular Shaft Nonunions in Pediatric Patients
The pediatric fibular shaft presents unique developmental challenges. A persistent defect in the fibular shaft in young children—whether iatrogenic (e.g., following resection for tumor or harvest for a Grice subtalar extra-articular arthrodesis) or congenital (e.g., congenital pseudarthrosis of the fibula)—often results in the proximal migration of the distal fibula. As skeletal growth progresses, this upward migration inevitably leads to a progressive valgus deformity of the ankle.
Surgical Pearl: To prevent valgus deformity in pediatric patients with congenital pseudarthrosis of the fibula, the Langenskiöld procedure is highly recommended. This operation creates a synostosis between the distal tibial and fibular metaphyses, effectively tethering the lateral malleolus and preventing its proximal migration.
For any persistent defect in the fibular shaft following segmental resection in a young child, prompt autogenous bone grafting is recommended. Restoring the normal mechanical thrust through the fibula stimulates the proximal fibular physis, preventing deformity or gradually correcting mild-to-moderate existing deformities. In older children presenting with an established valgus deformity of the ankle, a corrective osteotomy of the distal tibial and fibular metaphyses is indicated. If significant remaining growth is anticipated, the deformity should be intentionally overcorrected to accommodate future remodeling.
Fibular Shaft Nonunions in Adults
In the adult population, nonunion of the fibular shaft is rare. Asymptomatic or low-demand patients are best managed with benign neglect and observation. However, symptomatic nonunions require intervention.
Diagnostic Pitfall: Before committing to surgery for a fibular nonunion, confirm that the nonunion is the actual source of the patient's pain. A diagnostic injection of bupivacaine (Marcaine) directly into the nonunion site under fluoroscopic guidance is an invaluable tool. Complete temporary pain relief confirms the nonunion as the pain generator.
Surgical options for symptomatic adult fibular nonunions include:
1. Internal Fixation and Bone Grafting: Utilizing a 3.5mm dynamic compression plate (DCP) or locking compression plate (LCP) with autogenous iliac crest bone graft.
2. Partial Fibulectomy: Resection of 2 to 5 cm of the fibula centered over the nonunion site to eliminate painful micro-motion and impingement.
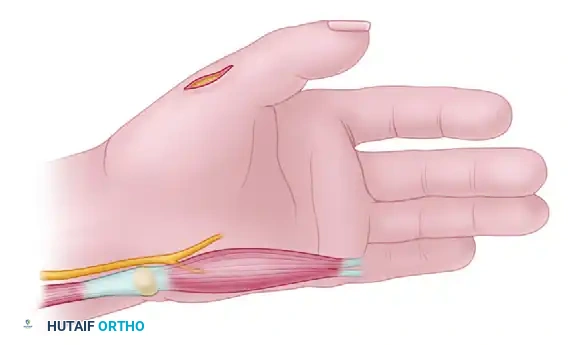
Surgical Technique 59-11: Partial Fibulectomy for Nonunion
- Positioning and Approach: Place the patient supine with a bump under the ipsilateral hip. Utilize a direct lateral approach over the palpable fibular nonunion.
- Exposure: Incise the fascia and carefully retract the peroneus longus and brevis anteriorly, protecting the superficial peroneal nerve.
- Resection: Open the fibula directly at the nonunion site. Using an oscillating saw, resect 2.0 to 2.5 cm of bone from the fibular shaft, ensuring the cuts are made in healthy, bleeding bone.
- Decompression: Perform a prophylactic lateral compartment fasciotomy if significant postoperative swelling is anticipated.
- Closure: Irrigate copiously and close the wound in a routine, layered fashion.
Postoperative Care:
Ankle and knee range of motion (ROM) exercises are initiated immediately post-surgery. Ambulation is permitted, and full weight-bearing is strongly encouraged in a short-leg, prefabricated walking boot to stimulate adjacent tibial hypertrophy and maintain functional mobility.
TIBIOTALAR AND FIBULAR INTRAMEDULLARY FIXATION PRINCIPLES
In cases where fibular nonunions are associated with tibial pathology, intramedullary nailing may be required. Malunions and nonunions in the highlighted area of the tibia can often be treated with reamed intramedullary nailing, which provides both mechanical stability and biological stimulation via the reaming products.

Internal Fixation Using Russell-Taylor Interlocking Nail
- Preparation: Prepare and drape the limb free on a radiolucent operative table to allow unimpeded fluoroscopic access in both anteroposterior (AP) and lateral planes.
- Incision and Entry: If the tibial medullary canal remains in continuity, the fracture site may not require formal opening. Open the entry portal in the proximal tibia (typically via a medial parapatellar or transpatellar tendon approach) using a curved awl.
- Guidewire Placement: Pass a ball-tipped guidewire down to the nonunion site. The proximal tibial shaft can be cautiously reamed to 10 mm to facilitate instrument passage.
- Crossing the Pseudarthrosis: Drive the pseudarthrosis chisel (from the Russell-Taylor interlocking nail set) across the dense fibrous tissue of the nonunion.
- Warning: This step must be performed under continuous AP and lateral radiographic control to prevent the chisel from exiting the tibial canal and causing an iatrogenic cortical breach.
- Distal Canal Access: After successfully opening the nonunion site with the chisel, advance the guidewire into the distal tibial canal from the proximal entry portal.
- Reaming and Insertion: Sequentially ream the tibia to 1.0 mm to 1.5 mm larger than the anticipated nail diameter. Insert the intramedullary nail according to standard technique.
- Locking Strategy: Lock the nail in a dynamic mode. This involves inserting either proximal or distal screws (most commonly distal screws in the smaller fragment), but not both. This allows for axial micromotion and compression at the nonunion site during weight-bearing.
- Implant Selection: Utilize the largest diameter nail that is practically feasible. Nonunions exhibit prolonged healing times, subjecting the implant to extended cyclic loading. A larger nail significantly reduces the risk of fatigue failure compared to standard fresh fracture fixation.
MANAGEMENT OF PATELLAR NONUNIONS
Nonunions of the patella are exceptionally rare, largely due to the robust vascular supply from the genicular anastomosis and the compressive forces generated during knee extension.
The management algorithm is dictated by the morphology of the original fracture and the current state of the articular surface:
* Comminuted Fractures: If a fresh fracture is highly comminuted, primary partial or total excision of the fragments eliminates the possibility of nonunion.
* Non-Comminuted Fractures: Standard internal fixation (e.g., tension band wiring) almost universally results in union.
When a nonunion does occur, the treatment depends on fragment position and articular congruity. If the fragments are in good anatomical position, a stable fibrous union may be entirely compatible with satisfactory, pain-free function. The severity of subsequent patellofemoral arthritic changes is directly proportional to the irregularity and step-off of the articular surface. Conversely, if the fragments are widely separated and the extensor mechanism is compromised, partial or complete excision of the patella, combined with meticulous repair of the extensor retinaculum, is indicated.
MANAGEMENT OF FEMORAL NONUNIONS
Femoral nonunions are significantly less common today than in previous decades. With the widespread adoption of modern, anatomically contoured interlocking femoral nails, primary healing rates now approach 99%. However, when nonunions do occur, late treatment—especially after fragments have migrated, shortened, or deformed significantly—is extremely technically demanding.
The treatment of almost all femoral nonunions in adults is operative. The strategy depends on the existing hardware:
* Existing Plate Fixation: If a nonunion occurs with an intact, mechanically effective plate in place, the treatment of choice is autogenous bone grafting (typically iliac crest) combined with a period of protected weight-bearing.
* Existing Statically Locked Nail: If a nonunion occurs with a statically locked intramedullary nail, the surgeon may choose bone grafting in situ or dynamization of the nail (removal of the interlocking screws furthest from the fracture to allow axial compression).
Clinical Pearl: Exchange nailing is the gold standard alternative for a persistent hypertrophic nonunion. This involves removing the existing nail, reaming the canal to a larger diameter (stimulating endosteal bleeding and providing autogenous graft), and inserting the next larger diameter nail. Most nails inserted for nonunions should be locked dynamically, or statically if rotational instability is a concern.
Supracondylar Femoral Nonunions
The supracondylar area is anatomically defined as the region extending 9 cm proximally from the most distal portion of the femur. Union in this metaphyseal region can be notoriously difficult to obtain due to poor bone stock, wide medullary canals, and the deforming forces of the gastrocnemius. According to Graves et al., the worldwide incidence of supracondylar femoral fracture nonunion is less than 9%.
A short supracondylar fragment can be managed via one of five primary methods:
- Plating and Grafting: For recent nonunions, the fragments can be fixed with a 95-degree blade plate, a buttress plate, or a dynamic condylar screw, supplemented with copious iliac crest autograft. While double plate fixation through an anterior Henry approach was historically recommended, modern laterally based distal femoral locking plates (LCP) are now the standard of care, providing fixed-angle stability.
- Short Interlocking Nails: Intraarticular placement of a short retrograde interlocking nail has been utilized; however, these have largely been superseded by longer retrograde nails that provide superior working length and initial fracture stability. Biomechanical studies show no advantage to placing a second proximal locking screw in a long nail.
- External Fixation / Locked Plating for Osteoporosis: When fragments are too osteoporotic for standard plating, external fixation can restore apposition. This often requires crossing the knee joint with the frame for stability, which unfortunately frustrates joint rehabilitation. Today, locked plating techniques are the preferred standard of care for osteoporotic metaphyseal bone.
- Knee-Spanning Intramedullary Nailing: In cases of severe comminution or an exceptionally small distal fragment, fixation can be achieved using a long intramedullary nail traversing the femur, the knee joint, and the proximal tibia, combined with autogenous bone grafting.
- Arthrodesis or Arthroplasty: If the knee joint is irreparably damaged, preventing painless weight-bearing and useful motion, knee arthrodesis (fusion) is performed concurrently with nonunion grafting. Alternatively, in older or lower-demand patients, a total knee replacement utilizing a hinged tumor prosthesis is an excellent salvage option.

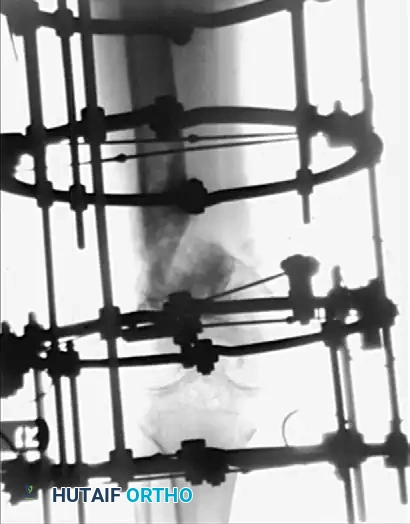
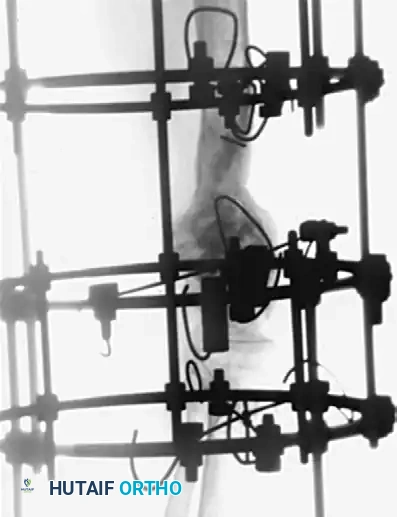


Figure 59-23: (A) Deformity and nonunion 7 years after a supracondylar femoral fracture in a 35-year-old woman; the knee joint is ankylosed. (B and C) Application of an Ilizarov external fixator for the correction of length and offset deformity. (D and E) Successful union achieved at 10 months.
Femoral Shaft Nonunions
The vast majority of femoral shaft nonunions can be treated successfully with intramedullary nails. Recognized risk factors for nonunion include open fractures, delayed weight-bearing, and tobacco use.
A nonunion in continuity with existing intramedullary fixation should be treated by reamed exchange nailing. The surgeon must use, at minimum, the next larger nail size (the larger the better to maximize mechanical stability), locked either dynamically or statically. A multicenter randomized clinical trial by the Canadian Orthopaedic Trauma Society demonstrated a significantly higher rate of nonunion following unreamed intramedullary nailing compared to reamed nailing. Reaming is essential as it deposits osteogenic reamings directly into the fracture site.
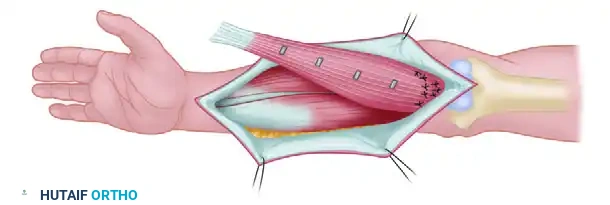
Judet and Patel Subperiosteal Decortication
For recalcitrant cases, Judet and Patel described an elegant biological technique: subperiosteal decortication. This involves elevating osteoperiosteal flaps (bone chips attached to the periosteum) around the nonunion site, followed by rigid internal fixation (plates or IM nails) with compression. In their series of 195 femoral nonunions, union failed in only 4.6% of cases.
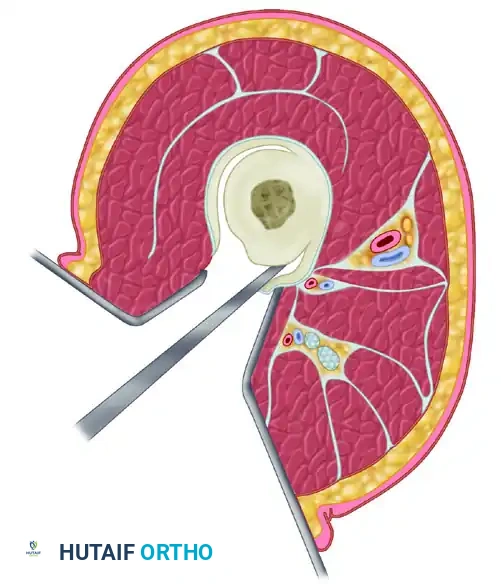
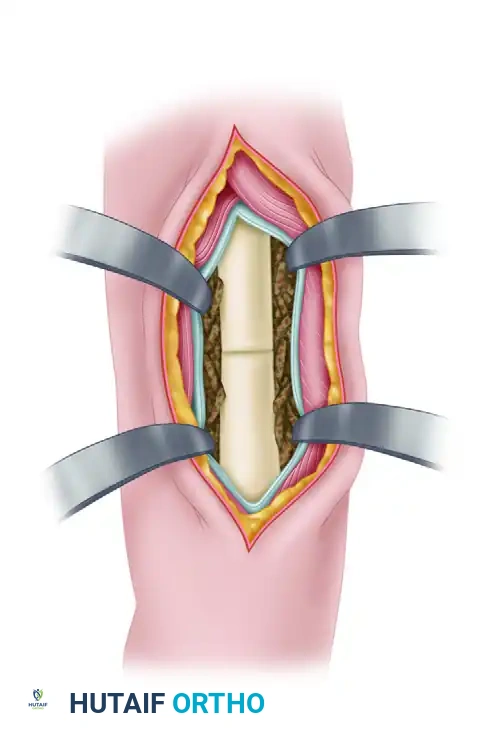


Figure 59-24: Judet and Patel subperiosteal decortication. (A) Exposure of the femur, demonstrating autogenous bone chips elevated subperiosteally. (B) Cross-section illustrating the separation of cortical bone and periosteum from the femoral shaft.
Management of Large Femoral Defects
Massive osseous defects of the femur (e.g., following high-energy trauma or gunshot wounds) can be managed via interlocking intramedullary nailing combined with massive medullary autogenous bone grafting. Protected weight-bearing is strictly enforced until the graft has hypertrophied sufficiently. Alternatively, Johnson and Urist reported excellent results utilizing human bone morphogenetic protein (BMP) allograft for reconstruction.




Figure 59-25: (A and B) A massive femoral defect in a 16-year-old boy following a type IIIB hunting accident injury. (C and D) Radiographs at six months demonstrating consolidation after medullary bone grafting and fixation with a static-locked, unreamed intramedullary nail.
For critical-sized defects or septic nonunions, the Ilizarov external fixator with internal bone
Associated Surgical & Radiographic Imaging



You Might Also Like