Extensor Digitorum Brevis Transfer for Crossover Toe Deformity: The Haddad Technique
Key Takeaway
The extensor digitorum brevis (EDB) transfer is a powerful dynamic reconstruction technique for correcting crossover toe deformity. By rerouting the EDB tendon beneath the deep transverse metatarsal ligament, surgeons can restore the plantar-flexion and lateralizing forces lost due to plantar plate and lateral collateral ligament insufficiency. This guide details the Haddad technique, encompassing biomechanical principles, step-by-step surgical execution, and postoperative protocols to optimize patient outcomes.
Introduction to Crossover Toe Deformity and Dynamic Reconstruction
Crossover toe deformity is a complex, multiplanar pathology most commonly affecting the second metatarsophalangeal (MTP) joint. It is characterized by dorsal and medial subluxation of the lesser toe, frequently resulting in the second digit overriding the hallux. This debilitating condition is driven by progressive attenuation and ultimate failure of the plantar plate and the lateral collateral ligament (LCL) complex, often exacerbated by a long second metatarsal or severe hallux valgus.
While static repairs (such as direct plantar plate repair) and bony procedures (such as the Weil osteotomy) are mainstays of treatment, dynamic soft-tissue reconstruction is often required to restore the intricate biomechanical balance of the MTP joint. The Extensor Digitorum Brevis (EDB) Transfer, popularized by Haddad, is a highly effective dynamic tenodesis procedure. By harvesting the EDB tendon and rerouting it beneath the deep transverse metatarsal ligament (DTML), the surgeon converts a dorsal extensor force into a plantar-flexing and lateralizing vector, directly counteracting the deforming forces of the crossover toe.
This comprehensive guide details the indications, biomechanical rationale, and step-by-step surgical execution of the EDB transfer for crossover toe deformity, providing orthopedic surgeons with a masterclass in this advanced forefoot reconstruction.
Biomechanical Rationale and Pathoanatomy
To successfully execute the EDB transfer, the surgeon must possess a profound understanding of lesser MTP joint biomechanics. The stability of the MTP joint relies on a delicate interplay between static stabilizers (the plantar plate, collateral ligaments, and joint capsule) and dynamic stabilizers (the intrinsic and extrinsic musculature).
- The Pathologic Cascade: Crossover toe deformity typically begins with chronic synovitis leading to LCL insufficiency, allowing medial deviation of the digit. Subsequent or concurrent failure of the plantar plate removes the primary restraint to dorsal translation. The extensor digitorum longus (EDL) and lumbricals gain a mechanical advantage, pulling the toe into fixed dorsal and medial subluxation.
- The Role of the EDB: In its native anatomical position, the EDB assists the EDL in extending the toes. In the setting of a crossover toe, this dorsal vector exacerbates the deformity.
- Vector Conversion via Transfer: The Haddad technique elegantly solves this imbalance. By detaching the EDB proximally, routing it plantar to the DTML, and securing it, the tendon's line of pull is fundamentally altered. The DTML acts as a pulley. When the EDB muscle contracts, it now exerts a plantar-directed and laterally-directed force on the proximal phalanx, dynamically resisting dorsal and medial subluxation.
💡 Clinical Pearl: The Rotary Force Vector
A critical, often overlooked step in this procedure is the management of the distal EDB stump. If left unaddressed, the native insertion can impart an unwanted rotary force on the toe. Suturing the distal EDB stump to the plantar-lateral base of the proximal phalanx neutralizes this rotational vector, ensuring pure sagittal and coronal plane correction.
Preoperative Evaluation and Indications
Clinical Assessment
Patients typically present with pain localized to the plantar aspect of the second MTP joint, accompanied by the visible crossover deformity. A thorough clinical examination must include:
* The Lachman Test of the MTP Joint: Assesses dorsal instability and plantar plate integrity.
* Deformity Flexibility: Differentiating between a flexible, semi-rigid, and rigid deformity dictates the necessity of concomitant bony procedures (e.g., Weil osteotomy).
* Hallux Valgus Evaluation: Severe hallux valgus must be corrected concurrently; otherwise, the transferred EDB will fail against the mechanical pressure of the overriding hallux.
Indications
- Flexible or semi-rigid crossover toe deformity (typically the second toe).
- Chronic plantar plate insufficiency with medial and dorsal MTP joint subluxation.
- Failed conservative management (taping, orthotics, NSAIDs).
Contraindications
- Rigid, fixed deformities without planned concomitant bony shortening (Weil osteotomy).
- Severe degenerative joint disease of the MTP joint (better served by arthroplasty or arthrodesis).
- Inadequate or absent EDB muscle belly/tendon.
- Active local infection or severe peripheral vascular disease.
Surgical Technique: Step-by-Step Execution
The following technique describes the Haddad modification of the EDB transfer, emphasizing meticulous soft-tissue handling and precise vector recreation.
1. Patient Positioning and Anesthesia
The patient is placed in the supine position on the operating table. A regional ankle block or popliteal sciatic nerve block is administered, supplemented by intravenous sedation or general anesthesia based on patient preference and comorbidities. A calf or thigh tourniquet is applied to ensure a bloodless surgical field, which is paramount for identifying delicate anatomical structures such as the digital nerves and the DTML.
2. Surgical Approach and Neurological Protection
Begin with a dorsal longitudinal incision.
* Initiate the incision just distal to the proximal interphalangeal (PIP) joint.
* Carry the incision proximally with a gentle curve at the level of the MTP joint, following the lateral border of the metatarsal shaft.
* Extend the incision approximately 5 cm proximal to the MTP joint to allow adequate exposure of the EDB musculotendinous junction.
⚠️ Surgical Warning: Nerve Preservation
Immediately upon deepening the incision through the subcutaneous tissues, identify the dorsal digital nerves. These must be meticulously dissected free and retracted with vessel loops. Iatrogenic injury or aggressive retraction will result in painful postoperative neuromas or permanent sensory deficits.
3. Tendon Harvest and Proximal Sectioning
Identify the EDB tendon and trace it proximally to its musculotendinous junction. The EDB lies lateral to the EDL tendon.
* Once the musculotendinous junction is clearly visualized, place two stay sutures (e.g., 3-0 Ethibond or similar non-absorbable braided suture) using a Krackow or whipstitch technique on either side of the proposed sectioning site.
* Section the tendon proximally, near the musculotendinous junction, ensuring maximum tendon length is preserved for the transfer.
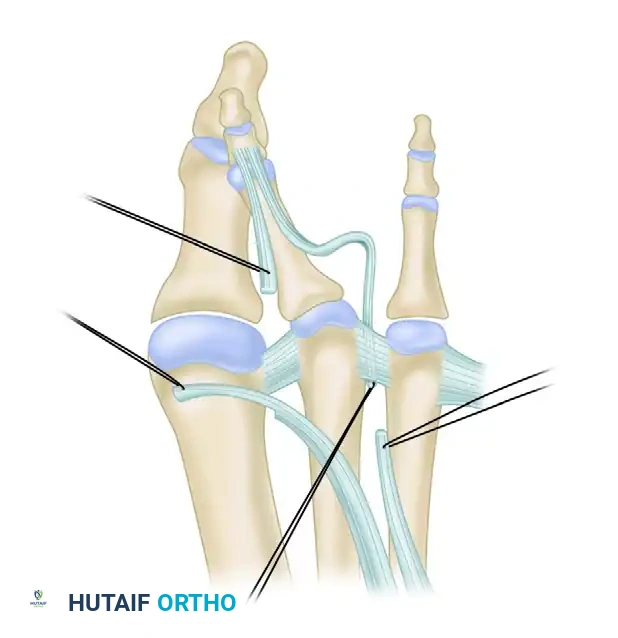
Figure 83-10A: Identification of the extensor digitorum brevis. The tendon is traced to the musculotendinous junction proximally, stay sutures are placed, and the tendon is sectioned to maximize length for the transfer.
4. Distal Preparation and Joint Release
Following proximal sectioning, direct attention to the distal aspect of the EDB tendon.
* Identify the EDB tendon distally to its insertion.
* Carefully free the tendon from the capsular aponeurosis (the extensor hood) progressing proximally toward the transverse metatarsal ligament.
* To correct the fixed deformity, perform a sequential soft-tissue release. Completely section the medial collateral ligament (MCL) and the dorsal capsule of the MTP joint.
⚠️ Surgical Pitfall: Plantar Plate Violation
When sectioning the MCL and medial capsule, the surgeon must maintain strict superficial dissection. Deep, aggressive medial sectioning risks violating the medial aspect of the plantar plate, which can destabilize the joint further and compromise the reconstructive effort.
5. Plantar Plate Mobilization
To assist with postoperative stability, the volar (plantar) plate must be addressed.
* Utilize a McClamary elevator or a small curved gouge to carefully strip the volar plate at its proximal origin on the metatarsal neck.
* This controlled mobilization allows the plantar plate to shift and scar down to the metatarsal slightly proximal to its current insertion, effectively tensioning the static restraint and assisting with long-term sagittal stability.
6. Lateral Collateral Ligament (LCL) Reconstruction
The LCL is invariably attenuated or ruptured in a crossover toe deformity.
* Examine the LCL complex. If the tissue is severely attenuated, excise the redundant, non-functional tissue.
* Place permanent sutures (e.g., 2-0 or 3-0 non-absorbable) in a figure-of-eight configuration to repair and imbricate the LCL.
* Do not tie these sutures yet. They will be tied later after the joint is reduced and pinned, to avoid pulling the repair apart under tension.
7. Management of Concomitant Hammer Toe Deformity
If a rigid hammer toe deformity is present at the PIP joint, it must be addressed to ensure a straight digit.
* Perform a minimal resection arthroplasty of the distal aspect of the proximal phalanx and the proximal aspect of the middle phalanx (condylectomy).
* This stimulates a fibrous union or formal PIP joint fusion, eliminating the deforming forces at the PIP level.
8. Distal EDB Stump Management
As previously noted, the native insertion of the EDB can create an unwanted rotational vector.
* Suture the distal stump of the sectioned EDB tendon directly to the plantar-lateral base of the proximal phalanx using a permanent suture.
* This step neutralizes rotary forces on the toe, ensuring the digit remains rectus in the coronal plane postoperatively.
9. Tendon Routing and Dynamic Vector Creation
This is the most critical biomechanical step of the procedure. The EDB must be routed beneath the deep transverse metatarsal ligament (DTML) to convert its function.
* Identify the DTML located between the second and third metatarsal heads.
* Crucial Identification: It is imperative not to mistake the more superficial dorsal fascia for the DTML. The dorsal fascia lacks the structural integrity required to act as a pulley and will fail under load.
* Use a lamina spreader between the metatarsal heads to place tension on the DTML, clearly defining its borders.
* Pass a 90-degree right-angle clamp from proximal to distal, passing deep (plantar) to the DTML.
* Grasp the previously placed stay sutures on the proximal EDB tendon and pull the tendon from distal to proximal, routing it deep to the DTML.
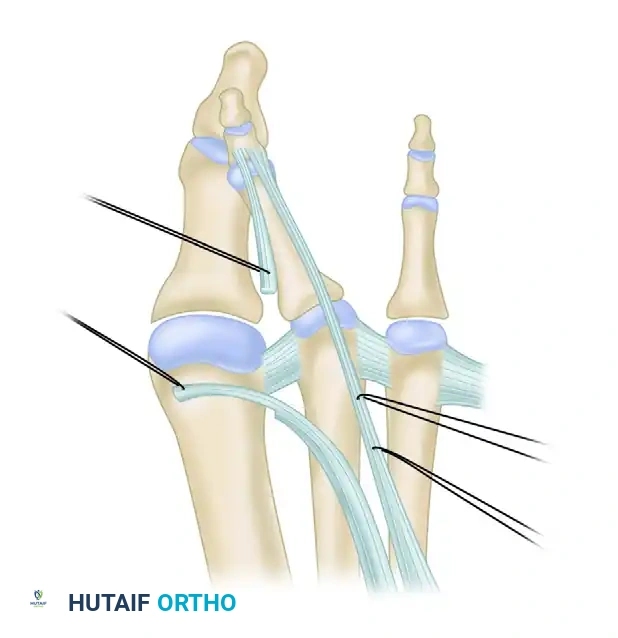
Figure 83-10B: The extensor digitorum brevis tendon is passed from distal to proximal, deep to the deep transverse metatarsal ligament, utilizing the ligament as a biomechanical pulley.
10. Joint Reduction and Kirschner Wire Fixation
With the tendon routed, the joint must be stabilized to protect the soft-tissue reconstructions during the initial healing phase.
* Manually reduce the MTP joint.
* Tie the previously placed figure-of-eight sutures to complete the LCL repair.
* Drive a 0.062-inch Kirschner wire (K-wire) antegrade through the distal tip of the toe, across the PIP and MTP joints, and into the metatarsal shaft.
* Positioning: The K-wire must hold the MTP joint in slight valgus (lateral deviation) and slight plantar flexion. This specific positioning takes all tension off the LCL repair and the newly transferred EDB tendon.
11. Tendon Anastomosis and Final Tensioning
With the joint securely pinned in the corrected position, the tendon transfer is finalized.
* Reflect the routed EDB tendon back upon itself or secure it to the adjacent lateral soft tissues/periosteum, depending on length and reach.
* Tie the tendon transfer end-to-end under physiologic tension, completing the anastomosis. The tension should be sufficient to hold the toe in the corrected position if the K-wire were to be removed, but not so tight as to cause a rigid plantarflexion contracture.
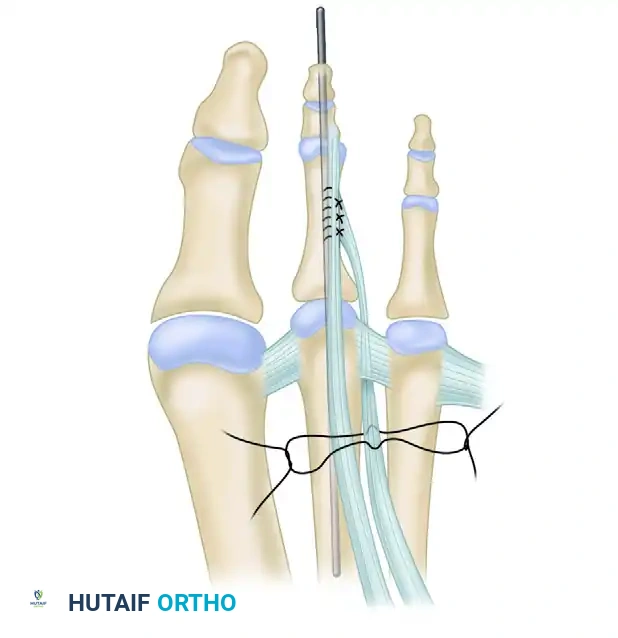
Figure 83-10C: Final construct. The lateral collateral ligament is repaired, the MTP joint is pinned in slight valgus and plantar flexion with a 0.062-inch K-wire, and the EDB tendon transfer is tied end-to-end to complete the dynamic reconstruction.
12. Hemostasis and Layered Closure
- Deflate the tourniquet prior to closure.
- Meticulously evaluate the vascularity of the digit. Capillary refill should return promptly. If the toe is ischemic, the K-wire may be holding the joint in excessive distraction or the deformity correction may be stretching the neurovascular bundles. Adjust the pin if necessary.
- Once vascularity is confirmed, irrigate the wound copiously.
- Perform a layered closure. Use 4-0 Monocryl (poliglecaprone) for the deep subcutaneous tissues to eliminate dead space, and 4-0 Nylon or Prolene for the skin.
Postoperative Care and Rehabilitation Protocol
The success of the EDB transfer relies heavily on strict adherence to postoperative protocols to allow the tendon transfer and ligament repairs to heal without stretching out.
Weeks 0 to 6: Protection Phase
- Weight-Bearing: The patient is placed in a rigid postoperative shoe or a controlled ankle motion (CAM) boot. Weight-bearing is strictly limited to the heel to avoid bending or breaking the K-wire and to protect the MTP joint.
- Pin Care: The exposed tip of the K-wire is protected with a pin cap. The patient is instructed on daily pin site care to prevent superficial infections.
- Immobilization: The 0.062-inch K-wire remains in place for a full 6 weeks to ensure adequate scarring of the LCL repair and the EDB tenodesis.
Weeks 6 to 12: Mobilization and Taping Phase
- Pin Removal: At the 6-week mark, the K-wire is removed in the clinic.
- Taping: Immediately following pin removal, the toe must be taped into slight valgus and plantar flexion. This taping protocol is maintained continuously for an additional 6 weeks. Taping prevents sudden dorsal or medial stress on the newly healed tissues.
- Physical Therapy: Gentle active and passive range of motion (ROM) exercises of the MTP joint are initiated. The focus is on restoring plantar flexion strength and preventing dorsal contracture.
- Footwear: The patient may transition to a stiff-soled, wide-toe-box shoe.
Months 3 and Beyond: Return to Function
- Taping is gradually weaned.
- Patients may return to normal footwear as tolerated, though high heels and narrow toe boxes should be permanently avoided to prevent recurrence.
- Full athletic activities are typically resumed between 4 to 6 months postoperatively, depending on the recovery of intrinsic foot strength and resolution of swelling.
Complications and Pitfalls
While highly effective, the EDB transfer is technically demanding. Surgeons must be prepared to navigate potential complications:
- Recurrence of Deformity: The most common cause of recurrence is failure to address a concomitant long second metatarsal. If the metatarsal is excessively long, the soft-tissue transfer will eventually stretch out. A Weil osteotomy should be performed concurrently in these cases.
- Floating Toe Deformity: Over-tensioning the EDB transfer or excessive stripping of the plantar plate can result in a toe that fails to purchase the ground during the stance phase of gait. Precise tensioning with the joint pinned in neutral to slight plantar flexion is critical.
- Neurovascular Injury: Aggressive dissection can injure the dorsal digital nerves, leading to complex regional pain syndrome (CRPS) or painful neuromas. Ischemia can occur if the deformity correction places excessive longitudinal traction on the digital arteries; always check capillary refill after tourniquet deflation.
- MTP Joint Stiffness: Prolonged K-wire fixation (beyond 6 weeks) or failure to initiate aggressive ROM therapy after pin removal can lead to a rigid, non-functional MTP joint. Patient compliance with the postoperative therapy protocol is mandatory.
By adhering to the meticulous surgical steps and biomechanical principles outlined in this guide, orthopedic surgeons can reliably utilize the Extensor Digitorum Brevis transfer to restore function, alleviate pain, and correct the complex pathoanatomy of the crossover toe deformity.
📚 Medical References
You Might Also Like
