Principles and Techniques of Wrist Arthroscopy: Equipment, Positioning, and Indications
Key Takeaway
Wrist arthroscopy has evolved into an indispensable diagnostic and therapeutic modality in hand and upper extremity surgery. This comprehensive guide details the essential equipment, precise patient positioning, and broad surgical indications required for successful outcomes. From managing triangular fibrocartilage complex (TFCC) tears and carpal instability to assisting in the reduction of intraarticular distal radius fractures, mastering these foundational principles is critical for the modern orthopedic surgeon.
INTRODUCTION TO WRIST ARTHROSCOPY
Over the past three decades, wrist arthroscopy has transitioned from a purely diagnostic tool to a highly sophisticated therapeutic modality. It is now considered the gold standard for evaluating intraarticular pathology of the radiocarpal and midcarpal joints. The complex, multi-articulated nature of the wrist demands meticulous attention to detail regarding equipment selection, patient positioning, and portal placement. Mastery of these foundational elements is paramount for the orthopedic surgeon to safely navigate the tight confines of the carpus, minimize iatrogenic chondral injury, and optimize clinical outcomes.
SURGICAL INDICATIONS
The applications for wrist arthroscopy have expanded exponentially, driven by advancements in small-joint instrumentation and a deeper biomechanical understanding of carpal kinematics. The indications can be broadly categorized into soft tissue repairs, fracture management, bone excision procedures, and the treatment of chondral or inflammatory conditions.
Triangular Fibrocartilage Complex (TFCC) Pathology
Arthroscopy remains the definitive modality for the diagnosis and treatment of TFCC lesions.
* Débridement: Indicated for central, avascular tears (Palmer Type 1A) where the mechanical symptoms of catching and clicking predominate without concomitant distal radioulnar joint (DRUJ) instability.
* Repair: Peripheral tears (Palmer Type 1B, 1C, 1D) occurring in the vascularized zone are amenable to arthroscopic or arthroscopically assisted open repair techniques (e.g., outside-in, inside-out, or all-inside capsular repairs).
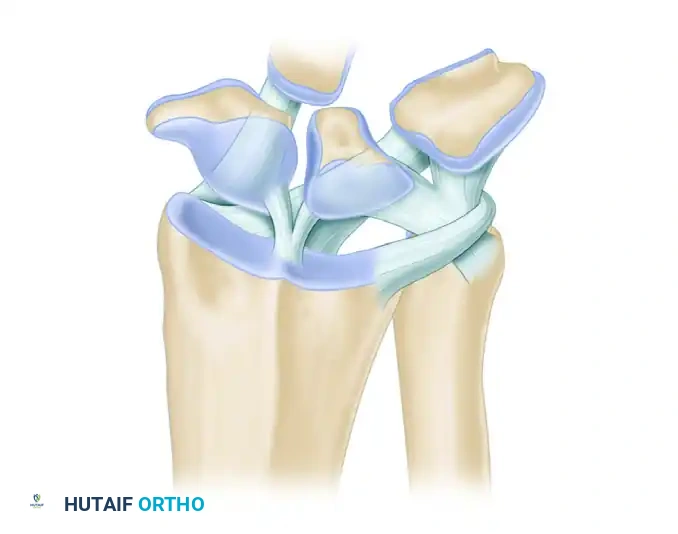
Carpal Instability
Arthroscopy provides dynamic, magnified visualization of the intrinsic carpal ligaments, far surpassing the sensitivity of magnetic resonance imaging (MRI) or fluoroscopic arthrography.
* Scapholunate (SL) and Lunotriquetral (LT) Tears: Arthroscopy allows for the precise grading of interosseous ligament injuries (Geissler classification).
* Therapeutic Interventions: Management ranges from simple arthroscopic débridement and thermal shrinkage for partial tears (Geissler Grades I-II) to arthroscopically assisted percutaneous pinning or open repair for complete, unstable tears (Geissler Grades III-IV).
Wrist Fractures
- Distal Radial Fractures: Arthroscopically assisted reduction is invaluable for evaluating and restoring intraarticular congruity. It allows for the direct visualization of articular step-offs, the clearance of fracture hematoma and chondral debris, and the concurrent management of associated soft-tissue injuries (e.g., TFCC tears, which occur in up to 40% of displaced distal radius fractures).
- Scaphoid Fractures: Arthroscopy assists in the percutaneous fixation of scaphoid fractures, ensuring precise guidewire placement and confirming the absence of screw protrusion into the radiocarpal or midcarpal joints.
Bone Excision and Chondral Procedures
- Arthroscopic Wafer Procedure: Partial resection of the distal ulna (typically 2-3 mm) through the TFCC defect for the treatment of ulnar impaction syndrome.
- Radial Styloidectomy: Indicated for early-stage scaphoid nonunion advanced collapse (SNAC) or radioscaphoid arthritis.
- Proximal Row Carpectomy (PRC) and Scaphoid Excision: Advanced arthroscopic techniques now allow for the complete excision of the proximal carpal row or the proximal pole of the scaphoid in cases of advanced collapse or nonunion.
- Kienböck Disease: Arthroscopic evaluation of lunate articular cartilage integrity dictates staging and treatment, occasionally involving lunate excision or core decompression.
Miscellaneous Indications
- Dorsal Ganglion Excision: Arthroscopic resection of the ganglion stalk at the scapholunate interval reduces recurrence rates and minimizes postoperative stiffness compared to open excision.
- Synovectomy: Highly effective for inflammatory arthritides (e.g., Rheumatoid Arthritis) to delay articular destruction.
- Septic Arthritis: Arthroscopic lavage and extensive débridement provide superior joint clearance with minimal morbidity.
- Adhesion Release: Arthroscopic arthrolysis for post-traumatic wrist stiffness.
Clinical Pearl: When evaluating a patient for wrist arthroscopy, always correlate clinical examination findings with advanced imaging. While arthroscopy is the gold standard, it is an invasive procedure that should be reserved for cases where conservative management has failed or when precise intraarticular intervention is definitively required.
ESSENTIAL EQUIPMENT AND INSTRUMENTATION
The tight confines of the radiocarpal and midcarpal joints necessitate specialized, low-profile equipment. Utilizing standard knee or shoulder arthroscopy equipment in the wrist significantly increases the risk of iatrogenic scuffing of the articular cartilage.
Optical Systems
- Arthroscope: A short-barrel arthroscope with a diameter of 2.5 to 3.0 mm is considered the standard workhorse for routine radiocarpal and midcarpal evaluation.
- Optional Scopes: Smaller scopes ranging from 1.7 to 2.0 mm are highly beneficial for navigating extremely tight joints, evaluating the DRUJ, or assessing pediatric patients.
- Length and Angulation: The ideal length is 50 to 60 mm. A 30-degree lens-offset angle provides the optimal field of view for general diagnostic sweeps. A 70-degree scope is occasionally utilized to visualize the volar capsule or the undersurface of the TFCC.
- Imaging Chain: A solid-state chip high-definition television camera coupled with a high-resolution color monitor is mandatory. Digital recording capabilities (video printer, CD/DVD burner, or modern secure cloud capture) are essential for documentation and medicolegal purposes.
Fluid Management Systems
Adequate joint distension is critical for visualization and to prevent iatrogenic cartilage injury during instrument insertion.
* Gravity Feed: Suspending 3-liter bags of normal saline or lactated Ringer's solution high above the operative field is usually satisfactory for routine diagnostic procedures.
* Mechanical Pumps: Automated infusion pumps provide superior, consistent irrigation and allow for the aggressive use of motorized suction-cutting tools.
* Inflow/Outflow: Inflow is typically established through the arthroscope sheath. Outflow can be managed via an 18-gauge needle placed in an accessory portal (e.g., 6U) or through dedicated sterile tubing connected to a suction device.
Surgical Warning: When using mechanical infusion pumps in the wrist, strict pressure monitoring is imperative. The wrist capsule is small and relatively non-compliant. Excessive hydrostatic pressure can lead to rapid fluid extravasation into the forearm compartments, precipitating acute compartment syndrome. Pressures should generally not exceed 30 to 40 mm Hg.
Manual and Powered Instruments
- Probes: A four-jaw, shallow probe (40 mm long, 1.5 to 2.0 mm in diameter) is the most critical diagnostic tool. It acts as an extension of the surgeon's finger to palpate cartilage softening, test ligamentous tension, and elevate meniscal flaps.
- Manual Forceps: Basket forceps (2 to 3 mm in diameter, 40 to 60 mm long) and grasping forceps with thin jaws (straight and curved) are required for precise tissue resection and loose body retrieval.
- Powered Resectors (Shavers): A full-radius resector, 2.0 to 3.0 mm in diameter, is optimal for synovectomy and débridement.
- Radiofrequency (RF) Wands: Bipolar RF wands (1.5 to 2.5 mm) are utilized for hemostasis, capsular shrinkage, and precise ablation of the TFCC or interosseous ligaments.
PATIENT POSITIONING AND PREPARATION
Proper patient positioning is the foundation of a successful wrist arthroscopy. It dictates the ease of portal placement, the efficiency of the procedure, and the safety of the neurovascular structures.
Anesthesia and Tourniquet Control
Wrist arthroscopy can be performed under regional block anesthesia (e.g., supraclavicular or axillary brachial plexus block) or general anesthesia.
* General Anesthesia: Often preferred if multiple complex procedures are anticipated, if bone grafting from a distant site (e.g., iliac crest) is required, or to ensure absolute patient immobility during delicate intraarticular work.
* Tourniquet: The use of a pneumatic arm tourniquet is highly recommended to maintain a bloodless field, which is critical given the small volume of the joint space. It is particularly helpful when treating intraarticular fractures or performing extensive synovectomies. The tourniquet is typically inflated to 250 mm Hg after exsanguination of the limb.
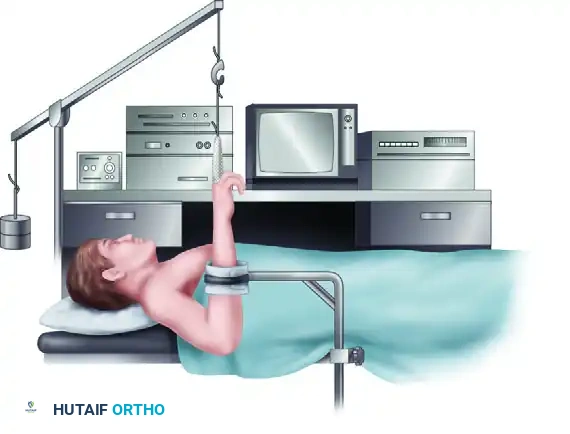
The Vertical Setup (Standard Positioning)
The most common configuration for wrist arthroscopy is the vertical traction setup.
1. The patient is positioned supine on the operating table.
2. The operative shoulder is abducted to 90 degrees and supported on a radiolucent hand table.
3. The elbow is flexed to 90 degrees, directing the hand and fingers vertically toward the ceiling.
4. Traction Application: Sterile fingertraps (wire mesh or nylon) are applied to the index and long fingers. Applying traps to the ring or small fingers is generally avoided to prevent ulnar nerve traction neurapraxia.
5. Distraction Force: The fingertraps are connected to a ceiling hook, an overhead pole and pulley system, or a specialized robotic traction tower. Traction weights ranging from 4 to 7 lbs (approx. 2 to 3 kg) are applied.
6. Counter-Traction: A padded forearm or wrist stabilizer (counterweight strap) is placed across the proximal forearm to provide counter-traction and stabilize the limb in space.
This vertical distraction utilizes the principle of ligamentotaxis to open the radiocarpal and midcarpal spaces, allowing safe introduction of the arthroscope and instruments.
The Horizontal Setup
An alternative positioning technique is the horizontal setup, where the elbow is extended, and the hand is placed flat on the hand table.
* Indications: This position is particularly advantageous for the arthroscopically assisted reduction of intraarticular distal radius fractures.
* Biomechanics: It allows the surgeon to freely pronate and supinate the forearm, facilitating the reduction of specific fracture fragments. Furthermore, it allows for unimpeded, orthogonal fluoroscopic imaging (C-arm) without the traction tower obstructing the radiographic view. Traction in this position is usually maintained manually by an assistant or via a specialized horizontal distraction frame.
SURGICAL APPROACH: STEP-BY-STEP PORTAL PLACEMENT
Precise portal placement is critical to avoid injury to the extensor tendons, superficial sensory nerves, and articular cartilage. Portals are named based on their relationship to the dorsal extensor compartments.
Radiocarpal Portals
- 3-4 Portal: The primary viewing portal. Located between the 3rd compartment (Extensor Pollicis Longus - EPL) and the 4th compartment (Extensor Digitorum Communis - EDC). It is palpated as a soft spot just distal to Lister's tubercle.
- 4-5 Portal: The primary working portal. Located between the 4th compartment (EDC) and the 5th compartment (Extensor Digiti Minimi - EDM).
- 6R Portal: Located immediately radial to the Extensor Carpi Ulnaris (ECU) tendon. Used for viewing the TFCC and ulnar carpus.
- 6U Portal: Located immediately ulnar to the ECU tendon. Often used as an outflow portal or for instrumentation of peripheral TFCC tears. Care must be taken to avoid the dorsal sensory branch of the ulnar nerve.
Midcarpal Portals
- Radial Midcarpal (MCR) Portal: Located approximately 1 cm distal to the 3-4 portal, in the palpable depression between the scaphoid, lunate, and capitate. Used to evaluate the scapholunate interval from the midcarpal perspective.
- Ulnar Midcarpal (MCU) Portal: Located approximately 1 cm distal to the 4-5 portal, in line with the axis of the fourth metacarpal. Used to evaluate the lunotriquetral interval and the triquetrohamate articulation.
Pitfall: Never use a scalpel to blindly incise the capsule. The skin should be incised superficially (only the epidermis and dermis). A blunt hemostat should then be used to spread the subcutaneous tissues down to the capsule to push away the superficial sensory branches of the radial and ulnar nerves. The capsule is then punctured with a blunt trocar to enter the joint.
POSTOPERATIVE PROTOCOLS
Postoperative management is highly dependent on the specific pathology treated.
- Diagnostic Arthroscopy / Simple Débridement: Patients are typically placed in a bulky soft dressing or a removable volar splint for comfort. Immediate active range of motion (ROM) of the fingers is encouraged to prevent tendon adhesions and reduce edema. Wrist ROM exercises begin within 3 to 5 days postoperatively.
- TFCC Repairs / Ligamentous Pinning: Patients require rigid immobilization. A Muenster-style cast or a long-arm splint restricting forearm rotation is often utilized for 4 to 6 weeks to protect the repair, followed by a phased rehabilitation program focusing on progressive ROM and eventual strengthening.
- Fracture Management: Postoperative protocols follow the standard guidelines for the specific fracture pattern and the rigidity of the internal fixation achieved.
Meticulous attention to equipment setup, precise anatomical portal placement, and a thorough understanding of carpal biomechanics are the hallmarks of a master wrist arthroscopist. By adhering to these rigorous standards, surgeons can maximize diagnostic accuracy and deliver superior therapeutic outcomes for complex wrist pathologies.
You Might Also Like