Masterclass in Elbow Arthroscopy: Principles and Techniques

Key Takeaway
Elbow arthroscopy is an advanced, minimally invasive surgical technique utilized for the diagnosis and treatment of complex intra-articular elbow pathology. This comprehensive guide details critical indications, precise patient positioning—including supine, prone, and lateral decubitus—and meticulous portal placement. Mastery of these foundational principles, alongside strict adherence to neurovascular safety protocols, is essential for orthopedic surgeons to optimize patient outcomes and minimize perioperative complications.
Introduction to Elbow Arthroscopy
Arthroscopic evaluation and surgical management of the elbow have advanced exponentially in both popularity and technical sophistication. Historically considered a high-risk procedure due to the intimate proximity of major neurovascular structures to the joint capsule, elbow arthroscopy has evolved into a safe and highly effective modality. The description of new, safer portals, the development of advanced surgical instrumentation, and a more profound biomechanical understanding of elbow pathology have collectively expanded the surgeon's armamentarium.
This comprehensive guide delineates the critical indications, precise patient positioning strategies, and meticulous portal placement techniques required to master elbow arthroscopy.
Indications and Contraindications
Primary Indications
Elbow arthroscopy is a powerful diagnostic and therapeutic tool. It has proven to be highly efficacious in the following clinical scenarios:
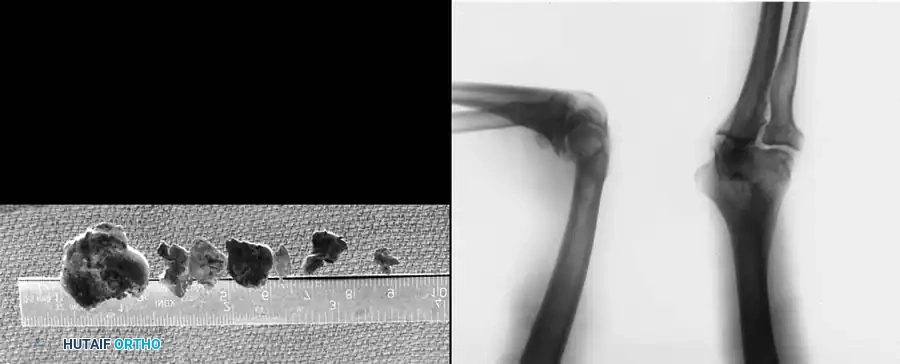
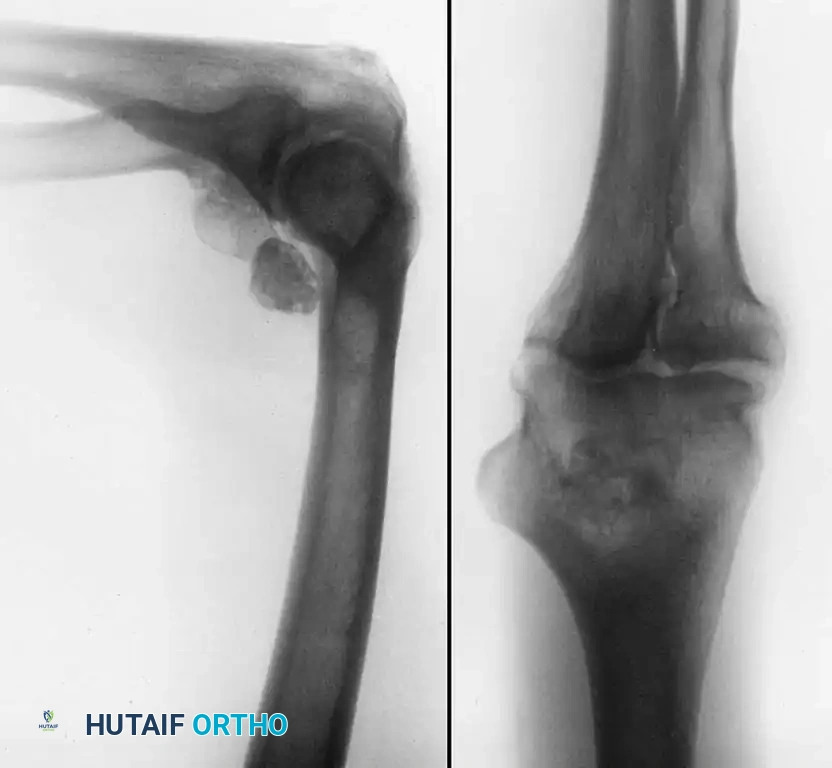
- Loose Body Removal: Evaluation and extraction of chondral or osteochondral loose bodies, which frequently reside in the olecranon or coronoid fossae.
- Osteochondritis Dissecans (OCD): Evaluation and treatment of OCD lesions, particularly of the capitellum in adolescent throwing athletes.
- Radial Head Pathology: Assessment and management of chondral or osteochondral lesions of the radial head.
- Degenerative Joint Disease: Excision of impinging osteophytes from the humerus (coronoid/olecranon fossae) and the olecranon tip to restore terminal extension and flexion.
- Inflammatory Arthropathy: Partial or subtotal synovectomy, which is particularly beneficial in patients with rheumatoid arthritis or synovial chondromatosis.
- Arthrofibrosis: Débridement and lysis of intra-articular adhesions in posttraumatic or severe degenerative disease to restore range of motion.
- Lateral Epicondylitis: Arthroscopic tennis elbow release (resection of the extensor carpi radialis brevis origin).
- Diagnostic Dilemmas: Evaluation of the chronically painful elbow when advanced imaging (MRI, CT arthrography) and other diagnostic tests remain inconclusive.
Furthermore, the arthroscope is increasingly utilized for the débridement of inflamed olecranon bursae, arthroscopic-assisted stabilization procedures (e.g., LUCL plication), and the reduction and internal fixation of select intra-articular fractures (such as radial head or capitellar shear fractures).

Absolute and Relative Contraindications
While the applications of elbow arthroscopy are broad, strict adherence to contraindications is paramount to avoid catastrophic complications.
- Ankylosis: Bony ankylosis or severe fibrous ankylosis that obliterates the joint space prevents the safe introduction of the arthroscope and instruments.
- Altered Anatomy: Previous surgery that distorts normal elbow anatomy is a major red flag.
Surgical Warning: Anterior transposition of the ulnar nerve is an absolute contraindication to standard medial portal placement. The altered course of the nerve places it at extreme risk during the establishment of the anteromedial or proximal medial portals.
- Infection: As with all elective arthroscopic procedures, elbow arthroscopy should not be performed in the presence of active periarticular soft-tissue infection (cellulitis), unless the procedure is specifically indicated for the irrigation and débridement of a septic joint.

Anesthesia and Tourniquet Management
Elbow arthroscopy can be performed under general anesthesia, regional anesthesia, or a combination of both.
General Anesthesia: This is the preferred modality for most complex elbow arthroscopies. It affords complete muscle relaxation, which is critical for joint manipulation, and eliminates intraoperative patient discomfort.
Regional Anesthesia: Local or regional anesthesia (e.g., interscalene, axillary, or Bier block) can be utilized, particularly when the patient is in the supine position. However, regional blocks carry distinct disadvantages:
1. Neurological Assessment: An accurate neurovascular examination cannot be performed immediately postoperatively, which delays the diagnosis of potential iatrogenic nerve injury.
2. Tourniquet Pain: Patients frequently experience tourniquet pain with an axillary block.
3. Operative Crowding: With a Bier block, the required double tourniquet system often compromises and crowds the proximal operative field.
While local anesthesia allows the patient to communicate paresthesias if instruments approximate neurovascular structures, it precludes the use of a tourniquet. Therefore, local anesthesia should be strictly reserved for highly experienced arthroscopists performing minor procedures (e.g., simple loose body removal) requiring minimal portals.
A pneumatic tourniquet is routinely used to control hemostasis. It must be placed as high as possible on the proximal arm to avoid crowding the surgical field and interfering with proximal portal placement.
Patient Positioning
The choice of patient positioning—supine, prone, or lateral decubitus—depends on surgeon preference, the specific pathology being addressed, and the need for airway access. Each position offers distinct biomechanical advantages.
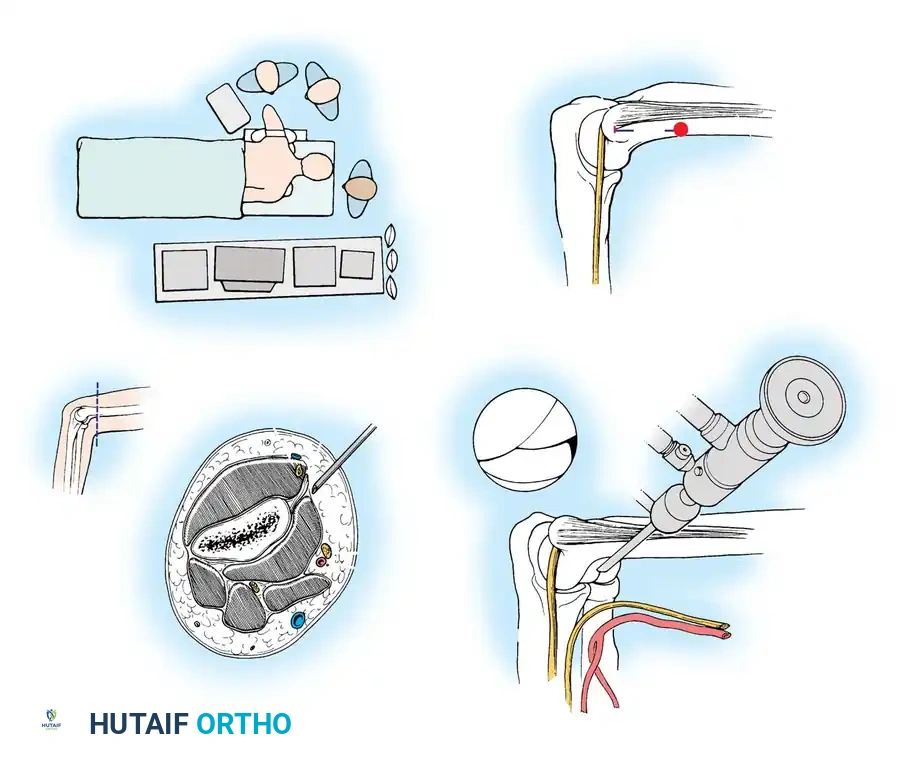
The Supine Suspended Position
With the patient supine, the hand and forearm are placed in a sterile, waterproof stockinette suspension device. This is connected to a rope and pulley system utilizing 5 to 6 lbs of weight to provide balanced suspension.

The patient is positioned so the arm hangs free off the side of the operating table. The shoulder is placed in neutral rotation and 90 degrees of abduction, while the elbow is flexed at 90 degrees.
Advantages of the Supine Position:
* Provides excellent access to both the medial and lateral sides of the elbow.
* The 90-degree flexion relaxes the anterior neurovascular structures in the antecubital fossa, allowing them to fall away from the joint capsule.

The Carson Modification: To eliminate the need for an overhead suspension system, Carson described utilizing two small arm boards placed side-by-side and attached to the operating table at shoulder level. The arm rests on this platform, and an assistant supports the hand upright. This stabilizes the elbow, preventing it from swinging in space, while the narrowness of the boards ensures unobstructed maneuvering of the arthroscope.
The Prone Position
Introduced by Poehling et al. in 1989, the prone position is favored by many advanced elbow arthroscopists.
The patient is placed prone on chest rolls to ensure adequate ventilation. A tourniquet is applied around the proximal arm. An arm board is placed parallel to the operating table, and the shoulder and proximal arm are elevated on a sandbag. The arm is positioned with the shoulder in neutral rotation and 90 degrees of abduction, with the elbow flexed 90 degrees so the hand points directly toward the floor.

Advantages of the Prone Position:
* Improves arthroscopic mobility and makes joint manipulation highly ergonomic.
* Provides superior access to the posterior aspect of the joint (olecranon fossa).
* Gravity assists in pulling the anterior neurovascular structures further away from the anterior capsule, enhancing safety during anterior portal placement.

The surgeon stands with the operating table elevated to chest level to prevent contamination of the dependent hand.
The Lateral Decubitus Position
Developed as a modification of the prone position, the lateral decubitus setup allows excellent access to the posterior compartment while maintaining easier airway access for the anesthesiologist.
The patient is stabilized in the lateral decubitus position using a beanbag and kidney rest. The arm is placed over a bolster attached to the bed. This bolster must be small enough to remain out of the operative field, allowing the elbow to hang freely at 90 degrees of flexion with unobstructed access to all portals. While Takahashi et al. advocated for continuous traction to assist in joint visualization, manual distraction by an assistant is often sufficient to improve exposure.

Portal Placement and Neurovascular Anatomy
Precise portal placement is the most critical aspect of elbow arthroscopy. A thorough understanding of the neurovascular anatomy is mandatory.


Joint Distention and Preparation
Before establishing any portal, the bony landmarks must be meticulously outlined with a marking pen:
* Lateral: Lateral epicondyle and radial head.
* Medial: Medial epicondyle and the course of the ulnar nerve.
* Posterior: Tip of the olecranon.
The joint must be maximally distended with 20 to 30 mL of sterile normal saline prior to portal placement. Distention pushes the anterior capsule—and the overlying neurovascular structures—anteriorly, significantly increasing the margin of safety.
Clinical Pearl: Fluid extravasation is the Achilles heel of elbow arthroscopy. Maintaining established portals with interchangeable cannulas (or cannulas with rubber diaphragms) is essential. This reduces the risk of damaging adjacent nerves with repeated instrument passage and decreases fluid extravasation, which can lead to devastating neurovascular compression (compartment syndrome) in the antecubital fossa.

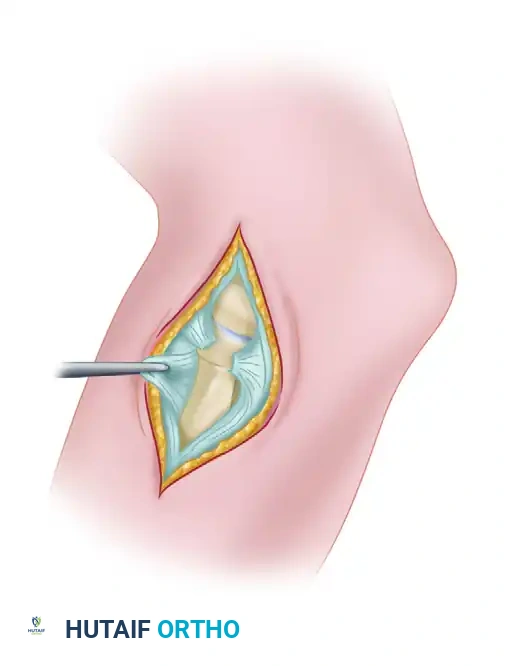
Lateral Portals
The Direct Lateral Portal:
Located in the "lateral soft spot" where elbow effusions are most easily palpable and aspirated. It is situated in the center of the triangle formed by the lateral epicondyle, the radial head, and the tip of the olecranon. Instruments passed through this portal traverse the skin, subcutaneous tissue, anconeus muscle, and joint capsule. This is typically the first portal established to distend the joint.
Anterior Portals
The Anterolateral Portals:
Traditionally the standard diagnostic portal, the anterolateral portal is established after joint distention. There are three variations:
1. Distal Anterolateral: 2 to 3 cm distal and 1 cm anterior to the lateral epicondyle.
2. Midanterolateral: Just proximal and 1 cm anterior to the palpable radiocapitellar joint.
3. Proximal Anterolateral: 2 cm proximal and 1 cm anterior to the lateral epicondyle (described by Field et al.).

The anterolateral portal traverses the extensor carpi radialis brevis (ECRB) muscle and passes beneath the radial nerve.
Surgical Pitfall: The radial nerve is at extreme risk during anterolateral portal placement. Lynch et al. demonstrated that instruments may pass within 4 mm of the radial nerve in an undistended elbow. However, with 90 degrees of flexion and maximal joint distention, the distance increases to an average of 11 mm.
Field et al. found the safety margin is greatest with the proximal anterolateral portal (13.7 mm), followed by the midanterolateral (10.9 mm), and least with the distal anterolateral portal (7.2 mm).

Surgical Technique for Portal Entry:
Skin incisions must be made superficially with a No. 11 blade to protect the lateral and posterior antebrachial cutaneous nerves. A small hemostat is used to bluntly spread the soft tissues down to the capsule before a blunt trocar is introduced into the joint.

The Anteromedial Portal:
Located 2 cm distal and 2 cm anterior to the medial epicondyle, approximating the medial extension of the flexor crease. It passes through the tendinous portions of the pronator teres and the radial aspect of the flexor digitorum sublimis.

When the elbow is flexed 90 degrees and maximally distended, cannulas pass a mean distance of 14 mm posterior to the median nerve and 17 mm posterior to the brachial artery. The medial antebrachial cutaneous (MABC) nerve and basilic vein are highly vulnerable here; transillumination from the lateral portal is strongly recommended before incision.
The Proximal Medial Portal (Supracondylar Anteromedial):
Highly recommended when the patient is prone. It is located 2 cm proximal to the medial epicondyle, just anterior to the medial intermuscular septum. The blunt trocar is directed anterior to the humerus, aiming toward the radial head, keeping constant contact with the anterior humeral cortex to avoid the median nerve and brachial artery.

Posterior Portals
Posterior portals are essential for evaluating the olecranon fossa, the posterior trochlea, and the triceps insertion.
- Direct Posterior Portal: Located 3 cm proximal to the tip of the olecranon, directly in the midline. It traverses the triceps tendon.
- Posterolateral Portal: Located 2 to 3 cm proximal to the olecranon tip, just lateral to the lateral border of the triceps.
These portals are relatively safe, provided the ulnar nerve has not been previously transposed and the instruments are directed accurately into the olecranon fossa.
Postoperative Protocols and Rehabilitation
At the conclusion of the procedure, the joint is thoroughly irrigated to remove any remaining debris. The portals are typically closed with simple interrupted non-absorbable sutures or sterile adhesive strips, depending on the size of the cannula used.

A bulky, sterile compressive dressing is applied to minimize postoperative swelling and hemarthrosis. The neurovascular status of the extremity must be documented immediately in the recovery room.
Rehabilitation protocols are highly dependent on the specific pathology treated. For simple diagnostic arth
📚 Medical References
- elbow arthroscopy, Orthopedics 16:1037, 1993.
- Aoki M, Wada T, Isogai S, et al: Magnetic resonance imaging fi ndings of refractory tennis elbows and their relationship to surgical treatment, J Shoulder Elbow Surg 14:172, 2005.
- Azar FM: Elbow. In Miller MD, Cooper DE, Warner JJP, eds: Review of sports medicine and arthroscopy, Philadelphia, 2002, Saunders. Azar FM, Andrews JR, Wilk KE, et al: Operative treatment of
You Might Also Like