Gracilis and Tensor Fasciae Latae Muscle Flaps: A Master Surgical Guide
Key Takeaway
The gracilis and tensor fasciae latae (TFL) muscles provide versatile options for soft tissue coverage and functional reconstruction. The gracilis is ideal for free innervated functioning muscle transfer due to its reliable medial femoral circumflex pedicle. Conversely, the TFL flap, based on the lateral femoral circumflex artery, offers robust coverage with potential for osteomusculocutaneous harvest. This guide details the precise vascular anatomy, patient positioning, and step-by-step surgical dissection required for successful flap elevation and transfer.
INTRODUCTION TO LOWER EXTREMITY MUSCLE FLAPS
The reconstructive orthopedic surgeon must possess a profound understanding of lower extremity myocutaneous and muscle flaps to address complex soft tissue defects, osteomyelitis, and functional motor deficits. Among the most versatile and reliable options in the reconstructive armamentarium are the Gracilis Muscle Transfer and the Tensor Fasciae Latae (TFL) Muscle Flap.
While the gracilis is highly prized for its utility as a free innervated functioning muscle transfer (e.g., in brachial plexus reconstruction or facial reanimation), the TFL flap provides robust, sensate coverage for massive trochanteric, ischial, or sacral defects, with the added capability of incorporating vascularized bone from the iliac crest. This masterclass delineates the precise vascular anatomy, biomechanical considerations, and step-by-step surgical dissection required for the safe and effective harvest of both flaps.
PART I: GRACILIS MUSCLE TRANSFER
The gracilis can be utilized as either a free muscle flap or a musculocutaneous flap. Because it is relatively small with a long, narrow contour, it has limited utility for massive soft tissue coverage. However, its predictable neurovascular anatomy, excellent excursion, and minimal donor site morbidity make it the premier choice for a free innervated functioning muscle transfer.
Indications and Biomechanics
Biomechanically, the gracilis acts as an adductor of the hip, a weak flexor of the knee, and an internal rotator of the leg. Because its synergistic muscles (adductor longus, brevis, and magnus) are powerful, the harvest of the gracilis results in negligible functional deficit. Its parallel fiber arrangement allows for excellent contractile excursion, making it ideal for restoring finger flexion, elbow flexion, or facial animation.
Vascular Anatomy and Innervation
The gracilis arises from the anterior body and the inferior ramus of the pubis and the ischium. It passes distally in the medial thigh, posterior to the adductor longus and sartorius muscles, and inserts on the medial aspect of the proximal tibia (the pes anserinus), posterior and deep to the sartorius tendon and anterior to the semitendinosus muscle insertion.
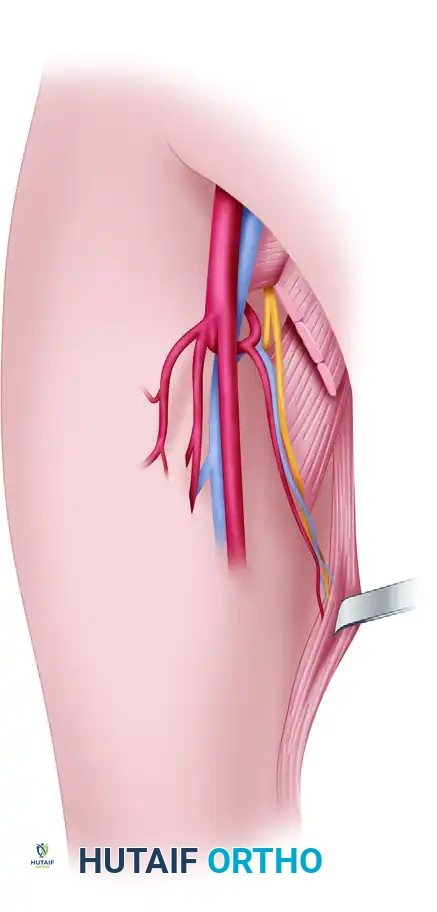
- Dominant Pedicle: The vascular pedicle is short and based on a terminal branch of the medial femoral circumflex artery (arising from the profunda femoris artery). The pedicle typically has a diameter of 1 to 2 mm.
- Pedicle Location: The artery and its venae comitantes enter the deep surface of the muscle approximately 8 to 12 cm distal to the muscle origin at the pubic tubercle. A vascular pedicle of 4 to 6 cm in length can reliably be obtained.
- Innervation: Motor innervation is supplied by a branch of the anterior division of the obturator nerve. This nerve accompanies the dominant vascular pedicle and typically divides into two to four fascicles that enter the muscle 6 to 10 cm from its origin.
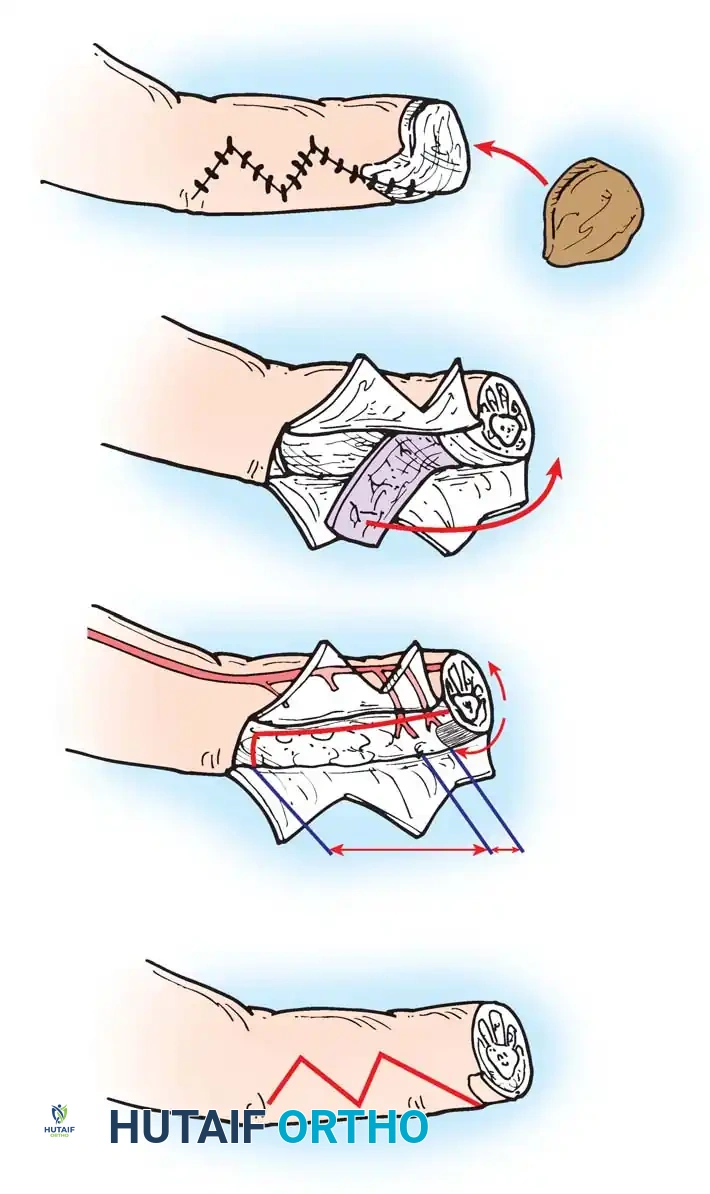
Figure 1: Gracilis muscle retracted. The major neurovascular pedicle enters in the proximal third of the muscle, including a branch of the medial femoral circumflex artery, a tributary of the femoral vein, and the anterior branch of the obturator nerve.
Patient Positioning and Preoperative Markings
The gracilis is conveniently harvested with the patient in the supine position. The hip is abducted and externally rotated, and the knee is slightly flexed (the "frog-leg" position).

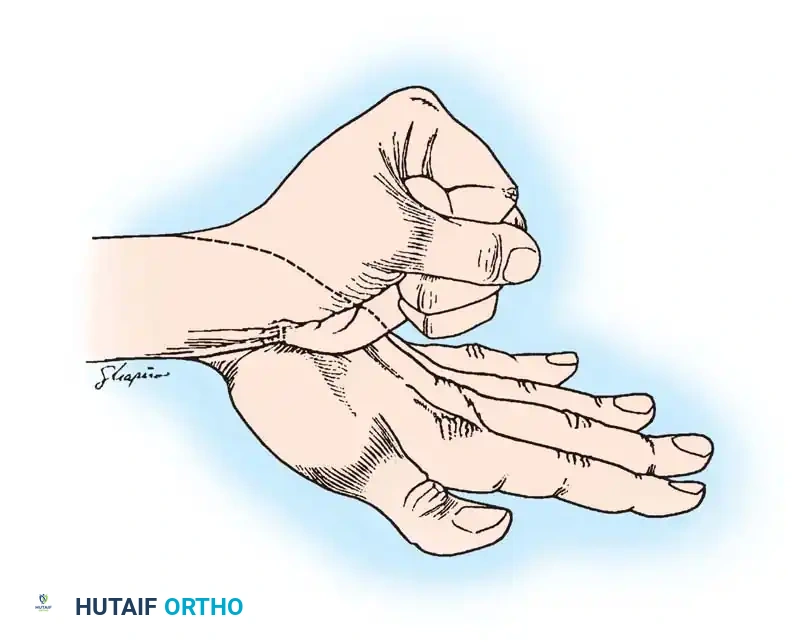
Figure 2: Gracilis muscle dissection positioning. The gracilis muscle lies posterior to a line drawn between the adductor origin and the tibial tuberosity.
- Palpate the pubic tubercle and the adductor longus tendon.
- Draw a straight line from the pubic tubercle to the medial epicondyle of the femur. The gracilis lies immediately posterior to this line.
- Mark the anticipated entrance of the neurovascular pedicle approximately 8 to 10 cm distal to the pubic tubercle.
Surgical Dissection of the Gracilis
- Incision: Make a longitudinal incision over the proximal third of the muscle, centered over the marked pedicle location. If a skin paddle is required, design it centered over the proximal third of the muscle to ensure capture of the musculocutaneous perforators.
- Identification: Incise the deep fascia and identify the interval between the adductor longus (anterior) and the gracilis (posterior).
- Pedicle Dissection: Retract the adductor longus anteriorly to expose the underlying adductor brevis and magnus. The neurovascular bundle will be found in the areolar tissue between the adductor longus and adductor magnus, entering the deep, anterior surface of the gracilis.
- Nerve Harvest: Trace the anterior branch of the obturator nerve proximally. Ensure sufficient length is harvested for the planned neurorrhaphy at the recipient site.
- Distal Release: Extend the incision distally to the medial knee. Identify the gracilis tendon at the pes anserinus, transect it, and reflect the muscle proximally.
- Proximal Release: Transect the proximal muscle belly near its tendinous origin on the pubis, isolating the muscle entirely on its neurovascular pedicle.
- Pedicle Division: Leave the vascular pedicle intact and perfused until the recipient site is fully prepared. Once ready, ligate and divide the vessels.
CLINICAL PEARL: When harvesting the gracilis for a functional transfer, secure the resting length of the muscle with marking sutures placed at 5 cm intervals before detaching the origin and insertion. This ensures accurate tensioning when the muscle is inset at the recipient site.
PART II: TENSOR FASCIAE LATAE (TFL) MUSCLE FLAP
The Tensor Fasciae Latae (TFL) flap is a highly versatile workhorse in reconstructive orthopedics. It can be harvested as a standard muscle flap, a musculocutaneous flap, a neurosensory flap, or an osteomusculocutaneous flap incorporating the anterior iliac crest.
Indications and Biomechanics
The TFL muscle functions as an abductor, medial rotator, and weak flexor of the hip. It also assists in stabilizing the knee in extension via its insertion into the iliotibial tract. Because the gluteus medius and minimus are the primary hip abductors, harvest of the TFL results in minimal functional loss, provided the gluteal insertions are undisturbed. The TFL flap is primarily indicated for the coverage of massive trochanteric pressure sores, lower abdominal wall defects, and complex pelvic reconstructions.
Vascular Anatomy and Innervation
- Dominant Pedicle: The TFL is a Type I muscle flap supplied by the ascending branch of the lateral femoral circumflex artery (LFCA), which arises from the profunda femoris.
- Pedicle Location: The vascular pedicle enters the deep surface of the muscle approximately 10 cm inferior to the anterior superior iliac spine (ASIS).
- Sensory Innervation: The skin overlying the TFL is innervated by the lateral femoral cutaneous nerve (L2, L3), which enters the flap 5 to 10 cm inferior to the ASIS, and the sensory branch of the T12 nerve posterolaterally.
- Motor Innervation: The superior gluteal nerve provides motor innervation, entering the muscle proximally.
Preoperative Planning and Markings
- Pedicle Marking: Mark the location of the anticipated entrance of the vascular pedicle approximately 10 cm inferior to the ASIS. This point is usually located along a line drawn transversely and laterally from the pubic tubercle.
- Nerve and Bone Planning: If the transfer is to be a neurosensory, osteomusculocutaneous, or functional free flap, identify the areas of the lateral femoral cutaneous nerve anteromedially, the sensory branch of the T12 nerve posterolaterally, the anticipated location of the motor branch, and any required bone before making the skin incision.
- Flap Design: Plan the flap dimensions so that the required neurovascular repairs and bone placement (if used) can be located appropriately in the recipient site without tension.
Step-by-Step Surgical Dissection of the TFL Flap
1. Anterior Dissection and Nerve Identification
- Incise the anterior margin of the flap through the subcutaneous tissue and the underlying fascia lata.
- If sensory nerves are to be incorporated in the transfer, dissect and identify them at this stage. The lateral femoral cutaneous nerve enters the flap 5 to 10 cm inferior to the ASIS. Identify the nerve in the subcutaneous tissue, dissect it proximally, and divide it, ensuring you provide sufficient nerve length for repair before identifying the vascular pedicle.
- Continue the dissection anteriorly and medially, deep to the fascia lata, until the interval between the tensor fasciae latae and the rectus femoris is encountered. This intermuscular septum is usually obvious and serves as the primary gateway to the pedicle.
2. Pedicle Isolation
- Use blunt dissection to locate the transverse branches of the lateral femoral circumflex vessels deep to the rectus femoris.
- Identify the descending branch of the LFCA that courses distally into the vastus lateralis, and ligate it to mobilize the main trunk.
- Trace the lateral femoral circumflex artery with its two venae comitantes medially, beneath the rectus femoris, to its origin off the profunda femoris.
SURGICAL WARNING: During the medial dissection of the lateral femoral circumflex artery beneath the rectus femoris, meticulous care must be taken to avoid iatrogenic injury to the motor branches of the femoral nerve, which lie in close proximity to the vascular origin.
3. Posterior and Distal Release
- After the vascular pedicle has been clearly delineated and protected, incise the posterior margin of the skin flap.
- Crucial Step: Suture the margins of the skin flap to the muscle superiorly and to the fascia lata distally. This prevents shearing forces from disrupting the delicate musculocutaneous perforators during flap manipulation.
- Deepen the dissection through the interval between the gluteus maximus and the TFL. Continue medially until the vascular pedicle is encountered from the posterior aspect. Protect the vascular pedicle with a vessel loop or soft retractor during this portion of the dissection.
- Section the tensor fasciae latae distally at the required length, and develop the flap in a cephalad direction, elevating it off the underlying vastus lateralis.
4. Proximal Release and Osteotomy (If Indicated)
- Elevate the superior margin of the flap proximally. Incise and divide the proximal muscle superior to the entrance of the vascular pedicle.
- Osteocutaneous Harvest: If vascularized bone is to be included, carry the dissection more proximally after the incision and elevation of the superior skin to the level of the iliac crest. Using a sharp osteotome or oscillating saw, include the tensor fasciae latae with the underlying block of the anterior iliac crest.
- Leave the vascular pedicle intact until the recipient site is completely prepared and hemostasis is achieved. Once ready, section the vessels for transfer.
PART III: COMPARATIVE ANATOMY - THE RECTUS ABDOMINIS
While the Gracilis and TFL are primary choices for lower extremity and functional reconstruction, the Rectus Abdominis muscle flap remains a critical comparative workhorse, particularly for massive soft tissue defects requiring a long vascular pedicle.
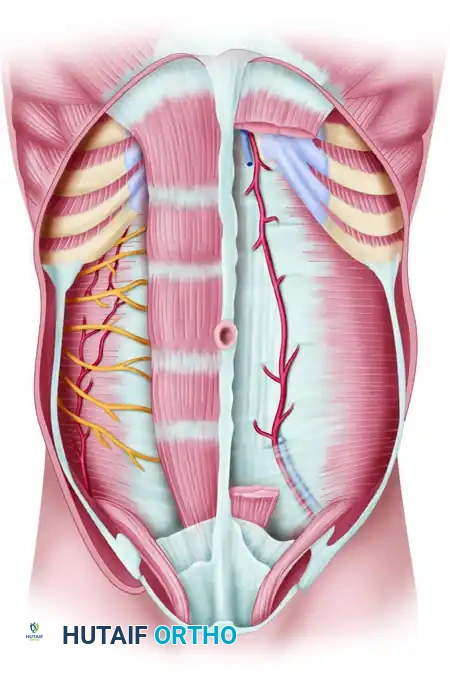
Figure 3: Anatomy of the rectus abdominis muscle and its sheath. Note the tendinous intersections, the superior and inferior epigastric vessels, and the arcuate line.
The rectus abdominis is a Type III muscle flap with two dominant pedicles: the superior epigastric artery and the deep inferior epigastric artery (DIEA). For free tissue transfer, the flap is almost exclusively based on the DIEA due to its larger caliber (2.5 to 3.0 mm) and longer pedicle length. Understanding the anatomical relationship between the rectus sheath, the arcuate line, and the deep inguinal ring is essential when comparing donor site morbidities. Unlike the TFL or Gracilis, harvest of the rectus abdominis carries a higher risk of donor site morbidity, specifically abdominal wall herniation or bulging, necessitating meticulous fascial closure or mesh reinforcement.
POSTOPERATIVE PROTOCOLS AND REHABILITATION
The success of a free or pedicled muscle transfer relies as much on postoperative management as it does on surgical execution.
Flap Monitoring
- Microvascular Checks: For free tissue transfers, monitor the flap clinically (color, capillary refill, turgor) and via handheld Doppler ultrasonography or implantable venous Doppler every 1 hour for the first 24 hours, then every 2 hours for the next 48 hours.
- Temperature: Maintain a warm ambient room temperature to prevent vasospasm.
Donor Site Management
- Drainage: Close the donor site wounds (both Gracilis and TFL) over large, closed-suction drains. Leave drains in place until output is less than 30 cc per 24 hours to prevent seroma formation, which is particularly common in the TFL donor site due to the large dead space over the lateral thigh.
- Closure: The TFL donor site can usually be closed primarily if the skin paddle is less than 8-10 cm wide. Larger defects may require split-thickness skin grafting over the vastus lateralis.
Mobilization and Weight-Bearing
- Early Motion: Hip and knee motion, as well as weight-bearing ambulation, can generally be started on the first postoperative day, strictly as allowed by the recipient site's stability.
- Restrictions: If an osteocutaneous TFL flap was harvested, limit active hip abduction and excessive weight-bearing for 4 to 6 weeks to allow the iliac crest donor site to heal and to prevent avulsion fractures of the ASIS.
- DVT Prophylaxis: Institute chemical and mechanical deep vein thrombosis (DVT) prophylaxis immediately postoperatively, balancing the risk of microvascular thrombosis against the risk of donor/recipient site hematoma.
By adhering to these meticulous anatomical dissections and rigorous postoperative protocols, the orthopedic microsurgeon can achieve highly reliable, functional, and aesthetically acceptable outcomes using both the Gracilis and Tensor Fasciae Latae muscle flaps.
You Might Also Like