Pectoralis Major Transfer and Tensor Fasciae Latae Flap: Advanced Surgical Techniques
Key Takeaway
The pectoralis major and tensor fasciae latae (TFL) muscle flaps are versatile workhorses in orthopaedic reconstructive surgery. This guide details the precise surgical dissection, neurovascular anatomy, and microneurovascular techniques required for successful free functioning muscle transfers and pedicled coverage. Mastery of these approaches ensures optimal restoration of upper extremity function and reliable soft tissue coverage for complex extremity defects.
INTRODUCTION TO ADVANCED MUSCLE TRANSFERS
In the realm of complex orthopaedic reconstruction, the utilization of vascularized muscle and musculocutaneous flaps remains a cornerstone for limb salvage, functional restoration, and the management of massive soft tissue defects. The pectoralis major and the tensor fasciae latae (TFL) represent two highly reliable, anatomically consistent donor sites.
The pectoralis major is frequently employed as a free functioning muscle transfer (FFMT) to restore critical upper extremity functions, such as elbow flexion or digital flexion/extension, particularly following devastating brachial plexus injuries or severe Volkmann’s ischemic contracture. Conversely, the TFL flap is a highly versatile option, capable of being harvested as a pedicled flap for regional coverage (e.g., trochanteric pressure sores, pelvic reconstruction) or as a free flap for distant extremity coverage. It can be tailored as a sensory-innervated flap, a functioning neuromuscular unit, or even an osteomusculocutaneous flap incorporating the iliac crest.
This comprehensive guide details the rigorous surgical dissection, neurovascular anatomy, and microneurovascular techniques required to successfully harvest and transfer these vital muscular units.
PART I: DISSECTION FOR PECTORALIS MAJOR TRANSFER
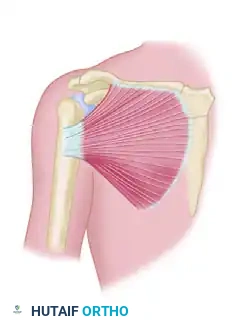
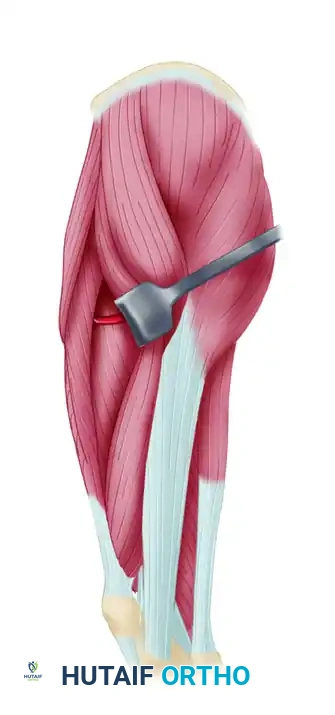
The pectoralis major is a broad, fan-shaped muscle that offers substantial bulk and excellent contractile excursion. When utilized as an innervated free muscle transfer to the forearm, it is typically reversed—the anatomical origin becomes the new insertion—to facilitate optimal alignment of the neurovascular pedicle with the recipient vessels and nerves in the proximal forearm.
Indications and Biomechanics
The primary indication for a free functioning pectoralis major transfer is the restoration of lost motor function in the upper extremity. Its robust cross-sectional area provides significant force generation, while its fiber length allows for adequate excursion (typically 5 to 7 cm), making it an excellent substitute for the flexor digitorum profundus or the extensor digitorum communis.
Clinical Pearl: When planning a pectoralis major FFMT for finger flexion, the muscle must be tensioned appropriately. Over-tensioning can lead to ischemic contracture of the transferred muscle, while under-tensioning will result in a profound lag and failure to achieve a functional fist.
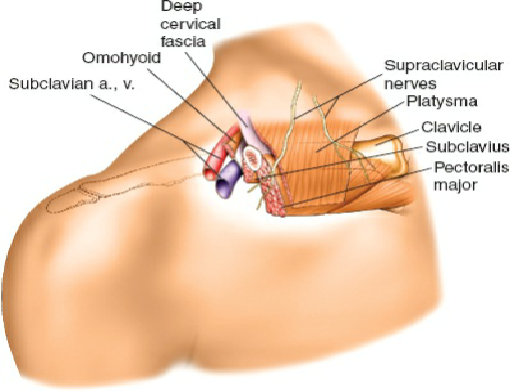
Vascular and Neural Anatomy
The pectoralis major is classified as a Type V muscle flap (Mathes and Nahai classification), possessing one dominant vascular pedicle and secondary segmental pedicles.
* Dominant Arterial Supply: The pectoral branch of the thoracoacromial artery.
* Venous Drainage: Venae comitantes accompanying the pectoral artery, draining into the cephalic or axillary vein.
* Motor Innervation: The medial and lateral pectoral nerves. The lateral pectoral nerve (C5, C6, C7) primarily innervates the clavicular head, while the medial pectoral nerve (C8, T1) innervates the sternocostal head.
Surgical Technique: Pectoralis Major Harvest
The harvest of the pectoralis major requires meticulous dissection to preserve the delicate neurovascular pedicle while ensuring adequate muscle volume is obtained. A two-team approach is highly recommended to minimize total ischemia time; one team prepares the recipient site in the forearm while the second team harvests the muscle.
Step 1: Incision and Exposure
* Position the patient supine with the ipsilateral arm abducted to 60 degrees.
* Design the incision along the lateral border of the pectoralis major, extending from the anterior axillary fold toward the sternum, depending on the required muscle volume.
* Elevate and mobilize the overlying skin and subcutaneous tissue off the anterior surface of the muscle.
* Remove the rectus fascia in continuity with the pectoral fascia to allow for full mobilization of the muscle's insertion attachment.
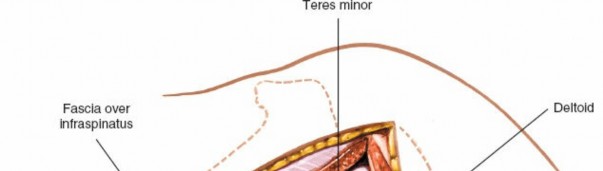
Step 2: Identification of the Neurovascular Pedicle
The neurovascular pedicle can be approached via two distinct methods:
* Approach A (Inferior Elevation): Elevate the lower margin of the muscle, exposing its deep surface. Carefully dissect superiorly to identify the major branch of the inferior pectoral artery and its accompanying venae comitantes.
* Approach B (Sternal-Clavicular Separation): Separate the sternal head from the clavicular head of the pectoralis major. This natural anatomical split provides direct, safe access to the underlying neurovascular pedicles.
Surgical Warning: Before encountering the main vascular pedicle, you will identify the lateral and inferior pectoral nerves. Dissect these structures with extreme caution, as they are highly susceptible to traction injury during muscle elevation.

Step 3: Muscle Mobilization and Detachment
* Once the muscle has been dissected from medial to lateral and the neurovascular pedicle is completely isolated and protected, confirm with the recipient team that the forearm site is prepared for immediate transfer.
* Section the insertion of the pectoralis major from the bicipital groove of the humerus.
* Ligate the vascular pedicle only when the recipient vessels are fully dissected and ready for anastomosis.
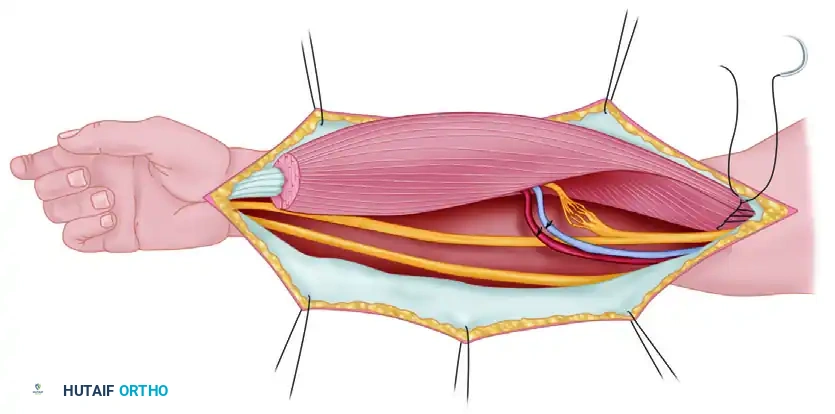
Step 4: Transfer and Microneurovascular Repair
* Transfer the muscle to the forearm. If using the muscle as an innervated free muscle transfer, reverse its orientation. The anatomical origin (sternal/clavicular attachments) becomes the distal insertion (sutured to the recipient tendons), and the anatomical insertion becomes the proximal origin (sutured to the medial epicondyle or proximal ulna).
* This reversal allows the neurovascular pedicle, located on the deep surface of the muscle, to naturally align with the recipient vessels (e.g., radial or ulnar artery) and nerves (e.g., anterior interosseous nerve) in the proximal forearm.
- Perform the microvascular anastomoses using standard microsurgical techniques (typically 9-0 or 10-0 nylon).
- Perform a perineurial (fascicular) neurorrhaphy between the donor pectoral nerve and the recipient motor nerve. Tension-free coaptation is critical for successful motor reinnervation.
Step 5: Closure
* The donor site team achieves meticulous hemostasis and closes the chest defect over closed-suction drainage tubes to prevent hematoma formation.
* The recipient team completes the tendon weaves (e.g., Pulvertaft weave) to the target digits, setting the resting tension with the wrist in neutral and the fingers in a functional cascade.
PART II: TENSOR FASCIAE LATAE (TFL) MUSCLE FLAP
The Tensor Fasciae Latae (TFL) flap is a highly adaptable reconstructive option. While its fascial surface may not readily adhere to a recipient site without proper preparation, the TFL can be utilized for broad soft tissue coverage in the upper or lower extremity. Furthermore, it can be designed as a sensory-innervated flap, a functioning neuromuscular unit, or an osteomusculocutaneous flap incorporating a vascularized segment of the anterior iliac crest.
Indications and Limitations
- Soft Tissue Coverage: Excellent for massive defects, particularly around the pelvis, greater trochanter, and lower extremity.
- Functional Transfer: Its function as an innervated flexor substitute is limited due to its relatively short muscle fiber length and limited excursion. However, it demonstrates significant potential as an extensor replacement where massive excursion is less critical.
- Sensory Flap: Can provide protective sensation to weight-bearing areas (e.g., heel reconstruction) when the lateral femoral cutaneous nerve is coapted to a local sensory nerve.
Vascular and Neural Anatomy
Understanding the precise anatomical landmarks of the TFL is paramount for safe harvest.
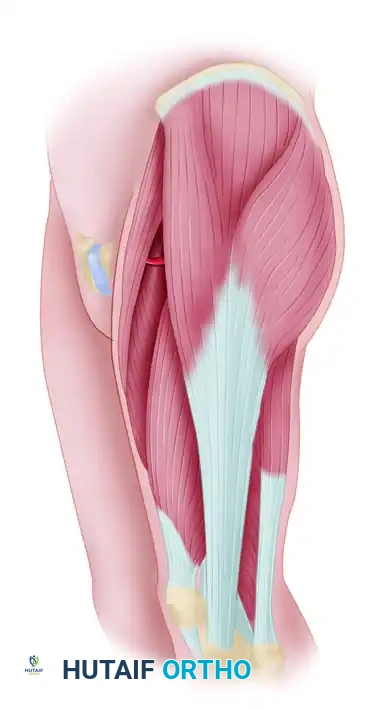
* Origin and Insertion: Originates from the anterior portion of the iliac crest and inserts into the fascia lata (iliotibial tract) of the lateral thigh.
* Arterial Supply: The TFL is a Type I muscle flap, supplied by a single major artery: the transverse branch of the lateral femoral circumflex artery (LFCA), which arises from the profunda femoris artery.
* Pedicle Characteristics: The vascular pedicle enters the deep surface of the muscle at its midpoint, approximately 10 cm inferior to the anterior superior iliac spine (ASIS). The arterial supply lies deep to the rectus femoris muscle and gives collateral branches to the rectus femoris, vastus lateralis, and gluteus minimus. A pedicle length of 6 to 8 cm can be reliably dissected, with vessel diameters ranging from 2.0 to 2.5 mm.
* Venous Drainage: Two venae comitantes accompany the arterial pedicle.
* Motor Innervation: A branch of the superior gluteal nerve enters the muscle proximal to the vascular pedicle.
* Sensory Innervation: The overlying skin paddle (which can be harvested up to 10 × 30 cm) receives sensory innervation from two sources:
1. Cutaneous branch of the T12 nerve: Enters the subcutaneous tissue near the posterosuperior aspect of the flap.
2. Lateral Femoral Cutaneous Nerve (LFCN): Enters the medial portion of the flap in the subcutaneous tissue, approximately 8 to 10 cm distal to the ASIS.
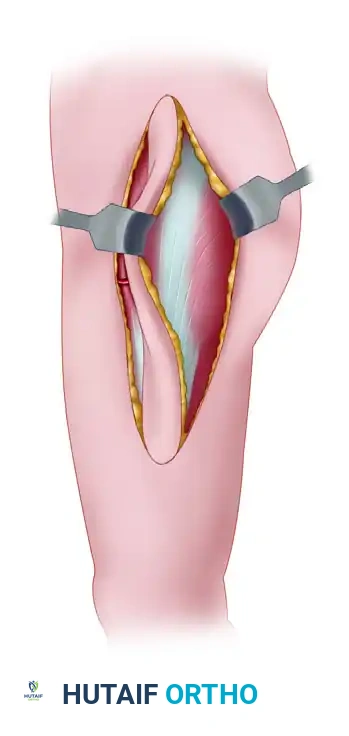
Surgical Technique 63-20: TFL Flap Harvest
Step 1: Preoperative Marking and Incision
* Position the patient supine with a bump under the ipsilateral hip to internally rotate the leg slightly, exposing the lateral thigh.
* Outline the required skin paddle on the proximal lateral thigh. The midaxis of the muscle flap (and musculocutaneous flap) lies along a line drawn from a point 3 cm posterior to the ASIS extending distally to the head of the fibula.
Step 2: Anterior and Medial Dissection
* Incise the anterior border of the designed skin paddle down through the subcutaneous tissue and fascia lata.
* Identify the interval between the TFL and the rectus femoris. Retract the rectus femoris medially.
* Carry the dissection anteriorly and medially deep to the rectus femoris to identify the transverse branch of the lateral femoral circumflex artery.
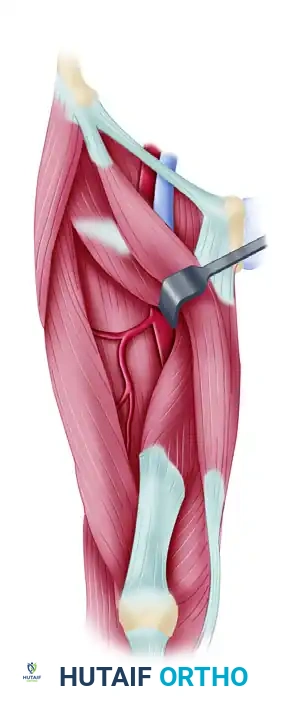
Clinical Pearl: The descending branch of the LFCA will be seen traveling distally to supply the vastus lateralis. Ensure you are isolating the transverse branch that courses laterally into the deep surface of the TFL.
Step 3: Isolation of the Vascular Pedicle
* Carefully dissect the transverse branch of the LFCA and its venae comitantes back toward their origin from the profunda femoris to maximize pedicle length.
* Identify and preserve the motor branch from the superior gluteal nerve if a functional transfer is planned. If a sensory flap is planned, identify and dissect the lateral femoral cutaneous nerve at the proximal-medial margin of the flap.
Step 4: Posterior Dissection
* Incise the posterior margin of the skin paddle.
* Develop the plane between the posterior border of the TFL and the anterior border of the gluteus maximus. The fascia lata must be incised longitudinally to separate these two structures.
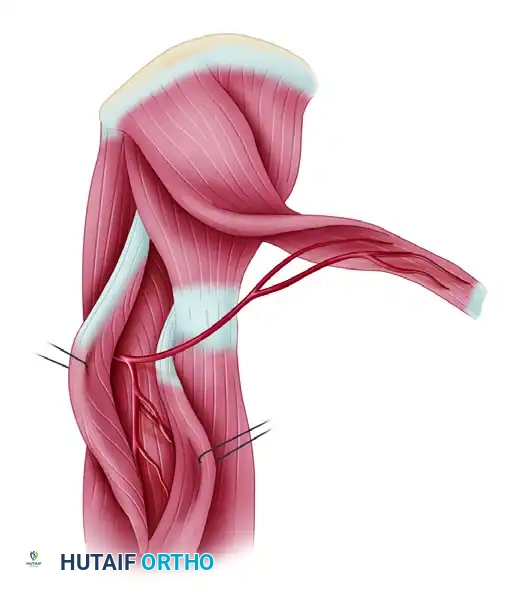
Step 5: Elevation of the Flap
* Once the anterior, posterior, and distal margins are incised, elevate the TFL flap from distal to proximal.
* The distal fascia lata is transected at the required length.
* Elevate the muscle off the underlying vastus lateralis, working towards the isolated neurovascular pedicle.
* If harvesting as a free flap, ligate the pedicle only when the recipient site is fully prepared. If harvesting as a pedicled flap for trochanteric or pelvic coverage, rotate the flap on its pedicle into the defect.
Step 6: Donor Site Closure
* Donor sites less than 8 to 10 cm in width can often be closed primarily by widely undermining the adjacent thigh skin.
* Larger defects will require a split-thickness skin graft (STSG) applied directly over the vastus lateralis muscle.
* Always place closed-suction drains beneath the closure or the STSG to prevent seroma or hematoma formation, which are common complications in this region.
POSTOPERATIVE PROTOCOL AND REHABILITATION
The success of any free functioning muscle transfer or complex pedicled flap relies heavily on rigorous postoperative management.
Immediate Postoperative Care (Days 0-7)
- Monitoring: Flap viability must be monitored hourly for the first 48 hours, then every 2-4 hours. Monitoring modalities include clinical assessment (color, capillary refill, turgor, temperature), handheld Doppler ultrasonography of the marked perforators, or implantable venous Doppler probes.
- Positioning: The reconstructed extremity must be elevated to minimize venous congestion. Avoid any pressure over the pedicle or the flap itself.
- Anticoagulation: Protocols vary by institution, but many microsurgeons utilize a combination of intravenous dextran, subcutaneous heparin, or daily aspirin to prevent microvascular thrombosis.
- Immobilization: For FFMTs (like the pectoralis major transfer), the limb is immobilized in a bulky splint that removes tension from the muscle origin and insertion repairs. For example, if transferred for finger flexion, the wrist is splinted in slight flexion with the fingers in a resting cascade.
Intermediate Phase (Weeks 2-6)
- Wound Care: Sutures are typically removed at 14 to 21 days. If a skin graft was used at the donor site, bolster dressings are removed at day 5-7.
- Passive Range of Motion (PROM): Gentle, therapist-guided PROM begins around week 3 to 4 to prevent tendon adhesions at the repair sites, ensuring no active tension is placed on the newly coapted muscle.
Late Phase and Neuromuscular Reeducation (Months 3-12)
- Reinnervation: Motor reinnervation occurs at a rate of approximately 1 mm per day. Clinical signs of muscle contraction may not be visible for 3 to 6 months, depending on the distance from the nerve coaptation to the motor endplates.
- Biofeedback: Once early contraction is palpated or detected via EMG, aggressive neuromuscular reeducation begins. Patients must cognitively link the original function of the donor nerve (e.g., chest adduction for the pectoral nerve) to the new function of the transferred muscle (e.g., finger flexion).
- Strengthening: Progressive resistance exercises are initiated only after full active range of motion is achieved and the muscle demonstrates sustained, coordinated contraction.
COMPLICATIONS AND PITFALLS
- Vascular Thrombosis: The most devastating complication of free tissue transfer. Venous congestion is more common than arterial insufficiency. Immediate return to the operating room for pedicle exploration and thrombectomy is mandatory if compromise is detected.
- Nerve Traction Injury: The medial and lateral pectoral nerves are highly sensitive to stretch during the elevation of the pectoralis major. Excessive traction will lead to a neuropraxia that can severely delay or permanently impair the functional outcome of the transfer.
- Donor Site Morbidity: TFL harvest can result in lateral thigh contour deformities and seroma formation. Meticulous closure over drains and the use of compressive garments are essential. Pectoralis major harvest results in a loss of forceful internal rotation and adduction of the shoulder, which must be discussed with the patient preoperatively.
- Inadequate Excursion: If the TFL is chosen for a functional transfer requiring large excursion (e.g., finger flexion), the outcome will likely be poor due to its short fiber length. Proper patient selection and matching the donor muscle biomechanics to the recipient site requirements are the hallmarks of a master reconstructive surgeon.
You Might Also Like