Gracilis and Rectus Abdominis Muscle Transfers: Operative Techniques
Key Takeaway
Free functioning muscle transfers and pedicled flaps, including the gracilis and rectus abdominis muscles, are foundational techniques in orthopaedic reconstructive surgery. This guide details the critical surgical anatomy, step-by-step harvesting techniques, and biomechanical considerations required for successful soft tissue coverage and functional restoration. Mastery of these procedures ensures optimal outcomes in complex extremity reconstruction and brachial plexus injuries.
INTRODUCTION TO MUSCLE TRANSFER IN ORTHOPAEDICS
The evolution of reconstructive microsurgery has revolutionized the orthopaedic surgeon's ability to salvage severely traumatized extremities, restore function following brachial plexus injuries, and provide robust soft tissue coverage for massive composite defects. Among the armamentarium of available donor sites, the Gracilis and Rectus Abdominis muscles remain the undisputed workhorse flaps.
The gracilis muscle is highly favored for free functioning muscle transfers (FFMT) due to its reliable neurovascular anatomy, expendable nature, and excellent excursion properties, making it ideal for restoring finger flexion or elbow flexion. Conversely, the rectus abdominis muscle provides a massive volume of well-vascularized tissue, making it the premier choice for covering large, complex defects such as Gustilo-Anderson Type IIIB tibial fractures or extensive pelvic resections.
This comprehensive guide details the precise surgical anatomy, biomechanical considerations, and step-by-step operative dissections required to safely harvest both the gracilis and rectus abdominis muscles.
PART I: GRACILIS MUSCLE TRANSFER
Indications and Biomechanics
The gracilis is a Mathes and Nahai Type II muscle flap, characterized by a single dominant vascular pedicle and several minor secondary pedicles. Its parallel fiber architecture allows for significant excursion, making it biomechanically ideal for functional restoration.
Primary Indications:
* Free Functioning Muscle Transfer (FFMT): Restoration of elbow flexion (e.g., Steindler flexorplasty alternative in brachial plexus palsy) or digital flexion/extension (e.g., Volkmann’s ischemic contracture).
* Soft Tissue Coverage: Small to medium-sized defects of the distal third of the lower extremity, heel, or upper extremity.
* Facial Reanimation: Microvascular transfer for long-standing facial nerve palsy.
Surgical Anatomy
- Origin: The anterior margins of the lower half of the pubic symphysis and the upper half of the pubic arch.
- Insertion: The medial surface of the proximal tibia, distal to the condyle, forming the pes anserinus along with the sartorius and semitendinosus.
- Vascular Supply: The dominant pedicle is the ascending branch of the medial circumflex femoral artery (MCFA), which enters the muscle approximately 8 to 10 cm distal to the pubic tubercle. The pedicle is typically 1.5 to 2.0 mm in diameter and is accompanied by two venae comitantes.
- Innervation: The anterior branch of the obturator nerve. It enters the muscle obliquely, slightly proximal to the main vascular pedicle, and contains 2 to 4 fascicles, allowing for potential splitting if dual innervation is required at the recipient site.
Preoperative Preparation and Positioning
- Positioning: The patient is placed in the supine position. The donor leg is abducted, externally rotated, and the knee is slightly flexed (the "frog-leg" position).
- Preparation: The entire lower extremity from the iliac crest to the toes is prepped and draped to allow for intraoperative manipulation. A sterile tourniquet may be applied proximally but is often left uninflated to facilitate identification of the vascular pedicle via pulsation.
- Marking: Draw a straight line from the pubic tubercle to the medial epicondyle of the femur. The gracilis muscle lies immediately posterior to this axis.
Step-by-Step Surgical Dissection
The harvest of the gracilis muscle requires meticulous dissection to preserve its neurovascular bundle and prevent ischemic injury or denervation.
- Incision and Identification: Make a short longitudinal incision in the distal thigh along the posterior border of the marked axis. Deepen the incision through the subcutaneous tissue and fascia lata. Identify the gracilis tendon by blunt dissection. It is located posterior to the sartorius and anterior to the semimembranosus.
- Distal Tenotomy: Once the tendon is isolated, apply distal traction. Section the tendon distally after determining the exact length needed for the recipient site reconstruction.
- Muscle Mobilization: Extend the incision proximally as needed, or use a minimally invasive endoscopic approach if only a short muscle belly is required. Elevate the muscle belly from distal to proximal, separating it from the adductor longus anteriorly and the adductor magnus posteriorly. Ligate the minor distal vascular pedicles using hemoclips or bipolar electrocautery.
Surgical Warning: During proximal elevation, be acutely aware of the dominant neurovascular pedicle entering the deep surface of the muscle approximately 10 cm distal to the pubic tubercle. Overzealous traction can cause avulsion of the medial circumflex femoral vessels.
- Pedicle Isolation: Identify the dominant vascular pedicle (MCFA) and the anterior branch of the obturator nerve. Dissect the pedicle proximally toward its origin from the profunda femoris to maximize pedicle length (typically 6 to 8 cm can be achieved).
- In Situ Preservation:
Clinical Pearl: To avoid displacement, contraction, or spasm of the muscle, suture it loosely in situ. Leave it attached to the remaining pedicle and origin until the recipient site (e.g., the forearm or brachial plexus) is fully prepared and the recipient vessels are isolated.
- Final Harvest: Once the recipient site is ready, section the muscular origin at the pubis. Ligate and section the neurovascular pedicle using micro-clips or fine silk ties. Deliver the muscle unit immediately to the recipient site to minimize ischemia time.
PART II: RECTUS ABDOMINIS MUSCLE FLAP
Indications and Biomechanics
The rectus abdominis is a Mathes and Nahai Type III muscle flap, possessing two dominant vascular pedicles (the superior and deep inferior epigastric arteries). It is highly versatile, capable of being utilized as a pedicled flap (superiorly or inferiorly based) or as a free tissue transfer.
Primary Indications:
* Pedicled Flap (Superiorly Based): Sternal wound reconstruction, breast reconstruction (TRAM flap).
* Pedicled Flap (Inferiorly Based): Pelvic, perineal, and groin defect reconstruction following tumor extirpation or trauma.
* Free Flap: Massive extremity trauma (e.g., Gustilo IIIB/IIIC fractures), extensive soft tissue avulsions, and chronic osteomyelitis coverage.
Surgical Anatomy of the Rectus Abdominis
Understanding the complex fascial and vascular anatomy of the anterior abdominal wall is paramount to a successful harvest and the prevention of postoperative ventral hernias.
- Muscle Architecture: The rectus abdominis is a long, flat muscle extending from the pubic symphysis to the xiphoid process and the 5th-7th costal cartilages.
- Tendinous Intersections: The muscle is divided into four or five transverse sections by tendinous intersections that adhere tightly to the anterior rectus sheath. One intersection occurs at the level of the umbilicus, another at the inferior end of the xiphoid process, a third occurs at a point equidistant between these two, and a fourth can occasionally occur between the umbilicus and the pubis.
- The Rectus Sheath and Arcuate Line: The muscle is enclosed within the rectus sheath throughout its length. However, the posterior wall of the sheath is complete distally only as far as the arcuate line of Douglas, which is located approximately halfway between the umbilicus and the pubis. Inferior to the arcuate line, the posterior wall is composed solely of transversalis fascia and subserous fascia, making this area particularly vulnerable to herniation if the anterior sheath is not meticulously repaired.
- Vascular Supply (Deep Inferior Epigastric Artery - DIEA): The DIEA arises from the external iliac artery just deep to the inguinal canal. It is a robust vessel, measuring 3 to 4 mm in diameter at its origin, and is accompanied by two venae comitantes. It pierces the transversalis fascia and enters the rectus sheath lateral and inferior to the arcuate line. It then enters the rectus abdominis muscle along its deep (posterior) surface, courses superiorly, and ramifies with branches from the superior epigastric artery.
- Innervation: The muscle receives segmental motor innervation from the 7th through 12th intercostal nerves, which enter the muscle laterally.
Surgical Technique 63-22: Rectus Abdominis Harvest
The following technique describes the harvest of the rectus abdominis muscle, typically based on the deep inferior epigastric pedicle for free tissue transfer.
1. Patient Positioning and Preparation
* Position the patient supine on the operating table.
* Prepare and drape the entire abdomen from the costal margins above to the pubic tubercle below, extending laterally to the mid-axillary lines. Ensure a Foley catheter is placed to decompress the bladder prior to making the inferior incision.
2. Incision and Exposure
* Make a longitudinal paramedian incision from just below the costal margin extending distally to 3 to 4 cm proximal to the pubic tubercle.
- Deepen the incision through the subcutaneous fat and Scarpa's fascia to expose the anterior rectus sheath. Maintain strict hemostasis using electrocautery.
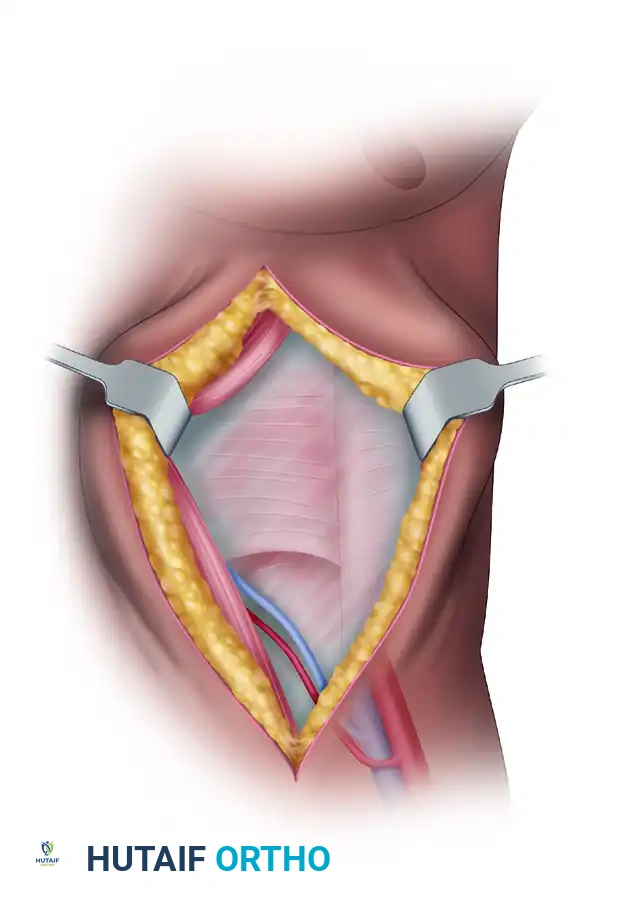
3. Opening the Anterior Rectus Sheath
* Incise the anterior rectus sheath longitudinally, slightly medial to the midline of the muscle belly.
* Carefully elevate the anterior sheath off the muscle. This requires sharp dissection at the level of the tendinous intersections, as the muscle is intimately fused to the anterior sheath at these transverse bands.
Surgical Warning: Do not use excessive electrocautery when separating the tendinous intersections from the anterior sheath, as thermal injury can damage the underlying muscle fibers and compromise the flap's viability.
4. Muscle Mobilization and Nerve Ligation
* Once the anterior surface is completely exposed, begin mobilizing the lateral border of the muscle.
* Identify the segmental intercostal nerves (T7-T12) entering the lateral aspect of the muscle. For a free tissue transfer intended for soft tissue coverage (non-functional), these nerves must be ligated and divided.
5. Pedicle Isolation (Deep Inferior Epigastric Artery)
* Retract the muscle medially to expose its posterior surface.
* Identify the arcuate line. Inferior to this line, carefully dissect the areolar tissue to locate the deep inferior epigastric artery and its accompanying venae comitantes.
- Trace the pedicle proximally toward its origin at the external iliac vessels. The pedicle is seen entering the posterior aspect of the muscle within the inferior lateral portion of the sheath.
- Clear the pedicle of surrounding lymphatic and adipose tissue to maximize length and prepare the vessels for microvascular anastomosis.
6. Superior Ligation and Flap Elevation
* Divide the muscle superiorly at the costal margin. Ligate the superior epigastric vessels securely using suture ligatures or medium surgical clips.
* Elevate the muscle from superior to inferior, separating it from the posterior rectus sheath (above the arcuate line) and the transversalis fascia (below the arcuate line).
* Divide the muscle inferiorly just above the pubic symphysis, leaving the flap attached solely by the deep inferior epigastric pedicle.
* Allow the flap to perfuse in situ until the recipient site is fully prepared. Once ready, ligate the DIEA and venae comitantes, and transfer the flap.
7. Donor Site Closure
* Closure of the abdominal wall is the most critical step to prevent postoperative ventral herniation.
* Achieve meticulous hemostasis within the rectus sheath.
* Close the anterior rectus sheath using heavy, non-absorbable or slowly absorbable monofilament sutures (e.g., #1 PDS or Prolene) in a continuous or interrupted figure-of-eight fashion.
* If the anterior sheath is deficient or under excessive tension, reinforce the closure with a synthetic or biologic mesh inlay.
* Place a closed-suction drain superficial to the fascial repair, and close the subcutaneous tissue and skin in layers.
POSTOPERATIVE PROTOCOLS AND FLAP MONITORING
The success of a free functioning muscle transfer or a pedicled muscle flap relies heavily on rigorous postoperative management.
1. Flap Monitoring:
* Clinical Assessment: The muscle should be monitored hourly for the first 24 to 48 hours. Assess for color, turgor, capillary refill (if a skin paddle is included), and surface bleeding upon needle prick. A healthy muscle flap should appear beefy red and bleed bright red blood when gently pricked.
* Instrumental Monitoring: Implantable venous Doppler probes or surface handheld Dopplers are highly recommended to continuously monitor arterial inflow and venous outflow. Loss of the venous signal often precedes arterial thrombosis and requires immediate surgical re-exploration.
2. Patient Positioning and Environment:
* Maintain the patient in a warm ambient room temperature (>24°C) to prevent peripheral vasospasm.
* The reconstructed extremity should be elevated to promote venous drainage and reduce edema, but avoid extreme elevation that could compromise arterial inflow.
* Ensure the limb is immobilized in a custom splint to prevent tension or shearing forces across the microvascular anastomoses and the muscle inset.
3. Medical Management:
* Hydration: Maintain aggressive intravenous hydration to ensure high cardiac output and optimal flap perfusion.
* Anticoagulation: Protocols vary by institution, but many microsurgeons utilize a combination of low-molecular-weight dextran, aspirin (81 mg daily), or subcutaneous heparin to prevent microvascular thrombosis.
* Analgesia: Adequate pain control is essential to prevent sympathetic nervous system activation, which can lead to detrimental peripheral vasoconstriction.
COMPLICATION MANAGEMENT
Despite meticulous surgical technique, complications can arise. Early recognition and intervention are paramount.
- Vascular Thrombosis: The most dreaded complication of free tissue transfer. Venous congestion (flap appears dark, swollen, with rapid dark bleeding on prick) is more common than arterial occlusion (flap appears pale, empty, with no bleeding). Both require emergent return to the operating room for anastomotic revision. The salvage rate drops precipitously if re-exploration is delayed beyond 4 to 6 hours.
- Donor Site Morbidity:
- Gracilis: Generally well-tolerated with minimal functional deficit. Patients may experience transient medial thigh numbness due to neuropraxia of the medial femoral cutaneous nerve.
- Rectus Abdominis: Ventral hernia or abdominal wall bulge is the most significant risk. Strict adherence to fascial closure techniques and the judicious use of mesh reinforcement mitigate this risk. Patients must be counseled to avoid heavy lifting or Valsalva maneuvers for at least 8 to 12 weeks postoperatively.
- Hematoma: Accumulation of blood under the flap can compress the vascular pedicle. Drains must be maintained until output is minimal, and any expanding hematoma warrants surgical evacuation.
Mastery of the gracilis and rectus abdominis muscle transfers provides the orthopaedic reconstructive surgeon with powerful tools to address the most challenging soft tissue and functional deficits. Through precise anatomical knowledge, meticulous microvascular technique, and vigilant postoperative care, excellent limb salvage and functional outcomes can be reliably achieved.
You Might Also Like

