Disorders of the Patella: Diagnosis and Surgical Management
Key Takeaway
Disorders of the patella encompass a spectrum of pathologies including osteochondritis dissecans, dorsal defects, bipartite patella, and chondromalacia. Effective management requires a profound understanding of patellofemoral biomechanics and precise radiographic evaluation. This comprehensive guide details evidence-based diagnostic protocols, conservative management strategies, and advanced surgical techniques—such as the Ogata subperiosteal release—to optimize functional outcomes and restore extensor mechanism integrity in the orthopedic patient.
INTRODUCTION TO PATELLAR PATHOLOGY
The patella, the largest sesamoid bone in the human body, plays a critical biomechanical role in the extensor mechanism of the knee. By displacing the quadriceps tendon anteriorly, it significantly increases the moment arm of the extensor apparatus, thereby enhancing the mechanical advantage of the quadriceps muscle group. However, this unique anatomical arrangement subjects the patellofemoral joint to immense compressive and shear forces, predisposing it to a distinct spectrum of developmental, osteochondral, and degenerative disorders.
A profound understanding of patellofemoral kinematics, coupled with precise radiographic interpretation, is essential for the orthopedic surgeon. This masterclass delineates the etiology, clinical presentation, and evidence-based surgical management of primary patellar disorders, including osteochondritis dissecans, dorsal defects, bipartite patella, and chondromalacia.
OSTEOCHONDRITIS DISSECANS OF THE PATELLA
Pathophysiology and Demographics
Osteochondritis dissecans (OCD) of the patella is a relatively rare entity compared to its counterpart in the femoral condyles, and it typically carries a more guarded prognosis. The condition is characterized by the focal separation of an osteochondral fragment from the underlying subchondral bone, secondary to localized ischemia or repetitive microtrauma.
OCD of the patella predominantly manifests in the second and third decades of life. Topographically, lesions are most frequently localized to the lower half of the patella, particularly along the median ridge and paramedial areas. Notably, bilateral involvement is observed in up to one-third of patients, necessitating a thorough evaluation of the contralateral knee even in unilateral presentations.
Clinical Pearl: Always differentiate true osteochondritis dissecans from a benign dorsal defect of the patella. Misdiagnosis can lead to unwarranted surgical intervention in a self-limiting condition.
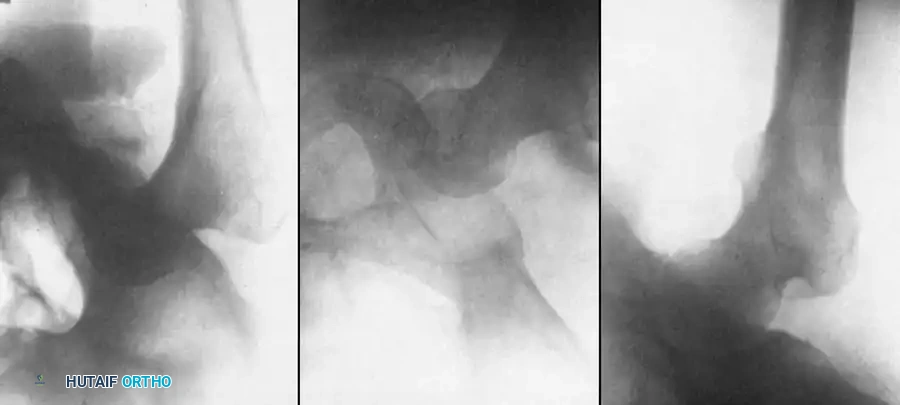
Radiographic Evaluation
Standard anteroposterior (AP) and lateral radiographs may fail to adequately delineate the lesion.
* Lateral Radiograph: The lesion is best visualized on a slightly overexposed lateral radiograph, which helps penetrate the dense subchondral bone.
* Axial ("Skyline") View: This is the definitive projection to determine whether the osteochondral defect is situated within the medial or lateral facet.
* Magnetic Resonance Imaging (MRI): MRI is the gold standard for assessing the stability of the osteochondral fragment, evaluating the integrity of the overlying articular cartilage, and identifying subchondral fluid indicative of instability.
Management Algorithms
Treatment principles mirror those established for OCD of the distal femur; however, patellar lesions are frequently complicated by surrounding chondromalacia that extends well beyond the peripheral margins of the avascular crater.
- Conservative Management: Indicated for stable lesions with intact articular cartilage, particularly in skeletally immature patients. Immobilization, activity modification, and protected weight-bearing can yield spontaneous healing.
- Surgical Intervention: Required for unstable lesions, detached fragments, or failure of conservative therapy.
- Fragment Excision and Curettage: For unsalvageable fragments, excision followed by curettage and marrow stimulation (microfracture or drilling) of the crater is performed. Arandes-Renu et al. demonstrated that excision and drilling yielded excellent long-term results with no restriction of activity at a 4-year follow-up.
- Internal Fixation: Salvageable fragments can be stabilized using retrograde or antegrade bioabsorbable pins or Herbert screws, as described by Marandola and Prietto.
- Patellar Preservation: Rarely is the surrounding chondromalacia so extensive as to necessitate a patellectomy. The patella must almost always be preserved to maintain extensor biomechanics.
DORSAL DEFECT OF THE PATELLA
Etiology and Characteristics
First described by Caffey in 1972, a dorsal defect of the patella is a benign, circular, well-circumscribed radiolucent lesion, typically measuring approximately 1 cm in diameter. It invariably abuts the articular cartilage and is characteristically located in the superolateral quadrant of the patella.
The exact etiology remains debated, though the prevailing consensus identifies it as a variant of normal ossification. Van Holsbeeck et al. proposed a traction injury hypothesis, noting a strong association between bipartite patella and dorsal defects. They postulated that repetitive traction at the insertion of the vastus lateralis muscle during the critical phases of patellar ossification leads to this localized defect.
Differential Diagnosis
In approximately 50% of cases, the lesion is entirely asymptomatic and discovered incidentally. When evaluating a lytic lesion in the patella, the differential diagnosis must include:
* Osteochondritis dissecans
* Brodie abscess (subacute osteomyelitis)
* Eosinophilic granuloma
* Enchondroma
* Osteoid osteoma
* Metastatic disease (in older demographics)
Surgical Warning: The paramount clinical objective is differentiating a dorsal defect from OCD. Dorsal defects are self-limiting and heal spontaneously. Unnecessary curettage or bone grafting should be strictly avoided unless the lesion is highly symptomatic and refractory to prolonged conservative care.
BIPARTITE PATELLA
Classification and Biomechanics
A bipartite patella represents a failure of secondary ossification centers to fuse with the primary patellar mass. It is bilateral in approximately 40% of cases. Saupe classified bipartite patellae into three distinct morphological types based on the location of the accessory fragment:
* Type I (5%): Located at the inferior pole. Often associated with Sinding-Larsen-Johansson syndrome.
* Type II (20%): Located along the entire lateral border. Must be differentiated from a nonunion of a longitudinal patellar fracture.
* Type III (75%): The most common variant, presenting as an elliptical fragment in the superolateral quadrant.
Clinical Presentation and Diagnosis
The vast majority of bipartite patellae are asymptomatic. When pain occurs, it is typically the result of overuse, repetitive microtrauma, or, rarely, acute traumatic separation of the synchondrosis.
Diagnostic Imaging:
* Squatting Skyline View: Ishikawa et al. described a dynamic radiographic test. A standard skyline view is compared to a skyline view taken with the patient in a squatting, weight-bearing position. The test is positive for symptomatic nonunion if the separation between the fragments widens during the squat.
* MRI: Kavanagh et al. demonstrated that bone marrow edema localized strictly within the bipartite fragment and the adjacent synchondrosis is the hallmark MRI finding of a symptomatic lesion.
Conservative and Surgical Management
Initial management of a painful bipartite patella is strictly non-operative, focusing on activity modification, NSAIDs, and a short-arc quadriceps strengthening program. Immobilization in extension for 3 to 4 weeks is highly effective for relieving symptoms caused by repetitive microtrauma.
Operative intervention is reserved for refractory cases or acute, displaced traumatic separations.
* Fragment Excision: Excision of the small, nonarticular fragment (especially in Type III lesions) yields excellent results. Arthroscopic excision has been shown to reduce morbidity compared to open techniques.
* Lateral Release: Mori et al. and Adachi et al. demonstrated that releasing the contracted lateral soft tissues (vastus lateralis) alleviates the traction forces on the fragment, resolving pain and allowing a rapid return to sports.
🔪 Surgical Technique: Ogata Subperiosteal Release
Ogata described a highly effective subperiosteal release of the lateral quadriceps mechanism. This technique detaches the vastus lateralis insertion from the painful fragment while preserving the continuity of the tendon-periosteum complex to the main patella. This relieves muscle traction without inducing a mediolateral tracking imbalance.
Step-by-Step Procedure:
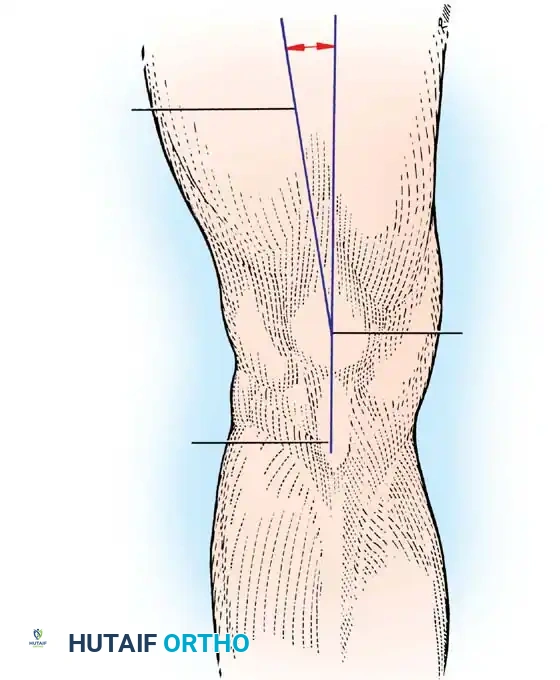
- Incision and Exposure: Following diagnostic arthroscopy, make an oblique skin incision over the distal portion of the vastus lateralis tendon. Extend this incision just distal to the midportion of the separated bipartite area.
Fig 1: Oblique skin incision over the distal vastus lateralis tendon, targeting the superolateral bipartite fragment.
- Tendon Splitting: Identify the vastus lateralis tendon, which is frequently hypertrophied in these patients. Split the tendon longitudinally along its middle fibers.
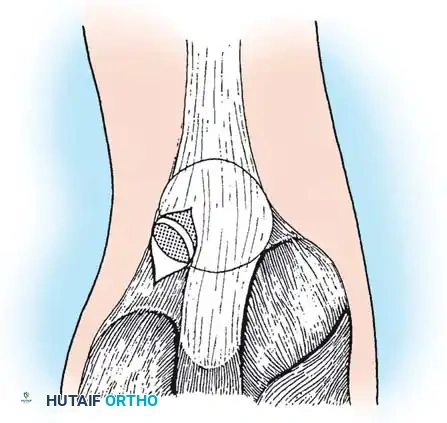
Fig 2: The vastus lateralis tendon is split, and the insertion to the painful patellar fragment is detached subperiosteally.
- Subperiosteal Detachment: Carefully detach the tendinous insertion to the painful bipartite fragment in a subperiosteal plane. It is critical to preserve the continuity of the tendinous expansion to the main mass of the patella.
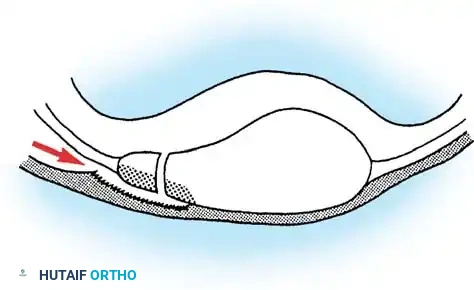
- Denuding the Fragment: Dissect the tendon-periosteum complex and sharply denude the smaller fragment completely.
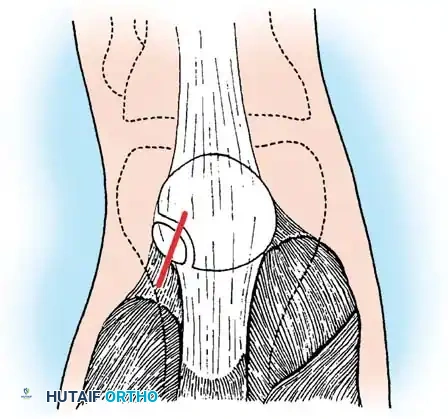
Fig 3: The fragment is relieved from muscle traction. The continuity of the extensor mechanism is maintained, preventing iatrogenic patellar instability.
- Stability Assessment: Apply bending stress to the denuded fragment using the thumb and index finger. Observe the synchondrosis. If the groove widens significantly, the fragment is grossly unstable and should be excised. If it demonstrates minimal mobility, it may be left in situ, as the traction relief will promote spontaneous union.
- Closure: Repair the longitudinal split in the vastus lateralis with No. 0 absorbable sutures and close the subcutaneous tissue and skin in a standard layered fashion.
Postoperative Protocol:
The patient is permitted immediate full weight-bearing in a hinged knee brace or splint locked in full extension. Range-of-motion exercises (0-90 degrees) are initiated at postoperative day 4 or 5. The extension splint is discontinued at 1 to 2 weeks. Return to competitive sports is permitted at 4 to 6 weeks, contingent upon the resolution of symptoms and restoration of quadriceps symmetry.
CHONDROMALACIA OF THE PATELLA
Nomenclature and Pathology
Introduced by Aleman in 1928, the term chondromalacia patellae specifically denotes the pathological softening, fibrillation, and degeneration of the articular cartilage of the patella.
Surgical Warning: Chondromalacia is a strict pathological and arthroscopic diagnosis, not a clinical syndrome. It should not be used synonymously with "anterior knee pain" or "patellofemoral pain syndrome." Patients with severe anterior knee pain may have pristine cartilage, while those with advanced chondromalacia may be entirely asymptomatic.
The fundamental pathophysiology of chondromalacia differs drastically from primary osteoarthritis. Osteoarthritis initiates at the superficial articular surface with the loss of transverse collagen fibers. Conversely, chondromalacia begins as basal degeneration—a disorder originating in the deep layers of the cartilage.
Histological and Biomechanical Progression
The initial lesion involves a biochemical degradation of the ground substance, specifically a marked decrease in sulfated mucopolysaccharides. Histologically, this is demonstrated by a loss of basophilia on hematoxylin and eosin (H&E) staining. During this early phase, the superficial articular surface remains macroscopically smooth and intact, though the cartilage feels softened or "boggy" to arthroscopic probing.
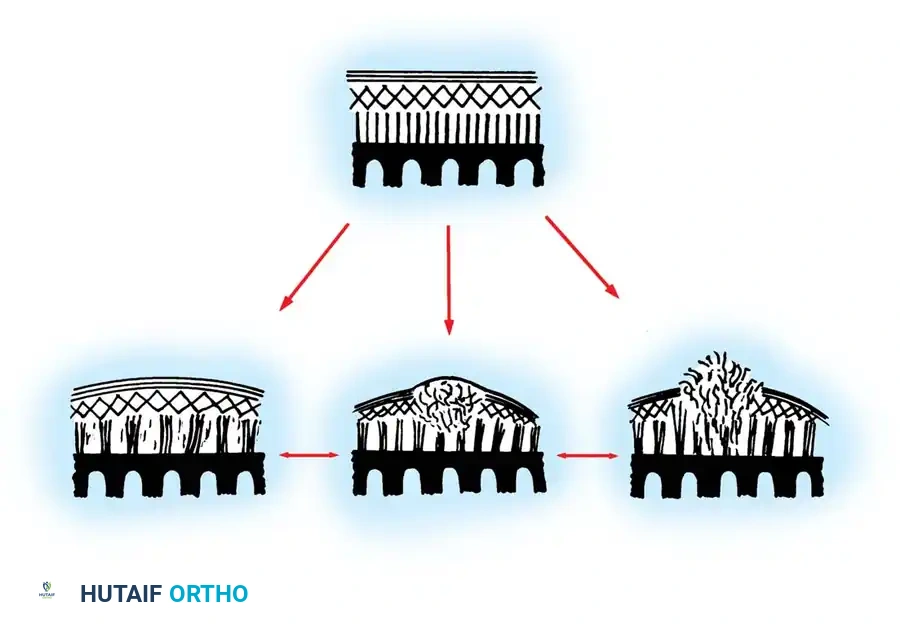
Fig 4: Stages of basal degeneration. The pathology begins deep within the cartilage matrix (fasciculation) before progressing to a macroscopic "blister" and eventual surface rupture.
Topographically, Goodfellow et al. mapped these lesions and found they predominantly occur in two specific non-contact areas:
1. An area approximately 1 cm in diameter astride the median ridge separating the medial and lateral facets.
2. An area straddling the inferior portion of the central ridge.
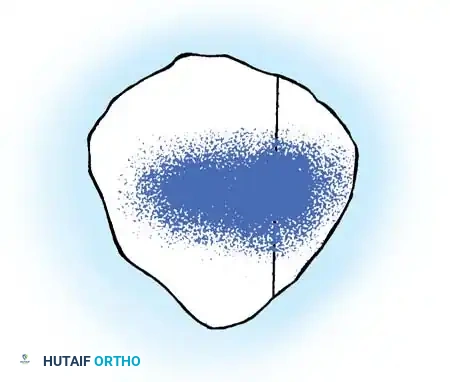
Fig 5: Topographical map of patellar chondromalacia. Lesions are most severe in the central zone, extending equally onto the medial and lateral facets.
While these areas are typically non-contact zones during standard gait, extreme ranges of knee flexion bring these softened areas into direct articulation with the femoral trochlea. Because the biochemically degraded ground substance is mechanically inadequate to support the collagen framework, the intermediate zone of collagen fibers begins to break up under shear stress. This leads to the next phase of degeneration: macroscopic fibrillation, blistering, and eventual full-thickness cartilage loss down to the subchondral bone.
Advanced Surgical Management: Extensor Mechanism Realignment
When conservative measures (physical therapy, McConnell taping, intra-articular injections) fail, and the patient develops severe, symptomatic, full-thickness chondromalacia or localized patellofemoral osteoarthritis, surgical offloading of the affected articular facets is indicated.
For advanced distal and lateral facet chondromalacia, anteriorization and medialization of the tibial tubercle (e.g., Fulkerson osteotomy or Maquet procedure) is a powerful biomechanical intervention.
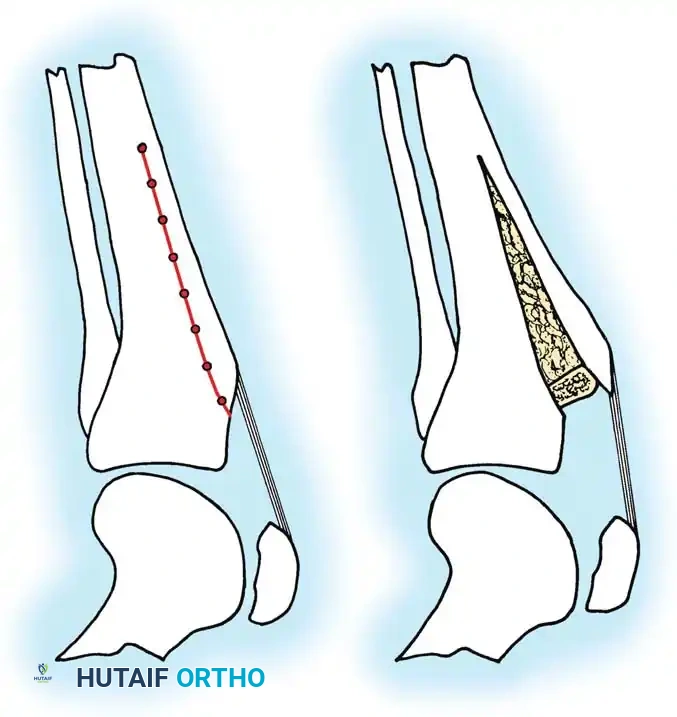
Fig 6: Tibial Tubercle Osteotomy. By elevating and anteriorizing the tibial tubercle (often utilizing a bone graft or specialized step-cut), the moment arm of the extensor mechanism is increased. This significantly decreases the joint reaction forces across the patellofemoral articulation, offloading the areas of severe chondromalacia and providing profound pain relief.
By shifting the mechanical axis of the extensor mechanism, the surgeon effectively transfers the contact stresses from the degenerated cartilage to relatively preserved areas of the patella, thereby restoring functional kinematics and delaying the need for patellofemoral arthroplasty.
You Might Also Like