Operative Management of Ingrown Toenails: A Comprehensive Surgical Guide
Key Takeaway
Onychocryptosis, commonly known as an ingrown toenail, is a painful condition driven by extrinsic pressure and improper nail trimming. Management depends on clinical staging, ranging from conservative cotton-mesh elevation in Stage I to partial or total nail plate avulsion with matrixectomy in Stages II and III. This guide details the relevant nail anatomy, biomechanics, and step-by-step surgical techniques required to achieve definitive resolution and minimize recurrence.
Disorders of Nails and Skin: Onychocryptosis
Ingrown toenail, medically termed onychocryptosis or unguis incarnatus, is one of the most frequent nail disorders encountered by orthopedic surgeons and foot and ankle specialists. While often perceived as a minor ailment, improper management can lead to chronic pain, recurrent infections, and significant morbidity, particularly in diabetic or immunocompromised patients. A thorough understanding of nail anatomy, biomechanics, and evidence-based surgical techniques is paramount for achieving definitive resolution.
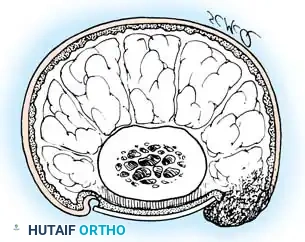
Anatomy of the Normal Nail Complex
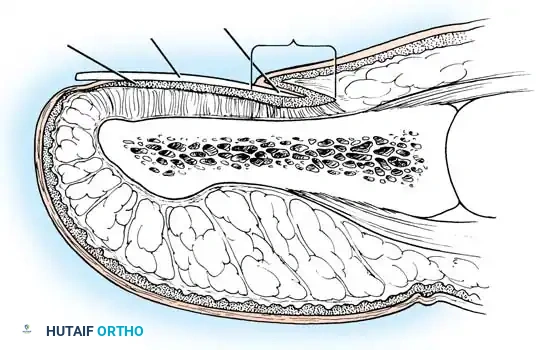
To perform effective surgical ablation and prevent recurrence, the surgeon must possess an intimate understanding of the perionychial anatomy. The normal nail complex consists of several distinct anatomical and functional components:
- Nail Root: The proximal portion of the nail plate that lies embedded beneath the skin.
- Nail Body: The exposed, visible portion of the nail plate, composed of dense, compacted keratin.
- Nail Walls (Labia Ungues): The cutaneous margins that overhang and border the two lateral edges of the nail body.
- Eponychium (Proximal Nail Fold): The distal extension of the stratum corneum of the skin that covers the nail root.
- Cuticle: The distal, acellular edge of the eponychium that forms a seal between the skin and the nail plate.
- Nail Bed: The continuation of the stratum germinativum upon which the nail plate rests.
- Lunula: The white, opaque, semilunar area visible at the base of the nail, representing the distal extent of the germinal matrix.
- Hyponychium: The horny thickening of the skin at the distal margin of the nail, serving as a barrier against subungual infection.
The Matrix Complex
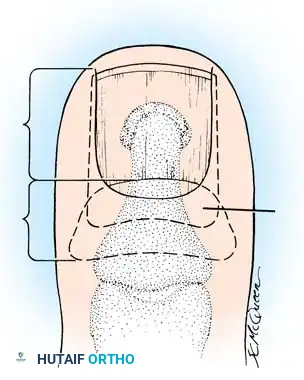
The matrix consists of several layers of cells derived from the stratum germinativum and is functionally divided into two components: the sterile matrix and the germinal matrix. In the skeletally mature foot, the germinal matrix extends from just distal to the lunula to approximately 5 to 8 mm proximally, lying deep to the eponychium. It is smoother and paler than the sterile matrix, unless the nail has been recently avulsed.
Surgical Warning: The germinal matrix sends microscopic projections into the adjacent soft tissues. Failure to meticulously excise or ablate these lateral horns is the primary cause of recurrent nail spicules following surgery.
The germinal matrix is the primary contributor to the longitudinal growth of the nail plate. While it remains a subject of academic debate whether the eponychium, lateral nail folds, or sterile matrix contribute to longitudinal new growth, extensive clinical and laboratory data (supported by Zaias, Lewis, Samman, Zook, and Heifetz) suggest their contribution is negligible compared to the germinal matrix.

Etiology and Pathomechanics
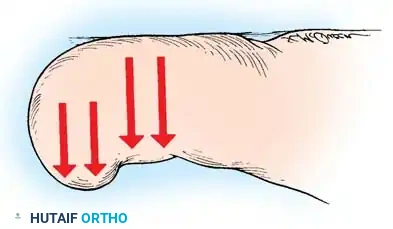
The term "ingrown toenail" is somewhat of a misnomer. It implies that the nail itself is the primary offender, actively growing into the soft tissue. In reality, the pathology is often a soft-tissue problem where the hypertrophied lateral nail fold is pushed into the nail plate.
The condition is exceedingly rare in barefoot populations, underscoring the role of extrinsic pressure. Within the confines of a narrow shoe toe box, the great toe is forced laterally toward the second toe. This generates pressure against the lateral border of the nail, while the shoe itself exerts counter-pressure on the medial side.
When this extrinsic pressure forces the nail fold into the sharp edge of an improperly trimmed nail, the skin is breached. The normal bacterial and fungal flora of the foot enter this micro-wound, initiating a robust inflammatory cascade.
As described by Lapidus, this creates a "bottlenecked, poorly draining abscess," characterized by erythema, edema, hyperhidrosis, and exquisite tenderness. Over time, hypertrophic granulation tissue forms, further inhibiting drainage and exacerbating edema. This vicious cycle renders the nail fold even more vulnerable to extrinsic pressure.


Clinical Staging and Nonoperative Management
Management is dictated by the clinical stage of the disease. Nonoperative management is highly effective in early stages but yields diminishing returns once hypertrophic granulation tissue develops.
Stage I (Inflammatory Stage)
In Stage I, the patient presents with mild erythema, localized swelling, and tenderness along the lateral nail fold. There is no purulent drainage.
Treatment:
The primary goal is to separate the nail plate from the embedded dermis.
* Gently lift the lateral edge of the nail plate.
* Insert a small pledget of nonabsorbent cotton, wool, or acrylic mesh beneath the corner of the nail.
* Prescribe intermittent warm water soaks (10-15 minutes, 3-4 times daily).
* Advise the use of open-toed shoes or wide toe boxes to eliminate extrinsic pressure.
* Educate the patient on proper nail trimming: nails must be cut straight across at right angles to the distal edge, leaving the corners protruding distal to the hyponychium.
With daily replacement of the cotton mesh, Stage I lesions typically resolve within 2 to 3 weeks.

Stage II (Abscess Stage)
Stage II represents an advancement of the inflammatory process. Erythema, edema, and hyperhidrosis intensify. The lateral nail fold bulges over the nail plate, and drainage commences—initially serous, rapidly progressing to purulent and fetid due to polymicrobial colonization. Walking becomes difficult, and shoe wear is often intolerable.
Treatment:
* Remove all constrictive pressure, including hosiery.
* Initiate warm soaks.
* Obtain cultures of the purulent drainage and begin broad-spectrum oral antibiotics (tailored to sensitivities).
* Once acute inflammation and drainage subside, attempt the cotton-lift technique described in Stage I.
* If drainage persists, surgical intervention is indicated.

Stage III (Granulation Stage)
In Stage III, exuberant hypertrophic granulation tissue covers the lateral nail fold, completely inhibiting free drainage. Epithelium begins to creep over the granulations, precluding any conservative attempt to elevate the nail edge. This stage often becomes a chronic, smoldering condition punctuated by acute inflammatory flares.
Treatment:
Nonoperative management is generally futile and associated with high recurrence rates. Surgical management is the definitive standard of care for Stage III lesions.
Preoperative Preparation
Anesthesia:
A digital block is the anesthetic technique of choice. Use 1% to 2% lidocaine or mepivacaine without epinephrine. Introduce a small-gauge needle (25G or 27G) approximately 1 cm distal to the first web space. Ensure that the proper plantar digital nerves and the dorsal sensory branches of the superficial peroneal nerve are completely anesthetized.
Hemostasis:
A bloodless field is critical for identifying the germinal matrix. A sterile Penrose drain or a commercial digital tourniquet is applied to the base of the proximal phalanx.




Operative Management
The operative treatment of ingrown toenails is based on two philosophical approaches: either the nail is the primary offender (requiring nail/matrix removal), or the soft tissues are the primary offender (requiring soft-tissue resection).
Total Nail Plate Removal
Total nail plate removal without concomitant matrixectomy is rarely indicated as a definitive procedure due to high recurrence rates (32% to 78%). It is primarily reserved for severe, circumducting abscesses that involve both lateral folds and the eponychium, where partial removal would fail to provide adequate drainage.
🔪 Surgical Technique 84-1: Total Nail Plate Avulsion
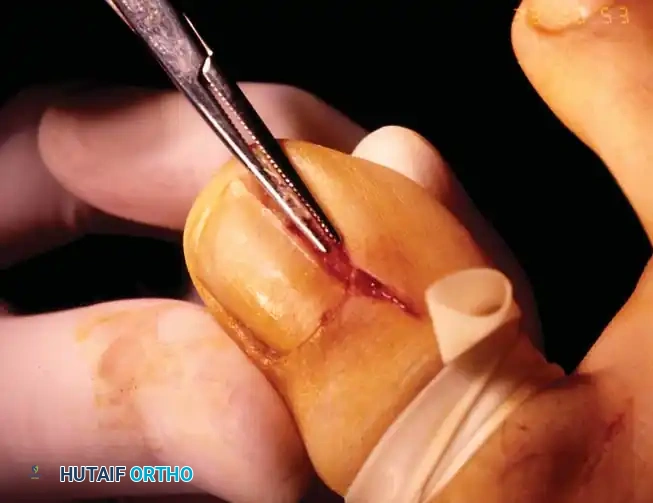
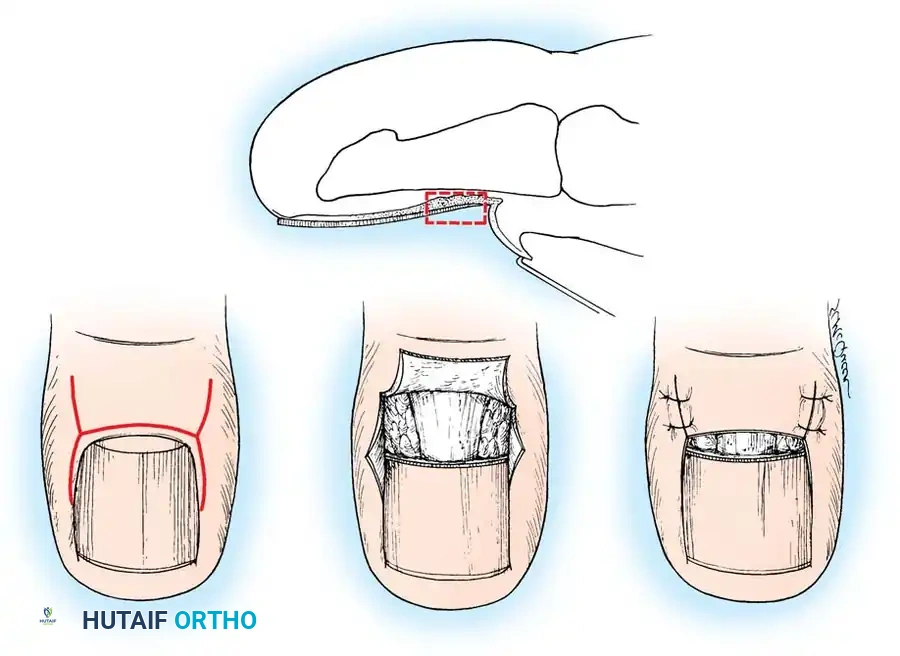
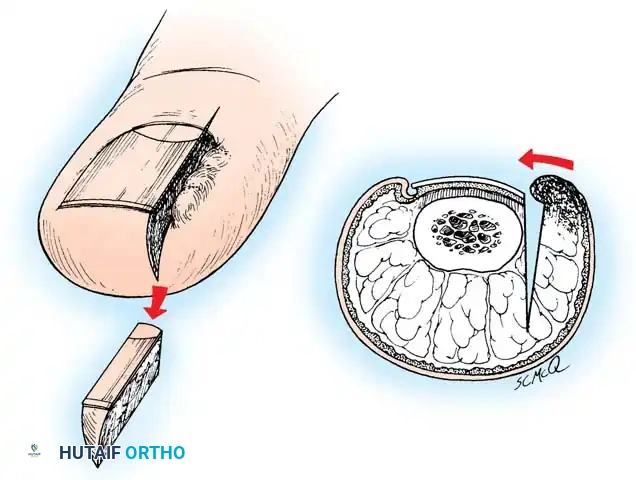
- Elevation: Following adequate anesthesia and exsanguination, pass a straight, thin hemostat or a small, flat nasal elevator beneath the nail plate in the midline. Start at the hyponychium and advance proximally to several millimeters beneath the eponychial fold, adjacent to the lunula.
- Lateral Freeing: Do not sweep the instrument back and forth. Instead, withdraw it and re-insert it in a similar longitudinal manner beneath each lateral margin of the nail, adjacent to the lateral nail folds.
- Extraction: Once the nail is sufficiently loosened, apply a firm, steady distal pull with a heavy hemostat.
- Eponychial Adhesions: If the nail root remains adherent to the eponychium, avoid forceful jerking. Use sharp dissection with a #15 blade between the nail plate and eponychium to gently lift the nail, minimizing iatrogenic damage to the underlying germinal matrix.
Aftertreatment for Total Avulsion:
Apply a nonadherent, single-layer dressing (e.g., Adaptic or Xeroform) to the exposed nail bed, followed by a gently wrapped compression bandage. Elevate the foot for 24 hours. Remove the dressing and commence warm soaks. Avoid constricting hosiery or shoes for 1 week.
Clinical Pearl: Forewarn the patient that the nail requires 4 to 6 months to regenerate completely. Furthermore, multiple total avulsions significantly increase the risk of developing an upward-turned deformity of the distal nail bed and pulp.



Partial Nail Plate Removal
Partial nail plate removal is a less morbid alternative, particularly attractive in adolescents where permanent alteration of nail appearance is undesirable. However, the recurrence rate remains high if the matrix is not addressed.
🔪 Surgical Technique 84-2: Partial Nail Plate Avulsion
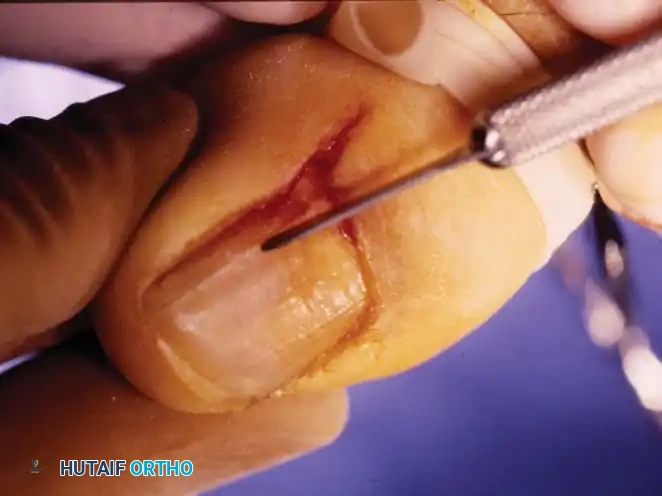
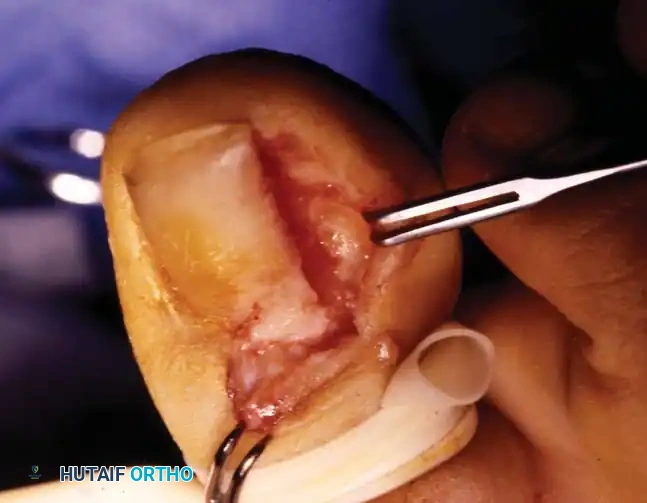
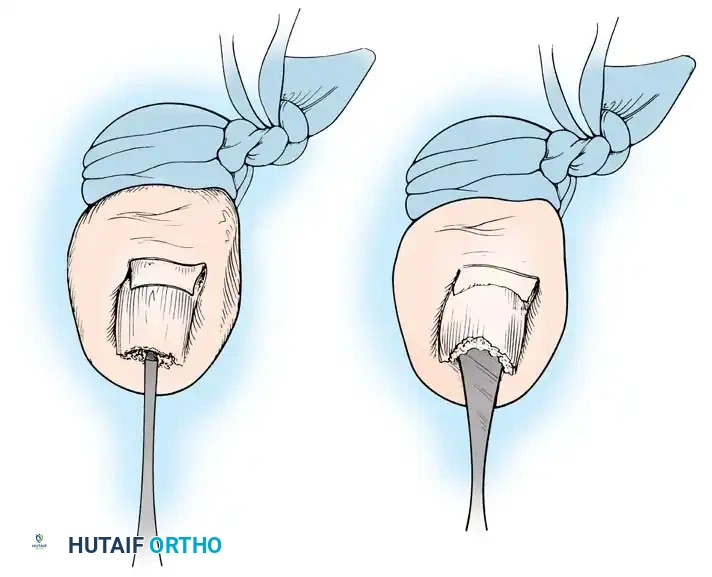
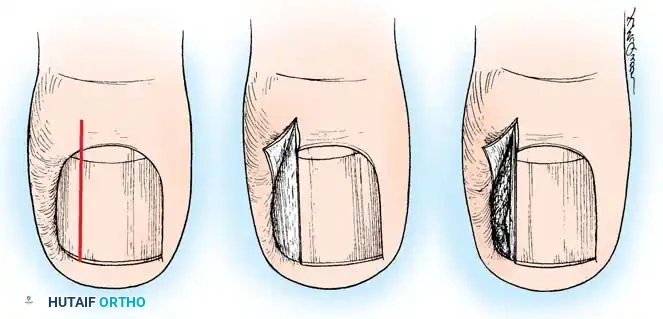
- Elevation: Lift the lateral fourth of the nail from its bed using a small, angled probe or one arm of a narrow, smooth hemostat. Avoid lifting too firmly to prevent detaching the central nail from its bed.
- Incision: Using heavy, straight scissors, cut the nail plate longitudinally while lifting the lateral fourth. A curved tip on the scissors helps prevent scoring the underlying matrix.
- Proximal Extension: The incision must extend to the absolute proximal end of the nail plate, deep beneath the eponychium.
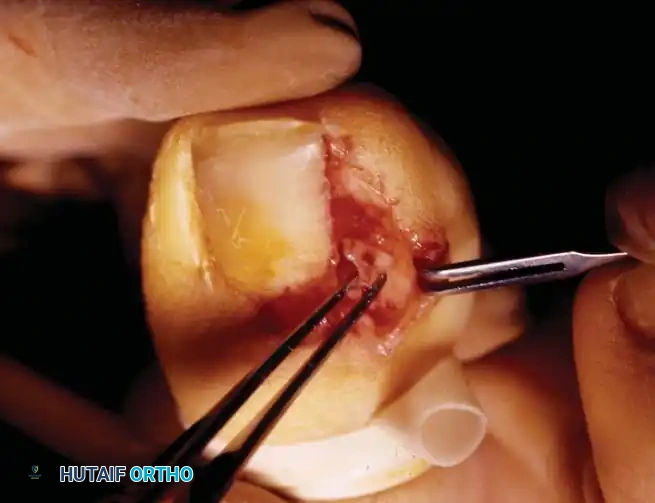
- Debridement: Remove the offending lateral nail spike. Gently scrape away the hypertrophic granulation tissue with a scalpel, or elliptically excise the hypertrophied portion of the lateral nail fold.

Aftertreatment for Partial Avulsion:
Similar to total avulsion, but patients can typically transition to a closed, wide toe box shoe by the third or fourth postoperative day. Counsel parents that inadvertent laceration of the matrix during scissor insertion can lead to permanent longitudinal nail deformities.


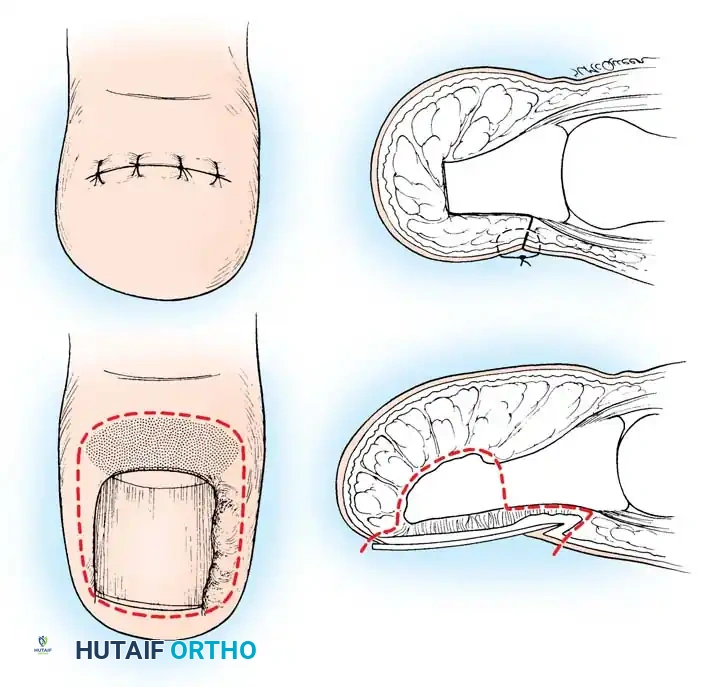
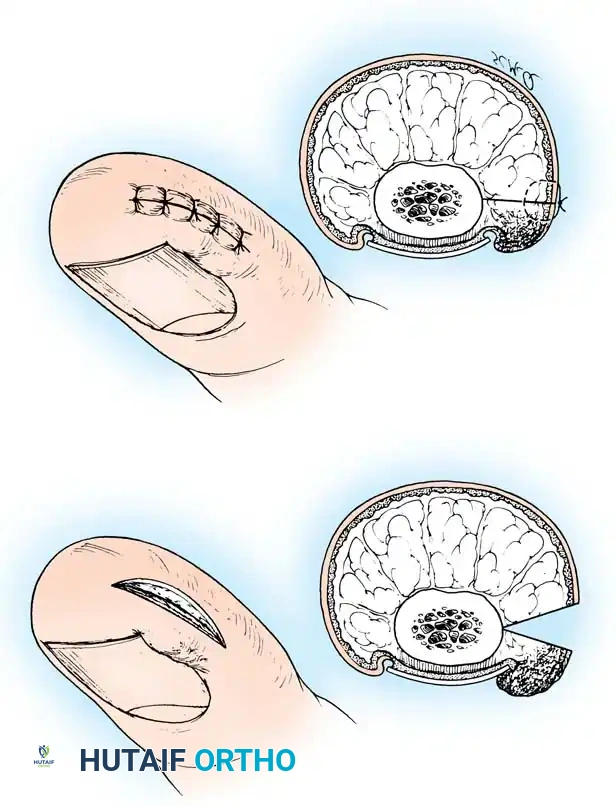
Partial Nail Plate and Matrix Removal (The Winograd Procedure)
Described by Winograd in 1929, the partial nail plate avulsion combined with surgical matrixectomy remains the gold standard for definitive management of Stage II and Stage III ingrown toenails. By excising the lateral horn of the germinal matrix, longitudinal growth of the offending nail border is permanently arrested.
🔪 Surgical Technique: The Winograd Procedure
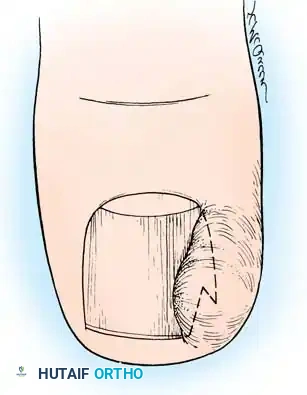
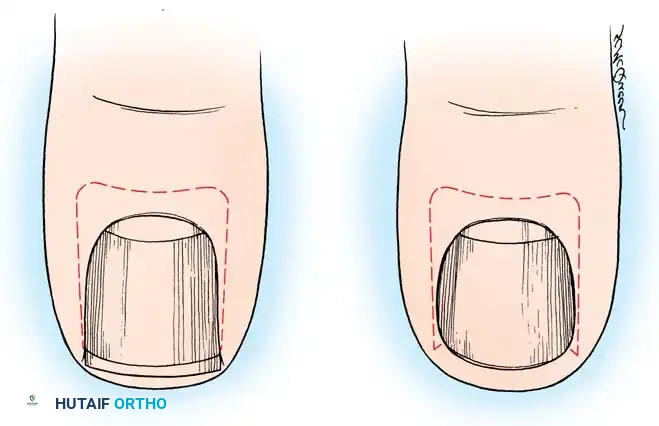
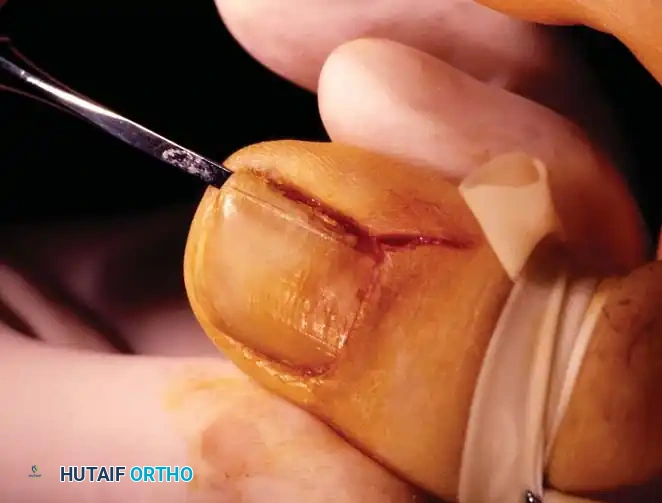
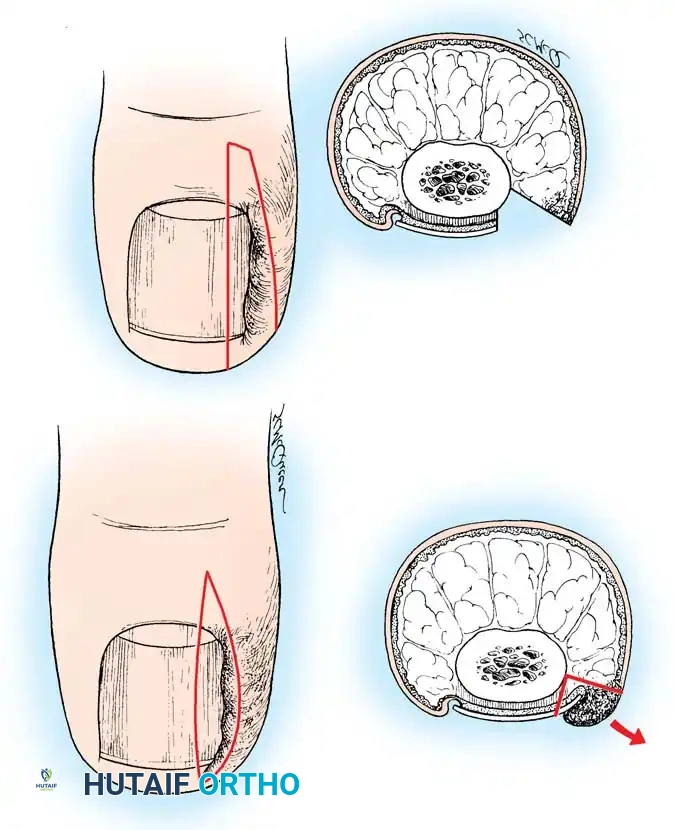
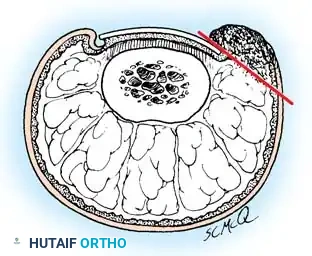
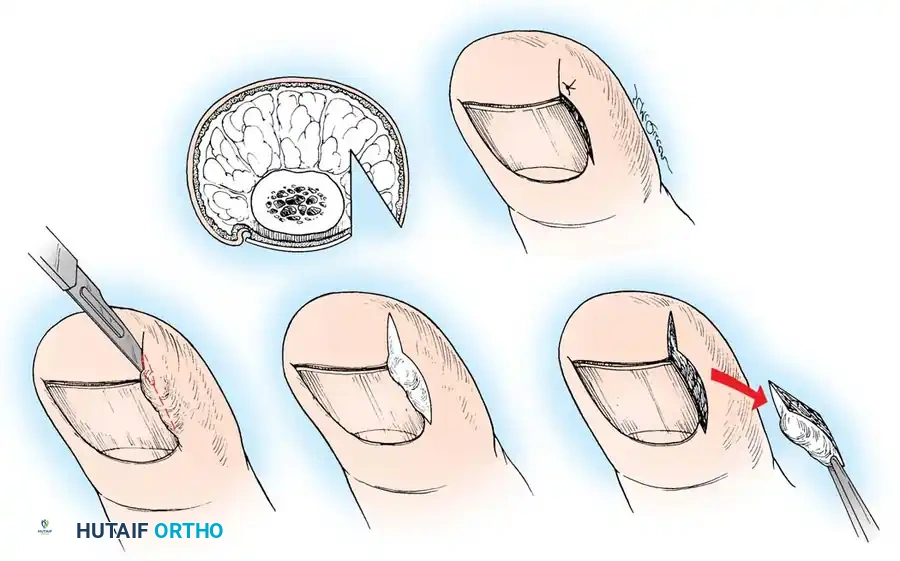
- Incision: Make a longitudinal incision through the nail plate, approximately 3 to 4 mm from the affected lateral border. Extend this incision proximally through the eponychium to expose the nail root and matrix.
- Wedge Excision: Make a second, elliptical incision in the soft tissue of the hypertrophied lateral nail fold. Connect this with the first incision to create a wedge containing the lateral nail margin, the underlying nail bed, and the inflamed lateral soft tissue.
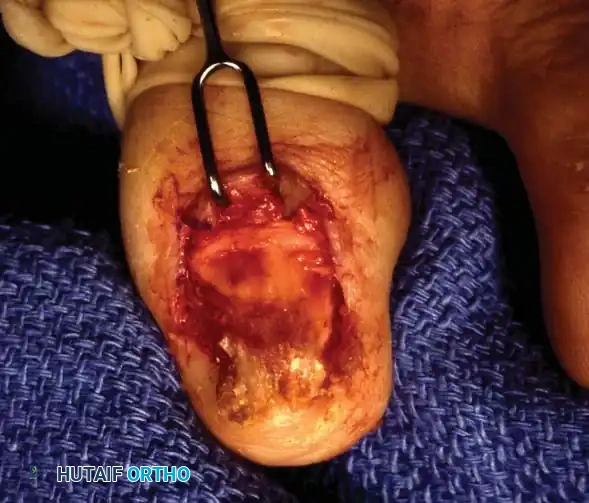
- Matrix Ablation: Deepen the dissection proximally to meticulously excise the lateral horn of the germinal matrix down to the periosteum of the distal phalanx.
- Curettage: Use a small curette to
Associated Surgical & Radiographic Imaging






You Might Also Like