Comprehensive Introduction and Patho-Epidemiology
Congenital scoliosis represents a highly complex, structural lateral curvature of the spine resulting from anomalous vertebral development that creates a profound biomechanical and kinematic imbalance in the longitudinal growth of the spinal column. The critical embryological window for spinal development occurs precisely between the fifth and sixth weeks of intrauterine life. During this highly sensitive period of somitogenesis and subsequent resegmentation, the paraxial mesoderm differentiates into somites, which then undergo a complex process of splitting and recombining to form the vertebral bodies. Any genetic, vascular, or environmental disruption during this cascading sequence can lead to permanent, irreversible congenital anomalies of the axial skeleton. The resulting deformities are not merely static structural defects; they are dynamic, driven by asymmetrical physeal growth that relentlessly exacerbates the curvature as the child matures.
Extensive epidemiological studies and historical analyses, notably those spearheaded by Wynne-Davies, have found no definitive, predictable genetic etiology for isolated congenital abnormalities such as solitary hemivertebrae. Furthermore, Winter’s comprehensive review of 1,250 family histories revealed only 13 patients with first- or second-degree relatives exhibiting congenital spinal deformities. Consequently, the prevailing consensus within the orthopedic community is that most isolated congenital scoliosis arises from non-genetic, sporadic fetal environmental factors or localized vascular watershed infarctions during embryogenesis. While specific teratogenic insults—such as maternal exposure to carbon monoxide, hypoxia, or valproic acid—have been implicated in animal models, they are rarely identifiable by patient history in clinical practice.
Because congenital scoliosis is inherently rigid and surgical correction of severe, neglected deformities is fraught with catastrophic neurological risk, early detection and proactive prognostication are paramount. The overarching philosophy of modern academic management is to institute appropriate, targeted surgical treatment while the curve is small and flexible, rather than attempting high-risk, morbidity-laden salvage procedures once severe, rigid deformity and secondary compensatory structural changes have established themselves. The natural history of these curves is highly variable but generally malignant; McMaster and Ohtsuka’s landmark natural history studies demonstrated that approximately 75% of congenital curves will progress, with 50% progressing rapidly enough to require surgical intervention before skeletal maturity.

Congenital scoliosis must never be viewed as an isolated orthopedic problem; it is frequently a musculoskeletal manifestation of broader, systemic embryological insults. The VACTERL association (Vertebral, Anorectal, Cardiac, Tracheoesophageal, Renal, and Limb anomalies) is a critical consideration in every presenting patient. Genitourinary anomalies are present in up to 18% to 40% of patients, necessitating routine screening via renal ultrasonography to rule out life-threatening obstructive uropathy or unilateral renal agenesis. Cardiovascular anomalies, including septal defects and tetralogy of Fallot, are present in approximately 7% to 10% of patients. Intraspinal anomalies, such as diastematomyelia, syringomyelia, and tethered cord syndrome, occur in up to 40% of patients with congenital spinal deformity, making comprehensive neural axis imaging an absolute prerequisite prior to any surgical intervention.

Detailed Surgical Anatomy and Biomechanics
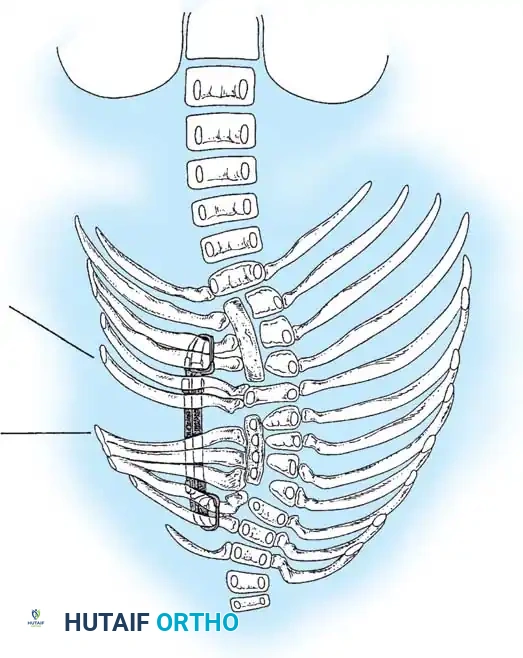
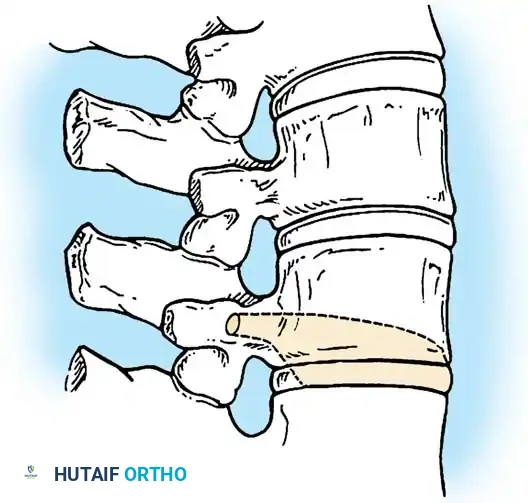
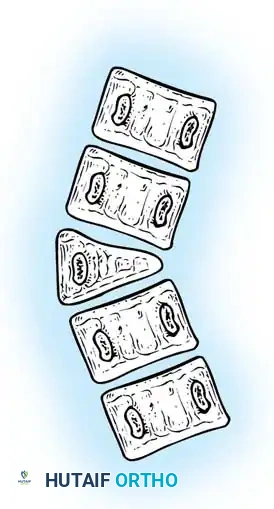
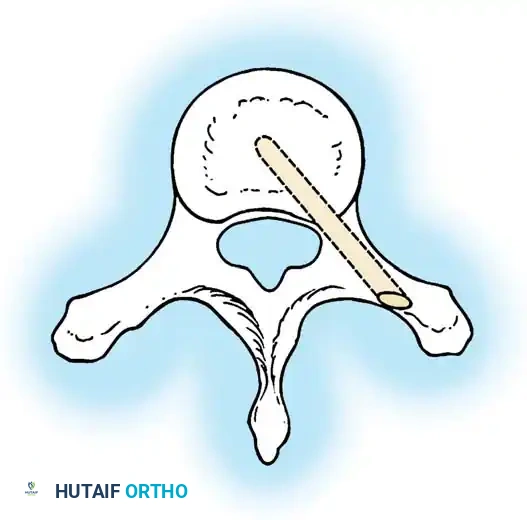
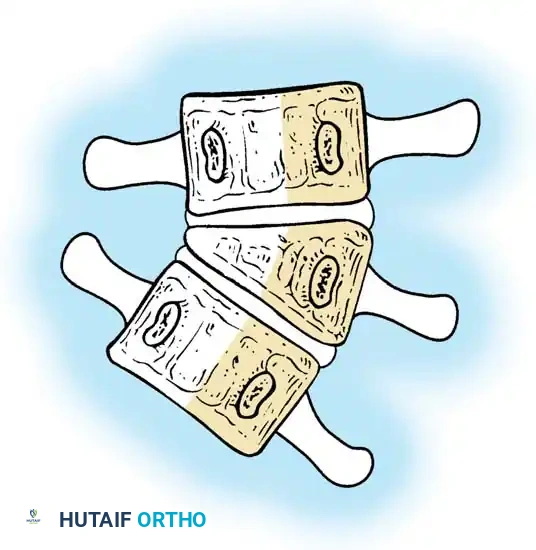
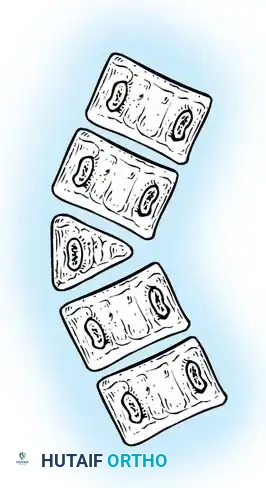
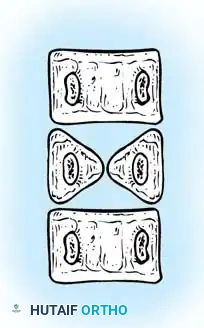
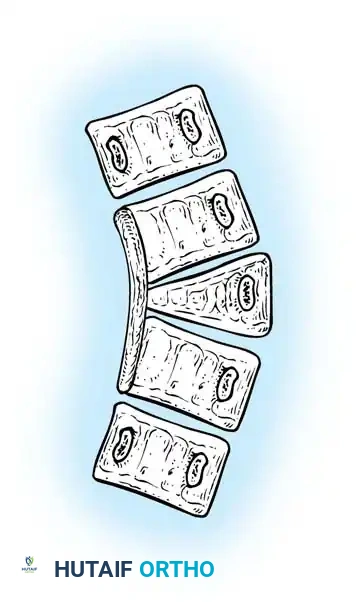
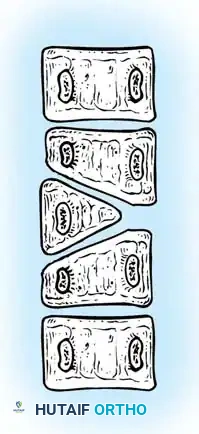
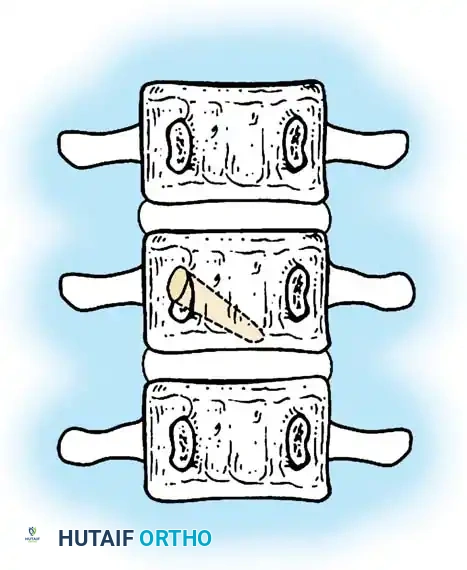
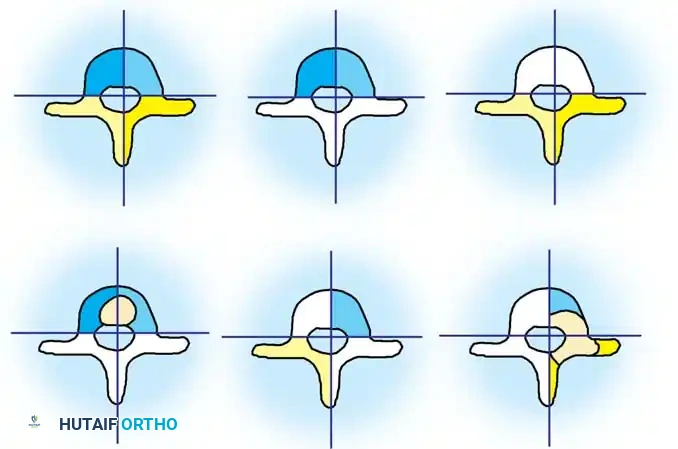
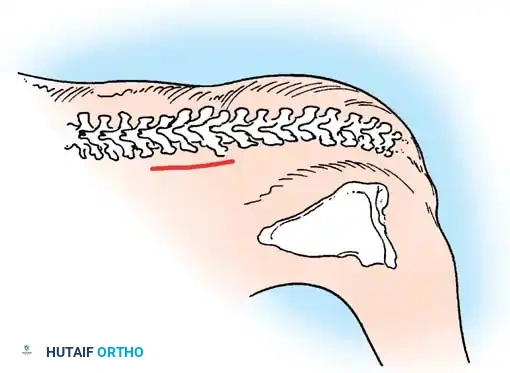
The anatomical classification system originally proposed by MacEwen et al., and subsequently refined by Winter, Moe, and Eilers, remains the universally accepted standard for categorizing congenital spinal deformities. This system meticulously categorizes anomalies based on the specific embryological failure: failure of formation, failure of segmentation, or a mixed combination of both. Failures of formation encompass partial failures, such as wedge vertebrae, and complete failures, such as hemivertebrae. Hemivertebrae are further subdivided into incarcerated types, which are tucked between adjacent normal vertebrae without causing significant angular deformity, and free or fully segmented types, which possess functional intervertebral discs and active physes on both superior and inferior surfaces, acting as an active, relentless wedge that drives progressive coronal and sagittal deformity.
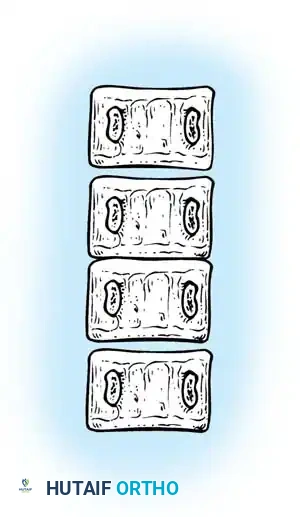
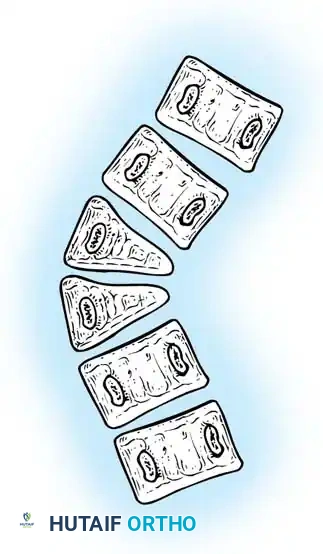
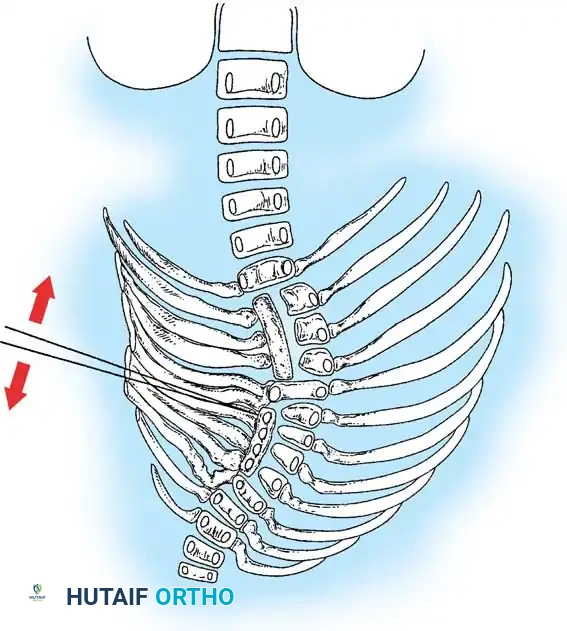
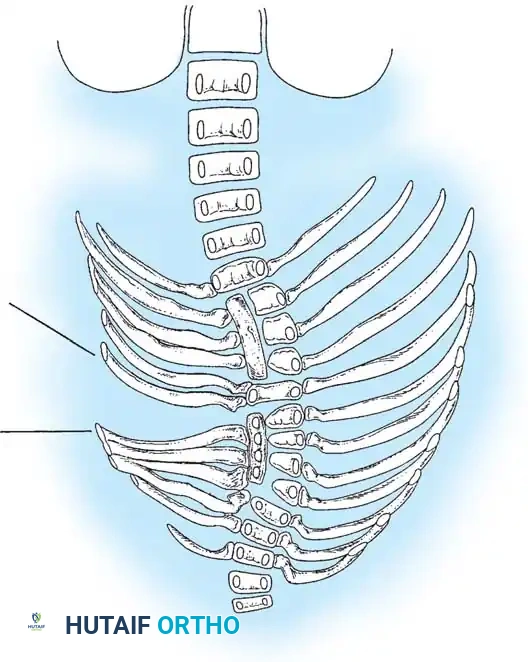
Failures of segmentation occur when the embryological somites fail to separate, creating a solid bony tether. A unilateral failure of segmentation, or unsegmented bar, creates a solid bony bridge on one side of the spine that completely tethers longitudinal growth on that concavity. Meanwhile, the contralateral convexity continues to grow unimpeded, leading to rapid, severe, and highly rigid curvature. Bilateral failures of segmentation result in block vertebrae, which typically cause segmental shortening and loss of mobility rather than severe lateral curvature. The most malignant and rapidly progressive of all congenital anomalies is the mixed deformity: a unilateral unsegmented bar with a contralateral fully segmented hemivertebra at the exact same apical level. This creates a devastating biomechanical environment featuring a simultaneous rigid tether on the concavity and a powerful expansile growth force on the convexity.
Regional biomechanics heavily dictate the prognosis and the anatomical approach to surgery. Cervicothoracic anomalies frequently present with severe cosmetic deformity, including torticollis and marked shoulder asymmetry, but are somewhat constrained by the rigid shoulder girdle. Thoracic anomalies are intimately tied to the development of the rib cage and pulmonary parenchyma; severe thoracic curves, particularly those involving fused ribs or unsegmented bars, can lead to Thoracic Insufficiency Syndrome (TIS), characterized by the inability of the thorax to support normal respiration and lung growth. Thoracolumbar anomalies carry the highest risk of rapid progression due to the lack of stabilizing rib cage structures and the exceptionally high biomechanical shear and compressive loads at the thoracolumbar transition zone. Lumbosacral hemivertebrae, even if small in angular magnitude, cause profound truncal shift and global coronal decompensation because they essentially tilt the entire foundation of the spine.
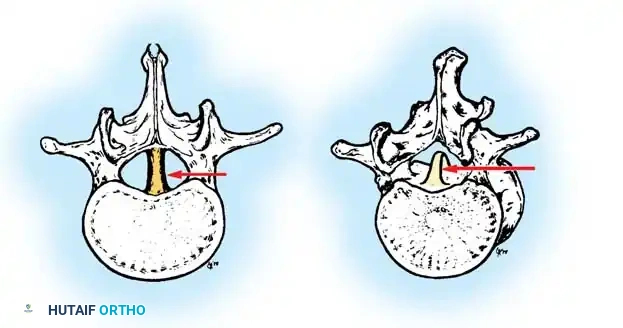
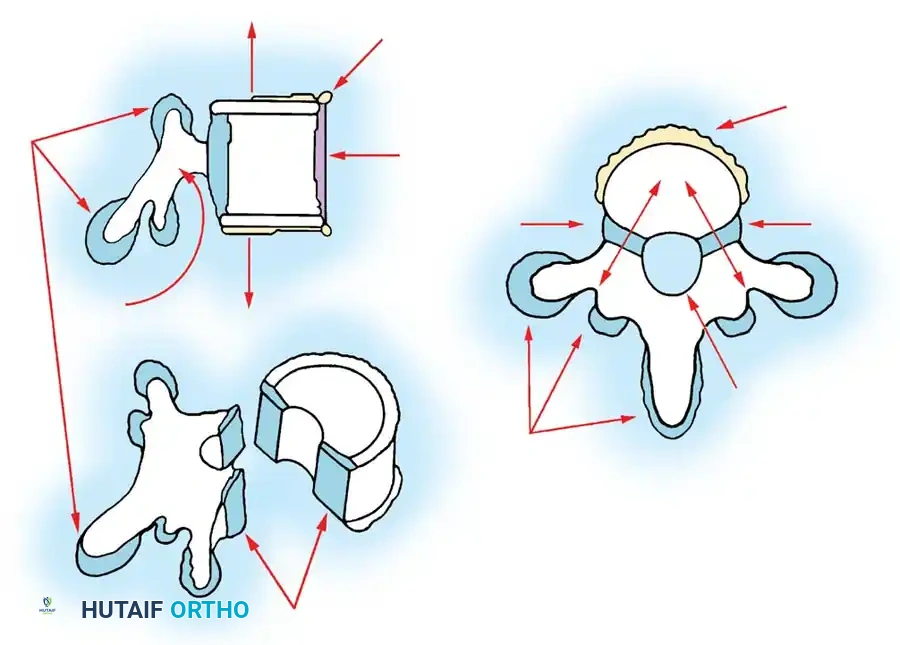
The intraspinal anatomy in congenital scoliosis is notoriously aberrant and presents a formidable challenge to the operating surgeon. The presence of spina bifida occulta, absent or hypoplastic laminae, and dysplastic pedicles makes standard anatomical landmarking unreliable and dangerous. The spinal cord itself may be tethered by a thickened filum terminale, or split by a bony or cartilaginous spur (diastematomyelia) that invaginates the dura. Segmental medullary vessels may follow unpredictable courses, increasing the risk of anterior spinal artery syndrome during exposure or deformity correction. Surgeons must rely on advanced 3D imaging and meticulous, unhurried subperiosteal dissection, frequently utilizing intraoperative navigation and continuous neuromonitoring to safely navigate this distorted anatomical landscape.
Exhaustive Indications and Contraindications
The decision-making process for surgical intervention in congenital scoliosis is highly nuanced, requiring a delicate balance between halting progressive deformity, preserving longitudinal spinal growth, and maximizing pulmonary development. Because conservative management, including rigid orthotic bracing, is universally ineffective at halting the progression of primary structural congenital anomalies, the presence of a documented, progressive curve is the primary indication for surgical intervention. Bracing is strictly reserved for controlling secondary, flexible compensatory curves that develop in the structurally normal spine above or below the congenital anomaly. Waiting for a child with a known progressive anomaly to reach a specific age or skeletal maturity is a historical fallacy that invariably leads to severe, rigid deformities requiring highly morbid, complex salvage osteotomies.
Specific surgical techniques carry distinct indications based on the patient's age, anomaly type, and curve magnitude. In situ posterior spinal fusion is indicated for young children with progressive curves that are currently of an acceptable magnitude, where the primary goal is simply to arrest progression. Combined anterior and posterior convex hemiepiphysiodesis is indicated for young patients (typically under 5 years old) with progressive curves less than 50 degrees, provided there is documented, healthy growth potential on the concave side of the curve. Hemivertebra excision is the gold standard for a fully segmented, progressive hemivertebra, particularly at the lumbosacral junction where it drives severe coronal decompensation. Growth-friendly constructs, such as Vertical Expandable Prosthetic Titanium Ribs (VEPTR) or traditional growing rods, are indicated for patients with complex anomalies spanning multiple segments, particularly when associated with Thoracic Insufficiency Syndrome.

Contraindications to surgical intervention must be rigorously respected to prevent catastrophic iatrogenic complications. Absolute contraindications include the presence of an untreated, symptomatic intraspinal anomaly (such as a tethered cord or diastematomyelia), which must be neurosurgically untethered prior to any structural correction of the spinal column to prevent acute traction injury to the spinal cord. Active surgical site infection or profound medical instability are also absolute contraindications. Relative contraindications include severe pulmonary hypertension or cor pulmonale, which dramatically increase the risk of perioperative mortality, and extreme immaturity where the bone quality precludes adequate fixation, necessitating alternative non-fusion strategies or delayed intervention.
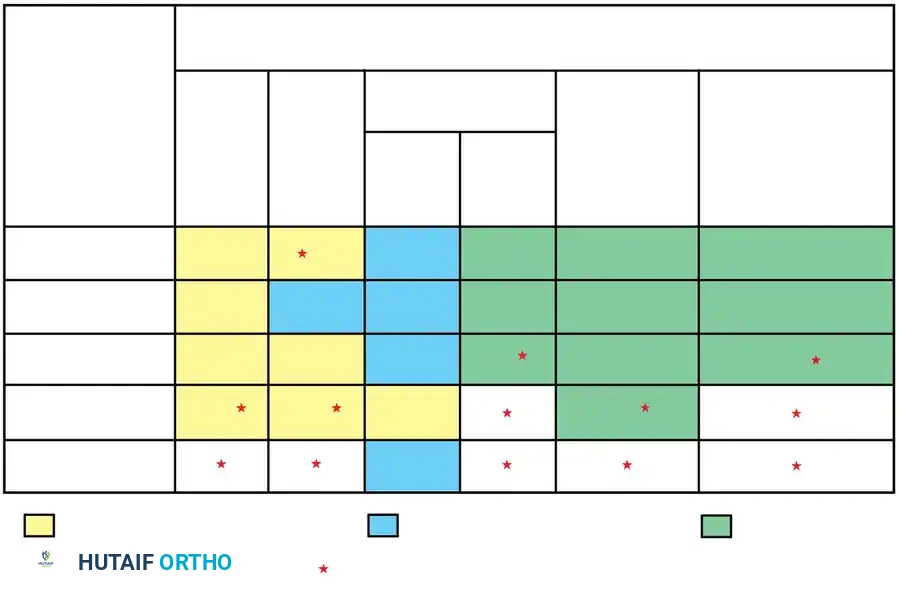
| Parameter | Indications for Surgical Intervention | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Curve Dynamics | Documented progression >5° over 6 months; Unsegmented bar with contralateral hemivertebra | Static, non-progressive block vertebrae without decompensation | Mild, non-progressive curves in skeletally mature patients |
| Neurological Status | Normal neural axis confirmed by MRI; Cleared by neurosurgery post-untethering | Untreated tethered cord; Untreated diastematomyelia; Active syrinx | Progressive neurological deficit requiring emergent decompression first |
| Pulmonary Function | Thoracic Insufficiency Syndrome (TIS) requiring expansion thoracostomy | Severe, irreversible Cor Pulmonale | Severe restrictive lung disease (FVC < 30% predicted) |
| Anatomical Factors | Lumbosacral hemivertebra causing coronal shift; Severe rigid focal kyphosis | Active osteomyelitis or discitis at the proposed surgical site | Extreme osteopenia; Inadequate soft tissue coverage |
Pre-Operative Planning, Templating, and Patient Positioning
Comprehensive pre-operative planning is the bedrock of successful outcomes in congenital scoliosis surgery. The clinical evaluation must extend far beyond the spinal deformity itself. A meticulous neurological examination is mandatory, seeking subtle upper motor neuron signs, asymmetric abdominal reflexes, unilateral calf atrophy, or cavovarus foot deformities that may herald an occult tethered cord. Cutaneous stigmata of spinal dysraphism, such as hairy patches, sacral dimples, or hemangiomas along the midline, must be documented. Because of the high incidence of VACTERL associations, every patient must undergo a renal ultrasound to evaluate for unilateral agenesis or obstructive uropathy, and an echocardiogram to rule out structural cardiac defects that could compromise intraoperative hemodynamic stability.


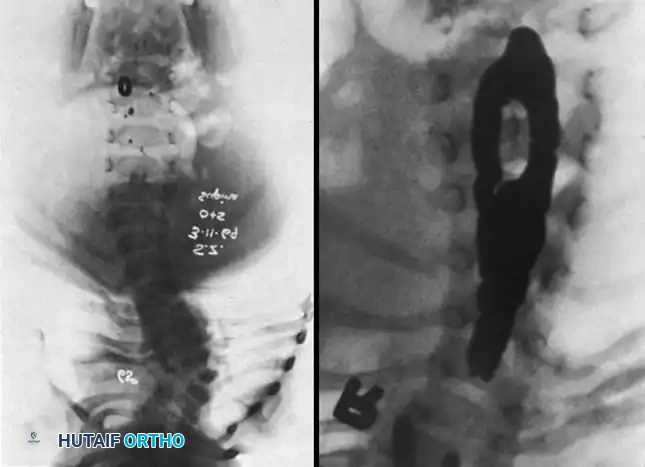
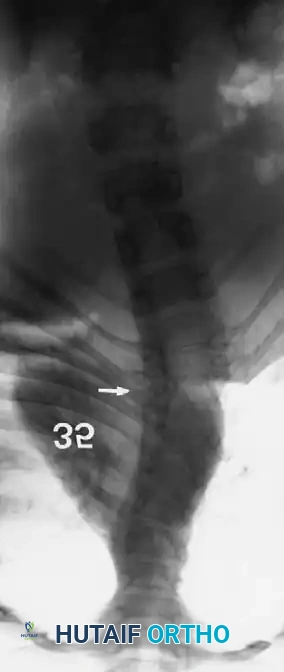
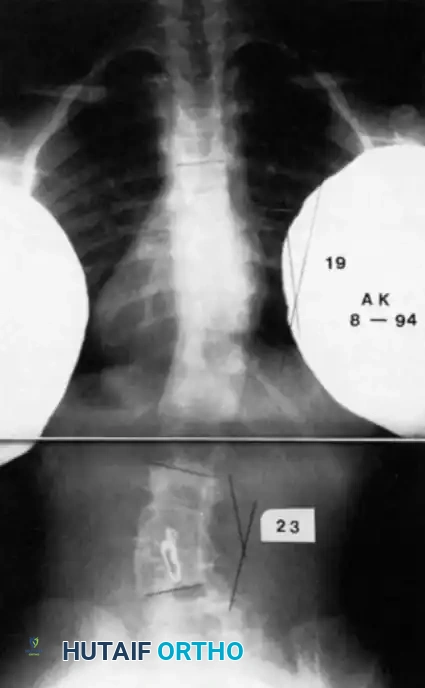
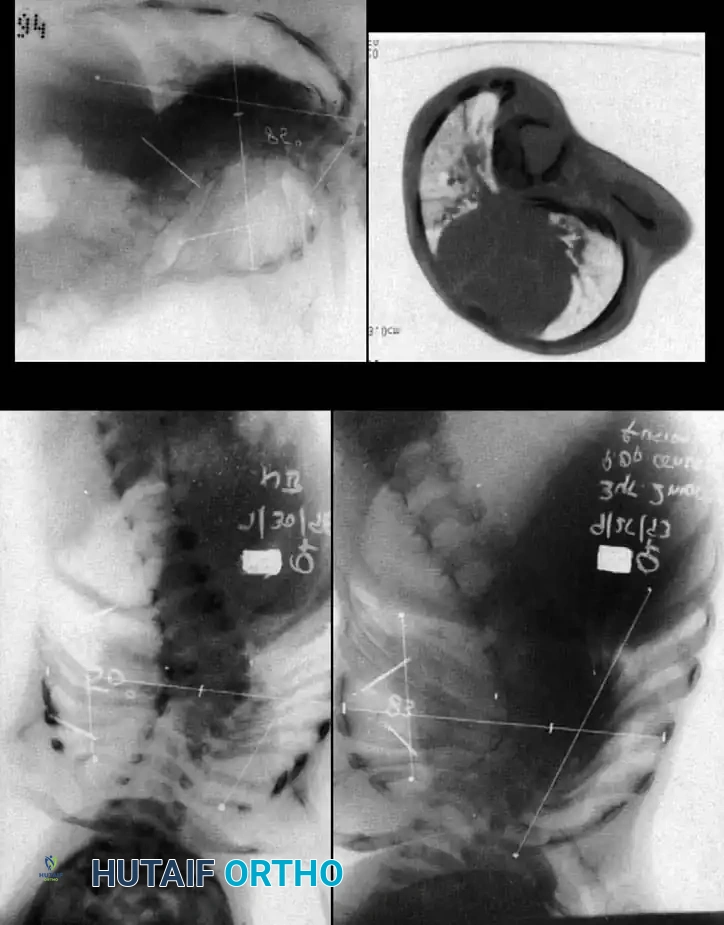
Radiographic evaluation requires a highly systematic approach. High-quality, 36-inch standing (or supine in infants) anteroposterior and lateral radiographs are the cornerstone of initial assessment. Supine lateral bending films and push-prone or traction films are critical for differentiating the rigid, primary congenital structural curve from the flexible, secondary compensatory curves. Because plain radiography often fails to delineate the complex, overlapping anomalous bony anatomy, a fine-cut 3D computed tomography (CT) scan is indispensable. 3D CT reconstructions allow the surgeon to map aberrant pedicle morphology, identify hidden unsegmented bars, and meticulously template pedicle screw trajectories and osteotomy planes prior to entering the operating room.


Magnetic Resonance Imaging (MRI) of the entire neural axis (from the craniocervical junction to the sacrum) is an absolute, non-negotiable requirement for every patient with congenital scoliosis prior to surgical intervention. MRI is essential for identifying tethered cords, syringomyelia, diastematomyelia, and Chiari malformations. In infants, where much of the vertebral anatomy remains cartilaginous and radiolucent on plain films and CT, MRI provides critical visualization of the unossified physes and intervertebral discs, which is vital for planning procedures like hemiepiphysiodesis. If an intraspinal anomaly is identified, it must be addressed sequentially or concurrently by a pediatric neurosurgeon before any corrective forces are applied to the spinal column.

Patient positioning and intraoperative setup require meticulous attention to detail. The patient is typically positioned prone on a radiolucent Jackson table or Relton-Hall frame. The abdomen must hang completely free to prevent compression of the inferior vena cava, which would otherwise engorge the epidural venous plexus and lead to massive, uncontrollable intraoperative hemorrhage. Multimodality intraoperative neuromonitoring (IONM), including Somatosensory Evoked Potentials (SSEPs) and Motor Evoked Potentials (MEPs), is mandatory. The anesthesia team must utilize Total Intravenous Anesthesia (TIVA) to avoid halogenated inhalational agents that severely depress MEP signals. Adequate large-bore intravenous access and invasive arterial blood pressure monitoring are established before the patient is turned prone.
Step-by-Step Surgical Approach and Fixation Technique
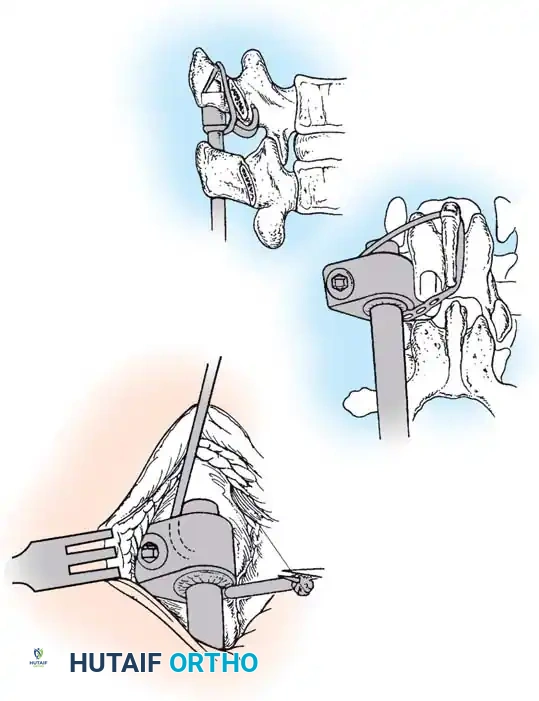
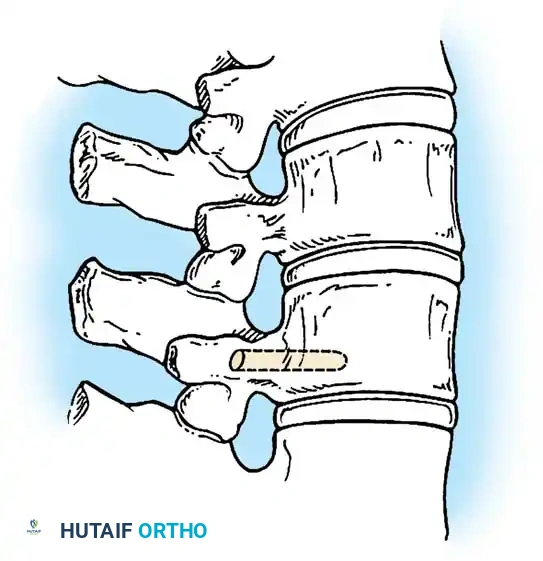
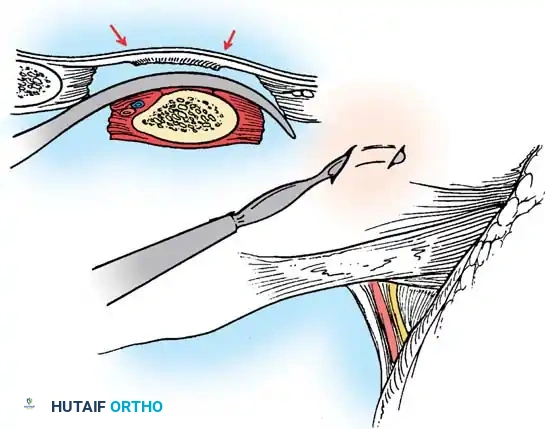
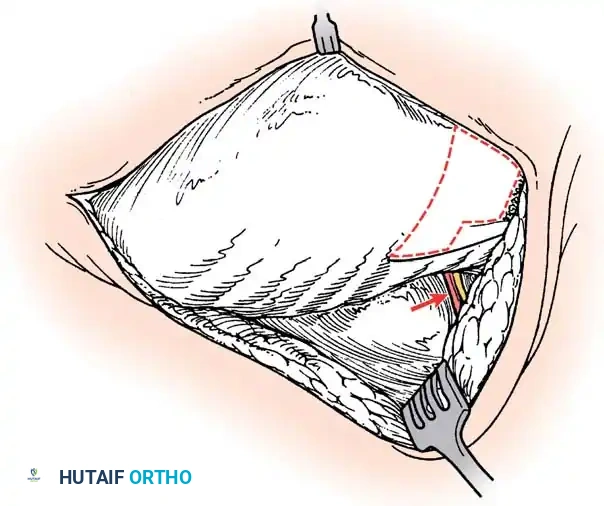
The surgical approach to congenital scoliosis is highly individualized, but the posterior-only hemivertebra excision has emerged as the modern gold standard for fully segmented, progressive hemivertebrae. This procedure is essentially a highly modified, asymmetric Pedicle Subtraction Osteotomy (PSO). The patient is positioned prone, and a standard midline incision is made. Subperiosteal dissection is performed with extreme caution, as the laminae over the hemivertebra may be absent or dysplastic, leaving the dura exposed immediately deep to the fascia. Dissection is carried laterally to expose the transverse processes and the costovertebral junctions in the thoracic spine.
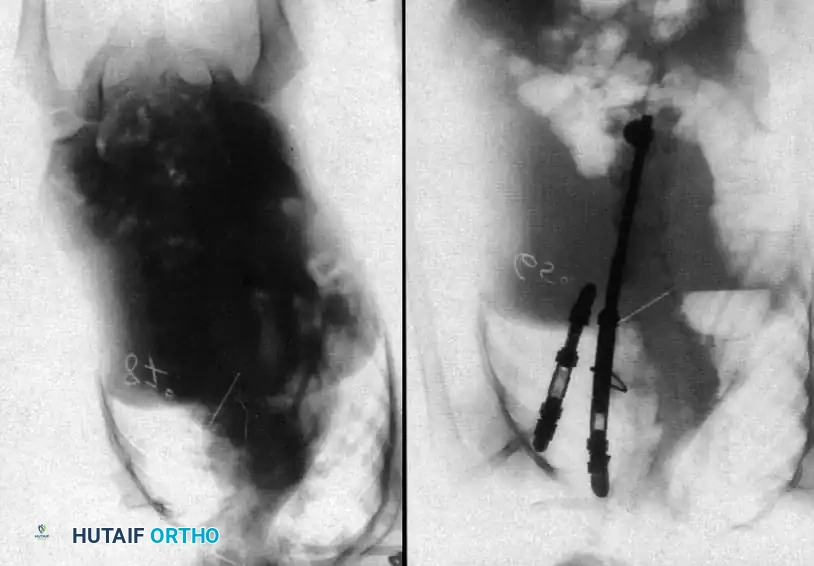
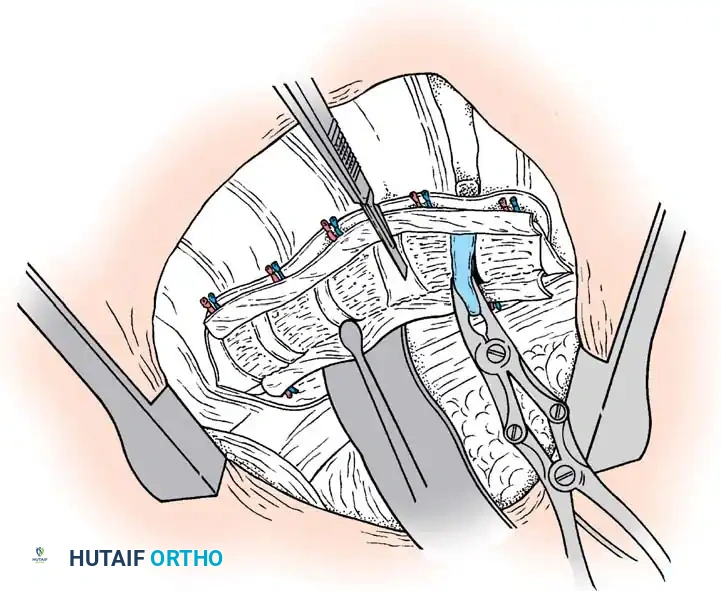
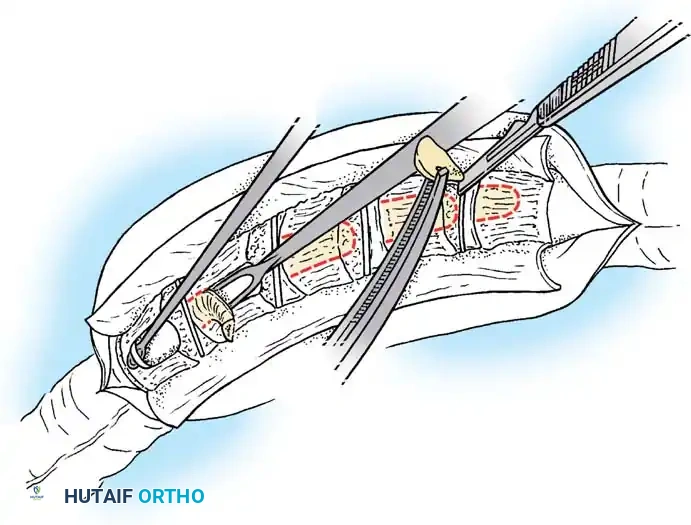
Once exposure is complete, pedicle screws are placed in the normal vertebrae immediately cephalad and caudad to the hemivertebra. In young children with small pedicles, extreme care is taken, often utilizing intraoperative fluoroscopy or 3D navigation. Following instrumentation, the excision begins. The posterior elements of the hemivertebra (lamina, facet joints, and pedicle) are systematically removed using a high-speed burr, Kerrison rongeurs, and osteotomes. The nerve roots exiting above and below the hemivertebra pedicle must be meticulously identified and protected throughout the procedure, as they are frequently compressed in the concavity of the deformity.
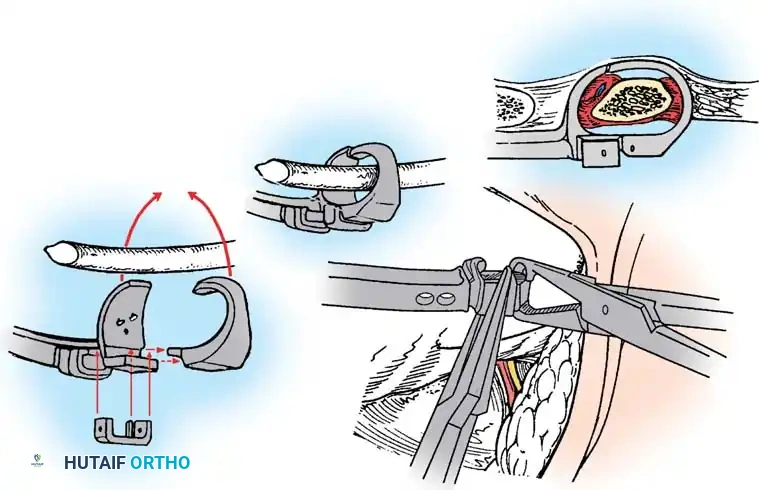
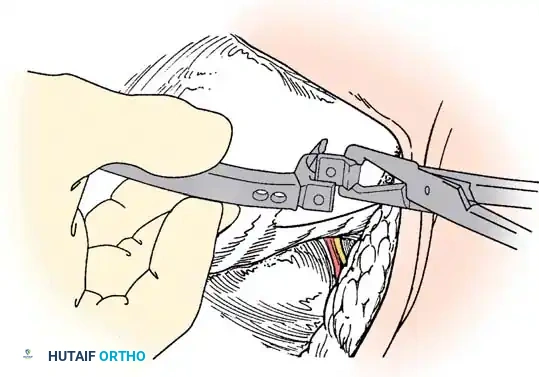
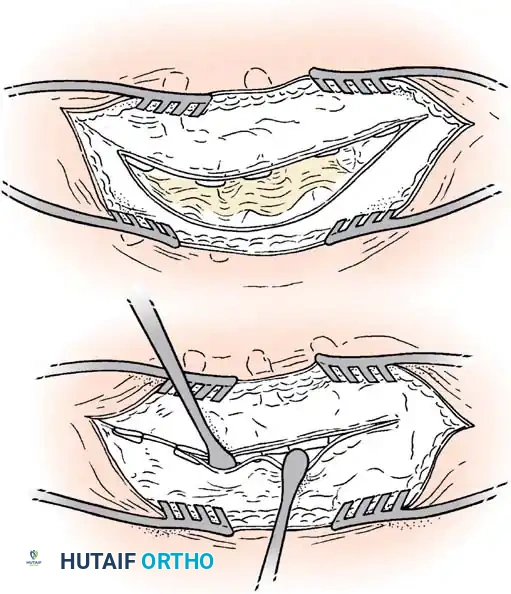
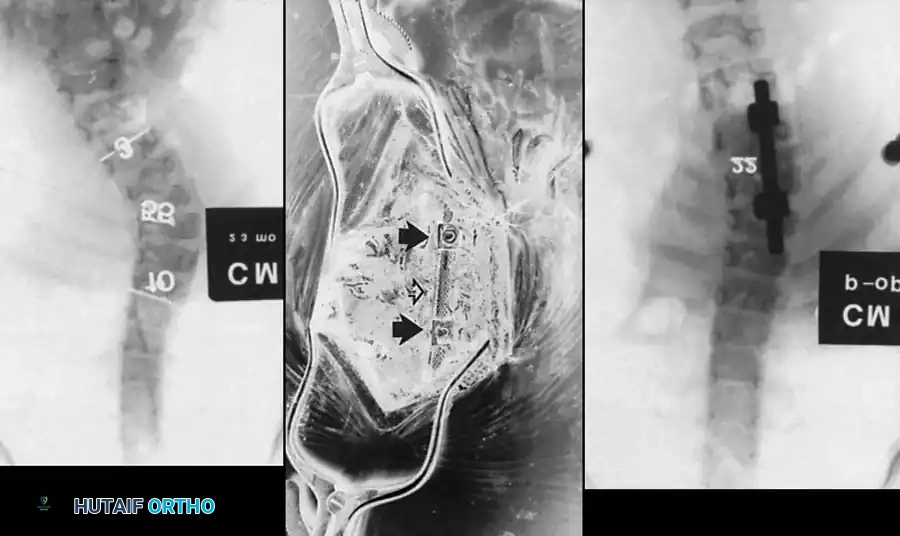
With the neural elements protected, the vertebral body of the hemivertebra is decancellated. An eggshell technique is often employed, where the cancellous bone is curetted out, leaving the cortical margins intact until the very end to protect the anterior vascular structures. The adjacent superior and inferior intervertebral discs are completely excised back to the posterior longitudinal ligament. A temporary rod is placed on the contralateral (concave) side to stabilize the spine. The remaining cortical shell of the hemivertebra is then collapsed and removed. Finally, a pre-contoured rod is placed on the convex side, and the osteotomy is slowly closed by applying compression across the convex pedicle screws, effectively correcting the focal coronal and sagittal deformity. The posterior elements are then decorticated, and local autograft mixed with allograft is placed to ensure a robust arthrodesis.
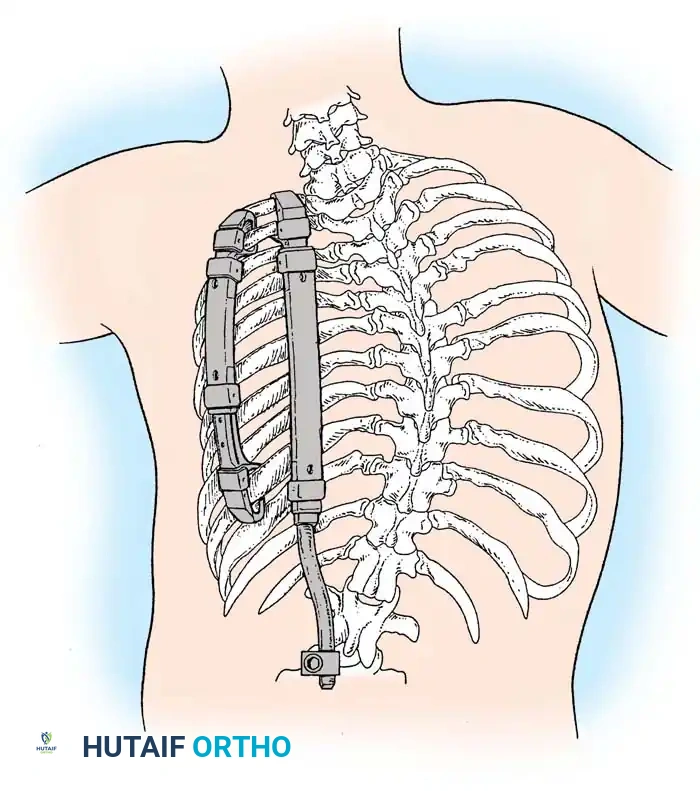
For patients with long, rigid, unsegmented bars or those too young for definitive fusion, growth-sparing techniques are employed. The Vertical Expandable Prosthetic Titanium Rib (VEPTR) or traditional growing rod constructs are utilized to bypass the anomalous segments. These systems are anchored proximally and distally in healthy tissue (ribs, spine, or pelvis) and are periodically lengthened (either surgically or magnetically) to allow for continued spinal and pulmonary growth. In cases of Thoracic Insufficiency Syndrome, opening wedge thoracostomies may be performed in conjunction with VEPTR placement to directly expand the constricted hemithorax and improve pulmonary compliance.
Complications, Incidence Rates, and Salvage Management
Surgical intervention for congenital scoliosis carries one of the highest complication profiles in pediatric orthopedics due to the inherent rigidity of the curves and the high prevalence of associated anomalies. Neurological injury is the most devastating complication, occurring in approximately 1% to 3% of cases. This can result from direct mechanical trauma during osteotomy, over-distraction or over-correction of a stiff spine leading to ischemic injury of the spinal cord, or failure to recognize and untether an occult diastematomyelia prior to correction. If Motor Evoked Potentials (MEPs) are lost intraoperatively, a strict algorithm must be followed: immediately halt the procedure, reverse any corrective forces, optimize mean arterial pressure (MAP > 85 mmHg), normalize hemoglobin and oxygenation, and rule out technical monitoring errors. If signals do not return, a wake-up test may be indicated, and the surgeon must be prepared to abandon the correction and fuse in situ.
Pseudarthrosis and hardware failure are significant risks, particularly in long fusions or when attempting to halt the progression of a powerful, active hemiverte
Clinical & Radiographic Imaging Archive