Comprehensive Surgical Management of Malignant Tumors of the Hand
Key Takeaway
Malignant tumors of the hand are rare but require aggressive, evidence-based surgical management to prevent recurrence and metastasis. Chondrosarcoma is the most common primary bone malignancy, while squamous cell carcinoma dominates soft-tissue lesions. Treatment principles dictate wide en bloc excision or ray amputation, prioritizing oncologic margins over limb salvage. Multidisciplinary approaches, including neoadjuvant therapies, are essential for high-grade sarcomas to optimize patient survival and functional outcomes.
Introduction to Malignant Hand Tumors
Malignant tumors of the hand are exceedingly rare, particularly those arising beneath the skin. The complex, compact anatomy of the hand—characterized by a lack of robust fascial compartments and the close proximity of neurovascular bundles, tendons, and bone—presents unique challenges in oncologic resection. A landmark 65-year retrospective review (1920–1985) from the Mayo Clinic by Frassica et al. identified only 22 primary malignant bone tumors of the hand in 18 patients. This cohort included 10 chondrosarcomas, seven hemangioendotheliosarcomas, two osteosarcomas, two fibrosarcomas, and one Ewing sarcoma.
Of the primary bone malignancies, chondrosarcoma is the most prevalent. Conversely, the most common soft-tissue sarcomas include malignant fibrous histiocytoma (MFH), liposarcoma, leiomyosarcoma, synovial sarcoma, fibrosarcoma, rhabdomyosarcoma, epithelioid sarcoma, and malignant nerve sheath tumors.
Surgical Warning: The fundamental tenet of orthopedic oncology in the hand is that oncologic margins must never be compromised for functional preservation. Proper surgical treatment frequently necessitates the sacrifice of normal tissue, ray resections, or occasionally, below-elbow amputations. The ultimate success of the intervention is strictly dependent on achieving negative margins.
While historical literature suggested that malignant bone tumors of the hand rarely metastasize, contemporary evidence confirms that metastasis does occur, particularly following local recurrence. In a critical series of 24 patients with soft-tissue sarcomas of the hand, McPhee et al. demonstrated that amputation yielded superior outcomes compared to lesser resections. Furthermore, tumor size greater than 5 cm and advanced histological stage were significant negative prognosticators for survival. Interestingly, local recurrence alone did not independently reduce overall survival in their cohort. Advances in limb-sparing surgery combined with brachytherapy have shown promise; Alektiar et al. reported a 70% overall survival rate at a 61-month follow-up for high-grade extremity soft-tissue sarcomas treated with this multidisciplinary approach.
Differential Diagnosis: Synovial Chondromatosis
Before diagnosing a primary malignancy, surgeons must rule out aggressive benign or premalignant conditions that mimic sarcomatous growth. Synovial chondromatosis of the hand and wrist, particularly around the distal radioulnar joint (DRUJ), can present with destructive arthritis and a palpable soft-tissue mass.

Fig. 74-19 A, Clinical appearance of synovial chondromatosis of the distal radioulnar joint, presenting as a firm, lobulated mass.

Fig. 74-19 B, Radiograph demonstrating secondary arthritis and a significant soft-tissue mass with stippled calcifications.
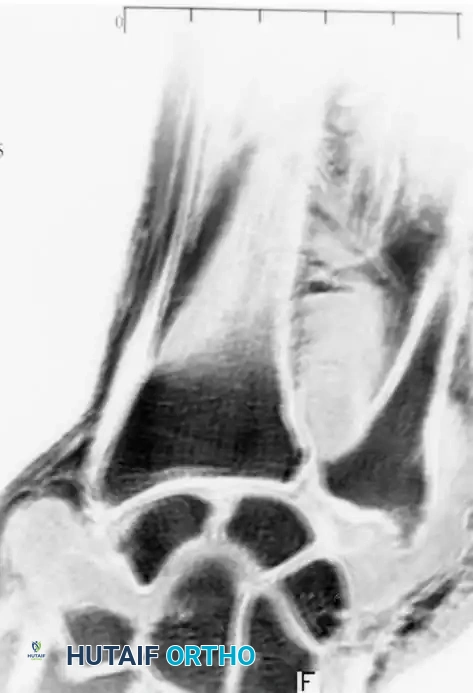
Fig. 74-19 C, MRI detailing the extent of cartilaginous loose bodies within the joint capsule.

Fig. 74-19 D, Intraoperative view of surgical excision and radical synovectomy required to prevent recurrence.
Primary Malignant Bone Tumors
Chondrosarcoma
Chondrosarcomas are the most common primary malignant bone tumors of the hand. They typically present in the metacarpals or proximal phalanges. While they can arise de novo, they occasionally develop secondary to malignant transformation of a preexisting enchondroma, though this is statistically rare.
Clinical Presentation & Biomechanics:
Unlike benign enchondromas, which are typically asymptomatic unless complicated by a pathologic fracture, chondrosarcomas present with insidious, deep, and unremitting pain. The biomechanical integrity of the bone is progressively compromised by endosteal scalloping and cortical destruction, leading to microfractures or overt pathologic fractures.
Radiographic Evaluation:
Imaging often reveals a destructive, expansile radiolucent lesion with intralesional "popcorn" or stippled calcifications. Cortical breakthrough and soft-tissue extension are hallmarks of high-grade lesions. Granberry and Bryan noted that chondrosarcoma in the carpus (e.g., trapezium) can radiographically mimic advanced osteoarthritis.
Surgical Management:
Clinical Pearl: A painful cartilaginous lesion in the hand, or one that recurs after routine curettage and bone grafting of a presumed enchondroma, must be treated as a chondrosarcoma until proven otherwise.
Dahlin and Salvador established that intralesional procedures (curettage) are universally unsuccessful for chondrosarcoma. Treatment mandates total en bloc resection or ray amputation. If radical surgery is executed as the primary index procedure, local recurrence is highly unlikely, and the overall prognosis is excellent.
Osteogenic Sarcoma (Osteosarcoma)
Osteogenic sarcoma is exceptionally rare in the hand, with only about 36 proven cases documented in the literature. The average age of presentation is 49 years, which is significantly older than the typical adolescent demographic for appendicular osteosarcoma.
Etiology:
A notable subset of hand osteosarcomas is secondary to prior irradiation (e.g., occupational overexposure to x-rays) or the historical ingestion/handling of radium salts.

Fig. 74-21 A, Clinical appearance of an osteogenic sarcoma presenting as a massive, fungating lesion of the proximal phalanx.
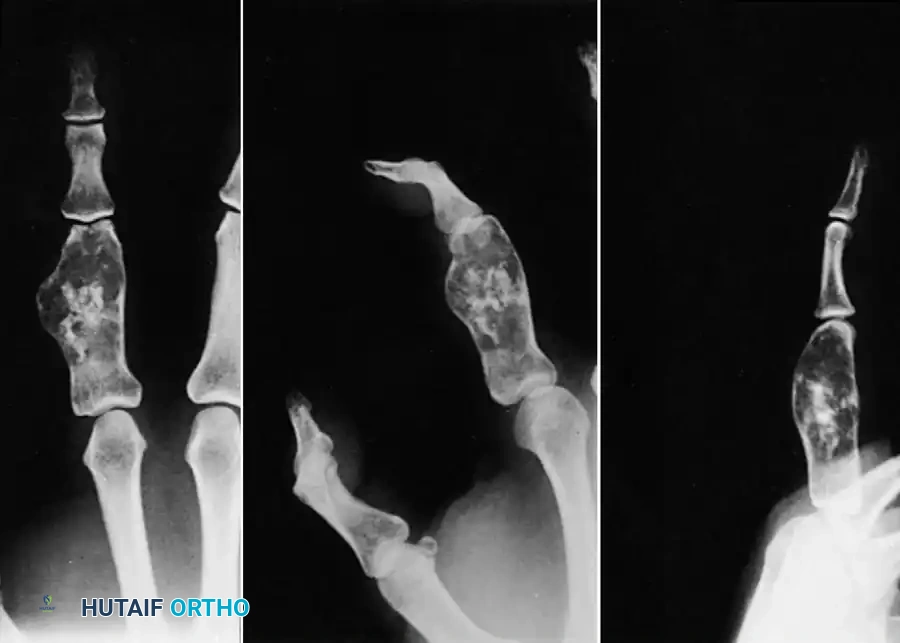
Fig. 74-21 B, Radiograph showing aggressive, permeative bone destruction with a classic "sunburst" periosteal reaction.
Surgical Approach:
Careful wide excision or amputation offers a favorable prognosis, which is generally better than for osteosarcomas located in the long bones. The periosteal variant of osteogenic sarcoma can often be managed with a digital amputation. However, intramedullary or high-grade variants typically require a formal ray amputation or, in cases of proximal carpal/metacarpal involvement, a below-elbow amputation. Honoki et al. successfully utilized neoadjuvant chemotherapy followed by ray amputation in a pediatric patient, highlighting the evolving role of multidisciplinary care.
Ewing Sarcoma
Ewing sarcoma rarely involves the hand. When it does, it predominantly affects males in their second decade of life.
Clinical Pitfalls:
Clinically, Ewing sarcoma is notorious for mimicking a localized pyogenic infection. Patients frequently present with localized pain, erythema, swelling, low-grade fever, leukocytosis, and an elevated erythrocyte sedimentation rate (ESR).
Management:
Radiographs demonstrate a permeative, "moth-eaten" pattern of bone destruction with an "onion-skin" periosteal reaction. Ewing sarcoma is highly aggressive. Historically, 5-year survival rates were a dismal 10% to 15%. However, modern protocols combining multi-agent neoadjuvant chemotherapy, radiation therapy, and aggressive surgical excision have improved survival rates to 50% to 75%.
Soft-Tissue Sarcomas of the Hand
Epithelioid Sarcoma
Epithelioid sarcoma is the most common soft-tissue sarcoma of the hand and upper extremity in young adults. It is infamous for its deceptive, benign-appearing clinical course, leading to frequent misdiagnosis.
Pathology and Presentation:
It typically presents as a firm, painless, subcutaneous nodule. It has a strong predilection to track proximally along fascial planes, tendon sheaths, and neurovascular bundles, forming multiple satellite nodules. It is frequently misdiagnosed as a simple inflammatory process, a ganglion cyst, or a rheumatoid nodule. Overlying skin ulceration with central necrosis is common in advanced stages. Histologically, it exhibits a granulomatous pattern with central necrosis surrounded by inflammatory cells; under high magnification, the tumor cells mimic epithelial cells.
Surgical Warning: Epithelioid sarcoma is unique among sarcomas due to its high propensity for regional lymph node metastasis. Metastasis to the lungs typically follows multiple local recurrences.
Surgical Management:
Inadequate excision invariably leads to recurrence. Enzinger and Weiss reported an 85% local recurrence rate, mostly within 6 months of marginal excision. Primary wide en bloc excision or amputation (digit or ray) is mandatory.

Fig. 74-23 A, Small epithelioid sarcoma involving the distal second web space, deceptively appearing as a benign ulceration.

Fig. 74-23 B, Intraoperative planning for a wide double-ray excision to achieve negative margins.

Fig. 74-23 C, The resected specimen demonstrating the necessity of radical margins.

Fig. 74-23 D, Acceptable functional outcome following double-ray amputation and soft-tissue reconstruction.
Even after wide excision, microscopic tumor may persist at the margins. Recurrences proximal to the metacarpophalangeal (MCP) joints often necessitate a below-elbow amputation. Regional lymph node dissection is recommended by many oncologic surgeons in conjunction with the primary excision.
Malignant Fibrous Histiocytoma (MFH) and Fibrosarcoma
MFH (now often classified under undifferentiated pleomorphic sarcoma) and fibrosarcoma are aggressive soft-tissue malignancies. Fibrosarcomas are of mesothelial origin and can arise in areas of prior radiation or severe burn scars (Marjolin's ulcer variant).

Fig. 74-20 A, Radiographic appearance of malignant fibrous histiocytoma invading the middle metacarpal base.

Fig. 74-20 B, Wide surgical excision achieved via a formal ray amputation.
Patients typically present with a painless, rapidly enlarging mass, though nerve compression can induce neuropathic pain. Treatment consists of radical wide excision or amputation.
Rhabdomyosarcoma
Rhabdomyosarcoma in the hand is exceptionally rare and historically carries a fatal prognosis. It can present in alveolar, embryonal, or pleomorphic subtypes, with the alveolar form being most common in the extremities. These tumors are deeply situated, intimately associated with striated intrinsic muscles (e.g., thenar/hypothenar eminences), and grow rapidly without causing pain. Bone erosion is a frequent complication. Survival depends on a rigorous multidisciplinary approach, including neoadjuvant chemotherapy and total compartmental excision or amputation.
Cutaneous Malignancies of the Hand
Squamous Cell Carcinoma (SCC)
Squamous cell carcinoma is the most common malignancy of the hand, accounting for 58% to 90% of all hand cancers. It is four times more common in men, typically presenting in the 50s.
Etiology and Presentation:
SCC has a strong predilection for sun-exposed areas (dorsum of the hand) and is the most common malignancy of the nail bed, where it is frequently misdiagnosed as chronic paronychia or a fungal infection. Lesions vary from small, erythematous, desquamating plaques to large, fungating, ulcerative masses.
Surgical Management:
While SCC grows slowly and rarely metastasizes, it is locally destructive. Poor prognostic factors include size > 2 cm, poor differentiation, immunosuppression, perineural invasion, and recurrence.

Fig. 74-24 A, Squamous cell carcinoma of the nail bed, mimicking a chronic benign inflammatory process.

Fig. 74-24 B, Wide excision including a portion of the underlying distal phalanx to ensure adequate deep margins.

Fig. 74-24 C, Final closure utilizing a local advancement flap after wide excision.
Tumor-free margins must be strictly adhered to: at least 0.5 cm for small, superficial lesions, and up to 3 cm for recurrent or fixed lesions. Subungual SCC often requires amputation at the distal interphalangeal (DIP) joint to ensure clear deep margins. Lymph node dissection is reserved for clinically palpable nodes or recurrent disease.
Basal Cell Carcinoma (BCC)
Basal cell carcinoma is far less common on the hand than SCC. It classically presents as a raised, nodular lesion with a pearly, telangiectatic border in fair-skinned individuals. Because BCC rarely metastasizes and grows by direct local extension, it can be safely managed with a 0.5-cm surgical margin. Recurrence rates following adequate excision are approximately 1%.
Malignant Melanoma
The incidence of malignant melanoma is rising faster than any other cancer, heavily linked to ultraviolet radiation exposure. Survival is directly correlated with Breslow thickness: 97% for lesions ≤ 0.75 mm, dropping to 50% for lesions ≥ 3 mm.
Early detection relies on the ABCDE criteria (Asymmetry, Border irregularity, Color variation, Diameter > 6 mm, Evolution). Lesions thicker than 1 mm require referral to a surgical oncologist for wide local excision (1–2 cm margins depending on thickness) and sentinel lymph node biopsy. Subungual melanomas (Hutchinson's sign) require amputation proximal to the DIP or IP joint.
Metastatic Tumors to the Hand (Acro-metastases)
Metastatic lesions to the hand are rare, representing roughly 0.1% of all osseous metastases. The most frequent primary source is bronchogenic (lung) carcinoma, followed by renal, prostate, breast, uterine, and colon carcinomas.
Clinical Presentation:
Acro-metastases frequently mimic acute osteomyelitis or septic arthritis. The digit becomes erythematous, swollen, exquisitely tender, and warm. Radiographs reveal aggressive, osteolytic destruction of the cortical bone, most commonly in the distal phalanges.
Management:
A tissue biopsy is imperative to differentiate metastasis from infection, gout, or a primary bone cyst. The presence of an acro-metastasis carries a grim prognosis, with a median patient survival of only 5 to 6 months. Treatment is strictly palliative. If the lesion is painful or fungating, a simple amputation through the joint proximal to the lesion provides rapid pain relief, swift wound healing, and improved quality of life in the patient's final months.
General Surgical Principles: Ray Amputation Technique
When a primary malignancy dictates the removal of an entire digit and its corresponding metacarpal, a formal ray amputation is the gold standard.
Positioning and Preparation
- Anesthesia: General anesthesia or a regional brachial plexus block.
- Positioning: Supine with the arm extended on a radiolucent hand table.
- Tourniquet: Exsanguination by elevation only (avoid Esmarch bandages to prevent proximal tumor seeding). Inflate the pneumatic tourniquet to 250 mm Hg.
Surgical Approach (Index or Small Finger Ray)
- Incision: Design a racquet-shaped incision. The handle of the racquet extends proximally over the dorsal metacarpal shaft, while the loop encircles the base of the proximal phalanx. Ensure the incision remains well clear of the tumor's reactive zone.
- Neurovascular Dissection: Identify the digital arteries and nerves. Ligate the arteries securely with non-absorbable suture. Draw the digital nerves distally, transect them sharply under tension, and allow them to retract deep into the intrinsic musculature to prevent painful neuroma formation.
- Tendon Management: Transect the extensor and flexor tendons under tension, allowing them to retract proximally.
- Osteotomy: Expose the metacarpal base. Using an oscillating saw, perform an oblique osteotomy at the proximal metaphysis (or disarticulate at the carpometacarpal joint if margins dictate).
- Intrinsic Muscle Transfer: For an index ray amputation, transfer the first dorsal interosseous muscle to the base of the second dorsal interosseous or the third proximal phalanx to preserve pinch strength.
- Closure: Deflate the tourniquet and achieve meticulous hemostasis. Close the deep tissues over the bone end. Trim redundant skin to create a smooth, aesthetic web space. Close the skin with interrupted non-absorbable sutures.
Postoperative Protocol
- Apply a bulky, non-compressive soft dressing with a volar orthosis to support the wrist in slight extension.
- Strict elevation of the limb for 48–72 hours to minimize edema.
- Initiate immediate active range of motion (ROM) of the uninvolved digits to prevent stiffness.
- Suture removal at 14 to 21 days, followed by referral to a multidisciplinary oncology board for consideration of adjuvant chemotherapy or radiation, depending on final pathologic margins and tumor grade.
You Might Also Like
