Surgical Management of Peroneal and Sciatic Nerve Injuries

Key Takeaway
The common peroneal nerve is highly susceptible to injury due to its superficial course around the fibular neck. This comprehensive guide details the surgical anatomy, clinical evaluation, and operative techniques for managing peroneal and sciatic nerve lesions. It covers indications for neurolysis, primary neurorrhaphy, and autogenous nerve grafting, alongside rigorous postoperative immobilization protocols to optimize functional recovery and mitigate footdrop.
Comprehensive Introduction and Patho-Epidemiology
The surgical management of lower extremity peripheral nerve injuries, specifically involving the sciatic nerve and its terminal bifurcations—the common, superficial, and deep peroneal nerves—represents one of the most formidable challenges in reconstructive orthopaedic microsurgery. Unlike the upper extremity, where the brachial plexus and its outflow tracts have been the subject of exhaustive surgical innovation and relatively predictable reconstructive algorithms, the lower extremity presents unique biological and biomechanical hurdles. The sheer length of the sciatic nerve dictates that proximal lesions require regenerating axons to traverse extraordinary distances to reach their target motor endplates in the leg and foot. Consequently, by the time regenerating axons reach these distal targets, irreversible target organ atrophy and motor endplate degradation have frequently occurred, severely compromising functional recovery. A profound understanding of the patho-epidemiology of these lesions is therefore critical for the orthopaedic surgeon to establish realistic patient expectations and formulate an optimal, time-sensitive surgical strategy.
Epidemiologically, the common peroneal nerve is the most frequently injured nerve in the lower extremity, and its vulnerability is well documented in both orthopedic trauma and iatrogenic settings. High-energy lower extremity trauma, particularly multiligamentous knee injuries (MLKIs) and knee dislocations (specifically KD-III and KD-IV variants), carries a staggering 16% to 40% incidence of common peroneal nerve injury. The mechanism is typically an extreme varus and hyperextension force that imparts catastrophic traction to the posterolateral corner structures and the tethered peroneal nerve. Furthermore, fractures of the fibular head and neck, complex tibial plateau fractures, and severe crush injuries to the lower leg frequently precipitate direct contusion, laceration, or secondary ischemic compression of the peroneal nerve and its branches. The sciatic nerve, while better protected by the robust musculature of the gluteal region and posterior thigh, is nonetheless susceptible to high-energy pelvic ring disruptions, posterior hip dislocations, and penetrating trauma.
Iatrogenic nerve injuries remain a persistent and medicolegally perilous complication in orthopaedic surgery. Total hip arthroplasty (THA) is the most common surgical etiology for sciatic nerve palsy, with an incidence ranging from 0.1% to 2.0% in primary cases, escalating to as high as 7% in complex revision scenarios or developmental dysplasia of the hip (DDH) requiring significant limb lengthening. The peroneal division of the sciatic nerve is disproportionately affected in these iatrogenic injuries due to its distinct fascicular topography and relative lack of supportive epineurial connective tissue. Additionally, the common peroneal nerve is uniquely susceptible to compression neuropathy at the fibular neck due to improperly padded casts, rigid orthoses, prolonged surgical positioning (especially in the lateral decubitus or lithotomy positions), and even habitual leg crossing, which can induce focal demyelination or, in severe cases, axonal loss.
The pathophysiology of these nerve injuries follows the classic cascades described by Seddon and Sunderland. While pure neuropraxia (Sunderland Grade I) involves focal myelin disruption with an intact axon and carries an excellent prognosis for spontaneous recovery within weeks, higher-grade injuries (axonotmesis and neurotmesis) initiate Wallerian degeneration distal to the zone of injury. In the context of the sciatic and peroneal nerves, the robust inflammatory response and subsequent fibroblastic proliferation often result in the formation of a dense neuroma-in-continuity or a terminal neuroma. The intraneural scarring disrupts the delicate endoneurial tubes, preventing regenerating axonal growth cones from reaching their distal targets. Understanding this temporal and spatial pathophysiology is paramount, as it dictates the critical window for surgical intervention—typically before the 12-to-18-month threshold, after which the muscle fibers undergo irreversible fatty infiltration and fibrosis.
Detailed Surgical Anatomy and Biomechanics
A profound, three-dimensional understanding of the neuroanatomy and biomechanics of the lower extremity is paramount for the orthopaedic surgeon, particularly when navigating the complex topography of the sciatic nerve and its distal arborizations. The sciatic nerve is the largest peripheral nerve in the human body, originating from the ventral rami of the lumbosacral plexus (L4, L5, S1, S2, and S3). It exits the pelvis through the greater sciatic foramen, typically emerging inferior to the piriformis muscle. However, the surgeon must be acutely aware of the anatomical variants described by Beaton and Anson, where the nerve or its divisions may pierce the piriformis or exit superior to it, predisposing the patient to piriformis syndrome or complicating surgical exposure. The nerve is composed of two distinct trunks—the medial tibial division and the lateral common peroneal division—which are enclosed within a common, robust epineurial sheath but maintain separate fascicular bundles throughout their course in the posterior thigh.
The biomechanics of the sciatic nerve are dictated by its requirement to accommodate significant excursion during hip and knee mobilization. During combined hip flexion and knee extension (the classic straight-leg raise), the sciatic nerve must glide up to 20 millimeters to prevent catastrophic tension. The nerve is supplied by a rich extrinsic segmental blood supply from the inferior gluteal, medial circumflex femoral, and perforating arteries, which feed an intricate intrinsic vasa nervorum. Biomechanical studies have demonstrated that an acute stretch of merely 8% of the nerve's resting length significantly compromises venular outflow, while a stretch of 15% induces complete arterial ischemia and structural failure of the perineurial tubes. This biomechanical vulnerability is particularly pronounced in the common peroneal division, which possesses larger, fewer fascicles and significantly less protective epineurial connective tissue compared to the tibial division, rendering it highly susceptible to stretch-induced axonotmesis.
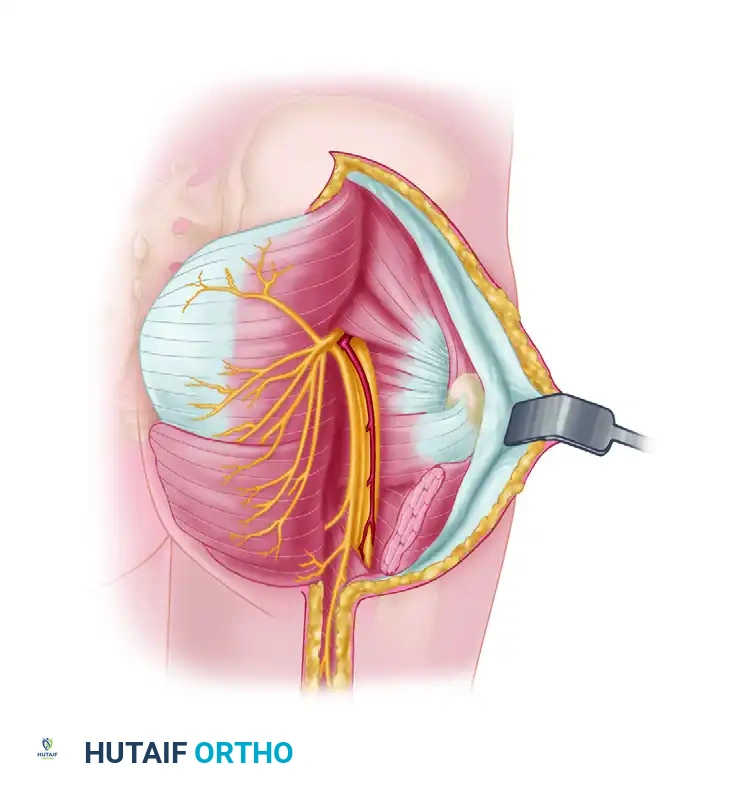
Near the proximal angle of the popliteal fossa, the sciatic nerve formally bifurcates. The common peroneal nerve (composed of fibers from L4, L5, S1, and S2) deviates laterally, tracking along the medial border of the biceps femoris tendon. It then executes a sharp, tethered arch around the posterior aspect of the fibular head and tightly encircles the fibular neck before piercing the fibrous arch of the peroneus longus muscle. This anatomical bottleneck is the most common site for external compression and entrapment. Before its bifurcation, the common peroneal nerve provides critical sensory branches: the lateral sural cutaneous nerve, supplying the lateral knee and proximal calf, and the peroneal anastomotic branch, which joins the tibial contribution to form the sural nerve.
At or just inferior to the fibular neck, the common peroneal nerve divides into its two major terminal branches: the superficial and deep peroneal nerves. The superficial peroneal nerve courses distally in the lateral compartment, situated between the peroneus longus and extensor digitorum longus muscles, providing essential motor innervation for foot eversion. In the distal third of the leg, it pierces the deep crural fascia to provide broad sensory coverage to the dorsum of the foot. Conversely, the deep peroneal nerve dives deep into the anterior compartment, coursing alongside the anterior tibial artery. It supplies the primary dorsiflexors—the tibialis anterior, extensor hallucis longus, and extensor digitorum longus—before terminating as a sensory branch to the highly specific first dorsal web space.
Exhaustive Indications and Contraindications
The decision to proceed with surgical exploration and reconstruction of the sciatic or peroneal nerve requires a meticulous synthesis of the mechanism of injury, serial clinical examinations, and electrodiagnostic findings. The overarching philosophy of nerve surgery dictates that intervention must occur before irreversible degradation of the distal motor endplates, yet premature exploration of a lesion destined for spontaneous recovery exposes the patient to unnecessary surgical morbidity. Therefore, the indications for surgery are broadly stratified into acute, early, and delayed interventions based on the pathology. Acute exploration (within 72 hours) is unequivocally indicated in the setting of open injuries with visually confirmed or highly suspected sharp nerve transection, such as those caused by glass lacerations or machete wounds. Similarly, an expanding hematoma in the posterior thigh or popliteal fossa causing progressive compressive neuropathy demands emergent decompression to prevent irreversible ischemic necrosis of the nerve.
Early exploration (within 3 to 6 weeks) is indicated for severe traction injuries where neurotmesis is suspected, particularly in the context of multiligamentous knee dislocations with complete foot drop and no evidence of clinical or electrical continuity. Furthermore, iatrogenic injuries recognized postoperatively—such as a complete sciatic palsy following a complex total hip arthroplasty where a suture or retractor entrapment is suspected—warrant early re-exploration if initial imaging (MRI neurography) suggests structural disruption or severe mechanical compression. Delayed exploration is the standard of care for closed, blunt trauma or traction injuries that fail to demonstrate clinical or electromyographic (EMG) improvement after 3 to 6 months of expectant management. In these scenarios, the presence of a persistent neuroma-in-continuity lacking nerve action potentials (NAPs) across the lesion dictates the need for resection and grafting.
Contraindications to surgical intervention are equally critical to delineate to avoid futile procedures. Absolute contraindications include the presence of an active, uncontrolled infection at the surgical site, which would inevitably lead to graft lysis and failure. Severe systemic medical comorbidities that preclude safe administration of prolonged general anesthesia also represent an absolute contraindication. A critical relative contraindication is the timing of presentation; patients presenting with complete motor deficits greater than 18 to 24 months post-injury are generally poor candidates for primary nerve repair or grafting. By this time, the distal musculature (e.g., the tibialis anterior) has undergone irreversible fibrotic and fatty degeneration, and reinnervation will not yield functional motor recovery. In such late presentations, the surgical algorithm must shift from nerve reconstruction to salvage procedures, such as tendon transfers or arthrodesis.
| Category | Specific Indications / Contraindications | Clinical Rationale |
|---|---|---|
| Acute Indications (< 72 hrs) | Sharp open transection, penetrating trauma, expanding hematoma, acute iatrogenic transection. | Immediate primary end-to-end epineurial repair yields the highest functional outcomes before retraction and scarring occur. |
| Delayed Indications (3-6 mos) | Closed traction injuries, blunt trauma, persistent foot drop failing conservative management, absent NAPs. | Allows time for spontaneous recovery of neuropraxia/axonotmesis. Failure to improve dictates resection of neuroma and grafting. |
| Absolute Contraindications | Active surgical site infection, severe medical instability, patient refusal. | Infection causes graft necrosis. Systemic instability precludes prolonged microsurgical procedures. |
| Relative Contraindications | Late presentation (>18-24 months post-injury), severe crush injuries with massive soft tissue loss, advanced age. | Irreversible motor endplate degradation renders nerve repair futile. Shift focus to tendon transfers or orthotic management. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough pre-operative planning is the cornerstone of successful peripheral nerve reconstruction. The initial phase involves an exhaustive clinical evaluation, focusing on precise motor grading using the Medical Research Council (MRC) scale and meticulous sensory mapping. The hallmark of a high peroneal nerve lesion is a profound foot drop, characterized by a complete inability to dorsiflex the ankle or extend the toes, coupled with absent foot eversion. The sensory examination is critical for localizing the lesion; while the superficial peroneal nerve supplies a broad area over the dorsum of the foot, the deep peroneal nerve's sensory territory is strictly confined. Testing the autonomous zone of the deep peroneal nerve—the first dorsal web space—is pathognomonic. Complete anesthesia in this highly specific wedge-shaped area, combined with foot drop, strongly localizes the lesion proximal to the bifurcation or indicates a massive combined anterior compartment injury.

Electrodiagnostic studies (EMG and NCS) are indispensable adjuncts in the pre-operative workup. Timing is crucial; an EMG performed immediately post-injury is of limited value for assessing axonal loss. However, at 3 to 4 weeks post-injury, the presence of fibrillation potentials and positive sharp waves in the denervated muscles (e.g., tibialis anterior, peroneus longus, short head of the biceps femoris) confirms Wallerian degeneration. Serial EMGs at 3 and 6 months are utilized to detect nascent motor unit action potentials (MUAPs), which herald early subclinical reinnervation and may justify continued conservative management. Advanced imaging, specifically high-resolution 3-Tesla MRI neurography, has revolutionized pre-operative templating. It allows the surgeon to visualize the exact location of the neuroma, the extent of fascicular disruption, the length of the anticipated nerve gap, and the degree of target muscle atrophy, thereby facilitating precise planning for the volume of autologous nerve graft required.
Surgical templating involves calculating the required length and number of cable grafts. For substantial defects of the sciatic or common peroneal nerve, the ipsilateral and, if necessary, contralateral sural nerves are the gold standard donor sites. The surgeon must anticipate a nerve gap that is often 20% to 30% longer than the resting defect measured on MRI, as the neuromatous ends must be resected back to healthy, bleeding fascicles ("bread-loafing"). If a 5 cm gap is anticipated in the common peroneal nerve, which typically requires 3 to 4 cable strands to match its cross-sectional area, the surgeon must plan to harvest 15 to 20 cm of sural nerve. This meticulous calculation ensures that the surgical team is prepared and that the patient is appropriately consented for donor site morbidity (loss of sensation over the lateral border of the foot).
Patient positioning and operating room setup must be meticulously orchestrated. For exploration of the sciatic nerve or the proximal common peroneal nerve, the patient is placed in the prone position on a radiolucent Jackson table with all bony prominences heavily padded. The entire affected lower extremity, from the iliac crest down to the toes, must be prepped and draped free. This circumferential draping is non-negotiable, as it allows the surgeon to dynamically flex the knee and extend the hip intraoperatively to assess tension on the nerve repair. A sterile tourniquet may be applied to the proximal thigh, though in very proximal sciatic lesions, a tourniquet may be impossible to utilize, necessitating meticulous hemostasis. The operating microscope must be positioned and balanced prior to the incision, and intraoperative nerve stimulation equipment must be tested and ready on the sterile field.
Step-by-Step Surgical Approach and Fixation Technique
The surgical approach to the sciatic and peroneal nerves demands a meticulous, extensile technique that respects the surrounding vascular structures and allows for proximal and distal control of the nerve before entering the zone of injury. For the common peroneal nerve, a curvilinear incision is utilized. It begins in the posterior thigh, tracking along the posterior border of the biceps femoris tendon, extends distally across the popliteal crease (avoiding a straight incision across the flexion crease to prevent scar contracture), and curves anteriorly over the fibular neck towards the lateral compartment of the leg. The deep fascia is incised, and the surgeon first identifies the nerve in virgin, unscarred tissue proximally in the popliteal fossa. The nerve is surrounded by a distinct fat pad in this region; once identified, it is encircled with a vessel loop for gentle, atraumatic handling. Dissection then proceeds distally, dividing the fibrous arch of the peroneus longus to completely decompress the nerve as it winds around the fibular neck.
Once the nerve is fully exposed and the zone of injury is isolated, the critical decision-making phase of neurolysis versus resection begins. If the nerve is in continuity but encased in dense epineurial scar tissue, an external neurolysis is performed under loupe or microscopic magnification. The surgeon must carefully excise the constricting fibrous bands without violating the perineurium. At this juncture, intraoperative nerve action potential (NAP) monitoring is paramount. Stimulating electrodes are placed proximal to the lesion, and recording electrodes are placed distally. If a NAP is conducted across the neuroma-in-continuity, it signifies that a functionally significant number of axons are regenerating through the scar; the nerve is left intact, and the external neurolysis is deemed sufficient. Conversely, the absence of a NAP across the lesion dictates that the neuroma is functionally impenetrable and must be resected.
The technique of nerve resection and preparation for "fixation" (neurorrhaphy) requires exacting microsurgical precision. The neuroma is sharply excised using a diamond knife or specialized nerve scissors. The proximal and distal nerve stumps are sequentially sectioned in 1-millimeter increments—a technique known as "bread-loafing"—until healthy, pouting fascicles with distinct perineurial architecture and punctate epineurial bleeding are visualized under high microscopic magnification. Failure to resect back to completely normal fascicular anatomy is the most common cause of graft failure, as regenerating axons cannot penetrate residual fibrotic tissue. Once the healthy stumps are prepared, the resulting gap is measured with the knee in a neutral or slightly flexed position to determine the surgical strategy.
If the gap is minimal (typically less than 1.5 to 2.0 cm) and the nerve ends can be coapted without any tension whatsoever, a primary end-to-end epineurial repair is performed. This is achieved using 8-0 or 9-0 non-absorbable monofilament nylon sutures, placing the initial sutures at 180 degrees to align the superficial epineurial vasculature, followed by intervening sutures to achieve a watertight seal. However, in the vast majority of traumatic sciatic and peroneal nerve injuries, a significant gap exists. In these cases, autogenous interfascicular nerve grafting is the absolute standard of care. Sural nerve cables are harvested, cut to the appropriate length (allowing for 10% redundancy to prevent tension during joint movement), and reversed in orientation to prevent regenerating motor axons from escaping down sensory side branches. The cables are interposed between the proximal and distal fascicular groups and secured with 9-0 or 10-0 microsutures. The repair is frequently augmented with a thin layer of fibrin tissue adhesive to enhance stability and seal the coaptation sites, minimizing axonal escape.
Complications, Incidence Rates, and Salvage Management
Despite flawless microsurgical technique, the management of lower extremity nerve injuries is fraught with complications, and the overall functional outcomes, particularly for proximal sciatic nerve lesions, remain historically guarded. The most profound complication is the failure of axonal regeneration to reach the distal target organs. This failure is multifactorial, stemming from severe retrograde neuronal apoptosis following high-energy proximal lesions, intraneural intermixing (where motor axons misdirect into sensory endoneurial tubes), and the sheer distance the axons must travel at a rate of 1 mm per day. Consequently, target organ atrophy frequently outpaces nerve regeneration. In complete sciatic nerve transections, functional recovery of the distally innervated anterior and lateral compartment musculature (foot and ankle dorsiflexion/eversion) is achieved in less than 30% of cases, even with optimal grafting.
Neuropathic pain and Complex Regional Pain Syndrome (CRPS) represent severely debilitating complications following both the initial injury and surgical intervention. The incidence of severe, intractable neuropathic pain following sciatic nerve trauma can approach 15% to 20%. Patients frequently describe a burning, dysesthetic pain in the distribution of the tibial or peroneal nerves, often accompanied by allodynia and hyperalgesia. Management is exceptionally challenging and requires a multimodal approach involving gabapentinoids, tricyclic antidepressants, sympathetic nerve blocks, and, in refractory cases, the implantation of spinal cord stimulators or peripheral nerve stimulators. Surgical site complications, including deep post-operative infections, hematoma formation, and wound dehiscence, occur in approximately 2% to 5% of cases. Infections are particularly catastrophic, as purulence and the associated inflammatory cascade will invariably lead to lysis of the delicate nerve repair or graft, resulting in complete failure of the reconstruction.
When primary nerve reconstruction fails, or when a patient presents too late for nerve repair (typically >18-24 months), the orthopaedic surgeon must pivot to salvage management to restore a functional, plantigrade foot. For isolated, irreversible common peroneal nerve palsy resulting in a rigid or flail foot drop, tendon transfer surgery is the gold standard salvage procedure. The classic technique involves the transfer of the robust, functioning posterior tibial tendon (PTT). The PTT is detached from its insertion on the navicular, routed through the interosseous membrane to the anterior compartment, and anchored to the lateral cuneiform or cuboid (or utilizing a "Bridle" procedure involving the tibialis anterior and peroneus longus) to restore active dorsiflexion and provide a balanced foot. This procedure yields excellent functional results and liberates the patient from the need for an Ankle-Foot Orthosis (AFO).
In scenarios of massive, combined nerve injuries (e.g., complete, irrecoverable sciatic nerve palsy) where tendon transfers are impossible due to a lack of available donor muscles, skeletal stabilization is required. Ankle arthrodesis or pantalar arthrodesis may be indicated to provide a stable, plantigrade, and braceable limb. However, the surgeon must be acutely aware of the insensate nature of the plantar aspect of the foot in combined sciatic lesions. An insensate foot is at extreme risk for neuropathic ulceration, Charcot arthropathy, and subsequent deep osteomyelitis. In cases where the limb is completely flail, insensate, and plagued by intractable neuropathic pain or recurrent life-threatening infections, below-knee or above-knee amputation remains a definitive, albeit final, salvage option that can significantly improve the patient's overall quality of life and mobility with a modern prosthesis.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Management / Treatment |
|---|---|---|---|
| Failure of Regeneration (Foot Drop) | 60-70% (Proximal lesions) | Distance to target, motor endplate atrophy, severe intraneural scarring. | Posterior Tibial Tendon (PTT) transfer through interosseous membrane; AFO bracing. |
| Neuropathic Pain / CRPS | 15-20% | Incomplete nerve lesions, neuroma formation, central sensitization. | Multimodal pharmacotherapy, sympathetic blocks, Spinal Cord Stimulation (SCS). |
| Graft / Repair Rupture | 1-3% | Premature mobilization, excessive tension at repair site, inadequate immobilization. | Re-exploration and revision grafting (prognosis significantly worsened). |
| Neuropathic Ulceration | 10-15% (Tibial involvement) | Loss of protective sensation on the plantar aspect of the foot. | Aggressive wound care, total contact casting, eventual arthrodesis or amputation if osteomyelitis develops. |
Phased Post-Operative Rehabilitation Protocols
The post-operative rehabilitation following major lower extremity nerve reconstruction is a highly structured, protracted process that demands absolute compliance from the patient and meticulous oversight by the surgical and physical therapy teams. The immediate post-operative immobilization strategy is paramount to protect the delicate neurorrhaphy from catastrophic tension. Following a primary repair of the sciatic nerve, where mobilization of the nerve ends was required, the limb must be immobilized in a manner that introduces maximum slack into the neuroaxis. This historically dictates the application of a double spica cast extending from the nipple line to the toes on the affected side, with the hip extended and the knee flexed to 60-90 degrees. While autogenous nerve grafting is inherently tension-free and may preclude the need for extreme joint positioning, rigid immobilization in a long-leg splint or cast with the knee in slight flexion remains mandatory for the first 3 to 4 weeks to allow for initial vascularization and structural integration of the grafts.
Phase I of the rehabilitation protocol (0 to 6 weeks) is characterized by strict protection. The patient is maintained in a non-weight-bearing status on the operative extremity. Edema control is critical, utilizing elevation and compressive stockings on the uninjured segments of the limb. During this phase, physical therapy is restricted to active and passive range of motion of the non-immobilized joints (e.g., toes, and the contralateral limb) to prevent global deconditioning and deep vein thrombosis. Wound care is meticulously managed, with sutures typically removed through a window in the cast or splint at 14 to 21 days post-operatively, given that incisions across the popliteal fossa are prone to delayed healing.
Phase II (6 to 12 weeks) marks the transition to gradual, protected mobilization. The rigid cast is removed and replaced with a custom-molded, long-leg hinged brace. The critical objective during this phase is to slowly stretch the regenerating nerve and the surrounding soft tissues without inducing traction injury at the coaptation sites. The knee hinge is adjusted to allow gradual extension, typically advancing 10 to 15 degrees per week. Aggressive passive stretching is strictly contraindicated. Concurrently, the patient may begin progressive partial weight-bearing as tolerated, utilizing crutches or a walker. During this period, an Ankle-Foot Orthosis (AFO) is prescribed and fitted to compensate for the persistent foot drop, preventing Achilles tendon contracture and allowing for a more normalized, energy-efficient gait while awaiting nerve regeneration.
Phase III (3 months and beyond) focuses on aggressive functional rehabilitation, sensory re-education, and long-term monitoring. Once full joint extension is achieved, physical therapy intensifies to restore full passive and active range of motion to the hip, knee, and ankle joints. Electrical muscle stimulation (EMS) may be employed on the denervated musculature (e.g., tibialis anterior) in an attempt to delay muscle atrophy, although its definitive efficacy remains debated in the literature. The surgeon monitors clinical progress by tracking the advancing Tinel's sign along the course
