Combined Hammer and Mallet Toe Deformity with Double Corns: Surgical Management
Key Takeaway
Combined hammer and mallet toe deformities present with minimal metatarsophalangeal extension but significant proximal and distal interphalangeal flexion. This leads to painful hyperkeratotic lesions, or double corns, over bony prominences. Management requires a thorough biomechanical evaluation to differentiate between hard, soft, and plantar corns. Operative intervention, including targeted condylectomies, resection arthroplasties, and partial syndactylization, is indicated when conservative measures fail, ensuring meticulous bone resection to prevent recurrence.
PATHOMECHANICS OF COMBINED HAMMER TOE AND MALLET TOE DEFORMITY
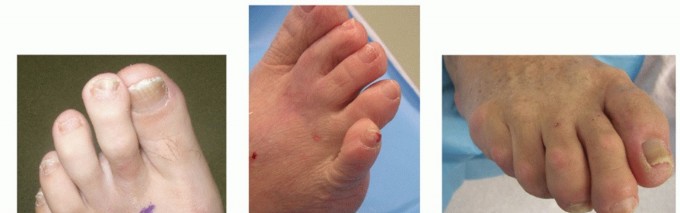
The combined hammer toe and mallet toe deformity, frequently presenting with associated double corns, represents a distinct biomechanical entity in forefoot pathology. It differs fundamentally from the traditional claw toe deformity in that there is minimal to no extension deformity at the metatarsophalangeal (MTP) joint. Instead, the primary deforming forces are concentrated distally, resulting in rigid flexion contractures at both the proximal interphalangeal (PIP) and distal interphalangeal (DIP) joints.
Because of this dual-level contracture, the toe is subjected to abnormal shear and compressive forces within the shoe. Large, prominent hyperkeratotic lesions—double corns—typically develop over the dorsal aspects of both the PIP and DIP joints. The management of these lesions requires a deep understanding of the underlying osseous prominences. In a retrospective review of combined DIP and PIP resection arthroplasties, Oliver et al. reported a 10% recurrence rate at the PIP joint, which they attributed directly to inadequate bone resection during the index procedure.

ETIOLOGY AND CLINICAL FINDINGS OF CORNS (HELOMATA AND CLAVI)
Corns are hyperkeratotic lesions occurring over bony prominences, involving the hypertrophy of the stratum corneum (the horny layer) of the skin in response to repetitive mechanical stress. Clinically, corns are classified into distinct morphological types based on their location, moisture content, and underlying biomechanical drivers. Both hard and soft corns are caused by pressure from unyielding structures, but their clinical presentations dictate different surgical approaches.
Hard Corns (Heloma Durum)
In hard corns, the phalangeal condyle beneath the skin and an unyielding shoe toe box over the skin generate intense pressure and friction. Over time, a painful, circumscribed lesion develops. The most common anatomical location is over the dorsolateral aspect of the PIP joint of the fifth toe.
Clinically, the lesion is firm, dry, and exquisitely tender to direct palpation. If the corn becomes acutely irritated, surrounding erythema, localized heat, and swelling are present. In chronic cases, an adventitial bursa may develop between the skin and the underlying bone, which can periodically become inflamed or infected.

Clinical Pearl: Differentiating Warts from Hard Corns
A plantar wart (verruca plantaris) should never be mistaken for a hard corn. Gentle paring of the lesion with a scalpel is diagnostic. Paring a wart reveals vertical blood vessels that present as punctate bleeding points. Paring a corn reveals layers of clear, avascular keratin.

Soft Corns (Heloma Molle / Interdigital Corns)
A soft corn is almost exclusively interdigital. The term "interdigital corn" is anatomically more descriptive than "soft corn." The macerated, soft appearance is secondary to the trapped moisture of the web space rather than a difference in the primary pathology. There are two primary types of interdigital corns:
- Distal Web Corn: The most common type, located in the distal portion of the web. It involves the base of the distal phalanx of the shorter toe abutting the head of the proximal phalanx of the longer toe. Occasionally, a dystrophic nail can produce the pressure necessary for this lesion to develop.
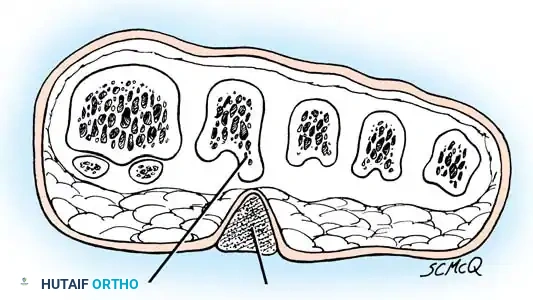
- Deep Web Space Corn: Slightly less common but significantly more troublesome, occurring at the base of the web space (most commonly the fourth web space).
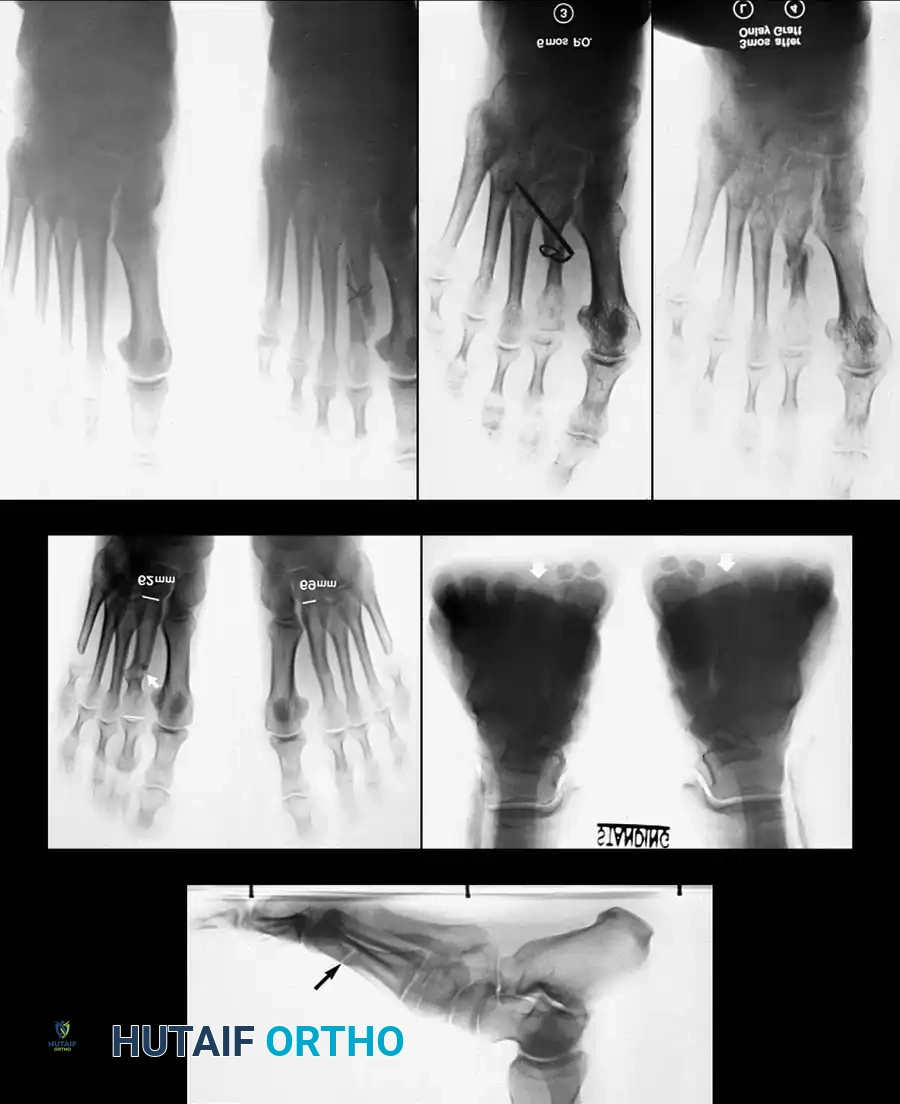
Deep web space corns are frequently associated with an abnormally short fifth metatarsal and occasionally with hallux valgus, which causes lateral adduction pressure on the fifth toe from the shoe. The lesion results from a "pincer" effect: pressure imposed by the lateral side of the base of the fourth proximal phalanx, the medial condyle of the head of the fifth proximal phalanx, or both.

Moisture softens the hyperkeratotic area, and occasionally a sinus tract develops between the central part of the corn and the deep web space. When this occurs, suppuration usually follows.
Surgical Warning: The Diabetic Foot
In a diabetic or immunocompromised patient, an infected soft corn is a limb-threatening emergency. This relatively minor lesion can rapidly progress to deep space infection, osteomyelitis, and catastrophic tissue loss if not aggressively managed.

Plantar Corns (Intractable Plantar Keratosis)
The plantar corn is another variant of a hard corn (heloma durum and clavus durus). Patients occasionally present with a circumscribed plug of keratin that has recently been plucked from the center of an isolated, hyperkeratotic lesion. These are located beneath a metatarsal head, usually of the lesser toes, just plantar to the prominent fibular side of the condyle of the metatarsal head (which projects more plantar than the tibial side).
If the lesion occurs beneath the first metatarsal head, it is usually under the tibial sesamoid. Mann and DuVries referred to a plantar corn that failed to respond to conservative treatment as an intractable plantar keratosis (IPK), or a localized invaginated callus, distinguishing between localized and diffuse lesions.

Neurovascular Corns
A rare but highly symptomatic lesion is the neurovascular corn. It is exquisitely painful and usually located beneath the first or fifth metatarsal head. It is frequently confused with a plantar wart. Gentle paring of the lesion reveals poorly demarcated edges with blood vessels that lie parallel to the plantar surface of the foot, as opposed to the vertical orientation of vessels seen in a plantar wart.
NONOPERATIVE MANAGEMENT
Keratotic lesions should be managed nonoperatively until the patient has exhausted conservative modalities. Patient education and physician assiduity are essential.
* Shoe Modification: A shoe with a wide, deep toe box is mandatory to eliminate dorsal and lateral friction.
* Padding and Sleeves: We recommend a digital sleeve with a friction-absorbing pad consisting of medical-grade paraffin (Silipos).
* Web Space Hygiene: For soft corns, the web spaces must be washed twice daily with household soap and dried completely. An antifungal/antibacterial powder and lamb’s wool, or a self-adherent rubber web spacer, should be applied.
If these measures fail to relieve symptoms or become too time-consuming for the patient on a daily basis, surgical treatment is warranted.
SURGICAL MANAGEMENT: HARD CORNS
Because the most common location of a hard corn is over the dorsolateral side of the PIP joint of the fifth toe, the procedure for this location is described below; however, the principles apply to all lesser toes. Coughlin and Kennedy reported the treatment of 31 lateral fifth toe corns with lateral condylectomy and flexor tenotomy, or complete condylectomy (hammer toe repair) for more severe deformities, yielding 97% good or excellent subjective ratings.

🔪 Surgical Technique 80-8: Resection Arthroplasty for Hard Corns
- Anesthesia and Positioning: Administer a digital block using local anesthesia. Apply a sterile digital tourniquet at the base of the toe.
- Incision: Make a dorsolateral incision skirting the medial border of the corn. Begin 5 to 6 mm proximal to the nail fold and extend proximally for approximately 1.5 cm.
- Exposure: Deepen the incision through the subcutaneous tissue, taking care to protect the dorsal cutaneous nerves. Retract the extensor tendon medially to expose the PIP joint capsule.
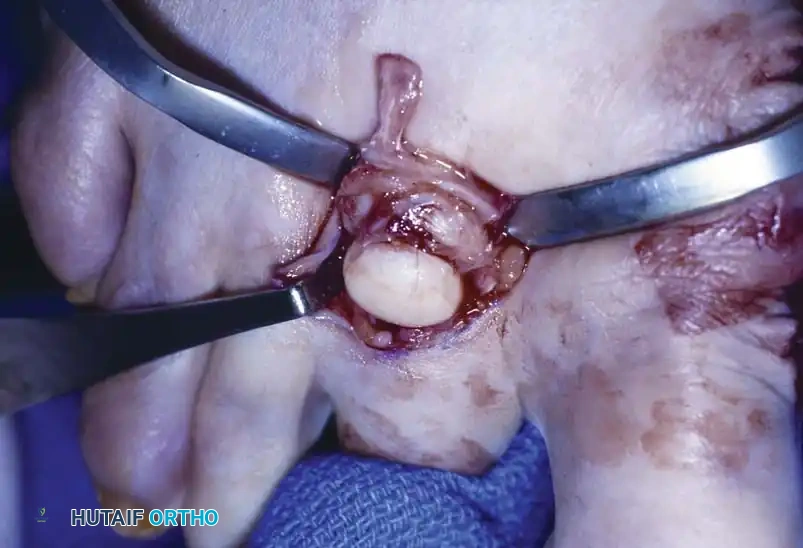
- Bone Resection: Remove the bony prominence on the dorsolateral aspect of the condyle of the proximal phalanx by sharp dissection with a small-blade knife. Using a rongeur or a small sagittal saw, resect any bony prominence from the adjacent side of the middle phalangeal base.
- Assessment of Resection: Palpation of this area after removing the prominence is far more revealing than visual inspection. Ensure that absolutely no bony prominence remains. If necessary, resect the entire head and neck of the proximal phalanx.
- Complete Resection (Hammer Toe Repair): Resection of the head and neck of the proximal phalanx more reliably prevents recurrence and is the most commonly utilized procedure for rigid deformities. While this creates instability at the resected PIP joint, this annoyance is mitigated by appropriate postoperative taping.
Surgical Warning: Inadequate Resection
If only the lateral bony prominence is removed (simple condylectomy), it is wise to inform the patient preoperatively of a higher possible recurrence rate and the potential later need for a formal resection arthroplasty.
Postoperative Protocol for Hard Corns
- Dressings: Apply a non-adherent dressing and a mild compressive wrap.
- Weight-Bearing: A wooden-soled postoperative shoe, or any shoe with the toe box removed laterally, is worn for 3 to 4 weeks.
- Splinting: Following the initial 3 to 4 weeks, tape splinting (buddy taping) is utilized for an additional 3 to 4 weeks to stabilize the pseudoarthrosis.
- Patient Education: Enlargement and swelling of the toe frequently persist for weeks or even months after the procedure. Because the toes lack a thick soft-tissue envelope, acute or chronic edema has "no place to hide." Informing the patient preoperatively of this prolonged swelling prevents postoperative misunderstanding and anxiety.
SURGICAL MANAGEMENT: SOFT CORNS (INTERDIGITAL CORNS)
Soft corns usually located in the fourth interdigital space are caused by underlying pressure from the medial flare of the base of the distal phalanx of the fifth toe abutting the PIP joint of the fourth toe. This problem can only be resolved surgically by removing the underlying bony conflict.
Appreciating bony prominences by palpation and inspection is notoriously difficult in the web space. Separating the toes draws the corn into the center of the web space; however, in a shod, weight-bearing position, the corn is actually superficial to the lateral base of the proximal phalanx of the fourth toe.
If the corn remains painful, becomes infected, or ulcerates despite conservative care, operative treatment is justified. Coughlin and Kennedy reported simple condylectomies and hammer toe repairs for interdigital corns with a 97% success rate.
Clinical Pearl: Managing Web Space Ulcerations
Surgery should never be performed through a moist, weeping ulcer. The web space must first be treated with drying agents, antibacterial solutions, and a spacer (such as lamb’s wool) until the web space is completely dry. Ulcers should not be primarily closed; they heal rapidly by secondary intention once the underlying bony pressure is removed.
🔪 Surgical Technique 80-9: Bony Resection and Partial Syndactylization
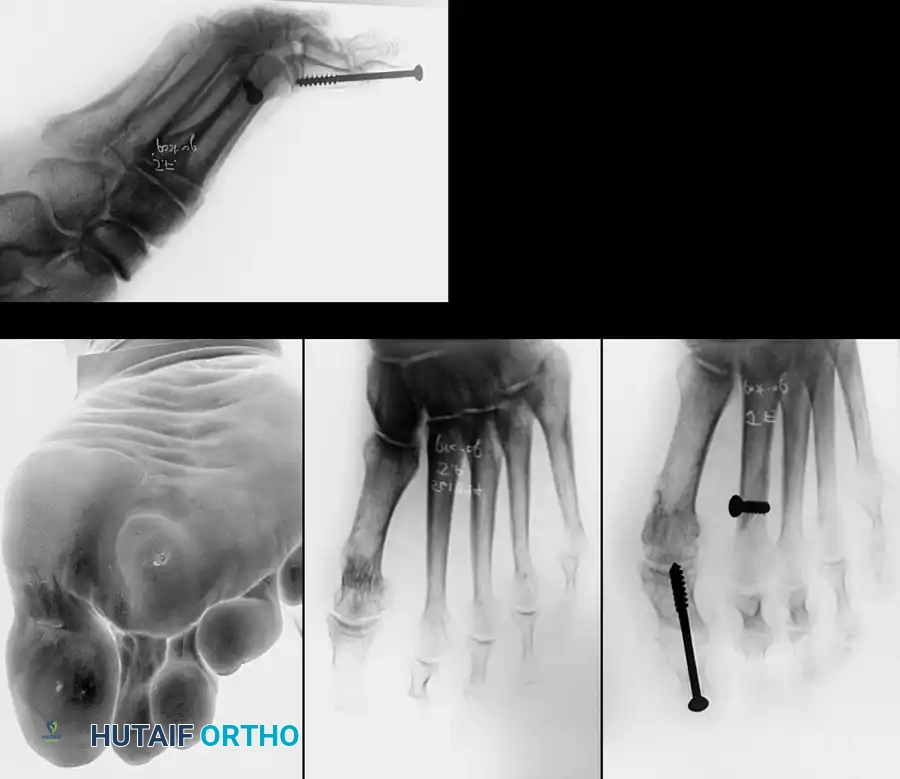
A web space corn is highly prone to recurrence if adequate bone is not removed. Resecting the lateral flare of the base of the proximal phalanx of the fourth toe flush with the diaphysis, or removing the head and neck of the proximal phalanx of the fifth toe, may be curative. Occasionally, both must be resected. For recurrent or intractable interdigital corns, a partial, simple syndactylization is highly effective.

- Incision Design: Make a dorsal longitudinal incision extending into the plantar portion of the interdigital space. Extend the two limbs into the adjacent sides of the plantar third of the opposing toes. Placing the digital limbs of the incision on the adjacent plantar sides retains the cosmetic cleft the patient sees from the dorsal aspect.
- Bone Resection (Fourth Toe): If the center of the hyperkeratotic area is more on the fourth phalangeal side, resect the lateral flare of the base of the proximal phalanx of the fourth toe flush with the diaphysis (Fig. 80-26A).
- Bone Resection (Fifth Toe): If the lesion is more on the fifth toe side, resect the medial portion of the head of the proximal phalanx of the fifth toe (Fig. 80-26B). This can be done through a dorsal transverse elliptical incision or a dorsolateral curved incision.
- Palpation: Palpate the web space after resection to determine if any residual bony impingement exists. If the resection seems inadequate, the opposite bony offender must be resected.
- Syndactylization Closure: Close the wound beginning proximally and extending distally, suturing the dorsal limbs together (Fig. 80-26C). Excise a small amount of skin at the apex of the dorsal skin
Associated Surgical & Radiographic Imaging
📚 Medical References
You Might Also Like