Arthroscopic Wafer Procedure & TFCC Debridement
Key Takeaway
The combined arthroscopic wafer distal ulnar resection and TFCC debridement is a minimally invasive technique for treating ulnocarpal impaction syndrome with central TFCC tears. By resecting the distal ulna through the TFCC defect, surgeons decompress the ulnocarpal joint while preserving the distal radioulnar joint ligaments. This guide details the step-by-step arthroscopic technique, biomechanical principles, and the modified Sauvé-Kapandji procedure for chronic derangement.
INTRODUCTION AND BIOMECHANICAL RATIONALE
Ulnocarpal impaction syndrome (UIS) is a degenerative condition caused by excessive load transmission across the ulnar aspect of the wrist, leading to progressive deterioration of the triangular fibrocartilage complex (TFCC), the chondral surfaces of the ulnar head, and the ulnar carpus (lunate and triquetrum). Biomechanical studies by Palmer and Werner established that in a wrist with neutral ulnar variance, the radius absorbs approximately 80% of the axial load, while the ulna absorbs 20%. However, an increase in ulnar variance of merely 2.5 mm shifts the load distribution dramatically, increasing the ulnar load transmission to 42%.
The Combined Arthroscopic “Wafer” Distal Ulnar Resection and Triangular Fibrocartilage Complex Débridement, popularized by Tomaino and Weiser, offers a joint-preserving, minimally invasive alternative to formal ulnar shortening osteotomy. By resecting the distal 2 to 3 mm of the ulnar dome directly through a central TFCC defect, the surgeon effectively decompresses the ulnocarpal joint. This technique avoids the morbidity of a diaphyseal osteotomy, eliminates the need for internal fixation, and allows for concurrent management of intra-articular pathology.
💡 Clinical Pearl: Indications vs. Contraindications
Indications: Ulnocarpal impaction syndrome with positive ulnar variance of less than 3 mm, accompanied by a central, non-repairable TFCC tear (Palmer Class 2C or 2D), with a stable and congruent distal radioulnar joint (DRUJ).
Contraindications: Ulnar variance exceeding 3 to 4 mm (where an ulnar shortening osteotomy is preferred), DRUJ arthritis, DRUJ instability, or a peripheral TFCC tear that is amenable to primary repair.
PREOPERATIVE PREPARATION AND PATIENT POSITIONING
Meticulous setup is paramount for successful wrist arthroscopy. The procedure is typically performed under regional anesthesia (supraclavicular or axillary block) or general anesthesia, depending on patient factors and surgeon preference.
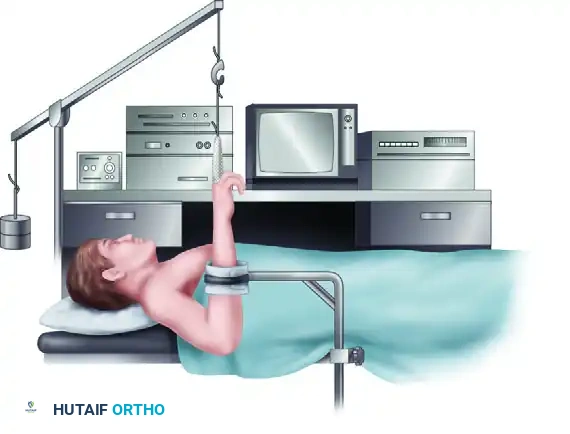
- Positioning: Place the patient supine on the operating table with the operative arm extended on a radiolucent hand table.
- Tourniquet: Apply a well-padded pneumatic tourniquet to the proximal arm. Exsanguinate the limb and inflate the tourniquet to 250 mm Hg.
- Traction Setup: Apply sterile fingertraps to the index and middle fingers. Suspend the arm using a wrist arthroscopy tower. Maintain longitudinal traction of 4.5 to 5.5 kg (10 to 12 lb). This specific weight is critical; inadequate traction prevents joint visualization, while excessive traction risks iatrogenic neuropraxia or ligamentous distraction.
- Countertraction: Apply a countertraction strap across the distal biceps, securing it to the table.
SURGICAL TECHNIQUE: ARTHROSCOPIC WAFER RESECTION AND TFCC DÉBRIDEMENT
Step 1: Joint Distension and Portal Placement
Accurate portal placement is the foundation of wrist arthroscopy. The radiocarpal joint must be adequately distended to prevent iatrogenic scuffing of the articular cartilage during trocar insertion.
- Distension: Distend the radiocarpal joint with 5 to 10 mL of sterile saline solution injected through the anatomic snuffbox or directly into the 3-4 portal site.
- Viewing Portal: Incise the skin longitudinally over the 3-4 portal (located between the extensor pollicis longus [EPL] and the extensor digitorum communis [EDC]). Use a mosquito hemostat to bluntly dissect the subcutaneous tissues, protecting the terminal branches of the superficial radial nerve. Insert a 2.7-mm, 30-degree arthroscope.
- Outflow: Establish outflow to maintain a clear visual field. Insert an 18-gauge needle into the radiostyloid-scaphoid joint space.
- Working Portals: Establish the 4-5 portal (between the EDC and extensor digiti minimi [EDM]) and the 6R portal (radial to the extensor carpi ulnaris [ECU] tendon) under direct intra-articular visualization.
Step 2: Diagnostic Arthroscopy and Soft Tissue Débridement
Perform a systematic diagnostic sweep of the radiocarpal joint. Evaluate the articular surfaces of the scaphoid, lunate, and radius.
- Assess the intrinsic ligaments. Use the 6R and the 4-5 portals as working portals for scapholunate and lunotriquetral evaluation.
- If partial, stable scapholunate or lunotriquetral tears are identified, débride the frayed margins using a 2.0-mm or 2.9-mm motorized shaver to prevent mechanical catching.
Step 3: TFCC Preparation
The central articular disc of the TFCC is avascular and incapable of healing; therefore, central tears (Palmer 2C/2D) are treated with excision rather than repair.
- Using a motorized shaver or arthroscopic punch through the 4-5 or 6R portal, excise enough of the central, degenerative triangular fibrocartilage disc to fully expose the underlying ulnar head.
- Critical Anatomy: The peripheral margins of the TFCC must be meticulously preserved. The dorsal and volar radioulnar ligaments (DRUL and VRUL) are the primary stabilizers of the DRUJ.
⚠️ Surgical Warning: Ligamentous Preservation
Avoid aggressive resection at the periphery. Iatrogenic injury to the dorsal and volar radioulnar ligaments, or their deep foveal attachments at the base of the ulnar styloid, will result in catastrophic, iatrogenic DRUJ instability. Resect only the central, avascular horizontal portion of the disc.
Step 4: Arthroscopic Wafer Resection (Ulnar Head Resection)
Once the ulnar head is exposed through the central TFCC window, the bony resection commences. The goal is to resect 2 to 3 mm of the distal ulna, converting a positive ulnar variance to a neutral or slightly negative variance.
- Instrumentation: Through the 6R portal, introduce a 2.0-mm or 2.9-mm shielded arthroscopic burr.
- Resection Trajectory: Begin the resection on the radial side of the ulnar head. Remove the cartilage and subchondral bone to a depth equal to the width of the 2-mm burr. This resection must occur strictly beneath the margin of the sigmoid notch at the medial (ulnar) edge of the lunate fossa of the radius.
- Medial Progression: Gradually move the burr more medially, toward the base of the ulnar styloid. Carefully remove the ulnar head dome.
- Sub-TFCC Resection: To achieve adequate decompression, place the burr beneath the remaining intact peripheral triangular fibrocartilage. This allows for the removal of the ulnar head proximal to (beneath) the TFCC, extending to the base of the ulnar styloid.
- Verification: Release the traction temporarily and passively pronate and supinate the wrist while viewing through the arthroscope. Ensure there is no residual impingement between the ulnar head and the carpus throughout the arc of motion.
ADVANCED RECONSTRUCTION: THE MODIFIED SAUVÉ-KAPANDJI PROCEDURE
While the arthroscopic wafer procedure is excellent for mild ulnocarpal impaction with an intact DRUJ, patients presenting with chronic posttraumatic derangement of the DRUJ, severe DRUJ osteoarthritis, or fixed DRUJ instability require a more robust reconstructive salvage procedure.
The Sauvé-Kapandji procedure involves an arthrodesis of the DRUJ combined with a proximal ulnar pseudarthrosis to restore forearm rotation. However, the classic technique is frequently complicated by painful instability of the proximal ulnar stump. To address this, the Modified Sauvé-Kapandji Procedure (Lamey and Fernandez) incorporates soft-tissue stabilization of the proximal stump.
Surgical Technique 69-35: Modified Sauvé-Kapandji
Step 1: Approach and Arthrodesis
- Make a dorsal longitudinal incision over the DRUJ, operating through the fifth extensor compartment.
- Expose the distal ulna and the DRUJ. Decorticate the articular cartilage of the ulnar head and the corresponding sigmoid notch of the radius to expose bleeding subchondral bone.
- Perform the ulnar neck osteotomy. Resect a segment of the ulnar neck to create a gap measuring exactly 10 mm. This gap is critical to prevent bony impingement during forearm rotation.
- Reduce the ulnar head into the sigmoid notch in neutral rotation. Fix the arthrodesis using two 3.5-mm or 2.7-mm cortical lag screws.
Step 2: Interposition and Stump Stabilization
To prevent heterotopic ossification and stabilize the proximal ulnar segment, soft tissue interposition and tenodesis are performed.
- Pronator Quadratus Interposition: Mobilize the pronator quadratus muscle and interpose it into the 10-mm nonunion gap. This acts as a biological spacer.
- FCU Tenodesis: To address proximal stump instability, harvest a distally based slip of the flexor carpi ulnaris (FCU) tendon. Route this slip through a drill hole in the proximal ulnar segment to tether and stabilize it.
- Capsular Closure: Suture the interposed pronator quadratus to the tendon sheath of the extensor carpi ulnaris (ECU) muscle to complete the soft tissue envelope.
FIGURE 69-73A: Posterior view of the wrist demonstrating the modified Sauvé-Kapandji procedure. Two cortical screws rigidly fix the ulnar head to the sigmoid notch of the radius. Following the ulnar neck resection, a 10 mm gap is created and meticulously filled with the pronator quadratus muscle to prevent bony regrowth and impingement.
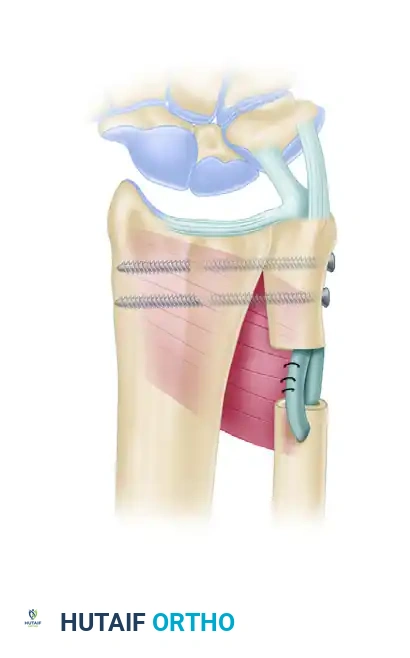
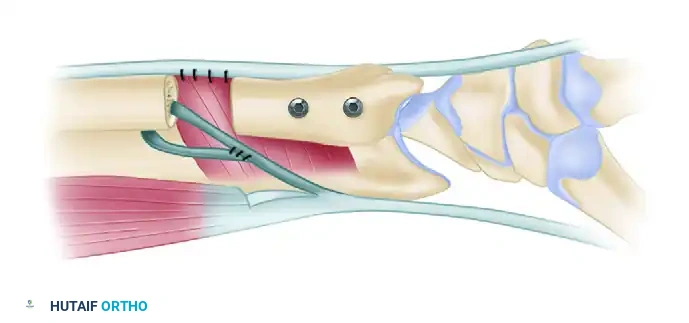
FIGURE 69-73B: Lateral view of the wrist illustrating the critical stabilization of the proximal ulnar segment. A distally based slip of the flexor carpi ulnaris (FCU) tendon is utilized to tether the proximal stump, preventing dynamic instability. The nonunion gap remains filled with the pronator quadratus, which is securely sutured to the tendon sheath of the extensor carpi ulnaris (ECU) muscle. (Adapted from Lamey DM, Fernandez DL: Results of the modified Sauvé-Kapandji procedure in the treatment of chronic posttraumatic derangement of the distal radioulnar joint, J Bone Joint Surg 80A:1758, 1998.)
POSTOPERATIVE REHABILITATION PROTOCOL
Arthroscopic Wafer Procedure
- Days 1-10: The wrist is immobilized in a bulky soft dressing and a volar short-arm splint. Immediate active range of motion (ROM) of the digits is encouraged to prevent tendon adhesions and reduce edema.
- Weeks 2-4: The splint is removed, and sutures are extracted. The patient is transitioned to a removable wrist orthosis. Gentle, active wrist flexion, extension, pronation, and supination are initiated under the guidance of a certified hand therapist.
- Weeks 4-8: Passive ROM and progressive strengthening exercises are introduced. Heavy lifting and forceful gripping are restricted until 8 weeks postoperatively.
- Return to Play/Work: Most patients achieve maximal medical improvement and return to unrestricted activities between 10 and 12 weeks.
Modified Sauvé-Kapandji Procedure
- Weeks 1-4: The patient is placed in a Muenster-style or long-arm cast to restrict forearm rotation and protect the arthrodesis and soft-tissue tenodesis.
- Weeks 4-8: Transition to a short-arm cast or rigid splint. Radiographs are obtained to confirm the progression of the DRUJ arthrodesis. Gentle active forearm rotation is initiated.
- Weeks 8-12: Once radiographic union of the DRUJ is confirmed, progressive strengthening begins. The patient is monitored for any signs of proximal stump instability or radioulnar impingement.
COMPLICATIONS AND PITFALLS
- Inadequate Resection (Wafer): The most common cause of failure in the arthroscopic wafer procedure is under-resection of the ulnar head, leading to persistent ulnocarpal impaction. The surgeon must ensure a full 2 to 3 mm of bone is removed, particularly at the volar-ulnar aspect, which is difficult to visualize.
- DRUJ Instability (Wafer): Overzealous use of the burr or shaver can damage the deep fibers of the radioulnar ligaments. If iatrogenic instability occurs, open repair or reconstruction may be necessitated.
- Proximal Stump Instability (Sauvé-Kapandji): Even with the modified FCU tenodesis, patients may experience dynamic convergence of the proximal ulna toward the radius during heavy lifting. Precise creation of the 10-mm gap and robust soft-tissue interposition are critical to minimizing this complication.
- Nonunion of Arthrodesis (Sauvé-Kapandji): Failure of the ulnar head to fuse to the sigmoid notch can result in painful hardware and persistent symptoms. Meticulous decortication down to bleeding subchondral bone and rigid lag screw fixation are mandatory.
You Might Also Like