
Caltrate 600+D3: An Expert Medical SEO Guide to Optimal Bone Health
1. Comprehensive Introduction & Overview
Welcome to the definitive medical guide on Caltrate 600+D3, a cornerstone supplement in the maintenance of skeletal health. As expert Medical SEO Copywriters and Orthopedic Specialists, we understand the critical role calcium and Vitamin D play in preventing and managing a myriad of bone-related conditions. This exhaustive guide is meticulously crafted to provide healthcare professionals, patients, and caregivers with an authoritative, in-depth understanding of Caltrate 600+D3, encompassing its scientific underpinnings, clinical applications, safety profile, and practical usage.
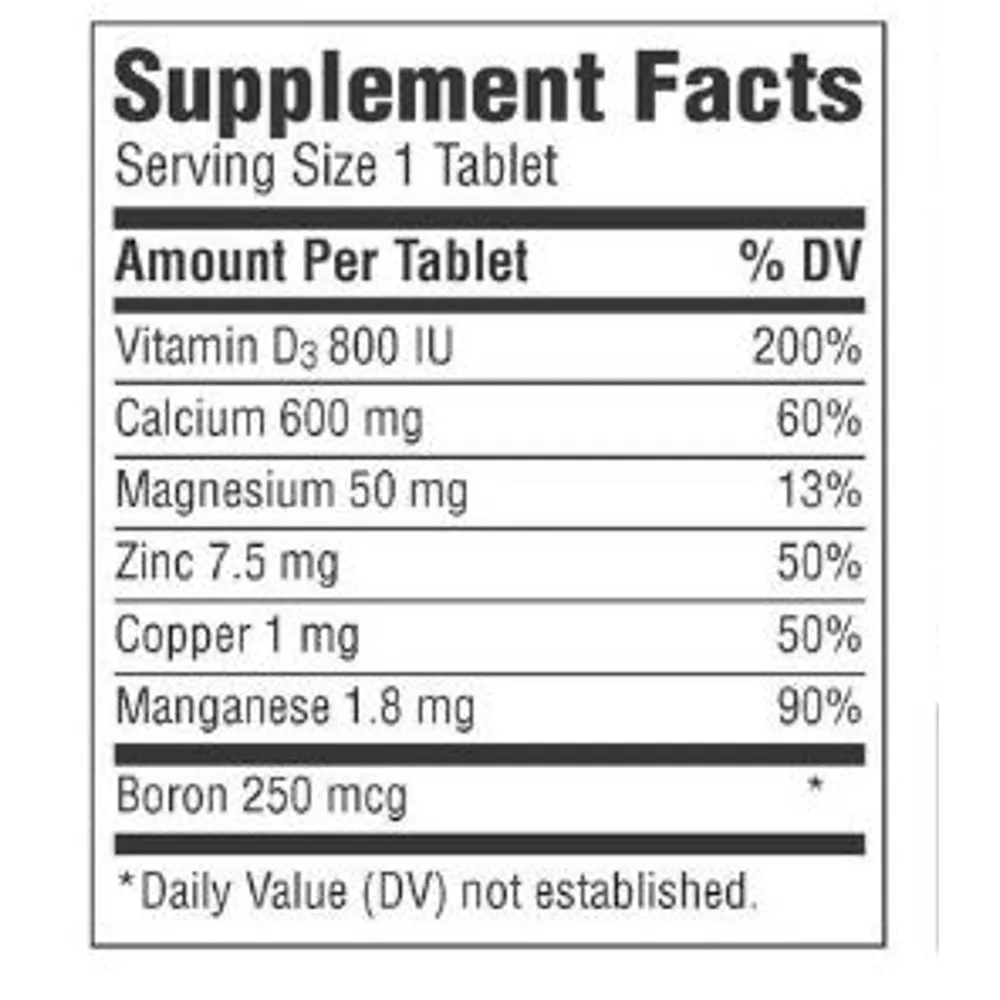
Caltrate 600+D3 is a widely recognized dietary supplement formulated to provide essential calcium and Vitamin D3. Each tablet typically contains 600 mg of elemental calcium (as calcium carbonate) and 800 IU (International Units) of Vitamin D3 (cholecalciferol). This combination is crucial because while calcium is the primary building block of bone, Vitamin D3 is indispensable for its efficient absorption and utilization within the body. In an era where osteoporosis and osteopenia are increasingly prevalent, understanding and effectively utilizing supplements like Caltrate 600+D3 is paramount for promoting lifelong bone vitality and reducing fracture risk.
This guide will delve into the intricate mechanisms by which Caltrate 600+D3 supports bone health, explore its pharmacokinetic profile, detail its extensive clinical indications, outline precise dosage guidelines, highlight potential risks and contraindications, discuss critical drug interactions, and provide essential information regarding its use during pregnancy and lactation, as well as strategies for overdose management. Our aim is to empower you with comprehensive knowledge, ensuring informed decisions regarding bone health supplementation.
2. Deep-dive into Technical Specifications / Mechanisms
2.1. Composition and Formulation
Caltrate 600+D3 primarily consists of two active ingredients:
* Calcium Carbonate: This is a highly concentrated form of calcium, providing a significant amount of elemental calcium per tablet. In Caltrate 600+D3, "600" refers to 600 mg of elemental calcium. Calcium carbonate requires stomach acid for optimal absorption, making it advisable to take with food.
* Vitamin D3 (Cholecalciferol): The "D3" signifies the presence of cholecalciferol, the naturally occurring form of Vitamin D produced in the skin upon exposure to sunlight. The "800" typically refers to 800 International Units (IU) of Vitamin D3, a potent dose designed to support calcium absorption and bone mineralization.
The tablets are formulated for ease of administration, often with a protective coating to facilitate swallowing. Inactive ingredients (excipients) vary by specific product version but generally include agents for binding, disintegration, and coating, ensuring stability and bioavailability.
2.2. Mechanism of Action
The synergistic action of calcium and Vitamin D3 is fundamental to their efficacy in bone health.
2.2.1. Calcium Carbonate
Calcium is the most abundant mineral in the human body, with approximately 99% stored in the bones and teeth, providing structural rigidity. The remaining 1% is found in the blood and soft tissues, where it plays vital roles in numerous physiological processes:
* Bone Mineralization: Calcium forms hydroxyapatite crystals, the primary mineral component of bone, providing strength and structure. Adequate calcium intake is essential for bone formation and remodeling throughout life.
* Nerve Transmission: Calcium ions are crucial for the release of neurotransmitters and the propagation of nerve impulses.
* Muscle Contraction: Calcium triggers muscle contraction in both skeletal and cardiac muscle.
* Blood Clotting: Calcium is a vital co-factor in the coagulation cascade.
* Hormone Secretion: It plays a role in the secretion of various hormones and enzymes.
* Calcium Homeostasis: The body tightly regulates serum calcium levels through a complex interplay of hormones, primarily parathyroid hormone (PTH), calcitonin, and activated Vitamin D. When dietary calcium is insufficient, PTH stimulates calcium release from bones, which can lead to bone demineralization over time.
2.2.3. Vitamin D3 (Cholecalciferol)
Vitamin D3, or cholecalciferol, is a fat-soluble vitamin that acts as a prohormone. Its primary role in bone health is to regulate calcium and phosphate metabolism:
* Activation: Cholecalciferol is biologically inert until it undergoes two hydroxylation steps. First, in the liver, it is converted to 25-hydroxyvitamin D [25(OH)D], also known as calcidiol, which is the main circulating form and indicator of Vitamin D status. Second, in the kidneys, 25(OH)D is further hydroxylated to 1,25-dihydroxyvitamin D [1,25(OH)2D], or calcitriol, the biologically active form.
* Enhanced Intestinal Absorption: Active Vitamin D (calcitriol) significantly enhances the absorption of dietary calcium and phosphate from the small intestine. This is its most critical function for bone health.
* Renal Reabsorption: Calcitriol also promotes the reabsorption of calcium and phosphate in the kidneys, preventing their excessive loss in urine.
* Bone Remodeling: Vitamin D directly influences osteoblasts (bone-forming cells) and osteoclasts (bone-resorbing cells), playing a crucial role in bone remodeling processes. It helps maintain a healthy balance between bone formation and resorption.
* Other Roles: Beyond bone health, Vitamin D is increasingly recognized for its roles in immune function, cell growth regulation, and neuromuscular function.
2.3. Pharmacokinetics
2.3.1. Absorption
- Calcium Carbonate: Absorption of calcium carbonate is optimal when taken with food, as gastric acid facilitates its dissolution and subsequent absorption in the small intestine. The elemental calcium is absorbed via both active transport (saturable, Vitamin D-dependent) and passive paracellular diffusion (non-saturable). Bioavailability can range from 20-30%.
- Vitamin D3: Being fat-soluble, cholecalciferol is absorbed from the small intestine into the lymphatic system, primarily within chylomicrons. Bile salts are essential for its emulsification and absorption. Malabsorption syndromes (e.g., celiac disease, Crohn's disease, cystic fibrosis) or conditions affecting bile production can impair Vitamin D absorption.
2.3.2. Distribution
- Calcium: Approximately 99% of total body calcium is stored in the bones. The remaining 1% circulates in the extracellular fluid, with about 40-45% bound to plasma proteins (primarily albumin), 10-15% complexed with anions (citrate, phosphate), and 45-50% as free ionized calcium, which is the biologically active form.
- Vitamin D3: Cholecalciferol and its metabolites circulate bound to Vitamin D-binding protein (DBP). It is stored primarily in adipose tissue and muscle, allowing for sustained release.
2.3.3. Metabolism
- Calcium: Calcium itself is not metabolized in the traditional sense but is constantly exchanged between bone and extracellular fluid.
- Vitamin D3: Cholecalciferol undergoes hydroxylation in the liver to 25-hydroxyvitamin D [25(OH)D]. This 25(OH)D is then transported to the kidneys, where it undergoes a second hydroxylation by 1-alpha-hydroxylase to form the active hormone 1,25-dihydroxyvitamin D [1,25(OH)2D]. The activity of 1-alpha-hydroxylase is tightly regulated by PTH, phosphate, and fibroblast growth factor 23 (FGF23).
2.3.4. Excretion
- Calcium: Unabsorbed dietary calcium is excreted in the feces. Absorbed calcium is primarily excreted via the kidneys, with a small amount lost in sweat. Renal excretion is regulated by PTH and calcitriol.
- Vitamin D3: Vitamin D and its metabolites, particularly inactive forms, are primarily excreted in the bile and subsequently in the feces. A small amount is excreted renally.
3. Extensive Clinical Indications & Usage
Caltrate 600+D3 is indicated for a broad range of conditions where calcium and Vitamin D supplementation is necessary.
3.1. Primary Indications
- Osteoporosis Prevention and Treatment:
- Postmenopausal Osteoporosis: Women after menopause experience accelerated bone loss due to decreased estrogen levels. Caltrate 600+D3 helps mitigate this loss and reduce fracture risk.
- Age-Related Osteoporosis (Senile Osteoporosis): As individuals age, bone density naturally declines. Supplementation is crucial for both men and women.
- Secondary Osteoporosis: Caused by underlying medical conditions (e.g., hyperthyroidism, chronic kidney disease) or medications (e.g., corticosteroids). Caltrate 600+D3 is often used as an adjunct to primary therapy.
- Osteopenia: A condition characterized by bone density that is lower than normal but not yet severe enough to be classified as osteoporosis. Supplementation can help prevent progression to osteoporosis.
- Calcium Deficiency (Hypocalcemia):
- Dietary Insufficiency: Individuals with inadequate dietary intake of calcium (e.g., those avoiding dairy, vegans) benefit significantly.
- Malabsorption Syndromes: Conditions like celiac disease, inflammatory bowel disease, or gastric bypass surgery can impair calcium absorption, necessitating supplementation.
- Certain Medical Conditions: Hypoparathyroidism, chronic kidney disease, or pancreatitis can lead to hypocalcemia.
- Vitamin D Deficiency:
- Insufficient Sun Exposure: Common in individuals living in higher latitudes, those with limited outdoor activity, or who consistently use sunscreen.
- Dietary Insufficiency: Few foods naturally contain significant Vitamin D.
- Impaired Absorption/Metabolism: Liver or kidney disease, certain anticonvulsants, or obesity can impair Vitamin D metabolism.
- Adjuvant Therapy: Often prescribed alongside other anti-resorptive medications like bisphosphonates (e.g., alendronate, risedronate), denosumab, or teriparatide to ensure adequate substrate for bone formation and reduce the risk of secondary hyperparathyroidism.
3.2. Other Potential Uses
- Fracture Healing Support: Adequate calcium and Vitamin D are essential for optimal bone repair and remodeling following fractures.
- Muscle Cramps: In cases where muscle cramps are related to hypocalcemia, supplementation may provide relief.
- Certain Parathyroid Disorders: Under strict medical supervision, Caltrate 600+D3 may be used in managing conditions like secondary hyperparathyroidism.
3.3. Dosage Guidelines
The recommended dosage of Caltrate 600+D3 varies based on individual needs, dietary intake, age, and underlying medical conditions. Always follow the advice of a healthcare professional.
| Patient Population | Typical Daily Dosage (Elemental Calcium & Vitamin D3) | Administration Notes |
|---|---|---|
| General Adults | 600 mg Calcium + 800 IU Vitamin D3 (1 tablet) | Usually once daily. May be split into two doses (e.g., 300mg Ca + 400 IU D3 twice daily) for better absorption if higher total doses are needed. |
| Postmenopausal Women | 600-1200 mg Calcium + 800-1000 IU Vitamin D3 | Often one tablet daily, sometimes two if dietary intake is very low, or as part of a combination therapy. |
| Elderly (>70 years) | 1000-1200 mg Calcium + 800-1000 IU Vitamin D3 | Increased need due to reduced calcium absorption and Vitamin D synthesis. |
| Patients on Corticosteroids | May require higher doses, as advised by physician. | Corticosteroids can impair calcium absorption and increase excretion. |
Important Administration Considerations:
* Take with Food: Calcium carbonate absorption is enhanced by stomach acid. Taking Caltrate 600+D3 with a meal optimizes absorption and may reduce gastrointestinal side effects.
* Adequate Fluid Intake: Drink a full glass of water with each dose.
* Avoid Exceeding Recommended Dose: Excessive intake of calcium and Vitamin D can lead to hypercalcemia and other adverse effects.
* Separate Doses: If taking more than 600 mg of elemental calcium daily, it is often recommended to split the dose (e.g., two tablets at different meals) to maximize absorption, as the body can only absorb a limited amount of calcium at one time.
3.4. Monitoring Parameters
For individuals on long-term Caltrate 600+D3 therapy, especially those with pre-existing conditions or on other medications, regular monitoring is crucial:
* Serum Calcium Levels: Both total and ionized calcium levels should be monitored to prevent hypercalcemia.
* Serum 25-hydroxyvitamin D [25(OH)D] Levels: To ensure adequate Vitamin D status and avoid deficiency or excess.
* Bone Mineral Density (BMD) Scans (DEXA): Periodically to assess the effectiveness of therapy in preventing or treating bone loss.
* Renal Function: Serum creatinine and estimated glomerular filtration rate (eGFR) should be monitored, particularly in elderly patients or those with kidney impairment, due to the risk of hypercalcemia and nephrolithiasis.
4. Risks, Side Effects, and Contraindications
While generally safe and well-tolerated, Caltrate 600+D3 is not suitable for everyone and can cause side effects.
4.1. Contraindications
Caltrate 600+D3 should not be used in individuals with:
* Hypercalcemia: Pre-existing abnormally high levels of calcium in the blood.
* Hypercalciuria: Excessive calcium excretion in the urine.
* Severe Renal Impairment: Patients with end-stage renal disease or significant kidney dysfunction are at increased risk of hypercalcemia and hyperphosphatemia.
* Known Hypersensitivity: Allergy to any component of Caltrate 600+D3 (calcium carbonate, cholecalciferol, or inactive ingredients).
* Nephrolithiasis (Kidney Stones): History of calcium-containing kidney stones. Use with extreme caution and under medical supervision, as supplementation can exacerbate this condition.
* Primary Hyperparathyroidism: A condition causing excessive PTH production, leading to hypercalcemia.
4.2. Potential Side Effects
Most side effects are mild and gastrointestinal in nature:
* Gastrointestinal:
* Constipation (most common)
* Bloating
* Gas (flatulence)
* Stomach upset/discomfort
* Nausea
* Renal:
* Increased risk of kidney stones (nephrolithiasis), especially in predisposed individuals or with high doses.
* Metabolic:
* Hypercalcemia: Rare at recommended doses but can occur with overdose or in individuals with pre-existing conditions that impair calcium regulation. Symptoms include:
* Anorexia, nausea, vomiting
* Muscle weakness, fatigue
* Polyuria (increased urination), polydipsia (increased thirst)
* Mental disturbances (confusion, lethargy)
* Cardiac arrhythmias (in severe cases)
4.3. Drug Interactions
Caltrate 600+D3 can interact with several medications, potentially altering their absorption or efficacy, or increasing the risk of adverse effects. It is crucial to inform your healthcare provider about all medications and supplements you are taking.
| Drug Class / Medication | Interaction Mechanism | Management / Recommendation |
|---|---|---|
| Tetracycline Antibiotics | Calcium can chelate (bind to) tetracyclines, reducing their absorption and effectiveness. | Separate administration by at least 2-4 hours before or after Caltrate 600+D3. |
| Fluoroquinolone Antibiotics | Similar to tetracyclines, calcium can chelate fluoroquinolones (e.g., ciprofloxacin, levofloxacin). | Separate administration by at least 2-6 hours before or after Caltrate 600+D3. |
| Thyroid Hormones (Levothyroxine) | Calcium can impair the absorption of levothyroxine, making it less effective. | Administer levothyroxine at least 4 hours before or after Caltrate 600+D3. |
| Bisphosphonates | Calcium can interfere with the absorption of bisphosphonates (e.g., alendronate, risedronate). | Take Caltrate 600+D3 at least 30-60 minutes after the bisphosphonate, or as specifically advised by your doctor (often several hours later). |
| Thiazide Diuretics | Can decrease urinary calcium excretion, increasing the risk of hypercalcemia. | Monitor serum calcium levels closely, especially at the start of co-administration and during dose adjustments. |
| Corticosteroids | Can decrease intestinal calcium absorption and increase renal calcium excretion, potentially worsening bone loss. | May require higher doses of calcium and Vitamin D supplementation. Consult your physician. |
| Digoxin | Hypercalcemia (even mild) can increase the risk of digoxin toxicity, leading to cardiac arrhythmias. | Use with extreme caution. Monitor serum calcium and digoxin levels closely, and perform regular ECGs. |
| Mineral Oil, Cholestyramine | These agents can impair the absorption of fat-soluble vitamins, including Vitamin D. | Separate administration. Consider alternative laxatives if mineral oil is used long-term. |
| Phenytoin, Barbiturates | Can increase the metabolism of Vitamin D, potentially reducing its effectiveness. | May require higher doses of Vitamin D supplementation. Monitor Vitamin D levels. |
| Iron Supplements | Calcium can inhibit iron absorption. | Separate administration by at least 2 hours. |
4.4. Pregnancy and Lactation Warnings
- Pregnancy: Adequate calcium and Vitamin D are crucial during pregnancy for fetal skeletal development and maternal bone health. However, excessive intake of Vitamin D can be teratogenic (cause birth defects). It is essential to adhere to recommended daily allowances and consult a healthcare professional before taking Caltrate 600+D3 during pregnancy, especially if already taking prenatal vitamins containing these nutrients.
- Lactation: Both calcium and Vitamin D pass into breast milk. At recommended doses, Caltrate 600+D3 is generally considered safe for breastfeeding mothers and helps ensure adequate nutrient levels for the infant. However, as with pregnancy, consultation with a physician is advised to prevent excessive intake.
4.5. Overdose Management
Acute or chronic overdose of Caltrate 600+D3 can lead to hypercalcemia and hypervitaminosis D.
4.5.1. Symptoms of Hypercalcemia/Hypervitaminosis D
Symptoms can be non-specific and range from mild to severe:
* Early/Mild: Anorexia, nausea, vomiting, constipation, abdominal pain, muscle weakness, fatigue, headache, polyuria, polydipsia (excessive thirst).
* Severe: Mental disturbances (confusion, lethargy, stupor, coma), nephrocalcinosis (calcium deposits in kidneys) leading to renal impairment, cardiac arrhythmias, hypertension, dehydration.
4.5.2. Treatment of Overdose
Management of hypercalcemia involves:
1. Discontinuation: Immediately stop Caltrate 600+D3 and any other calcium or Vitamin D supplements.
2. Hydration: Rehydration with intravenous (IV) normal saline is the cornerstone of treatment to increase urinary calcium excretion.
3. Loop Diuretics: After adequate rehydration, loop diuretics (e.g., furosemide) may be administered to further promote calcium excretion, but only after ensuring the patient is not dehydrated.
4. Corticosteroids: Can be used to reduce intestinal calcium absorption.
5. Bisphosphonates: Intravenous bisphosphonates (e.g., pamidronate, zoledronic acid) may be used in severe cases to inhibit bone resorption and lower serum calcium.
6. Calcitonin: Can rapidly but transiently lower serum calcium levels.
7. Dialysis: In severe, life-threatening hypercalcemia, especially with renal failure, hemodialysis may be necessary.
8. Monitoring: Close monitoring of serum calcium, phosphorus, magnesium, renal function (creatinine, BUN), and electrocardiogram (ECG) is essential.
5. Massive FAQ Section
Q1: What is Caltrate 600+D3 used for?
A1: Caltrate 600+D3 is primarily used to supplement calcium and Vitamin D intake, preventing and treating conditions like osteoporosis, osteopenia, and deficiencies in calcium or Vitamin D. It supports bone health, density, and strength.
Q2: How should I take Caltrate 600+D3?
A2: It is generally recommended to take Caltrate 600+D3 with food to enhance calcium absorption. Swallow the tablet whole with a full glass of water. Follow the specific dosage instructions provided by your healthcare professional or on the product label.
Q3: Can I take Caltrate 600+D3 if I have kidney stones?
A3: If you have a history of kidney stones, particularly calcium-containing stones, you should use Caltrate 600+D3 with extreme caution and only under the strict supervision of a healthcare professional. Calcium supplementation can increase the risk of stone formation in predisposed individuals.
Q4: What are the common side effects of Caltrate 600+D3?
A4: The most common side effects are mild gastrointestinal issues such as constipation, bloating, gas, stomach upset, and nausea. These can often be minimized by taking the supplement with food and adequate fluid intake.
Q5: Can Caltrate 600+D3 interact with other medications?
A5: Yes, Caltrate 600+D3 can interact with several medications, including certain antibiotics (tetracyclines, fluoroquinolones), thyroid hormones (levothyroxine), bisphosphonates, and thiazide diuretics. Always inform your doctor or pharmacist about all medications and supplements you are taking to avoid potential interactions. Often, separating the administration times is sufficient.
Q6: Is Caltrate 600+D3 suitable for pregnant or breastfeeding women?
A6: While calcium and Vitamin D are essential during pregnancy and lactation, it's crucial to consult a healthcare professional before taking Caltrate 600+D3. They can advise on the appropriate dosage, considering your dietary intake and any other prenatal supplements, to avoid excessive intake.
Q7: How long does it take for Caltrate 600+D3 to work?
A7: Caltrate 600+D3 works by providing the body with the necessary building blocks for bone health. While you won't feel immediate changes, consistent and long-term use, typically over months to years, is required to see measurable benefits in bone mineral density and to reduce fracture risk. Regular bone density scans (DEXA) can monitor its long-term effectiveness.
Q8: What is the difference between calcium carbonate and calcium citrate?
A8: Calcium carbonate, found in Caltrate 600+D3, contains a higher percentage of elemental calcium (about 40%) but requires stomach acid for absorption, so it's best taken with food. Calcium citrate contains less elemental calcium (about 21%) but can be absorbed efficiently with or without food, making it a good option for individuals with low stomach acid.
Q9: Do I need a prescription for Caltrate 600+D3?
A9: No, Caltrate 600+D3 is an over-the-counter (OTC) dietary supplement and does not require a prescription. However, it is strongly recommended to consult a healthcare professional before starting any new supplement, especially if you have underlying health conditions or are taking other medications.
Q10: What should I do if I miss a dose?
A10: If you miss a dose, take it as soon as you remember, unless it is almost time for your next scheduled dose. In that case, skip the missed dose and continue with your regular dosing schedule. Do not double the dose to make up for a missed one.
Q11: How much elemental calcium is in Caltrate 600+D3?
A11: Each tablet of Caltrate 600+D3 contains 600 mg of elemental calcium, derived from calcium carbonate.
Q12: Can men take Caltrate 600+D3?
A12: Absolutely. While often associated with women, men also experience bone loss with age and are susceptible to osteoporosis and Vitamin D deficiency. Caltrate 600