Sacroiliac (SI) Joint Fixation Screws: A Comprehensive Patient Guide
1. Comprehensive Introduction & Overview
The sacroiliac (SI) joint is a crucial, yet often overlooked, component of the human skeletal system. Located where the sacrum (the triangular bone at the base of the spine) meets the ilium (the large, flaring bone of the pelvis), these two joints play a vital role in weight-bearing, shock absorption, and transferring forces between the upper body and the legs. While designed for stability, the SI joints allow for a small degree of movement.
However, when these joints become dysfunctional—either too stiff (hypomobility) or too loose (hypermobility)—they can become a significant source of chronic pain, often radiating to the lower back, buttocks, groin, or even down the leg. This condition, known as SI joint dysfunction or sacroiliitis, can be debilitating, severely impacting a patient's quality of life.
For patients experiencing severe, chronic SI joint pain that has not responded to extensive conservative treatments (such as physical therapy, medications, and injections), sacroiliac (SI) joint fixation screws offer a highly effective surgical solution. These specialized orthopedic implants are designed to stabilize the SI joint, reduce painful motion, and promote long-term fusion (arthrodesis) of the joint. The primary goal is to alleviate pain, restore function, and significantly improve a patient's overall well-being.
This comprehensive guide will delve into the intricacies of SI joint fixation screws, covering their design, clinical applications, biomechanics, and the patient outcomes they aim to achieve.
2. Deep-dive into Technical Specifications / Mechanisms
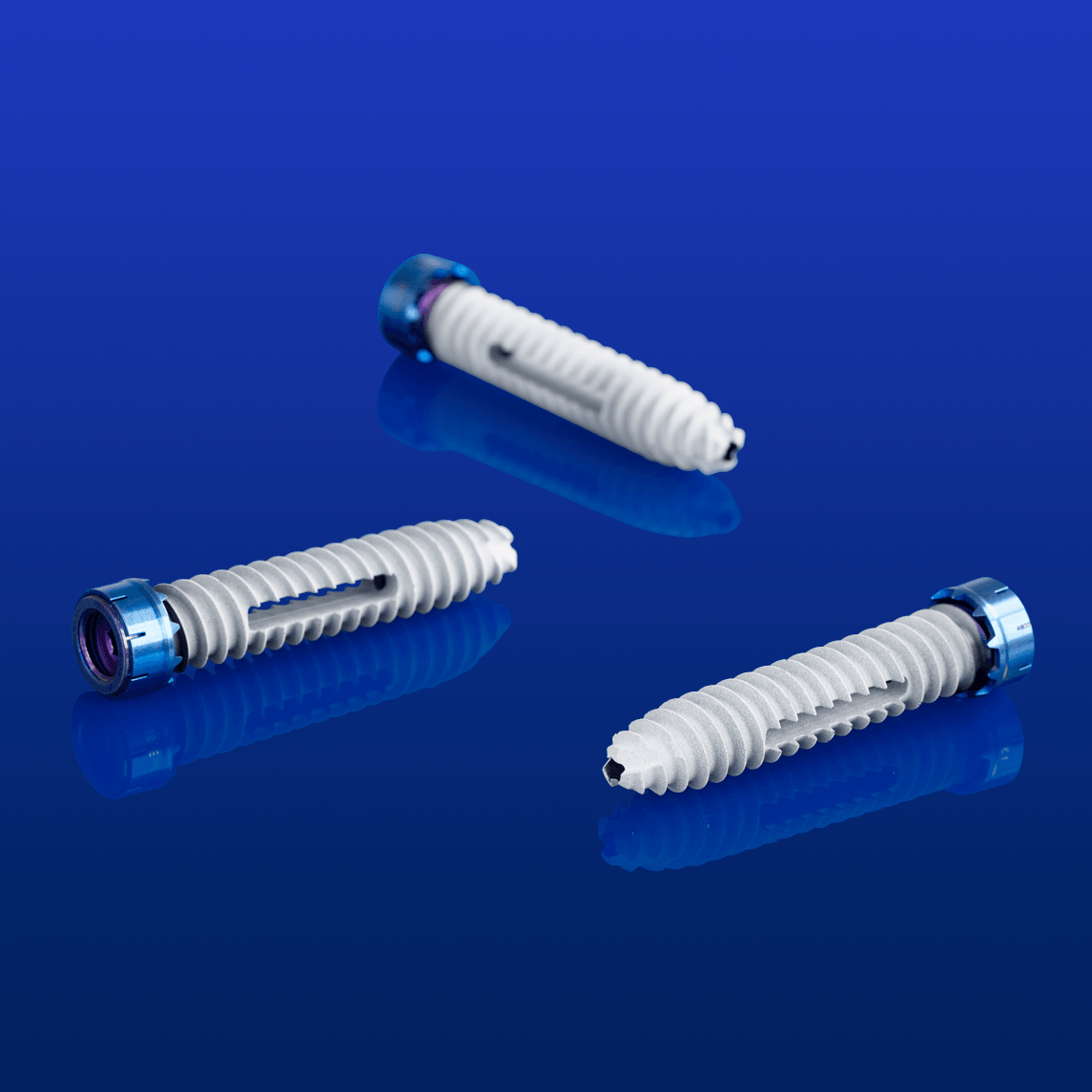
SI joint fixation screws are precision-engineered devices crucial for achieving stable arthrodesis. Their effectiveness lies in their advanced design and material properties.
Design and Materials
The choice of materials and specific design features are paramount for the success and longevity of SI joint fixation.
- Materials:
- Titanium Alloys (e.g., Ti-6Al-4V): The most common material due to its exceptional biocompatibility, high strength-to-weight ratio, and excellent corrosion resistance. Titanium also allows for MRI compatibility, which is crucial for post-operative imaging.
- Stainless Steel (e.g., 316L): Less commonly used for primary implants due to lower biocompatibility compared to titanium and potential MRI artifacts, but still found in some orthopedic applications.
- Surface Treatments: Some screws may feature porous or textured surfaces, or even bioactive coatings, to enhance osteointegration (the direct structural and functional connection between living bone and the surface of a load-bearing implant).
- Screw Types and Features:
- Cannulated Screws: These screws feature a hollow core, allowing them to be inserted over a guidewire. This technique is highly beneficial in minimally invasive surgery (MIS) as it enables precise placement under fluoroscopic (X-ray) guidance, minimizing tissue disruption.
- Self-Tapping / Self-Drilling Screws: Designed with specific tip geometries that eliminate the need for pre-drilling or tapping in some bone types, streamlining the surgical procedure.
- Thread Design:
- Fully Threaded: Threads extend along the entire length of the screw, providing consistent purchase.
- Partially Threaded: Threads are present only at the distal (far) end. This design allows for compression across the joint, drawing the two bone surfaces together to promote fusion.
- Diameter and Length: Screws come in various diameters (e.g., 7.0mm to 12.0mm) and lengths (e.g., 30mm to 100mm), allowing the surgeon to select the optimal size based on the patient's anatomy, bone density, and the specific surgical approach.
- Head Design: Low-profile heads minimize prominence and potential soft tissue irritation.
- System Components: Some SI joint fusion systems utilize a combination of screws, sometimes with an additional plate or specialized implants, to achieve multi-planar stability.
Mechanism of Action
The fundamental mechanism of SI joint fixation screws is to create a stable construct across the dysfunctional joint, thereby eliminating painful motion and encouraging bone growth across the joint space.
- Stabilization: By rigidly connecting the sacrum and ilium, the screws immediately reduce abnormal movement within the SI joint. This provides instant mechanical stability.
- Compression: Partially threaded screws, when tightened, can draw the two joint surfaces together, creating compression. This compression is crucial for promoting bone fusion, as it facilitates direct bone-to-bone contact and healing.
- Arthrodesis Promotion: The ultimate goal is arthrodesis, or surgical fusion. By maintaining stability and compression, the screws create an optimal biological environment for new bone to grow across the joint space, permanently uniting the sacrum and ilium. This process can take several months.
- Load Sharing: The screws help redistribute mechanical loads more evenly across the pelvic ring, reducing localized stress on the previously painful SI joint.
Biomechanics
Understanding the biomechanics of the SI joint and how screws influence it is key to appreciating their role in treatment.
- Complex Anatomy: The SI joint is inherently complex, with irregular surfaces and strong ligamentous support. It experiences significant shear and compressive forces during daily activities.
- Restoring Pelvic Ring Integrity: The SI joints are critical for the stability of the pelvic ring. Dysfunction can compromise this integrity. Fixation screws restore this stability, allowing for more efficient force transfer.
- Minimizing Micromotion: Excessive micromotion at the SI joint is a primary cause of pain. Screws effectively limit this motion, reducing inflammation and pain signals.
- Optimizing Fusion Environment: Biomechanically, a stable, compressed environment is ideal for bone fusion. The screws provide this stability, preventing motion that could disrupt bone healing.
- Avoiding Stress Shielding: Modern screw designs and appropriate sizing aim to provide sufficient stability without completely "stress shielding" the bone, which could lead to bone weakening over time. The goal is to allow physiological loading while the fusion process occurs.
3. Extensive Clinical Indications & Usage
SI joint fixation screws are reserved for specific patients after thorough diagnostic evaluation and failure of non-surgical treatments.
Clinical Indications
Patients considered for SI joint fixation typically present with:
- Chronic SI Joint Pain: Pain localized to the SI joint region, lasting for more than 6 months, and significantly impacting daily activities.
- Failed Conservative Treatment: Documented failure of a comprehensive course of non-surgical therapies, including:
- Physical therapy (strengthening, stretching, manual therapy).
- Anti-inflammatory medications (NSAIDs).
- Corticosteroid injections into the SI joint (providing temporary relief but not sustained).
- Radiofrequency ablation (if previously attempted).
- Diagnosed SI Joint Dysfunction/Sacroiliitis:
- Positive findings on provocative physical examination tests (e.g., Faber test, Gaenslen's test, thigh thrust test).
- Imaging evidence (X-rays, CT scans, MRI) showing degenerative changes, inflammation, or instability.
- Diagnostic SI joint injection (anesthetic injection into the joint) providing significant, temporary pain relief (typically >50-75%), confirming the SI joint as the primary pain generator.
- Traumatic SI Joint Instability: Following pelvic fractures or trauma that has compromised the SI joint ligaments, leading to chronic instability and pain.
- Degenerative Sacroiliitis: Age-related wear and tear leading to cartilage degeneration and bone-on-bone friction.
- Sacral Fractures: Fractures extending into the SI joint that require stabilization.
- Adjacent Segment Disease/Failed Back Surgery Syndrome: In some cases, after lumbar spinal fusion, increased stress on the SI joint can lead to new pain. If the SI joint is confirmed as the pain source, fusion may be indicated.
- Certain Inflammatory Conditions: For severe, intractable SI joint pain associated with conditions like ankylosing spondylitis, where the joint is significantly inflamed and unstable.
Surgical Applications (Fitting/Usage Instructions)
The most common method for SI joint fixation using screws is a minimally invasive approach. This technique aims to reduce tissue disruption, blood loss, and recovery time compared to traditional open surgery.
Pre-operative Planning:
- Comprehensive Evaluation: Detailed medical history, physical examination, and review of all imaging studies (X-rays, CT, MRI).
- Diagnostic Injections: Crucial for confirming the SI joint as the pain source.
- Surgical Templating: Using imaging (CT scans) to plan the optimal screw trajectory, length, and diameter, ensuring safe and effective placement.
The Minimally Invasive Surgical Procedure:
- Anesthesia: General anesthesia is typically administered.
- Patient Positioning: The patient is positioned face down (prone) on a specialized surgical table, allowing for optimal access to the posterior pelvis.
- Incision: A small incision (typically 2-3 cm) is made over the posterior aspect of the ilium, away from the midline of the spine.
- Fluoroscopic Guidance: Real-time X-ray imaging (fluoroscopy) is continuously used throughout the procedure to guide instrument placement and ensure accuracy.
- Guidewire Placement: A guidewire is carefully advanced across the SI joint, from the ilium into the sacrum, under fluoroscopic visualization. This is the critical first step for precise screw placement.
- Serial Dilation: A series of dilators are advanced over the guidewire to create a working channel to the SI joint without large muscle dissection.
- Drilling/Tapping (if needed): Depending on the screw type and bone density, the surgeon may drill a pilot hole or tap the bone to prepare for screw insertion.
- Screw Insertion: The cannulated SI joint fixation screws are carefully advanced over the guidewire, across the SI joint, and into the sacrum. Typically, 2-3 screws are placed to achieve robust fixation. The number and exact placement depend on the patient's anatomy and the surgeon's preference.
- Confirmation of Placement: Post-insertion fluoroscopic images are taken in multiple planes to confirm optimal screw position, ensuring no impingement on nerves or blood vessels.
- Wound Closure: The small incision is closed with sutures or surgical staples.
Post-operative Care and Rehabilitation:
- Initial Recovery: Patients usually spend one night in the hospital. Pain management is crucial.
- Weight-Bearing Restrictions: Depending on the surgeon's protocol and bone quality, patients may have partial weight-bearing restrictions for a few weeks, gradually progressing to full weight-bearing. Crutches or a walker may be used initially.
- Physical Therapy: A structured physical therapy program is essential for restoring strength, flexibility, and proper movement patterns. This typically begins a few weeks post-surgery.
- Activity Restrictions: Patients are advised to avoid heavy lifting, twisting, and impact activities for several months to allow for solid fusion.
Maintenance/Sterilization Protocols (for the implants)
It's important for patients to understand that the implants themselves are handled with the utmost care to ensure patient safety and surgical efficacy.
- Single-Use & Pre-Sterilized: SI joint fixation screws are manufactured as single-use devices and are delivered to the hospital in sterile packaging. They undergo rigorous sterilization processes (e.g., gamma irradiation or ethylene oxide) by the manufacturer.
- Sterile Field: During surgery, strict aseptic techniques are maintained. The screws are only opened from their sterile packaging within a sterile field in the operating room, just prior to implantation.
- Quality Control: Manufacturers adhere to stringent quality control standards (e.g., ISO 13485) to ensure the integrity, sterility, and performance of each implant.
4. Risks, Side Effects, or Contraindications
While SI joint fixation surgery is generally safe and effective, like any surgical procedure, it carries potential risks and contraindications.
General Surgical Risks:
- Infection: Risk of infection at the surgical site.
- Bleeding: Intraoperative or post-operative hematoma formation.
- Anesthesia Risks: Adverse reactions to anesthesia.
- Deep Vein Thrombosis (DVT) / Pulmonary Embolism (PE): Blood clot formation.
Specific Risks Related to SI Joint Fixation Screws:
- Screw Malposition: Incorrect placement of screws can lead to:
- Nerve Irritation/Damage: Particularly to the sacral nerve roots, causing new pain, numbness, weakness, or bowel/bladder dysfunction.
- Vascular Injury: Damage to nearby blood vessels (e.g., internal iliac vessels).
- Inadequate Fixation: If screws are not optimally placed, they may not provide sufficient stability, leading to persistent pain or non-union.
- Screw Loosening or Breakage: Over time, especially if fusion does not occur, screws can loosen or, rarely, fracture due to repetitive stress. This may necessitate revision surgery.
- Non-Union (Failure of Fusion): Despite fixation, the bones may not fuse together, leading to continued pain. This is more common in patients with poor bone quality (e.g., osteoporosis) or those who do not adhere to post-operative restrictions.
- Persistent Pain: Even with successful fusion, some patients may experience residual pain due to other factors or adjacent segment issues.
- Hardware Prominence: The screws may be palpable under the skin, or cause irritation to surrounding soft tissues, occasionally requiring removal after fusion is complete.
- Allergic Reaction: Very rare, but possible reaction to the implant material.
Contraindications:
- Active Systemic or Local Infection: Surgery should be postponed until any infection is fully resolved.
- Severe Osteoporosis: Extremely poor bone quality may not provide adequate purchase for the screws, increasing the risk of loosening or failure.
- Pregnancy: Elective surgery is generally contraindicated during pregnancy.
- Uncontrolled Systemic Diseases: Conditions such as uncontrolled diabetes, severe cardiovascular disease, or bleeding disorders may increase surgical risks.
- Unclear Pain Source: If diagnostic tests (especially diagnostic injections) do not clearly identify the SI joint as the primary pain generator, surgery is not indicated.
- Morbid Obesity: May increase surgical complexity and risks, though not an absolute contraindication for all patients.
5. Expert Tips from Dr. Mohammed Hutaif
As an orthopedic specialist, Dr. Mohammed Hutaif emphasizes several key aspects for patients considering or undergoing SI joint fixation:
- Accurate Diagnosis is Paramount: "The success of SI joint fusion hinges on a precise diagnosis. We must be absolutely certain that the SI joint is the primary source of your pain. This often involves a meticulous clinical examination, specific provocative tests, and critically, a diagnostic SI joint injection that provides significant temporary relief."
- Consider all Conservative Options First: "Surgery is a last resort. I always advocate for a comprehensive trial of conservative therapies, including targeted physical therapy, anti-inflammatory medications, and image-guided injections. Only after these have failed to provide lasting relief should surgical intervention be considered."
- Understand the Minimally Invasive Advantage: "Minimally invasive SI joint fusion techniques, utilizing cannulated screws, have revolutionized this procedure. They allow for precise screw placement with smaller incisions, less muscle disruption, reduced blood loss, and typically a faster recovery compared to traditional open approaches."
- Realistic Expectations are Key: "While SI joint fusion can provide dramatic pain relief, it's not a magic bullet. Patients should have realistic expectations about their recovery timeline and potential outcomes. Complete pain elimination is the goal, but significant pain reduction and improved function are more commonly achieved."
- Adherence to Post-operative Protocols: "Your commitment to post-operative instructions, including weight-bearing restrictions and physical therapy, is critical for successful fusion and long-term outcomes. This phase is as important as the surgery itself."
- Long-Term Follow-up is Essential: "Regular follow-up appointments are necessary to monitor your recovery, assess fusion progress, and address any concerns. We are partners in your journey to recovery."
6. Massive FAQ Section
Q1: What is the SI joint and why does it cause pain?
A1: The SI (Sacroiliac) joint is located at the base of your spine, connecting the sacrum (the triangular bone below your lumbar spine) to the ilium (the large bone of your pelvis). It's a strong, weight-bearing joint that allows for very little movement but is crucial for shock absorption and transferring forces between your upper body and legs. Pain occurs when this joint becomes dysfunctional—either too stiff (hypomobility) or too loose (hypermobility), leading to inflammation and irritation of the surrounding nerves and ligaments. This pain often radiates to the lower back, buttocks, groin, or even down the leg.
Q2: Who is a candidate for SI joint fixation screws?
A2: Candidates are typically individuals suffering from chronic, severe SI joint pain (lasting over 6 months) that has not responded to extensive non-surgical treatments like physical therapy, medications, and injections. A thorough diagnostic process, including a positive diagnostic SI joint injection, is crucial to confirm the SI joint as the primary pain source. Conditions like degenerative sacroiliitis, post-traumatic instability, or certain inflammatory conditions can also make one a candidate.
Q3: Is SI joint fixation a major surgery?
A3: Most SI joint fixation procedures today are performed using minimally invasive techniques (MIS). While it is still surgery and requires anesthesia, MIS approaches involve smaller incisions (typically 2-3 cm), less muscle dissection, and generally result in less blood loss, a shorter hospital stay (often one night), and a faster initial recovery compared to traditional open surgeries. It is considered a significant orthopedic procedure, but less invasive than many spinal fusions.
Q4: How long does the SI joint fixation surgery take?
A4: The actual surgical time for minimally invasive SI joint fixation typically ranges from 1 to 2 hours, depending on the complexity of the case, the number of screws placed, and the surgeon's technique. This does not include preparation and recovery time in the operating room suite.
Q5: What is the recovery like after SI joint screw placement?
A5: Recovery varies among individuals. Most patients spend one night in the hospital. You will likely experience some pain and discomfort in the surgical area, managed with medication. Initial weight-bearing restrictions (using crutches or a walker) are common for a few weeks, gradually progressing to full weight-bearing. A structured physical therapy program is essential for restoring strength and mobility, typically starting a few weeks post-op and continuing for several months. Full fusion can take 6-12 months.
Q6: Will I need to remove the screws later?
A6: In most cases, SI joint fixation screws are intended to be permanent implants and are not removed. They remain in place to maintain stability and support the fusion process. However, in rare instances, if the screws cause irritation (hardware prominence) or if there's an infection, removal may be considered after the fusion is complete and stable.
Q7: How effective are SI joint fixation screws for pain relief?
A7: Studies show that SI joint fixation using screws can be highly effective in reducing chronic SI joint pain, with many patients reporting significant improvement in pain levels and functional ability. Success rates for pain relief and improved quality of life are generally high, especially when patients are carefully selected and adhere to post-operative guidelines.
Q8: What are the alternatives to SI joint fixation surgery?
A8: Alternatives to surgery include a range of conservative treatments:
* Physical Therapy: Strengthening exercises, stretching, manual therapy.
* Medications: NSAIDs, muscle relaxants, neuropathic pain medications.
* Injections: Corticosteroid injections, prolotherapy, platelet-rich plasma (PRP), or stem cell injections.
* Radiofrequency Ablation (RFA): A procedure that uses heat to temporarily disrupt nerve signals from the SI joint.
* Bracing: Use of a specialized SI belt for support.
These are typically exhausted before considering surgery.
Q9: Can I have an MRI with SI joint fixation screws?
A9: Yes, most SI joint fixation screws are made from titanium alloys, which are generally considered MRI-safe. Titanium is non-magnetic, so it does not pose a hazard in an MRI machine. However, the presence of metal implants can create some artifact (distortion) in the MRI images, particularly close to the screws themselves. Always inform your healthcare provider and MRI technologist about your implants before undergoing an MRI.
Q10: What is the difference between SI joint fusion and SI joint stabilization?
A10: SI joint stabilization refers to the immediate effect of the screws in reducing abnormal movement and providing mechanical support to the joint. SI joint fusion (arthrodesis) is the long-term biological process where the bones of the sacrum and ilium grow together and permanently unite across the joint space. The screws facilitate stabilization, which in turn promotes and supports the eventual fusion. Fusion is the ultimate goal, providing lasting stability and pain relief.
Q11: How long does it take for the joint to fuse after SI joint fixation?
A11: The process of bone fusion is gradual. While immediate stability is achieved with the screws, complete biological fusion typically takes 6 to 12 months. Factors like individual healing capacity, bone quality, adherence to post-operative restrictions, and smoking status can influence this timeline. Your surgeon will monitor fusion progress with follow-up X-rays or CT scans.
Q12: What should I expect in terms of long-term outcomes?
A12: Long-term outcomes for appropriately selected patients are generally positive, with significant and sustained pain reduction, improved functional mobility, and enhanced quality of life. Many patients are able to return to activities they previously enjoyed. While the screws are designed to be permanent, regular follow-up with your surgeon is important to ensure continued well-being and to address any rare long-term issues.
Disclaimer: This information is intended for educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition.