Understanding the Radial Head Resection Arthroplasty Spacer: A Comprehensive Guide
1. Comprehensive Introduction & Overview
The human elbow is a complex hinge joint, crucial for a vast range of arm movements, from delicate tasks to heavy lifting. It comprises three bones: the humerus (upper arm bone), ulna, and radius (forearm bones). The radial head, located at the top of the radius, plays a vital role in both elbow flexion/extension and forearm rotation (pronation and supination). It articulates with the capitellum of the humerus and the radial notch of the ulna, contributing significantly to elbow stability and mechanics.
However, the radial head is susceptible to various injuries and degenerative conditions, most commonly severe fractures that are too comminuted to repair, or chronic conditions like arthritis. When the radial head is extensively damaged, it can lead to pain, instability, and restricted movement. In such cases, surgical intervention is often necessary.
Radial head resection arthroplasty involves the surgical removal of the damaged radial head. While this procedure can alleviate pain, simply removing the radial head can sometimes lead to long-term complications, such as proximal migration of the radius (the radius moving upwards towards the humerus), chronic wrist pain due to altered load distribution (Essex-Lopresti injury pattern), and elbow instability. To mitigate these risks and restore optimal elbow function, a "Radial Head Resection Arthroplasty Spacer" is often employed.
This specialized orthopedic implant is designed to replace the removed portion of the radial head. Its primary purpose is to maintain the correct anatomical relationship between the radius, ulna, and humerus, providing stability to the elbow and forearm while preserving the crucial rotational movements. The use of a spacer aims to reduce pain, improve joint mechanics, and facilitate a quicker, more effective return to function for patients. This guide will delve into the intricate details of these critical devices, from their sophisticated design to their profound impact on patient outcomes.
2. Deep-dive into Technical Specifications / Mechanisms
The efficacy of a radial head spacer lies in its meticulous design, choice of materials, and how it integrates with the complex biomechanics of the elbow.
Design and Material Innovations
Radial head spacers are engineered to mimic the natural articulation of the radial head, offering various designs to suit different patient anatomies and surgical needs.
- Design Variations:
- Anatomic vs. Spherical: Some spacers are designed to closely replicate the natural contour of the radial head (anatomic), while others utilize a more generalized spherical or hemispherical design. Anatomic designs aim for a more precise fit and articulation.
- Stemmed vs. Un-stemmed: Stemmed implants feature a shaft that extends into the medullary canal of the radius, providing enhanced fixation and stability. Un-stemmed implants rely on a press-fit or soft tissue encapsulation, often used in less demanding situations or as temporary solutions.
- Modular Systems: Many modern spacers are modular, allowing surgeons to select different head sizes and stem lengths independently. This versatility enables a highly customized fit for each patient, optimizing stability and range of motion.
- Material Science: The choice of material is paramount, influencing biocompatibility, durability, wear characteristics, and long-term outcomes.
- Silicone: Historically one of the first materials used. Silicone spacers are flexible and can provide good cushioning. However, they are prone to wear, fragmentation, and can induce a foreign body reaction known as "silicone synovitis," limiting their long-term use. They are generally considered for temporary use or in low-demand patients.
- Pyrolytic Carbon: This advanced material offers excellent biocompatibility, high strength-to-weight ratio, and a low coefficient of friction, mimicking articular cartilage properties. Pyrolytic carbon spacers are durable and have shown good long-term results with minimal wear on opposing cartilage.
- Metals (Cobalt-Chromium, Titanium Alloys): These materials are robust, highly durable, and commonly used in orthopedic implants. Cobalt-Chromium (CoCr) alloys offer excellent wear resistance, while Titanium (Ti) alloys provide good biocompatibility and osseointegration potential for stemmed designs. Metal spacers are very strong and can withstand significant loads.
- Polyetheretherketone (PEEK): An increasingly popular high-performance polymer offering radiolucency (allowing better post-operative imaging), good mechanical properties, and biocompatibility.
Biomechanics and Mechanism of Action
The radial head spacer functions by restoring critical biomechanical parameters of the elbow and forearm:
- Restoration of Radial Head Height: By replacing the resected radial head, the spacer maintains the physiological length of the radius. This is crucial for preventing proximal migration of the radius, which can lead to impingement, pain, and instability at the distal radioulnar joint (DRUJ) and wrist.
- Maintenance of Radiocapitellar Articulation: The spacer provides a smooth articulating surface against the capitellum of the humerus, allowing for pain-free flexion, extension, and, critically, forearm rotation (pronation and supination).
- Longitudinal Forearm Stability: The radial head, along with the interosseous membrane and DRUJ, forms a complex stabilizing unit for the forearm. A spacer helps restore this longitudinal stability, preventing the "Essex-Lopresti injury" cascade where radial head fracture leads to interosseous membrane disruption and DRUJ instability.
- Load Distribution: The spacer helps to distribute axial loads across the elbow joint, preventing excessive stress on other structures and potentially delaying degenerative changes.
3. Extensive Clinical Indications & Usage
The decision to use a radial head resection arthroplasty spacer is made after careful consideration of the patient's specific injury, overall health, and functional demands.
Key Clinical Indications
- Comminuted Radial Head Fractures: Fractures where the radial head is shattered into multiple pieces, making internal fixation (screws/plates) impossible or unlikely to succeed.
- Essex-Lopresti Injury: A severe injury involving a comminuted radial head fracture, disruption of the interosseous membrane of the forearm, and dislocation of the distal radioulnar joint (DRUJ). Spacers are crucial here to restore longitudinal stability and prevent chronic wrist pain and instability.
- Chronic Pain and Instability after Radial Head Excision: In cases where the radial head was previously removed without replacement, leading to persistent symptoms.
- Post-traumatic Arthritis of the Radiocapitellar Joint: When arthritis develops in the joint between the radius and humerus due to prior trauma, and conservative treatments fail.
- Failed Radial Head Fixation: If previous attempts to fix a radial head fracture have failed, leading to non-union, malunion, or persistent symptoms.
- Rheumatoid Arthritis: In specific cases where the radial head is severely damaged by inflammatory arthritis and causes significant pain and dysfunction.
Detailed Surgical Applications and Fitting/Usage Instructions
The surgical procedure for implanting a radial head spacer requires precision and adherence to strict protocols.
-
Pre-operative Planning:
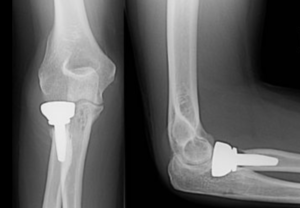
- Imaging: X-rays, CT scans, and sometimes MRI are essential to fully assess the extent of the injury, bone quality, and surrounding soft tissues.
- Templating: Surgeons use templates (physical or digital) of various implant sizes to estimate the appropriate dimensions for the spacer, ensuring optimal fit and restoration of radial length.
- Patient Education: Comprehensive discussion with the patient about the procedure, expected outcomes, and potential risks.
-
Surgical Approach:
- The most common approaches include the Kocher approach (posterior-lateral) or the Kaplan approach (anterior-lateral), chosen based on the specific injury and surgeon's preference. These approaches allow access to the radial head while protecting important nerves and blood vessels.
-
Radial Head Resection:
- The damaged radial head is carefully exposed and resected (removed) using an oscillating saw or osteotome. The resection level is critical to ensure proper seating of the implant and to avoid over-resection or under-resection.
-
Spacer Insertion and Fitting:
- Trial Implants: A set of trial spacers (sizers) corresponding to the definitive implant system are used first. The surgeon selects the trial that best restores radial length, maintains stability, and allows for smooth articulation and full range of motion without overstuffing the joint. Overstuffing can lead to increased joint pressure, stiffness, and pain, while understuffing can result in instability and proximal migration.
- Definitive Implant Placement: Once the optimal trial size is determined, the definitive radial head spacer is carefully inserted.
- Fixation:
- Press-fit: Many stemmed implants are designed for a press-fit into the radial canal, relying on the tight fit and eventual bone ingrowth for stability.
- Bone Cement: In some cases, especially in osteoporotic bone or when immediate rigid fixation is desired, bone cement (polymethylmethacrylate - PMMA) may be used to secure the stem within the radial canal.
- Un-stemmed/Non-constrained: For designs without a stem, the implant rests on the resected radial neck, relying on surrounding soft tissue and joint capsule for stability.
- Intraoperative Assessment: After insertion, the surgeon meticulously assesses the elbow's stability through a full range of motion (flexion, extension, pronation, supination). The DRUJ is also checked for stability, particularly in Essex-Lopresti injuries.
4. Risks, Side Effects, or Contraindications
While radial head spacer arthroplasty offers significant benefits, like any surgical procedure, it carries potential risks and may not be suitable for all patients.
Potential Risks and Side Effects
- Infection: A risk with any surgery involving implants. Can range from superficial wound infection to deep periprosthetic infection, potentially requiring further surgery and implant removal.
- Nerve or Vascular Injury: Nerves (e.g., posterior interosseous nerve, radial nerve) and blood vessels around the elbow can be inadvertently damaged during surgery.
- Implant Loosening or Dislocation: The spacer may loosen from its fixation or dislocate from its position, often requiring revision surgery.
- Periprosthetic Fracture: A fracture occurring around the implant, either during insertion or as a complication later.
- Stiffness or Restricted Range of Motion: Despite the spacer, some patients may experience ongoing stiffness or a limited range of motion, necessitating intensive physical therapy or further intervention.
- Persistent Pain: While the goal is pain relief, some patients may continue to experience pain, potentially due to other underlying issues or implant-related problems.
- Heterotopic Ossification: Abnormal bone growth in the soft tissues around the elbow, which can restrict movement.
- Wear of Articular Cartilage (Capitellum): Over time, the spacer can cause wear to the natural cartilage surface of the capitellum, potentially leading to arthritis in that part of the joint. This is more common with certain materials or in cases of implant malposition.
- Silicone Synovitis: Specific to silicone implants, this is an inflammatory reaction to silicone particles released from implant wear.
- Hardware Failure: Breakage of the implant itself, though rare with modern materials.
Contraindications
- Active Infection: Any active infection in the elbow or elsewhere in the body must be treated and resolved before considering implant surgery.
- Severe Bone Loss: Insufficient bone stock in the proximal radius may prevent stable fixation of the implant.
- Unrealistic Patient Expectations: Patients must have a clear understanding of the procedure's goals and limitations.
- Compromised Soft Tissue Envelope: Poor skin or soft tissue quality around the elbow may increase the risk of wound complications and infection.
- Allergy to Implant Materials: Rare but possible, requiring careful pre-operative screening.
- Neuropathic Joint: Conditions like Charcot arthropathy can compromise joint integrity and implant success.
5. Expert Tips from Dr. Mohammed Hutaif
"As an orthopedic specialist, I've seen firsthand the transformative impact a well-placed radial head resection arthroplasty spacer can have on a patient's quality of life. However, success hinges on meticulous planning, execution, and post-operative care. Here are my key recommendations:
- Patient Selection is Paramount: Not every radial head injury warrants a spacer. Thoroughly assess the patient's age, activity level, bone quality, and specific injury pattern. For instance, in an Essex-Lopresti injury, a spacer is often critical to prevent chronic forearm instability, whereas a simple radial head excision might suffice for a low-demand elderly patient with an isolated comminuted fracture.
- Precision in Sizing and Placement: The most common pitfalls relate to incorrect implant sizing. Overstuffing the joint leads to increased pressure, stiffness, and accelerated capitellar wear. Understuffing results in instability and proximal radial migration. Utilize intraoperative fluoroscopy and trial implants meticulously to achieve the perfect balance of stability and motion. Pay close attention to restoring the radial length accurately.
- Material Matters: The choice of implant material should be individualized. While silicone has historical relevance, I generally favor pyrolytic carbon or metal implants for their superior durability and reduced wear characteristics, especially in younger, more active patients. Understand the biomechanical properties of each material and select accordingly.
- Rigorous Post-operative Rehabilitation: Surgery is only half the battle. A structured, progressive rehabilitation program is essential. Early, controlled range of motion exercises are crucial to prevent stiffness, but always balanced with protecting the healing tissues and implant stability. Close collaboration with physical therapists is non-negotiable.
- Manage Expectations: It's vital to have an honest discussion with patients about realistic outcomes. While significant pain relief and functional improvement are common, full, pre-injury function may not always be achievable. Educate them about potential long-term considerations, such as the possibility of future revision surgery.
- Address Concomitant Injuries: Always look beyond the radial head. The elbow is a complex joint, and radial head fractures often occur with collateral ligament injuries or interosseous membrane disruption. These must be identified and addressed simultaneously to ensure overall elbow stability and optimal results."
6. Massive FAQ Section
Q1: What is a Radial Head Resection Arthroplasty Spacer?
A: It's a specialized orthopedic implant designed to replace the top portion of the radius bone (radial head) after it has been surgically removed due to severe damage (e.g., from a comminuted fracture or arthritis). Its main purpose is to maintain proper elbow and forearm mechanics, provide stability, and allow for rotational movements like turning your palm up and down.
Q2: When is a radial head spacer typically used?
A: Spacers are primarily used when the radial head is severely fractured and cannot be repaired, or when previous treatments have failed. Key indications include highly comminuted radial head fractures, chronic pain/instability after radial head excision, post-traumatic arthritis, and especially in cases of Essex-Lopresti injuries where there's associated forearm and wrist instability.
Q3: What materials are these spacers made from?
A: Common materials include:
* Silicone: Flexible, but prone to wear and can cause inflammatory reactions.
* Pyrolytic Carbon: Strong, durable, biocompatible, and has a low friction surface, mimicking natural cartilage.
* Metals (Cobalt-Chromium, Titanium): Very strong and durable, offering excellent stability.
* PEEK (Polyetheretherketone): A high-performance polymer offering good mechanical properties and allowing better post-operative imaging. The choice depends on the patient's needs and the surgeon's preference.
Q4: How long does the surgery to implant a radial head spacer take?
A: The duration of the surgery can vary depending on the complexity of the injury, the specific surgical approach, and whether other associated injuries need to be addressed. Generally, the procedure itself can take anywhere from 1 to 2 hours.
Q5: What is the typical recovery process like after radial head spacer surgery?
A: Recovery typically involves a period of immobilization (often in a sling) followed by a structured physical therapy program.
* Early Phase (0-2 weeks): Pain management, wound care, and gentle, controlled range of motion exercises, often passive.
* Intermediate Phase (2-6 weeks): Gradual increase in active range of motion, light strengthening, and continued swelling management.
* Late Phase (6+ weeks): Progressive strengthening, return to functional activities, and sport-specific training as appropriate.
Full recovery can take several months, with continuous improvement over a year.
Q6: Will I regain full elbow movement after this surgery?
A: The goal of the surgery is to restore significant pain-free range of motion, including flexion, extension, pronation, and supination. While many patients achieve excellent functional outcomes, regaining pre-injury full movement isn't always guaranteed, especially in cases of severe initial trauma or significant joint stiffness. Consistent engagement in physical therapy is crucial for maximizing motion.
Q7: Are there alternatives to a radial head spacer?
A: Yes, alternatives exist depending on the specific injury and patient factors:
* Radial Head Excision (without replacement): May be considered for low-demand patients or less severe fractures, but carries risks of long-term instability and pain.
* Open Reduction and Internal Fixation (ORIF): If the fracture is amenable to repair, plates and screws can be used to fix the radial head.
* Total Elbow Arthroplasty: In very severe cases of elbow arthritis or complex trauma involving multiple joint components, a total elbow replacement may be indicated, but this is a much larger procedure.
Q8: How long does a radial head spacer typically last?
A: The longevity of a radial head spacer varies greatly depending on the material, patient activity level, surgical technique, and presence of complications. While some can last for many years or even decades, they are not always considered lifetime implants. Pyrolytic carbon and metal implants generally offer better long-term durability compared to silicone. Regular follow-up with your surgeon is important to monitor the implant.
Q9: Can the radial head spacer be removed if there are problems?
A: Yes, in cases of complications such as infection, persistent pain, loosening, or wear, the radial head spacer can be surgically removed. This may sometimes be followed by the implantation of a different type of spacer, or in some scenarios, the elbow may be managed without a spacer, depending on the specific issue and patient condition.
Q10: What is the difference between a radial head spacer and a total elbow replacement?
A:
* Radial Head Spacer: Replaces only the radial head, a component of the elbow joint. It's a partial replacement aimed at restoring stability and movement of the forearm and elbow.
* Total Elbow Replacement (TEA): Replaces the entire elbow joint, including the ends of the humerus and ulna, and sometimes the radial head as well. It's a much more extensive procedure typically reserved for severe arthritis, instability, or complex fractures involving the entire joint.
Q11: How do I prepare for radial head spacer surgery?
A: Preparation typically involves:
* Medical Evaluation: A thorough check-up to ensure you are fit for surgery.
* Medication Review: Discuss all current medications with your surgeon, as some may need to be stopped before surgery (e.g., blood thinners).
* Smoking Cessation: If you smoke, you will be advised to stop, as smoking can impair healing.
* Home Preparation: Arrange for assistance at home during your initial recovery, as your arm will be restricted.
* Pre-operative Instructions: Follow all specific instructions provided by your surgical team regarding fasting, hygiene, and arrival times.
Q12: What improvements in patient outcomes can be expected with a radial head spacer?
A: Patients can typically expect:
* Significant Pain Reduction: Relief from the chronic pain caused by the damaged radial head.
* Improved Elbow Stability: Restoration of the structural integrity of the elbow and forearm.
* Enhanced Range of Motion: Better ability to bend, straighten, and rotate the forearm.
* Prevention of Long-term Complications: Particularly preventing proximal radial migration and chronic wrist pain associated with Essex-Lopresti injuries.
* Return to Daily Activities: Improved ability to perform everyday tasks and, for many, return to light recreational activities.
* Better Quality of Life: Overall enhancement in well-being due to reduced pain and improved function.
Maintenance and Sterilization Protocols (For Medical Professionals)
While patients do not directly maintain or sterilize their implants, it is crucial for them to understand that stringent protocols are in place to ensure their safety and the longevity of the device.
Manufacturer and Clinical Facility Responsibilities:
- Manufacturing Quality Control: Radial head spacers are manufactured under strict quality control standards, often in ISO-certified facilities, to ensure material purity, precise dimensions, and structural integrity.
- Packaging and Sterilization: Implants are typically supplied in sterile packaging by the manufacturer. Common sterilization methods include gamma irradiation or ethylene oxide (EtO) gas, ensuring the implant is free of microorganisms before use. Each package carries clear labeling with lot numbers, expiration dates, and sterilization indicators.
- Storage: Implants must be stored in a clean, dry environment, protected from extreme temperatures and physical damage, and within their specified shelf life.
- Intraoperative Handling: During surgery, strict aseptic techniques are paramount. The implant should only be handled with sterile instruments, and direct contact with non-sterile surfaces or personnel must be avoided. Any breach of sterility requires the implant to be discarded.
- Traceability: Each implant has a unique identifier (lot number, serial number) that is meticulously recorded in the patient's medical file. This ensures traceability in case of a product recall or adverse event reporting.
- Instrument Sterilization: All surgical instruments used in conjunction with the implant (e.g., reamers, sizers, inserters) undergo rigorous cleaning, disinfection, and sterilization processes (typically steam sterilization/autoclaving) according to hospital protocols and manufacturer guidelines.
- Post-operative Monitoring: While not "maintenance" in the traditional sense, regular post-operative follow-up appointments with imaging (X-rays) are essential to monitor the implant's position, stability, and detect any signs of loosening, wear, or other complications.
These comprehensive protocols ensure that the radial head resection arthroplasty spacer is delivered and used in the safest possible manner, contributing to successful patient outcomes.