


The Monoaxial Pedicle Screw: A Comprehensive Guide to Spinal Stabilization
Introduction & Overview
The human spine is a marvel of engineering, providing both flexibility and robust support for the entire body. However, various conditions—from degenerative diseases and trauma to deformities—can compromise its integrity, leading to pain, instability, and neurological deficits. In such cases, orthopedic surgeons often turn to advanced spinal instrumentation to restore stability and facilitate healing. Among the most critical components in spinal fusion surgery is the pedicle screw. This guide will focus specifically on the monoaxial pedicle screw, an essential tool in spinal stabilization, offering a deep dive into its design, applications, biomechanics, and the significant role it plays in improving patient outcomes.
A monoaxial pedicle screw is a specialized implant used in spinal surgery to provide rigid fixation to the vertebral column. Unlike its polyaxial counterpart, which features a screw head that can swivel or angulate relative to its shaft, the head of a monoaxial pedicle screw is fixed, allowing no angulation. This design choice imparts a direct, unyielding connection between the screw and the connecting rod, creating an exceptionally stiff and stable construct. Its primary purpose is to anchor spinal rods, facilitating spinal fusion—a process where two or more vertebrae are permanently joined to eliminate motion and alleviate pain. Understanding the nuances of this instrument is crucial for patients considering spinal surgery, as it directly impacts the stability and long-term success of the procedure.
Deep-Dive into Technical Specifications & Mechanisms
Design and Materials
The monoaxial pedicle screw is engineered for maximum strength and biocompatibility, crucial for long-term implantation within the human body.
Key Design Features:
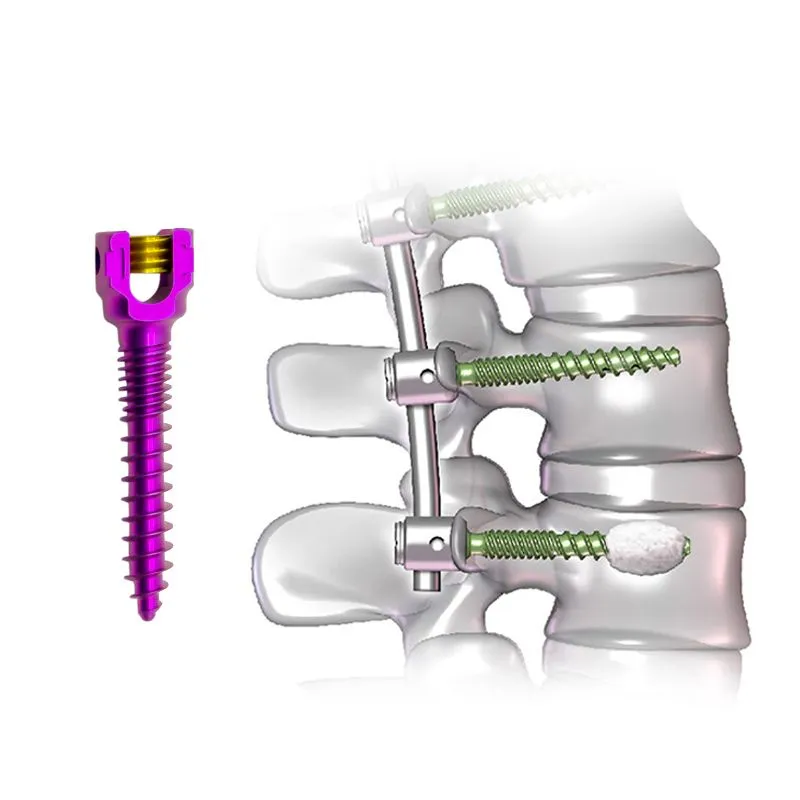
- Fixed Head: The defining characteristic. The screw head is rigidly connected to the threaded shaft, preventing any angular movement. This fixed interface ensures a direct and strong connection to the spinal rod.
- Threaded Shaft: Designed for optimal purchase within the vertebral pedicle. The threads typically feature a specific pitch and depth to maximize pullout strength and resist loosening in cancellous bone. Various diameters and lengths are available to match diverse patient anatomies and vertebral levels.
- Rod-Receiving Mechanism: The screw head is designed with a U-shaped or similar channel to securely cradle a spinal rod. A locking cap or set screw then tightens down onto the rod, firmly securing it within the screw head.
- Low Profile: Modern designs often aim for a low profile to minimize soft tissue irritation post-implantation.
Materials:
The choice of material is critical for implant longevity, strength, and patient safety.
* Titanium Alloys (e.g., Ti-6Al-4V): The predominant material due to an unparalleled combination of properties:
* Biocompatibility: Titanium is highly inert and well-tolerated by the human body, minimizing adverse reactions.
* High Strength-to-Weight Ratio: Provides excellent mechanical strength while being relatively lightweight.
* Corrosion Resistance: Highly resistant to degradation in the physiological environment.
* MRI Compatibility: Generally safe for MRI scans, allowing for post-operative imaging without significant artifact distortion.
* Stainless Steel (e.g., 316L): Less common now for primary pedicle screws but historically used. It offers good strength but is less biocompatible and creates more MRI artifact than titanium.
* Surface Treatments: Some screws may feature specialized surface treatments (e.g., plasma spray, hydroxyapatite coating, porous structures) to promote osteointegration—the direct structural and functional connection between living bone and the surface of a load-bearing implant. This can enhance long-term stability and fusion rates.
Mechanism of Action and Biomechanics
The monoaxial pedicle screw functions by creating a rigid anchor point within the vertebral pedicle, a strong bony bridge connecting the front and back parts of a vertebra.
How it Works:
- Anchoring: The threaded shaft is carefully inserted into the pedicle, extending into the vertebral body. This provides a robust purchase in both cortical and cancellous bone.
- Rod Connection: Once multiple monoaxial screws are placed at desired vertebral levels, a contoured spinal rod is laid into the fixed heads of the screws.
- Rigid Fixation: Locking caps are then tightened, securely clamping the rod within each screw head. Because the screw head is fixed, this creates an extremely stiff and unyielding connection between the screw, rod, and ultimately, the vertebrae.
Biomechanical Advantages:
- High Stiffness and Rigidity: The fixed head design provides a direct, unarticulated interface with the rod, resulting in a construct with superior stiffness. This is particularly advantageous in situations requiring maximal immediate stability.
- Enhanced Load Sharing: By rigidly connecting the vertebrae, the monoaxial system effectively transfers load across the fusion segment, reducing stress on the bone graft and promoting successful fusion.
- Resistance to Motion: This rigidity offers excellent resistance to all planes of motion—flexion, extension, lateral bending, and axial rotation—which is crucial for stabilizing unstable segments and allowing the fusion process to occur unimpeded.
- Specific Applications in Deformity Correction: In certain complex spinal deformities like severe scoliosis or kyphosis, the unyielding nature of monoaxial screws allows surgeons to apply powerful corrective forces directly to the spine, leveraging the rod's contour to achieve the desired alignment. While less forgiving for rod placement than polyaxial screws, their fixed nature can be an asset when precise, direct force application is needed.
Extensive Clinical Indications & Usage
The monoaxial pedicle screw is a versatile tool, indicated for a wide range of spinal pathologies requiring stabilization and fusion.
Primary Clinical Indications:
- Degenerative Spinal Conditions:
- Degenerative Disc Disease (DDD): When disc degeneration leads to chronic pain and instability, fusion can alleviate symptoms.
- Spondylolisthesis: Forward slippage of one vertebra over another, causing instability and nerve compression. Monoaxial screws provide robust fixation to prevent further slippage.
- Spinal Stenosis: Narrowing of the spinal canal or neural foramina, often accompanied by instability requiring decompression and fusion.
- Spinal Trauma:
- Vertebral Fractures: Unstable fractures that compromise spinal integrity often require surgical stabilization with pedicle screws to prevent neurological damage and promote healing.
- Spinal Deformities:
- Scoliosis: Lateral curvature of the spine. Monoaxial screws can be used, often in conjunction with polyaxial screws, to provide powerful correctional forces and maintain alignment.
- Kyphosis: Excessive forward curvature of the spine.
- Spinal Tumors: Resection of spinal tumors often leaves significant bone defects and instability, necessitating reconstruction and stabilization.
- Spinal Infections: In cases of severe spinal infection (e.g., osteomyelitis, discitis) requiring debridement, fusion with pedicle screws can stabilize the affected segment.
- Pseudarthrosis: Non-union after a previous spinal fusion. Revision surgery often involves re-instrumentation with robust fixation like monoaxial screws.
Detailed Surgical Application & Usage:
The implantation of monoaxial pedicle screws is a meticulous procedure requiring advanced surgical skills and precise planning.
- Pre-operative Planning:
- Thorough imaging (X-rays, CT, MRI) is used to assess spinal anatomy, pathology, and bone quality.
- Screw trajectory, length, and diameter are carefully planned to ensure optimal placement and avoid neurovascular structures.
- Rod contouring is often planned in advance, especially for deformity correction, to match the fixed screw heads.
- Patient Positioning and Incision:
- The patient is carefully positioned, typically prone, to allow optimal surgical access.
- A surgical incision is made to expose the posterior elements of the vertebrae.
- Pedicle Preparation:
- Under fluoroscopic or navigation guidance, the surgeon identifies the entry point for each pedicle screw.
- An awl or bur is used to create a starting hole.
- A pedicle probe is then carefully advanced through the pedicle into the vertebral body, creating a pilot hole. The integrity of the pedicle walls is checked with a ball-tipped probe.
- The pilot hole may be tapped (threaded) to prepare for screw insertion, especially in dense bone.
- Screw Insertion:
- The monoaxial pedicle screw is carefully inserted into the prepared pilot hole using a specialized driver.
- The surgeon ensures proper seating and torque, confirming good bone purchase.
- Fluoroscopy or navigation systems provide real-time feedback on screw trajectory and depth.
- Rod Placement and Fixation:
- Once all screws are in place, a pre-contoured spinal rod is carefully positioned into the fixed heads of the screws.
- A reduction instrument may be used to gently bring the rod closer to the screw heads if there's a slight misalignment.
- Locking caps (set screws) are then applied and tightened to firmly secure the rod within each screw head, creating a rigid construct.
- Compression/Distraction/Derotation:
- Depending on the surgical goal (e.g., correcting deformity, achieving compression across a fusion site), specific forces may be applied to the rods and screws before final tightening.
- Bone Grafting:
- Autograft (patient's own bone) or allograft (donor bone) is packed around the fusion site to promote bony union.
- Closure:
- Muscle and fascial layers are closed, followed by skin closure.
Maintenance & Sterilization Protocols
While pedicle screws are single-use implants, the instruments used for their insertion and the surrounding surgical environment demand stringent sterilization protocols to prevent surgical site infections (SSIs) and ensure patient safety.
Implant Handling:
- Single-Use Only: Monoaxial pedicle screws are designed and packaged for single use. They should never be re-sterilized or reused.
- Aseptic Presentation: Implants are provided in sterile packaging and must be handled using strict aseptic techniques in the operating room.
- Expiration Dates: Always check the expiration date on the sterile packaging.
Instrument Sterilization (for reusable surgical tools):
- Decontamination: Immediately after surgery, instruments are thoroughly cleaned to remove blood and tissue. This often involves manual scrubbing and/or automated washer-disinfectors.
- Inspection: Instruments are inspected for damage, wear, and cleanliness.
- Packaging: Cleaned instruments are arranged in specialized trays and wrapped or placed in rigid containers designed for sterilization.
- Sterilization Methods:
- Steam Sterilization (Autoclaving): The most common and effective method for heat- and moisture-tolerant instruments. High-pressure saturated steam kills microorganisms.
- Ethylene Oxide (EtO): Used for heat- or moisture-sensitive instruments, though less common for standard metal spinal instruments.
- Hydrogen Peroxide Gas Plasma: Another low-temperature sterilization method for sensitive items.
- Storage: Sterilized instruments are stored in a sterile environment until needed for surgery.
- Traceability: Implants and instrument sets are meticulously tracked from manufacturing to patient use to ensure accountability and recall capability if necessary.
Risks, Side Effects, or Contraindications
While monoaxial pedicle screws significantly improve spinal stability, like any surgical procedure involving implants, there are potential risks and considerations.
General Surgical Risks:
- Anesthesia Risks: Reactions to anesthesia.
- Bleeding: Intraoperative or postoperative hemorrhage.
- Infection: Surgical site infection, which can be superficial or deep, potentially involving the implant.
- Blood Clots: Deep vein thrombosis (DVT) or pulmonary embolism (PE).
Specific Risks Related to Monoaxial Pedicle Screws & Spinal Fusion:
- Nerve Root or Spinal Cord Injury: The most serious risk, often due to screw malposition. Can lead to pain, weakness, numbness, or paralysis. Meticulous surgical technique and intraoperative imaging/neuromonitoring minimize this risk.
- Dural Tear: Puncturing the dura mater (the membrane surrounding the spinal cord), leading to cerebrospinal fluid (CSF) leakage, which may require repair.
- Screw Loosening or Pullout: The screw may become loose or dislodge from the bone, especially in patients with poor bone quality (osteoporosis) or if fusion fails.
- Screw Breakage: Though rare with modern titanium implants, excessive stress or non-union can lead to screw fracture.
- Non-Union (Pseudarthrosis): Failure of the vertebrae to fuse, which can lead to continued pain, instability, and potentially hardware failure.
- Adjacent Segment Disease (ASD): Increased stress on the spinal segments immediately above or below the fused segment, potentially leading to accelerated degeneration and the need for further surgery.
- Hardware Prominence/Pain: The implant may be palpable or cause local irritation, sometimes requiring removal.
- Allergic Reaction: Extremely rare, but some individuals may have sensitivities to titanium or other implant materials.
Contraindications:
- Active Systemic Infection: Untreated infection elsewhere in the body increases the risk of implant infection.
- Active Local Infection: Infection at the surgical site or within the spine.
- Severe Osteoporosis: Extremely poor bone quality may prevent adequate screw purchase, leading to high risk of loosening or pullout (though augmentation techniques exist).
- Patients Unfit for Surgery: Those with severe comorbidities that make them high-risk for any major surgery.
- Lack of Clear Indication: Surgery should only be performed when conservative treatments have failed and a clear pathological indication for fusion exists.
Expert Tips from Dr. Mohammed Hutaif
"As an orthopedic specialist, I've seen firsthand the transformative impact that well-executed spinal fusion with pedicle screws can have on a patient's life. The monoaxial pedicle screw, with its inherent rigidity, is a cornerstone in achieving robust spinal stability, particularly in complex cases requiring precise biomechanical control.
My primary advice revolves around several critical pillars:
- Meticulous Pre-operative Planning: Every spine is unique. Advanced imaging and detailed surgical planning are non-negotiable. Understanding the patient's specific anatomy, bone quality, and the exact nature of their pathology allows us to select the optimal screw size, trajectory, and overall construct design. This precision is especially vital with monoaxial screws, as they offer less intraoperative flexibility in rod placement.
- Precision in Surgical Technique: The placement of pedicle screws demands exceptional anatomical knowledge and surgical skill. We utilize intraoperative fluoroscopy, navigation systems, and neuromonitoring to ensure screws are placed accurately and safely, minimizing risks to neural structures. The fixed nature of monoaxial screws means rod contouring must be exact to ensure a stress-free fit.
- Patient Selection and Education: Not every patient is a candidate for spinal fusion, and not every fusion requires monoaxial screws. A thorough evaluation, including a detailed discussion of risks, benefits, and alternatives, empowers patients to make informed decisions. We emphasize the importance of lifestyle modifications and adherence to post-operative rehabilitation protocols.
- Emphasis on Fusion Biology: While instrumentation provides stability, the ultimate goal is bony fusion. We optimize conditions for fusion by using appropriate bone graft materials and ensuring a pristine biological environment. Patients play a crucial role by avoiding smoking and strictly following post-operative activity restrictions.
- Understanding Biomechanics: The monoaxial screw provides unparalleled rigidity. I often choose it when maximum stiffness is desired, for instance, in certain deformity corrections where powerful, direct forces are needed to achieve and maintain alignment, or in revision surgeries where a very stable construct is paramount. Recognizing when this rigidity is an advantage, and when the flexibility of a polyaxial screw might be more appropriate, is key to successful outcomes."
Patient Outcome Improvements
The successful application of monoaxial pedicle screws in spinal fusion surgery leads to significant improvements in patient outcomes, restoring function and enhancing quality of life.
- Pain Reduction: By stabilizing unstable segments and decompressing neural structures, patients typically experience a substantial reduction in chronic back or leg pain.
- Improved Functional Mobility: With a stable spine, patients regain the ability to perform daily activities, walk further, and engage in light physical activity without debilitating pain.
- Spinal Stability: The primary goal of pedicle screw fixation is to provide immediate and long-term stability to the affected spinal segment, preventing further neurological compromise and allowing the fusion to heal.
- Correction of Deformity: In cases of scoliosis or kyphosis, monoaxial screws, often as part of a hybrid construct, enable powerful correction of spinal curvature, restoring a more balanced posture.
- Enhanced Quality of Life: The cumulative effect of pain relief, improved mobility, and stability is a significantly enhanced quality of life, allowing patients to return to work, hobbies, and social activities.
- High Fusion Rates: When combined with appropriate bone grafting and proper surgical technique, pedicle screw instrumentation contributes to high rates of successful bony fusion, which is the ultimate measure of long-term success.
Massive FAQ Section
1. What is a monoaxial pedicle screw?
A monoaxial pedicle screw is a specialized implant used in spinal fusion surgery. It features a fixed head that does not swivel or angulate relative to its threaded shaft. This design creates a very rigid and direct connection between the screw and the spinal rod, providing maximum stability to the vertebral column.
2. How does it differ from a polyaxial pedicle screw?
The main difference lies in the screw head. A monoaxial screw has a fixed head, meaning it cannot move or angulate. A polyaxial screw, however, has a "multi-axial" or "top-loading" head that can swivel in multiple directions, offering greater flexibility during rod placement. Monoaxial screws provide more rigidity, while polyaxial screws offer more surgical ease for rod connection.
3. Why would my surgeon choose a monoaxial screw for me?
Your surgeon might choose monoaxial screws when maximum rigidity and direct force transmission are desired. This can be beneficial in certain complex deformity corrections (like severe scoliosis), cases requiring very robust primary fixation, or revision surgeries where a super-stable construct is paramount. The choice depends on your specific spinal condition, anatomy, and the surgeon's biomechanical goals.
4. What materials are these screws made of?
Monoaxial pedicle screws are predominantly made from high-grade titanium alloys (e.g., Ti-6Al-4V). Titanium is chosen for its excellent biocompatibility (meaning it's well-tolerated by the body), high strength, corrosion resistance, and compatibility with MRI scans.
5. Is spinal fusion with pedicle screws a major surgery?
Yes, spinal fusion surgery involving pedicle screws is considered a major surgical procedure. It requires general anesthesia, an incision, and careful manipulation of spinal structures. Recovery involves a significant period of healing and rehabilitation.
6. What are the potential risks of having monoaxial pedicle screws implanted?
Risks include general surgical risks like bleeding, infection, and anesthesia complications. Specific risks related to the screws and spinal fusion include nerve damage (leading to pain, numbness, weakness, or paralysis), dural tear, screw loosening or breakage, failure of the bone to fuse (non-union), and adjacent segment disease. Your surgeon will discuss these thoroughly.
7. How long does it take to recover from spinal fusion with pedicle screws?
Recovery time varies greatly among individuals, but generally, initial recovery takes several weeks to a few months. Full bony fusion can take 6 to 12 months or even longer. You'll typically have restrictions on lifting, bending, and twisting for several months, followed by a guided physical therapy program.
8. Will the screws stay in my body forever?
In most cases, yes. The monoaxial pedicle screws and rods are designed to be permanent implants, providing long-term stability and support after successful fusion. They are typically not removed unless they cause complications like pain, infection, or hardware failure.
9. Can I have an MRI scan with titanium pedicle screws?
Yes, titanium pedicle screws are generally considered safe for MRI (Magnetic Resonance Imaging) scans. Titanium is a non-ferromagnetic material, meaning it is not attracted to the strong magnetic fields of an MRI. You should always inform your imaging technician and doctor about your implants before any MRI.
10. What are the long-term outcomes after spinal fusion with monoaxial pedicle screws?
Long-term outcomes are generally positive for appropriately selected patients. Many experience significant pain relief, improved spinal stability, and enhanced functional mobility. The goal is a successful bony fusion, which provides lasting stability and improved quality of life. Regular follow-ups with your surgeon are important.
11. How do these screws help correct spinal deformities?
Monoaxial screws, due to their fixed and rigid connection to the spinal rod, allow surgeons to apply powerful and precise corrective forces. The surgeon contours the rod to the desired spinal alignment, and then by securing the rod tightly into the fixed screw heads, the spine is effectively "derotated" or "straightened" into the new position, which is then maintained by the rigid construct.
12. What post-operative care is required after receiving these implants?
Post-operative care is crucial for successful recovery and fusion. It typically includes pain management, wound care, early mobilization (walking), physical therapy to strengthen core muscles and improve flexibility (once cleared by the surgeon), and strict adherence to activity restrictions (avoiding lifting, bending, twisting). Regular follow-up appointments and imaging studies will monitor your progress.
Disclaimer: This information is for educational purposes only and is not medical advice. Always consult with a qualified healthcare professional for diagnosis and treatment of any medical condition.