

The Lisfranc Midfoot Plating System: A Comprehensive Orthopedic Guide
Comprehensive Introduction & Overview
The Lisfranc joint complex, a critical anatomical structure in the midfoot, plays a pivotal role in maintaining the arch and transferring forces during gait. Injuries to this complex, often referred to as Lisfranc injuries, range from subtle sprains to severe fracture-dislocations of the tarsometatarsal (TMT) joints. These injuries are frequently misdiagnosed, leading to chronic pain, midfoot instability, and debilitating post-traumatic arthritis if not managed appropriately.
Surgical intervention is often the gold standard for unstable Lisfranc injuries, aiming to restore anatomical alignment and stability. Historically, K-wires and isolated screw fixation were common. However, advancements in orthopedic technology have led to the development of sophisticated Lisfranc Midfoot Plating Systems. These systems offer superior biomechanical stability, robust fixation, and improved patient outcomes by providing anatomical contouring and enhanced load-sharing capabilities, crucial for the complex mechanics of the midfoot. This guide will delve into the intricacies of these advanced plating systems, covering their design, application, maintenance, biomechanics, and impact on patient recovery.
Deep-Dive into Technical Specifications & Mechanisms
The effectiveness of a Lisfranc Midfoot Plating System lies in its meticulous design and material selection, engineered to address the complex anatomy and biomechanics of the midfoot.
Design Principles
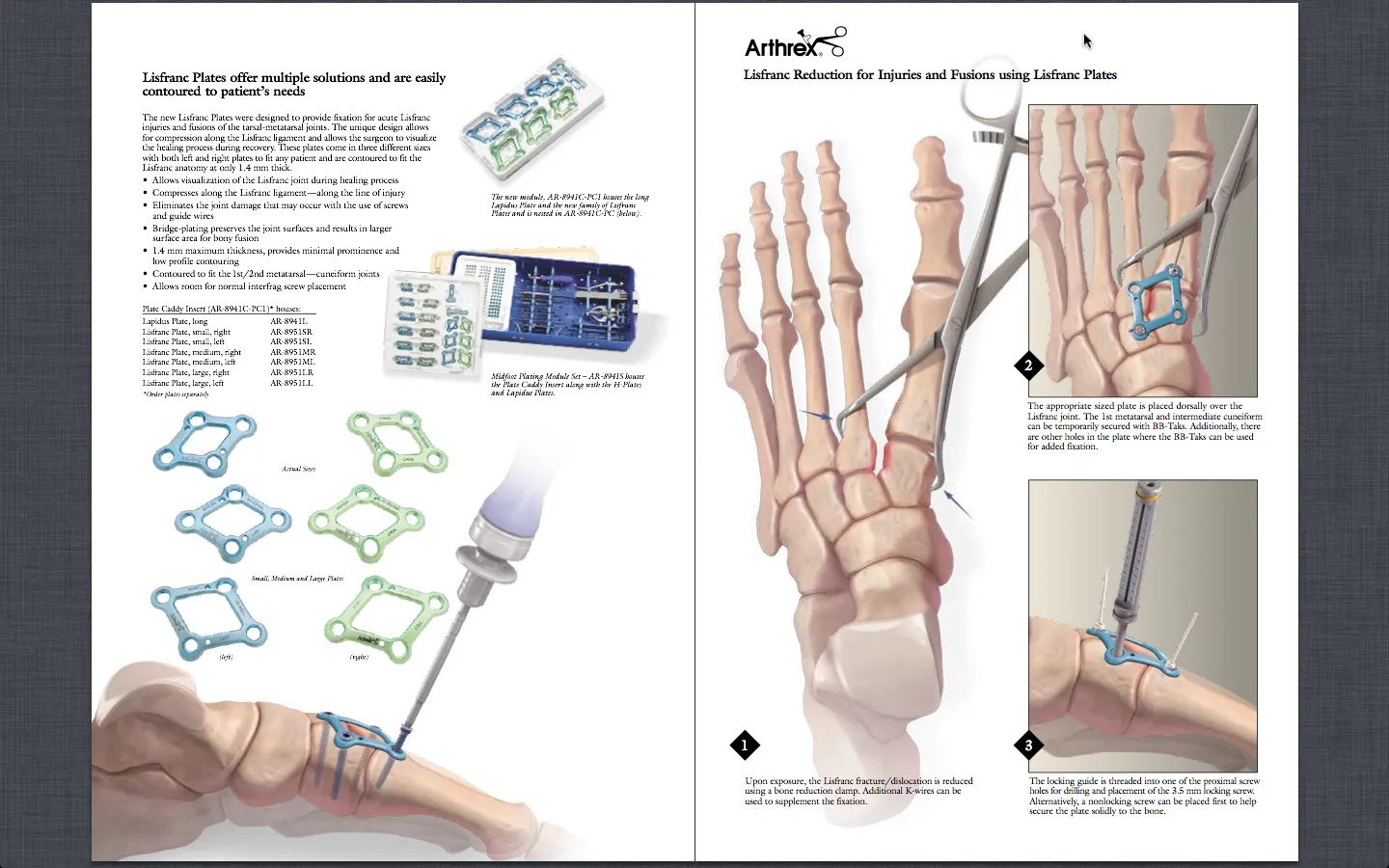
- Anatomical Contouring: Plates are pre-contoured to match the intricate dorsal anatomy of the midfoot, specifically designed for the medial, intermediate, and lateral cuneiforms, the cuboid, and the bases of the metatarsals. This minimizes the need for intraoperative bending, reduces soft tissue irritation, and ensures optimal fit.
- Low-Profile Design: Modern plates feature a low-profile construction to reduce palpability and irritation of the overlying soft tissues, including tendons and nerves, which is a common concern in the dorsum of the foot.
- Variable Angle Locking (VAL) and Fixed Angle Locking (FAL) Options:
- VAL Systems: Allow screws to be angled within a specific cone (typically ±15-30 degrees) while still achieving locking stability. This provides flexibility for the surgeon to avoid fracture lines, existing hardware, or critical anatomical structures.
- FAL Systems: Offer rigid, fixed-angle screw placement, providing maximum angular stability, particularly useful in osteoporotic bone or comminuted fractures where pull-out strength is critical.
- Compression Holes/Slots: Some plates incorporate dynamic compression units or slots, enabling the surgeon to apply compression across a fracture site or a TMT joint, promoting primary bone healing.
- Bridge Plating Capabilities: For highly comminuted fractures, especially of the metatarsal bases, plates can be used in a bridge fashion, spanning the comminuted segment without directly compressing it, thereby preserving the biology and promoting indirect healing.
- Screw Options: Systems typically include various screw lengths and diameters (e.g., 2.4mm, 2.7mm, 3.5mm) in both locking and non-locking configurations to suit different bone densities and anatomical requirements.
Materials
The choice of material is paramount for biocompatibility, strength, and long-term stability.
- Medical-Grade Titanium Alloys (e.g., Ti-6Al-4V ELI):
- Biocompatibility: Highly inert, minimizing adverse reactions within the body.
- Strength-to-Weight Ratio: Excellent mechanical properties provide robust fixation while being lightweight.
- Corrosion Resistance: Highly resistant to degradation in the physiological environment.
- MRI Compatibility: Generally considered MRI safe, though some artifact may be present depending on the field strength and implant size.
- Osseointegration: Titanium's surface properties can promote bone ingrowth, enhancing fixation.
- Stainless Steel (e.g., 316L): While historically used, it is less common for primary Lisfranc fixation due to its lower MRI compatibility and higher stiffness compared to titanium, which can lead to stress shielding.
Mechanisms of Action
The Lisfranc Midfoot Plating System functions by:
- Restoring Anatomical Alignment: The primary goal is to accurately reduce and maintain the anatomical relationship between the tarsals and metatarsals, recreating the normal arch and joint congruity.
- Stable Fixation of TMT Joints: By rigidly connecting the fractured or dislocated bones, the plates provide immediate stability, preventing further displacement and allowing for early soft tissue healing.
- Load Sharing: Unlike simple screw fixation, which can be load-bearing (carrying all the stress), well-designed plates can facilitate load sharing between the implant and the bone, promoting physiological stress distribution and reducing the risk of stress shielding.
- Prevention of Collapse and Arthritis: By maintaining reduction and stability, the system prevents the progressive collapse of the midfoot arch and significantly reduces the likelihood of developing debilitating post-traumatic arthritis, a common long-term complication of inadequately treated Lisfranc injuries.
Extensive Clinical Indications & Usage
The Lisfranc Midfoot Plating System is indicated for a range of complex midfoot pathologies, demanding precise surgical technique and careful patient selection.
Clinical Indications
- Acute Lisfranc Injuries:
- Fracture-Dislocations: The most common indication, involving disruption of the TMT joints with associated fractures of the metatarsal bases or cuneiforms.
- Pure Dislocations: Disruption of the TMT joints without significant bony fractures, often involving severe ligamentous injury.
- Ligamentous Injuries: Severe sprains or ruptures of the Lisfranc ligament complex leading to instability, even without overt dislocation or fracture on initial X-rays (often identified with stress views or advanced imaging).
- Chronic Lisfranc Instability: Patients presenting with persistent pain, arch collapse, and instability months or years after an inadequately treated or missed Lisfranc injury.
- Revision Surgery: For failed primary fixation with K-wires or screws, or for non-union/malunion following initial treatment.
- Specific Injury Patterns: Effective for homolateral, divergent, and isolated Lisfranc injury patterns, requiring tailored plating strategies.
Surgical Applications (Detailed Steps & Considerations)
- Pre-operative Planning:
- Imaging: Comprehensive evaluation with weight-bearing X-rays (AP, oblique, lateral), CT scans (for bony detail), and sometimes MRI (for ligamentous and soft tissue assessment).
- Templating: Using imaging to pre-plan plate size, screw lengths, and incision placement.
- Patient Education: Discussing the procedure, expected recovery, and potential complications.
- Patient Positioning and Exposure:
- Positioning: Supine position with a bump under the ipsilateral hip to internally rotate the foot. A thigh tourniquet is typically used for hemostasis.
- Incisions: Usually one or two dorsal longitudinal incisions (e.g., between 1st and 2nd metatarsals, and between 3rd and 4th metatarsals) to access the TMT joints. Careful soft tissue handling is crucial to protect dorsal nerves and vessels.
- Reduction Techniques:
- Direct Reduction: Using bone clamps, K-wires (as "joy-sticks"), or specialized reduction forceps to meticulously realign the TMT joints and fracture fragments.
- Indirect Reduction: Traction and manipulation to restore anatomical relationships.
- Temporary Fixation: K-wires are often used to temporarily hold the reduction before plate application.
- Plate Selection and Contouring:
- Plate Selection: Choosing the appropriate anatomical plate (e.g., specific plates for the first TMT joint, or bridge plates for metatarsal shafts).
- Contouring: While many plates are pre-contoured, minor adjustments may be necessary using plate bending instruments to achieve an optimal fit and minimize soft tissue impingement.
- Screw Insertion:
- Pilot Drilling: Creating a pilot hole with a drill bit corresponding to the chosen screw diameter.
- Depth Gauging: Measuring the required screw length precisely to ensure bicortical purchase without over-penetration.
- Screw Insertion:
- Non-locking Screws: Can be used first to achieve compression across a fracture or joint, pulling the fragments together.
- Locking Screws: Provide angular stability by locking into the plate, ideal for osteoporotic bone or comminuted fractures, and for maintaining reduction.
- Sequence: Often, non-locking screws are inserted first for reduction and compression, followed by locking screws for rigid fixation.
- Post-operative Care:
- Immobilization: Non-weight-bearing in a cast or splint for 6-8 weeks, depending on injury severity and surgeon preference.
- Weight-Bearing Progression: Gradual transition to partial and then full weight-bearing, often guided by clinical and radiographic healing.
- Physical Therapy: Essential for restoring range of motion, strength, and gait mechanics.
Fitting/Usage Instructions (Surgeon-Focused)
- Anatomical Reduction First: The plate is a holding device, not a reduction tool. Achieve and confirm anatomical reduction before applying the plate.
- Plate Positioning: Place plates dorsally, avoiding tension on soft tissues and ensuring adequate screw purchase in the metatarsal bases and cuneiforms.
- Screw Trajectory: Carefully consider screw trajectory to avoid joint penetration, damage to neurovascular structures, and to maximize bone purchase.
- Compression: Utilize compression holes or lag screws through the plate to achieve interfragmentary compression where appropriate, promoting primary healing.
- Bridge Plating: For comminuted fractures, use bridge plating principles to span the comminution, preserving periosteal blood supply.
- Intraoperative Imaging: Fluoroscopy is essential to confirm anatomical reduction and correct implant placement throughout the procedure.
Risks, Side Effects, or Contraindications
While Lisfranc Midfoot Plating Systems offer significant benefits, potential risks and complications must be considered.
Risks & Complications
- Infection: Superficial or deep surgical site infection, potentially requiring additional surgery and antibiotic treatment.
- Non-union/Malunion: Failure of bones to heal or healing in an unacceptable position, leading to persistent pain and dysfunction.
- Hardware Irritation/Prominence: Due to the subcutaneous location of the plates, hardware can be palpable and cause irritation, often necessitating removal after healing.
- Nerve or Vascular Injury: Damage to dorsal cutaneous nerves (e.g., superficial peroneal nerve branches) or dorsal pedal vessels during incision or dissection.
- Post-traumatic Arthritis: Despite optimal fixation, severe cartilage damage at the time of injury can still lead to progressive arthritis, sometimes requiring future fusion.
- Loss of Reduction: Failure of the construct to maintain anatomical alignment post-operatively.
- Complex Regional Pain Syndrome (CRPS): A severe, chronic pain condition that can develop after trauma or surgery.
- Deep Vein Thrombosis (DVT) / Pulmonary Embolism (PE): Risks associated with any lower extremity surgery and prolonged immobilization.
- Screw Breakage/Loosening: Though rare with modern systems, can occur, especially with premature weight-bearing or poor bone quality.
Contraindications
- Active Infection: Absolute contraindication at the surgical site. Surgery should be delayed until the infection is resolved.
- Severe Peripheral Vascular Disease: Compromised blood supply can impair healing and increase infection risk.
- Uncontrolled Diabetes: Poor glycemic control increases infection risk and impairs wound healing.
- Extremely Poor Bone Quality (Severe Osteoporosis): If bone stock is insufficient to hold screws and plates securely, alternative fixation or primary fusion may be considered.
- Patient Non-compliance: Patients unwilling or unable to adhere to strict post-operative weight-bearing and rehabilitation protocols may be at higher risk for complications.
- Significant Soft Tissue Damage: Open injuries with extensive soft tissue loss or severe swelling may require staged procedures or external fixation initially.
Maintenance & Sterilization Protocols
Maintaining the sterility and functionality of reusable surgical instruments is paramount in orthopedic surgery. Implants (plates, screws) are typically single-use and provided in sterile packaging.
Reusable Instruments (e.g., drivers, drill bits, bending tools, reduction forceps)
- Point-of-Use Cleaning: Immediately after use, instruments should be wiped clean of gross contamination with a damp cloth to prevent drying of blood and tissue.
- Decontamination (Manual or Automated):
- Manual Cleaning: Soaking in enzymatic detergent, brushing away debris, and rinsing thoroughly.
- Automated Cleaning: Use of ultrasonic cleaners and washer-disinfectors following manufacturer's instructions.
- Inspection: Thorough inspection for damage, corrosion, or wear. Damaged instruments should be removed from circulation.
- Packaging: Instruments are arranged in trays, often with specific layouts, and then wrapped in sterilization wraps or placed in rigid sterilization containers.
- Sterilization:
- Steam Sterilization (Autoclaving): The most common method. Instruments are exposed to saturated steam at high temperatures (e.g., 121°C for 30 minutes or 132°C for 4 minutes) and pressure. Parameters must adhere to manufacturer guidelines and hospital policies.
- Sterilization Indicators: Chemical and biological indicators are used to confirm successful sterilization cycles.
- Storage: Sterile instruments are stored in a clean, dry environment until needed.
Implants (Plates & Screws)
- Single-Use, Sterile Packaging: Lisfranc plates and screws are typically supplied sterile in individual or kit packaging.
- Storage: Store implants in their original, unopened, undamaged sterile packaging in a cool, dry place away from direct sunlight, adhering to manufacturer's specified temperature and humidity ranges.
- Expiration Dates: Always check expiration dates prior to use. Do not use expired implants.
- Handling: Handle implants only with sterile gloves and instruments to maintain sterility.
Biomechanics
The midfoot is a complex biomechanical region, and understanding its function is critical for effective Lisfranc injury treatment.
- Role of the Lisfranc Ligament Complex: This intricate network of ligaments, particularly the stout Lisfranc ligament connecting the medial cuneiform to the second metatarsal base, is the keystone of midfoot stability. It prevents dorsal and lateral displacement of the metatarsals relative to the tarsals and maintains the midfoot arch.
- Kinematics of the Midfoot: The TMT joints allow for limited but crucial motion during gait, accommodating uneven terrain and absorbing shock. The first TMT joint is the most mobile, while the second and third TMT joints are relatively rigid.
- How Plating Restores Stability and Load Transfer:
- By rigidly fixing the TMT joints, plating restores the anatomical relationship, preventing abnormal motion and subsequent degeneration.
- The plates act as internal splints, allowing the injured ligaments and bone to heal in a stable environment.
- Modern low-profile, contoured plates are designed to minimize stress shielding, allowing physiological loads to be transmitted through the bone, which is essential for bone healing and preventing osteopenia.
- Comparison of Screw-Only Fixation vs. Plating:
- Screw-Only: Traditionally used, particularly for the Lisfranc ligament. While effective for direct compression, screws can be prone to breakage or loosening, especially with early weight-bearing. They also tend to be more load-bearing, potentially leading to stress shielding.
- Plating: Offers broader distribution of forces, enhanced multi-planar stability, and is less prone to loosening. Anatomical plates provide superior contouring and can be used for bridge plating, which is advantageous for comminuted fractures. Studies often show reduced rates of hardware failure with plates compared to screws alone.
- Advantages of Bridge Plating: For comminuted metatarsal base fractures, bridge plating allows the fracture fragments to heal without direct compression, preserving the periosteal blood supply and promoting callus formation, which is crucial for indirect bone healing.
- Stress Shielding: Overly rigid implants can prevent physiological stress from being transmitted through the bone, leading to bone resorption (stress shielding). Modern Lisfranc plating systems are designed with material properties and designs that aim to minimize this effect while providing adequate stability.
Patient Outcome Improvements
The adoption of dedicated Lisfranc Midfoot Plating Systems has demonstrably improved patient outcomes compared to older fixation methods.
- Improved Anatomical Reduction: The pre-contoured nature and robust fixation capabilities facilitate more precise and stable anatomical reduction, which is the most critical factor in preventing long-term complications.
- Enhanced Stability: Plating provides superior multi-planar stability, maintaining reduction even under early controlled loading, which is vital for preventing displacement.
- Reduced Pain: Stable fixation and anatomical restoration contribute to significantly reduced post-operative pain and chronic pain often associated with malunion or instability.
- Earlier Weight-Bearing and Functional Recovery: With enhanced stability, surgeons can often implement more aggressive, earlier weight-bearing protocols, leading to faster rehabilitation and return to activities of daily living.
- Lower Incidence of Post-traumatic Arthritis: By preserving joint congruity and preventing abnormal motion, plating significantly lowers the incidence and severity of post-traumatic arthritis compared to non-operative treatment or inadequate fixation.
- Return to Activity/Sport: Patients, especially active individuals, have a higher chance of returning to pre-injury activity levels, including sports, due to the robust and stable reconstruction of the midfoot.
- Potential for Implant Removal: While some patients live comfortably with the plates indefinitely, the low-profile design and biocompatibility often mean hardware removal is not always necessary. However, if hardware prominence or irritation occurs, removal is a straightforward procedure, typically performed 6-12 months post-surgery after bony healing is confirmed.
Massive FAQ Section
1. What is a Lisfranc injury?
A Lisfranc injury refers to an injury to the Lisfranc joint complex, which includes the bones and ligaments that connect the midfoot (tarsals) to the forefoot (metatarsals). These injuries can range from mild sprains to severe fracture-dislocations.
2. How is a Lisfranc injury diagnosed?
Diagnosis typically involves X-rays (including weight-bearing views), often supplemented by CT scans for detailed bony assessment and sometimes MRI for ligamentous evaluation. Stress views may be used to uncover subtle instability.
3. Why is surgery often necessary for Lisfranc injuries?
Unstable Lisfranc injuries, where the bones are displaced or the ligaments are severely torn, require surgery to restore anatomical alignment and stability. Without proper surgical fixation, these injuries can lead to chronic pain, midfoot collapse, and debilitating post-traumatic arthritis.
4. What is the Lisfranc Midfoot Plating System?
It's a specialized orthopedic implant system consisting of anatomically contoured titanium plates and screws designed to stabilize and fix fractures and dislocations within the Lisfranc joint complex. These systems offer rigid fixation and promote anatomical healing.
5. What materials are used in these plates?
Modern Lisfranc Midfoot Plating Systems primarily use medical-grade titanium alloys (e.g., Ti-6Al-4V ELI). Titanium is chosen for its excellent biocompatibility, high strength-to-weight ratio, corrosion resistance, and MRI compatibility.
6. How long does the recovery take after Lisfranc plating surgery?
Recovery is typically a multi-stage process. Non-weight-bearing in a cast or boot for 6-8 weeks is common, followed by a gradual progression to partial and then full weight-bearing, often with the aid of physical therapy. Full recovery and return to activities can take 6-12 months or longer, depending on the injury severity and individual healing.
7. Will I need to have the plates removed?
Hardware removal is not always necessary. Many patients can live comfortably with the plates indefinitely. However, if the plates cause irritation, pain, or discomfort due to their prominence, or if an infection develops, removal may be recommended, typically 6-12 months after the initial surgery once healing is complete.
8. What are the potential complications of Lisfranc plating?
Potential complications include infection, non-union or malunion (bones not healing correctly), hardware irritation requiring removal, nerve damage, post-traumatic arthritis, loss of reduction, and Complex Regional Pain Syndrome (CRPS).
9. Can I put weight on my foot after surgery?
Generally, patients are advised to remain non-weight-bearing on the affected foot for the initial 6-8 weeks post-surgery to allow for proper bone and ligament healing and to protect the surgical repair. Your surgeon will provide specific instructions based on your injury and surgical outcome.
10. How does plating compare to traditional screw fixation for Lisfranc injuries?
Plating systems offer several advantages over traditional screw-only fixation, including superior multi-planar stability, better load distribution, reduced risk of screw breakage, and less incidence of stress shielding. Anatomical plates also conform better to the complex midfoot anatomy, potentially leading to more consistent anatomical reductions.
11. What is the role of physical therapy in recovery?
Physical therapy is crucial for restoring function. It typically begins after the initial non-weight-bearing period, focusing on regaining range of motion, strengthening the foot and ankle muscles, improving balance, and normalizing gait patterns.
12. Can I return to sports after a Lisfranc injury treated with plating?
Return to sports is possible but requires a gradual, guided rehabilitation program. The timeline varies significantly based on the severity of the injury, individual healing, and the demands of the sport. It can take 9-18 months, with careful progression from low-impact activities to sport-specific training. Your surgeon and physical therapist will guide this process.