

Kirschner Wires (K-Wires, 0.028" - 0.062"): The Definitive Orthopedic Guide
1. Comprehensive Introduction & Overview
Kirschner Wires, universally known as K-Wires, are fundamental instruments in orthopedic and trauma surgery. Since their introduction by Martin Kirschner in 1909, these simple yet remarkably versatile pins have become indispensable for temporary skeletal fixation, definitive stabilization of small bone fractures, and as guides for other implants. Ranging in diameter typically from 0.028 inches (0.7 mm) to 0.062 inches (1.6 mm), K-Wires offer a delicate balance of strength, flexibility, and minimal invasiveness, making them ideal for a myriad of applications, particularly in the hand, wrist, foot, and elbow.
Their primary function is to provide stable fixation for bone fragments, allowing for proper healing and anatomical alignment. K-Wires achieve this by traversing bone fragments, holding them in a reduced position without requiring extensive surgical exposure. This percutaneous nature minimizes soft tissue disruption, reduces surgical time, and often allows for a less invasive approach to fracture management. This guide will delve into the intricate details of K-Wires, covering their design, materials, extensive clinical applications, biomechanical principles, crucial maintenance protocols, and their profound impact on patient outcomes.
2. Deep-dive into Technical Specifications & Mechanisms
Design & Materials
K-Wires are characterized by their slender, cylindrical design, typically featuring a sharp tip for easy insertion and a smooth shaft. The choice of material and tip design is critical for their performance and safety.
- Materials:
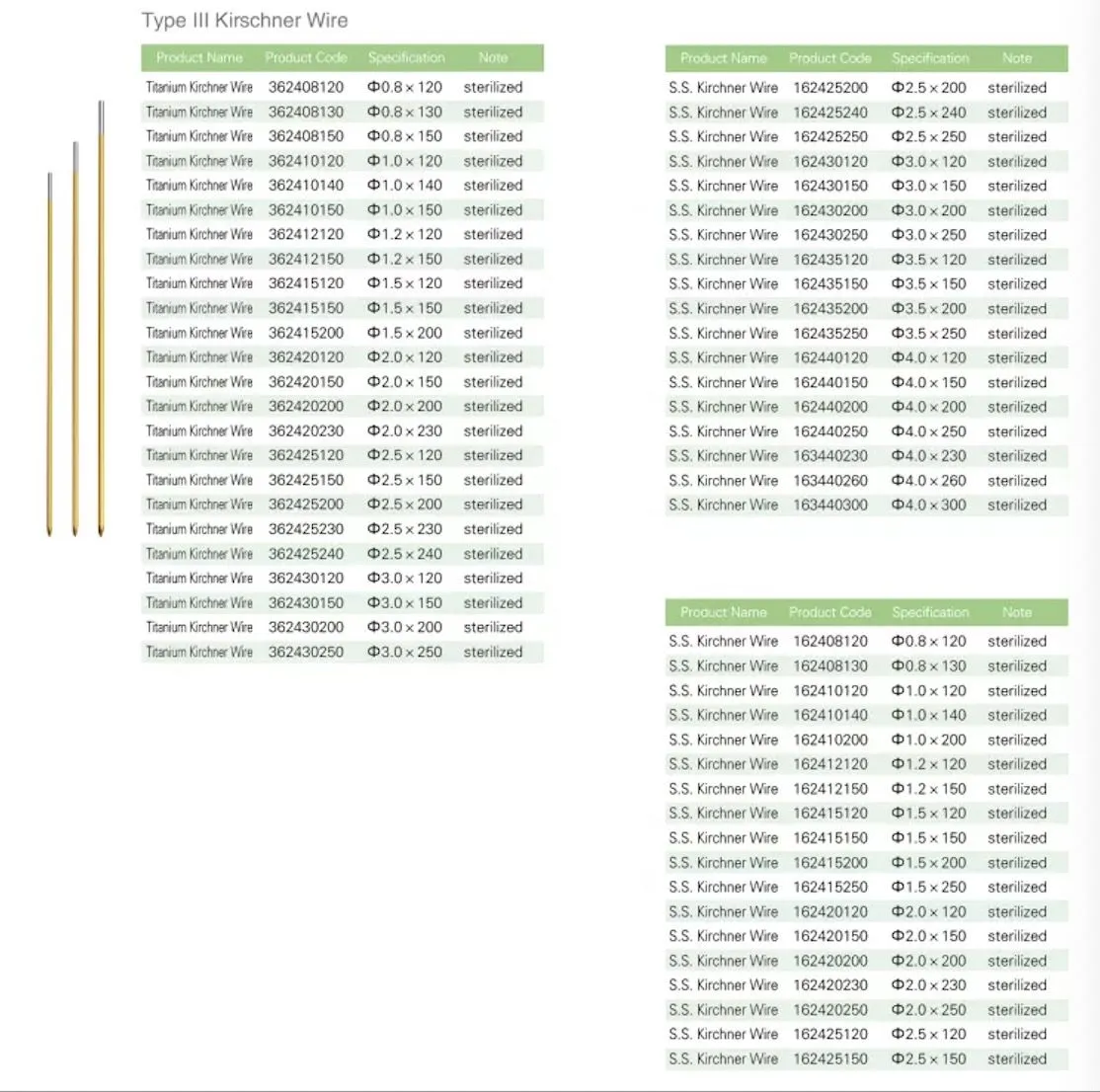
- 316L Stainless Steel: The most common material, offering excellent biocompatibility, high tensile strength, and corrosion resistance. This surgical-grade stainless steel ensures the wire can withstand the biological environment and the mechanical stresses of fixation.
- Titanium Alloys: Less common for standard K-wires but used when MRI compatibility is paramount or in patients with known nickel allergies (though rare with 316L SS). Titanium offers superior biocompatibility and strength-to-weight ratio.
- Tip Configurations: The tip design facilitates penetration through bone and soft tissue with minimal resistance.
- Trocar Tip: A three-sided, pyramidal tip, providing excellent cutting action and precise entry. Ideal for dense cortical bone.
- Diamond Tip: A four-sided, sharpened tip, offering good penetration and often preferred for softer bone or when a balance between cutting and pushing is desired.
- Chisel Tip: A two-sided, wedge-shaped tip, useful for directing the wire along a specific plane or for less aggressive penetration.
- Shaft Characteristics:
- Smooth Surface: The defining characteristic of a K-wire, allowing for easy insertion and removal.
- Diameter Range: As specified, from 0.028" (0.7 mm) to 0.062" (1.6 mm). The selection depends on the bone size, fracture pattern, and desired stiffness. Larger diameters offer greater rigidity but increase bone damage and risk of thermal necrosis if not drilled carefully.
- Length Variations: Available in various lengths, typically from 6 to 12 inches (15 to 30 cm), to accommodate different anatomical sites and fixation requirements.
Biomechanics of K-Wire Fixation
The effectiveness of K-wire fixation hinges on fundamental biomechanical principles. K-wires primarily act as internal splints, providing temporary stabilization rather than rigid, load-bearing support.
- Principle of Temporary Stabilization: K-wires are designed to hold reduced fracture fragments in place until biological healing provides sufficient stability. They are generally removed once callus formation is adequate.
- Load-Sharing vs. Load-Bearing: K-wires are typically load-sharing devices, meaning they share the load with the bone and surrounding soft tissues. They are not designed for full load-bearing in most applications, which is why external immobilization (casts, splints) often accompanies K-wire fixation.
- Factors Affecting Stability:
- Wire Diameter: Bending stiffness is proportional to the fourth power of the radius (d^4). A small increase in diameter significantly increases stiffness and resistance to bending and shear forces. However, too large a wire can compromise bone integrity.
- Number of Wires: Multiple wires in divergent or convergent configurations provide enhanced rotational and translational stability, creating a "construct."
- Wire Configuration:
- Crossed K-wires: Commonly used in distal radius or elbow fractures, offering good stability against bending and shear.
- Parallel K-wires: Effective for maintaining length and alignment.
- Tension Band Wiring: Utilizes K-wires and a cerclage wire to convert tensile forces into compressive forces, particularly for fractures of the olecranon or patella.
- Bone Quality: Fixation is stronger in dense cortical bone compared to cancellous bone.
- Entry Angle and Trajectory: Optimal angles minimize stress risers in the bone and provide maximum purchase.
- Limitations: While versatile, K-wires have limitations. They offer limited resistance to axial compression and rotation when used individually. Their percutaneous nature, while advantageous, carries a risk of pin tract infection.
3. Extensive Clinical Indications & Usage
K-Wires are exceptionally versatile and are employed across numerous orthopedic subspecialties for both definitive and temporary fixation.
Surgical Applications
K-wires are indispensable in the management of a wide array of fractures and orthopedic conditions.
- Fracture Fixation:
- Hand & Wrist:
- Metacarpal & Phalangeal Fractures: Common for stabilizing shaft, neck, and base fractures, particularly in displaced or unstable patterns.
- Distal Radius Fractures (Colles', Smith's, Barton's): Used for percutaneous pin fixation, often in conjunction with external fixation or cast immobilization, to maintain reduction.
- Scaphoid Fractures: Can be used for temporary stabilization or as guide wires for cannulated screws.
- Foot & Ankle:
- Metatarsal & Phalangeal Fractures: Similar to hand fractures, providing stable fixation for small bones.
- Malleolar Fractures: Used in tension band wiring for medial malleolus or for temporary stabilization during ORIF of bimalleolar/trimalleolar fractures.
- Calcaneal Fractures: Can be used for temporary stabilization or reduction techniques.
- Hallux Valgus Correction (Bunionectomy): For maintaining alignment after osteotomies.
- Elbow:
- Supracondylar Humerus Fractures (Pediatric): A cornerstone of treatment, often using crossed or lateral entry K-wires to stabilize the fracture while preserving the growth plate.
- Olecranon Fractures: Essential component of tension band wiring for stable fixation.
- Radial Head/Neck Fractures: For temporary fixation or specific fracture patterns.
- Patella Fractures: Used in tension band wiring or for temporary fixation.
- Pediatric Fractures: Preferred for many juxta-epiphyseal and physeal fractures due to their minimal impact on growth plates.
- Hand & Wrist:
- Temporary Fixation: During complex open reduction and internal fixation (ORIF) procedures, K-wires are invaluable for holding fracture fragments in anatomical position while definitive implants (plates, screws) are applied.
- Guide Wires: Smaller diameter K-wires are frequently used as guide wires for cannulated screws, allowing for precise placement of the screw without requiring a separate drill hole.
- Tension Band Wiring: A specific technique that employs K-wires and a cerclage wire to compress fracture fragments, particularly effective for avulsion fractures where muscle pull creates tensile forces (e.g., olecranon, patella, medial malleolus).
- Joint Arthrodesis (Fusion): For maintaining joint alignment during fusion procedures, especially in the hand and foot.
- External Fixation: K-wires can serve as pins for certain types of external fixators, particularly in the hand or foot, providing stability to complex fractures or for limb lengthening procedures.
Fitting & Usage Instructions
Precise technique is paramount to maximize the efficacy and minimize complications associated with K-wire insertion.
- Pre-operative Planning:
- Imaging: Thorough review of X-rays, CT scans, or MRI to understand fracture morphology, displacement, and bone quality.
- Wire Size Selection: Choose the smallest diameter wire that provides adequate stability. Larger wires increase bone damage and risk of thermal necrosis.
- Entry Points & Trajectory: Plan the optimal entry points to avoid neurovascular structures and achieve the desired purchase in bone.
- Aseptic Technique: Strict sterile protocols are essential to prevent pin tract infection. This includes surgical scrubbing, sterile draping, and sterile instruments.
- Anesthesia: Local, regional, or general anesthesia is administered to ensure patient comfort and muscle relaxation.
- Reduction: The fracture fragments must be anatomically reduced manually or with reduction clamps under fluoroscopic guidance.
- Wire Insertion:
- Power Drill: K-wires are typically inserted using a low-speed, high-torque power drill or a hand chuck. High-speed drilling generates excessive heat, leading to thermal necrosis of bone, which can cause loosening or infection.
- Controlled Insertion: Apply steady, gentle pressure. Advance the wire slowly, allowing the tip to cut through the bone.
- Fluoroscopic Guidance: Real-time imaging is crucial to monitor wire trajectory, ensure proper reduction, and avoid neurovascular structures.
- Bicortical Purchase: Aim for penetration of both cortices of the bone for optimal stability, but avoid excessive protrusion that could irritate soft tissues or nerves.
- Skin Protection: After insertion, the wires are usually bent and cut short, leaving a small segment protruding from the skin. K-wire caps or silicone tubing can be placed over the ends to protect the skin and prevent snagging.
- Post-operative Management:
- Dressing: Sterile dressings are applied around the pin sites.
- Immobilization: Often, an external cast or splint is applied to supplement the K-wire fixation and protect the fracture during healing.
- Pin Site Care: Meticulous pin site care is crucial to prevent infection (see Maintenance section).
- Wire Removal: K-wires are typically removed in an outpatient setting once sufficient healing has occurred, usually between 3-6 weeks, depending on the fracture and patient. Removal is generally quick and performed under local anesthesia.
4. Maintenance/Sterilization Protocols
Maintaining the integrity and sterility of K-wires is paramount for patient safety and optimal surgical outcomes.
- Single-Use Policy: The vast majority of Kirschner Wires are designed and intended for single-use only. This is critical to prevent cross-contamination, material fatigue, and dulling of the tip. Reusing K-wires can lead to:
- Increased risk of infection due to incomplete sterilization.
- Reduced cutting efficiency, requiring more force for insertion and increasing the risk of thermal necrosis.
- Potential for wire breakage due to material fatigue from previous use and sterilization cycles.
- Compromised biomechanical properties.
- Sterilization (for new, sterile-packaged K-wires):
- K-wires are typically supplied in sterile, individually packaged units.
- They are sterilized by the manufacturer using validated methods such as gamma irradiation or ethylene oxide (EtO) gas, ensuring a high sterility assurance level (SAL).
- Storage: Store in their original sterile packaging in a clean, dry environment, protected from extreme temperatures and physical damage.
- Inspection Prior to Use:
- Before opening the sterile package, visually inspect for any signs of damage to the packaging.
- After opening, inspect the K-wire itself for:
- Integrity: Ensure no bends, kinks, or deformities.
- Sharpness: Verify the tip is sharp and undamaged.
- Surface Finish: Check for any burrs, rough spots, or corrosion.
- Correct Size: Confirm the diameter and length match the surgical plan.
- Post-Operative Pin Site Care (Patient/Nursing Staff):
- Daily Cleaning: Pin sites should be cleaned daily or as directed by the surgeon, using sterile saline solution or antiseptic wipes (e.g., chlorhexidine).
- Dressing: Apply fresh, sterile, non-occlusive dressings to allow air circulation and absorb exudate.
- Monitoring: Regularly inspect pin sites for signs of infection (redness, swelling, pus, increased pain, warmth).
- Hygiene: Patients should be instructed on proper hand hygiene before touching pin sites. Showering may be permitted if pin sites are kept dry or appropriately covered, as advised by the surgeon.
5. Risks, Side Effects, or Contraindications
While K-wires are generally safe and effective, like any surgical intervention, their use carries potential risks and contraindications.
Risks & Complications
- Pin Tract Infection: The most common complication. Bacteria can migrate along the wire from the skin, leading to localized infection, osteomyelitis, or even systemic sepsis in severe cases. Meticulous pin site care and prophylactic antibiotics can reduce this risk.
- Neurovascular Injury: During insertion, K-wires can inadvertently damage nearby nerves, arteries, or veins, leading to pain, numbness, weakness, bleeding, or vascular compromise. Careful pre-operative planning and fluoroscopic guidance are crucial.
- Wire Breakage/Migration: Although rare with proper technique and material, wires can break, especially if subjected to excessive stress or if material fatigue occurs. Wires can also migrate, either proximally or distally, potentially irritating soft tissues or entering joint spaces.
- Loss of Reduction: If the K-wire fixation is insufficient or if the patient overloads the limb, the fracture fragments may displace, leading to malunion or nonunion.
- Thermal Necrosis: High-speed drilling generates heat, which can damage bone cells, leading to localized bone death. This can compromise fixation, increase infection risk, and impede healing.
- Soft Tissue Impingement/Irritation: Wires protruding too far or placed near tendons or ligaments can cause irritation, tenosynovitis, or restricted movement.
- Allergic Reactions: Extremely rare with 316L stainless steel, but theoretically possible, typically due to nickel content. Titanium wires are an alternative in such cases.
- Scarring: Pin sites can leave small scars.
- Pain: While generally well-tolerated, patients may experience some discomfort or pain at the pin sites or with movement.
Contraindications
- Active Infection at Insertion Site: Inserting K-wires through an infected area can spread the infection deeper into the bone and surrounding tissues.
- Severe Comminution Where K-wires Alone Are Insufficient: For highly comminuted or unstable fractures that require rigid, load-bearing fixation, K-wires alone may not provide adequate stability.
- Patient Non-compliance: Patients who are unable or unwilling to adhere to post-operative instructions (e.g., pin site care, weight-bearing restrictions) may be at higher risk for complications.
- Certain Open Fractures with Extensive Contamination: While K-wires can be used in some open fractures, extensive contamination might make them less suitable, and alternative fixation methods might be preferred.
- Bone Stock Insufficiency: In severe osteoporosis or highly fragile bone, K-wires may not achieve sufficient purchase, leading to early loosening or failure.
6. Massive FAQ Section
Q1: What are Kirschner Wires (K-Wires) made of?
A1: K-Wires are predominantly made from high-grade 316L stainless steel, which offers excellent biocompatibility, strength, and corrosion resistance. In specific cases, such as for MRI compatibility or nickel allergy concerns, titanium alloys may be used.
Q2: What are the common sizes of K-Wires?
A2: K-Wires are available in a range of diameters, typically from 0.028 inches (0.7 mm) to 0.062 inches (1.6 mm). The specific size chosen depends on the bone size, fracture pattern, and the required stability.
Q3: How long do K-Wires typically stay in?
A3: The duration K-Wires remain in place varies depending on the fracture type, bone location, and individual healing rates. Generally, they are kept in for 3 to 6 weeks, or until sufficient callus formation provides adequate bone stability, after which they are removed.
Q4: Is K-Wire removal painful?
A4: K-wire removal is generally a quick procedure and is typically performed in an outpatient setting, often under local anesthesia to minimize discomfort. Patients may feel a pulling sensation or brief pressure, but it is usually well-tolerated and much less painful than insertion.
Q5: Can K-Wires be reused?
A5: No, Kirschner Wires are designed and intended for single-use only. Reusing K-wires significantly increases the risk of infection, dulls the tip, and can lead to material fatigue and potential breakage.
Q6: What is the difference between K-Wires and Steinmann pins?
A6: Both are smooth, metallic pins used in orthopedics, but Steinmann pins are generally much larger in diameter (typically >2.0 mm up to 6.0 mm) and are used for heavier skeletal traction or for more robust temporary fixation in larger bones (e.g., femur, tibia). K-wires are smaller and primarily used for small bone fixation or temporary stabilization.
Q7: How do you care for K-Wire pin sites?
A7: Pin site care typically involves daily cleaning with a sterile saline solution or an antiseptic wipe (e.g., chlorhexidine) to remove any crusting or discharge. New, sterile, non-occlusive dressings should then be applied. It's crucial to follow your surgeon's specific instructions.
Q8: What are the signs of a K-Wire infection?
A8: Signs of a pin tract infection include increased redness, swelling, warmth, pain, tenderness around the pin site, and the presence of pus or foul-smelling discharge. Fever or chills can indicate a more systemic infection. Contact your doctor immediately if you notice these symptoms.
Q9: Can I shower with K-Wires in?
A9: Whether showering is permitted depends on your surgeon's specific instructions and the location of the K-wires. Some surgeons allow showering if the pin sites are covered with a waterproof dressing, while others may advise sponge baths to keep the sites dry. Always clarify with your healthcare provider.
Q10: What activities should be avoided with K-Wires?
A10: Generally, activities that put stress or direct impact on the injured limb or K-wires should be avoided. This includes heavy lifting, contact sports, strenuous exercise, and any movements that cause pain or could dislodge the wires. Follow your surgeon's weight-bearing and activity restrictions carefully.
Q11: Are K-Wires visible on X-rays?
A11: Yes, K-wires are made of radiopaque materials (stainless steel or titanium) and are clearly visible on X-rays, which allows surgeons to confirm their placement and monitor fracture healing.
Q12: What happens if a K-Wire breaks?
A12: While rare, if a K-wire breaks, it typically requires surgical removal of the retained fragment. The complexity of removal depends on the location of the break and how deeply the fragment is embedded. This is one of the reasons why K-wires are single-use only.
Q13: How are K-Wires sterilized?
A13: New K-wires are typically supplied in sterile packaging by the manufacturer, having been sterilized using methods like gamma irradiation or ethylene oxide (EtO) gas. They are not to be re-sterilized or reused by healthcare facilities.