The Intramedullary Fibula Nail: An Orthopedic Specialist's Comprehensive Guide
1. Comprehensive Introduction & Overview
The fibula, though non-weight-bearing in the traditional sense, plays a crucial role in ankle stability and lower leg biomechanics. Fractures of the fibula, particularly those involving the distal third, often compromise the integrity of the ankle mortise, necessitating surgical stabilization. Among the various fixation methods, the Intramedullary Fibula Nail (IFN) has emerged as a highly effective and increasingly preferred option for specific fracture patterns.
An intramedullary fibula nail is a specialized orthopedic implant designed to be inserted into the medullary canal of the fibula, providing internal fixation for fractures. Unlike traditional plating techniques that involve external application to the bone surface, intramedullary nailing offers a load-sharing construct, distributing stresses more physiologically and minimizing soft tissue disruption. This approach leverages the inherent stability of the bone's central axis, offering robust fixation with potential benefits for patient recovery and functional outcomes.
This comprehensive guide delves into the intricate details of the Intramedullary Fibula Nail, covering its design principles, material science, detailed clinical applications, biomechanical advantages, surgical considerations, maintenance protocols, and the profound impact it has on patient care. As orthopedic specialists, understanding the nuances of this implant is paramount for optimal patient selection and superior surgical results.
2. Deep-dive into Technical Specifications / Mechanisms
Design and Materials
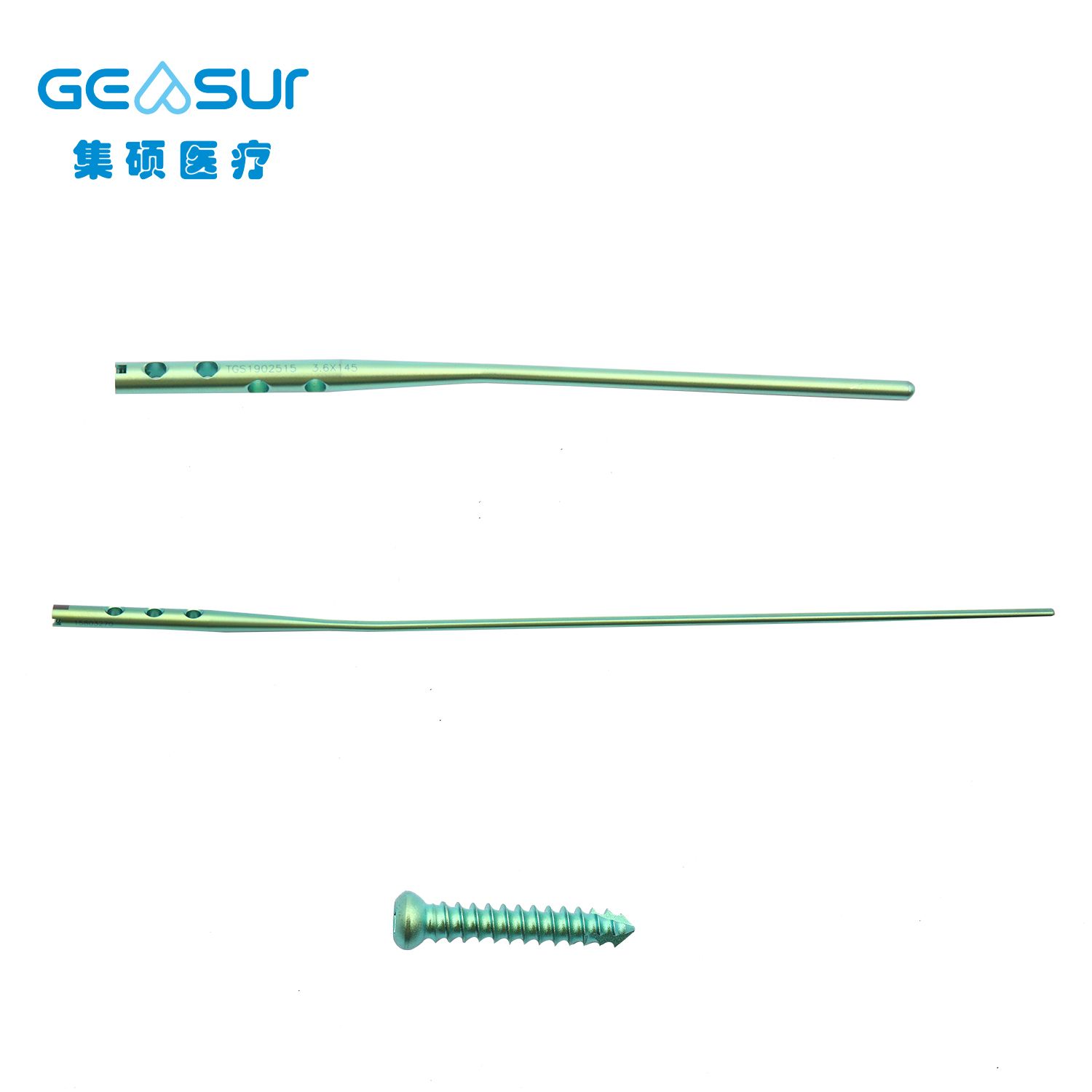
The design of an Intramedullary Fibula Nail is a testament to advanced biomechanical engineering, tailored to the unique anatomy and function of the fibula.
Nail Design Features:
- Anatomical Contouring: Many fibula nails feature a subtle pre-bend or anatomical curvature designed to conform to the natural bowing of the fibula, particularly in its distal segment. This ensures optimal fit and minimizes stress on the bone.
- Cannulation: Most modern fibula nails are cannulated, allowing for guidewire-assisted insertion. This facilitates precise placement, especially in complex fractures, and can aid in percutaneous distal locking.
- Locking Mechanisms:
- Proximal Locking: Typically achieved with one or two transverse or oblique screws through dedicated holes in the nail, securing it to the proximal fibula.
- Distal Locking: Often the most critical aspect for ankle stability. Distal locking can involve multiple screws (e.g., two or three) in various planes to capture small distal fragments and provide multiplanar stability to the ankle mortise. Some designs offer polyaxial or multi-directional locking options for enhanced fragment purchase.
- Tip Design: The nail tip is often tapered or bullet-shaped to facilitate smooth insertion and minimize cortical impingement.
- Diameter and Length: Available in a range of diameters (e.g., 3.0 mm to 4.5 mm) and lengths (e.g., 100 mm to 200 mm) to accommodate varying patient anatomies and fracture locations.
Material Science:
The choice of material for the Intramedullary Fibula Nail is critical for biocompatibility, mechanical strength, and fatigue resistance.
* Titanium Alloys (e.g., Ti-6Al-4V): The most common material.
* Biocompatibility: Excellent, minimizing adverse tissue reactions.
* Strength-to-Weight Ratio: High, providing robust fixation without excessive bulk.
* Elastic Modulus: Closer to that of cortical bone compared to stainless steel, which can lead to more physiological load sharing and reduce stress shielding.
* Radiolucency: Allows for better radiographic visualization of bone healing compared to denser materials.
* Stainless Steel (e.g., 316L Stainless Steel): Less common for fibula nails but used in some orthopedic implants.
* Strength: Very strong.
* Cost-Effective: Generally less expensive than titanium.
* Elastic Modulus: Higher than bone, potentially leading to more stress shielding.
* MRI Compatibility: Both titanium and stainless steel implants are generally considered MRI safe, though artifact generation can vary.
Biomechanics
The biomechanical principles underpinning the Intramedullary Fibula Nail are central to its efficacy.
* Load Sharing: Unlike plates which are load-bearing (carrying the majority of the load), intramedullary nails are load-sharing. They share axial loads with the bone, allowing for more physiological stress distribution across the fracture site. This encourages callus formation and reduces the risk of stress shielding, which can lead to osteopenia around the implant.
* Axial Stability: The nail provides excellent axial stability by resisting compressive and tensile forces along the long axis of the fibula.
* Torsional Stability: Locking screws (both proximal and distal) engage the bone fragments, preventing rotational displacement around the nail's axis. The design and number of locking screws are crucial for resisting torsional forces.
* Bending Stability: The nail's resistance to bending forces is proportional to its diameter and the material's stiffness. Its central placement within the medullary canal provides a strong lever arm against bending moments.
* Minimally Invasive: By preserving the periosteal blood supply, intramedullary nailing techniques are less disruptive to the bone's natural healing environment compared to extensive open plating, which can devascularize bone segments.
3. Extensive Clinical Indications & Usage
The Intramedullary Fibula Nail is indicated for a range of fibular fractures, particularly those associated with ankle instability.
Clinical Indications:
- Distal Fibula Fractures (Weber B and C equivalent):
- Spiral or oblique fractures of the distal fibula, especially those extending proximally.
- Fractures with associated syndesmotic injury (requiring additional syndesmotic screw fixation).
- Multifragmentary distal fibula fractures where plate fixation might be challenging due to comminution or soft tissue compromise.
- Maisonneuve Fractures: A highly unstable ankle injury involving a proximal fibula fracture, syndesmotic disruption, and often a deltoid ligament rupture or medial malleolus fracture. The fibula nail can stabilize the proximal fibula component.
- Fibular Shaft Fractures: Less common but can be treated with an IFN if isolated or part of a more complex injury pattern.
- Pilon Fractures with Fibular Involvement: To reconstruct the fibular length and rotation, which is critical for restoring the ankle mortise in complex pilon fractures.
- Open Fractures: In select cases, where soft tissue damage is extensive, an intramedullary device may be preferred over a plate to minimize further soft tissue stripping and reduce infection risk.
- Osteoporotic Bone: The load-sharing nature and broad cortical contact of an intramedullary nail can offer superior fixation in osteoporotic bone compared to plates, which rely on screw purchase in potentially weak cortical bone.
Fitting/Usage Instructions (Surgical Overview):
The implantation of an Intramedullary Fibula Nail follows a standardized surgical protocol, typically performed under fluoroscopic guidance.
- Patient Positioning: Supine position with a bump under the ipsilateral hip, allowing for medial ankle access and fluoroscopy.
- Incision: A small incision (typically 1-2 cm) is made proximally or distally, depending on the entry point chosen (e.g., lateral malleolus tip or just proximal to it).
- Entry Point Creation: Using an awl or drill, an entry portal is created into the medullary canal of the fibula. The entry point is critical for proper nail alignment and to avoid iatrogenic fracture.
- Reduction: The fibula fracture is anatomically reduced using gentle traction, manipulation, and sometimes reduction clamps. Fluoroscopy is used to confirm reduction.
- Guidewire Insertion: A guidewire is advanced across the fracture site and into the proximal fibular segment, extending to the desired length.
- Reaming (Optional): While some fibula nails are designed for unreamed insertion, reaming the medullary canal can be performed to create space for a larger diameter nail, potentially increasing stability. This is typically done with flexible reamers.
- Nail Insertion: The appropriate length and diameter nail is selected and advanced over the guidewire across the fracture site, ensuring proper rotational alignment.
- Proximal Locking: Using a targeting jig or freehand technique under fluoroscopy, proximal locking screws are inserted to secure the nail in the proximal fibula.
- Distal Locking: This is often the most challenging step. Distal locking screws are inserted through the nail, capturing the distal fibular fragment and stabilizing the ankle mortise. Precise fluoroscopic images (AP, lateral, mortise views) are essential for accurate screw placement, avoiding neurovascular structures and ensuring proper syndesmotic reduction.
- Syndesmotic Fixation (if indicated): If a syndesmotic injury is present, one or more syndesmotic screws may be placed across the syndesmosis after fibular fixation, either through the nail or as a separate construct.
- Wound Closure: The incisions are irrigated, and soft tissues and skin are closed in layers.
Advantages of Intramedullary Fibula Nailing:
- Minimally Invasive: Smaller incisions, less soft tissue stripping, and reduced periosteal damage compared to open plating.
- Load Sharing: Promotes physiological loading and bone healing, potentially reducing stress shielding.
- Reduced Infection Risk: Smaller incisions and less soft tissue exposure.
- Improved Cosmesis: Smaller, less conspicuous scars.
- Early Mobilization: The robust fixation often allows for earlier weight-bearing and rehabilitation.
- Reduced Hardware Prominence: The nail is entirely contained within the bone, reducing palpability and irritation compared to plates, which can be prominent, especially in the subcutaneous fibula.
4. Risks, Side Effects, or Contraindications
While highly effective, the use of an Intramedullary Fibula Nail is not without potential risks, side effects, or contraindications.
Potential Risks and Side Effects:
- Infection: As with any surgical procedure involving implants, there is a risk of superficial or deep infection.
- Malunion or Nonunion: Despite stable fixation, biological factors can lead to incomplete healing or healing in an unfavorable position.
- Hardware Failure: Breakage of the nail or locking screws, though rare with modern implants, can occur due to excessive stress or delayed union.
- Nerve or Vascular Injury: Risk of damage to superficial peroneal nerve, sural nerve, or associated vessels during incision, entry point creation, or screw placement.
- Pain: Persistent pain at the fracture site, entry point, or due to hardware prominence.
- Prominent Hardware: While less common than with plates, the nail's entry point or distal locking screws can sometimes be palpable or cause irritation, necessitating removal.
- Syndesmotic Over-compression/Distraction: Incorrect reduction of the syndesmosis during fixation can lead to long-term pain and functional impairment.
- Iatrogenic Fracture: Creation of new fractures during entry point creation, reaming, or nail insertion.
- Complex Regional Pain Syndrome (CRPS): A rare but severe complication characterized by chronic pain, swelling, and trophic changes.
- Ankle Stiffness: Can result from prolonged immobilization or inadequate rehabilitation.
Contraindications:
- Active Local Infection: Presence of an active infection in the surgical field.
- Severe Comminution: Extensive comminution of the fibula, especially the distal fragment, which may preclude adequate purchase of locking screws.
- Extremely Narrow Medullary Canal: If the fibular canal is too narrow to accommodate even the smallest available nail, or if significant reaming would risk iatrogenic fracture.
- Severe Osteoporosis: While nails can be advantageous in osteoporosis, extreme cases may not provide sufficient bone quality for screw purchase.
- Severe Peripheral Vascular Disease or Neuropathy: Conditions that compromise healing or sensation, increasing complication risk.
- Patient Non-compliance: Unwillingness or inability to follow post-operative instructions, including weight-bearing restrictions and rehabilitation protocols.
- Open Fractures with Gross Contamination: While some open fractures can be nailed, those with severe contamination may require initial debridement and external fixation before definitive internal fixation.
- Ankle Fractures Not Involving the Fibula: Clearly, if the fibula is intact and stable, this implant is not indicated.
5. Maintenance/Sterilization Protocols for Associated Instrumentation
The Intramedullary Fibula Nail itself is a single-use, sterile implant. It arrives pre-sterilized and packaged, requiring no further processing before implantation. However, the associated surgical instrumentation used for its insertion requires rigorous maintenance and sterilization protocols to ensure patient safety and implant longevity.
Pre-operative Checks for Sterile Implants:
- Packaging Integrity: Always inspect the sterile barrier system (packaging) for any signs of damage, punctures, or breaches. Do not use if compromised.
- Expiration Date: Verify the expiration date. Expired implants must not be used.
- Product Identification: Confirm the correct implant (type, size, and side) matches the surgical plan.
- Visual Inspection: If packaging allows, visually inspect the implant for any defects, though opening sterile packaging should only occur in the sterile field.
Sterilization Protocols for Reusable Instrumentation:
The instruments used to implant the fibula nail (e.g., targeting jigs, guidewires, reamers, drills, screwdrivers, awls) are reusable and require meticulous processing.
- Point-of-Use Cleaning: Immediately after use, instruments should be wiped clean of gross contamination (blood, tissue) and kept moist (e.g., with enzymatic spray or damp towel) to prevent drying of bioburden.
- Decontamination (Manual or Automated):
- Manual Cleaning: Instruments are thoroughly scrubbed with a neutral pH enzymatic detergent, paying close attention to crevices, lumens, and hinged areas. Brushes appropriate for lumens and fine instruments must be used.
- Automated Cleaning: Ultrasonic cleaners or automated washer-disinfectors are often used for high-volume processing, followed by thorough rinsing.
- Inspection: After cleaning, instruments are meticulously inspected for cleanliness, damage (e.g., bent tips, dull edges, cracks, corrosion), and functionality. Any damaged instruments should be removed from service.
- Assembly and Packaging: Instruments are assembled into sets according to manufacturer guidelines. They are then placed in appropriate sterilization wrap, rigid containers, or pouches, ensuring proper presentation for sterilization and maintaining sterility until use.
- Sterilization:
- Steam Sterilization (Autoclaving): This is the most common and preferred method. Instruments are exposed to saturated steam under pressure for a specified time and temperature (e.g., 121°C for 20-30 minutes or 132°C for 4-10 minutes, depending on the cycle type and load).
- Low-Temperature Sterilization: For heat-sensitive instruments, methods like hydrogen peroxide gas plasma or ethylene oxide (EtO) may be used, following strict guidelines.
- Storage: Sterilized instruments are stored in a clean, dry, and temperature-controlled environment, protected from dust, moisture, and physical damage, until needed for surgery.
- Traceability: All sterilization cycles, instrument sets, and implants must be meticulously documented, including lot numbers, sterilization dates, and patient identifiers, for traceability and recall purposes.
Adherence to these stringent protocols is non-negotiable for patient safety and to prevent surgical site infections.
6. Patient Outcome Improvements
The adoption of the Intramedullary Fibula Nail has significantly enhanced patient outcomes for specific fibular fractures, contributing to faster recovery and improved long-term function.
- Reduced Surgical Trauma: Smaller incisions and less soft tissue dissection lead to less post-operative pain, swelling, and tissue damage, facilitating earlier rehabilitation.
- Accelerated Rehabilitation: The inherent stability and load-sharing nature of the nail often permit earlier weight-bearing and initiation of physical therapy compared to traditional plating, which may require longer periods of non-weight-bearing. This translates to faster return to activities of daily living and work.
- Improved Functional Outcomes: Studies consistently show that patients treated with intramedullary fibula nails experience comparable or superior functional outcomes, including ankle range of motion, strength, and pain scores, compared to plate fixation, particularly for distal fibula fractures.
- Lower Complication Rates: While complications can occur, the minimally invasive nature of nailing can lead to lower rates of wound healing issues, infection, and hardware prominence compared to open plating, especially in patients with compromised soft tissues or comorbidities.
- Enhanced Cosmesis: The smaller incisions result in less noticeable scarring, which can be a significant psychological benefit for patients.
- Reduced Hardware-Related Symptoms: Being entirely internal, the nail is less likely to cause irritation or pain from prominent hardware, reducing the need for subsequent hardware removal surgery.
By carefully selecting appropriate patients and adhering to meticulous surgical techniques, the Intramedullary Fibula Nail stands as a cornerstone in modern orthopedic trauma care for fibular fractures, delivering tangible improvements in patient recovery and quality of life.
7. Massive FAQ Section
Q1: What is an Intramedullary Fibula Nail?
A1: An Intramedullary Fibula Nail (IFN) is a specialized orthopedic implant, typically made of titanium, designed to be inserted into the hollow center (medullary canal) of the fibula bone. It provides internal support and stability for fractures, allowing the bone to heal while maintaining alignment.
Q2: Why is a fibula nail used instead of a plate for some fractures?
A2: Fibula nails offer several advantages over plates for certain fractures. They are minimally invasive, preserving soft tissues and blood supply, which can lead to faster healing and reduced infection risk. Nails are also load-sharing, distributing stress more physiologically, and are less prone to causing prominent hardware symptoms as they are entirely internal.
Q3: What types of fibula fractures can be treated with an Intramedullary Fibula Nail?
A3: IFNs are commonly used for spiral or oblique fractures of the distal fibula (often associated with ankle instability, such as Weber B or C type fractures), Maisonneuve fractures (proximal fibula fracture with syndesmotic injury), and sometimes for fibular shaft fractures or as part of complex pilon fracture management.
Q4: Is the surgery painful? What kind of anesthesia is used?
A4: The surgery is performed under anesthesia (general or regional, such as a spinal block) so you won't feel pain during the procedure. Post-operatively, pain is managed with medications. The minimally invasive nature of the surgery often results in less post-operative pain compared to more extensive open procedures.
Q5: How long is the recovery period after fibula nail surgery?
A5: Recovery varies depending on the fracture severity, individual healing capacity, and adherence to rehabilitation protocols. Generally, patients may begin partial weight-bearing within a few weeks, progressing to full weight-bearing over 6-12 weeks. Full recovery and return to strenuous activities can take 3-6 months or longer.
Q6: Will the fibula nail need to be removed?
A6: In many cases, the fibula nail is intended to be a permanent implant and does not necessarily need to be removed. However, removal may be considered if it causes irritation, pain, infection, or if hardware failure occurs. The decision for removal is made on a case-by-case basis by your surgeon.
Q7: Can I put weight on my leg immediately after fibula nail surgery?
A7: This depends on the specific fracture pattern, the stability of the fixation, and your surgeon's preference. Some patients may be allowed early protected weight-bearing, while others may require a period of non-weight-bearing. Always follow your surgeon's specific post-operative instructions.
Q8: What are the main risks associated with fibula nail surgery?
A8: Risks include infection, nonunion or malunion (failure to heal or healing in a poor position), nerve or blood vessel injury, hardware failure, persistent pain, and the need for future hardware removal. Your surgeon will discuss these risks thoroughly before the procedure.
Q9: How is an intramedullary fibula nail different from a "rod"?
A9: An "intramedullary rod" is a general term often used for larger nails inserted into major long bones like the tibia or femur. An "intramedullary fibula nail" is specifically designed for the fibula, typically smaller in diameter and tailored to the fibula's unique anatomy and biomechanical role, particularly in ankle stability. The principle of intramedullary fixation is the same.
Q10: What materials are Intramedullary Fibula Nails typically made from?
A10: Most modern Intramedullary Fibula Nails are made from biocompatible titanium alloys (e.g., Ti-6Al-4V). These materials offer an excellent balance of strength, flexibility, and corrosion resistance, and are well-tolerated by the body.
Q11: How long does the fibula nail stay in the bone if not removed?
A11: If not removed, the fibula nail remains permanently in the bone. It continues to provide support and stability, especially in the long term, and is designed to withstand the physiological stresses of daily life indefinitely.
Q12: Is physical therapy necessary after fibula nail surgery?
A12: Yes, physical therapy is almost always a crucial part of the recovery process. It helps restore range of motion, strengthen the muscles around the ankle and leg, improve balance, and facilitate a safe return to your pre-injury activity levels.