The Charnley Initial Retractor: A Comprehensive Guide to Precision in Orthopedic Surgery
1. Comprehensive Introduction & Overview
In the intricate world of orthopedic surgery, precision, stability, and an unobstructed view of the surgical field are paramount. Among the pantheon of instruments that empower surgeons to achieve these goals, the Charnley Initial Retractor stands as a testament to ingenious design and enduring utility. Named after Sir John Charnley, the pioneering British orthopedic surgeon often hailed as the "father of modern hip replacement," this self-retaining retractor revolutionized how complex joint surgeries, particularly total hip arthroplasty, are performed.
The Charnley Initial Retractor is not merely a tool; it's a critical component in ensuring the safety, efficiency, and success of major joint reconstruction procedures. Its primary function is to hold back soft tissues – muscles, skin, and fascia – away from the surgical site, providing the surgeon with a clear, stable, and hands-free view of the bone structures and joint capsule. This sustained retraction minimizes the need for an assistant to manually hold tissues, freeing up surgical team members and reducing potential fatigue-related errors. By maintaining consistent exposure, it allows for meticulous preparation of bone surfaces, accurate implant placement, and thorough debris removal, all of which are crucial for long-term implant success and optimal patient outcomes. This guide aims to demystify this essential instrument, offering patients and interested individuals a deep understanding of its design, application, and profound impact on modern orthopedic care. Please remember, this information is for educational purposes only and does not constitute medical advice.
2. Deep-dive into Technical Specifications / Mechanisms
The genius of the Charnley Initial Retractor lies in its elegant simplicity and robust engineering. It is a self-retaining system, meaning once positioned and secured, it maintains its retraction force without continuous manual input.
Design and Components:
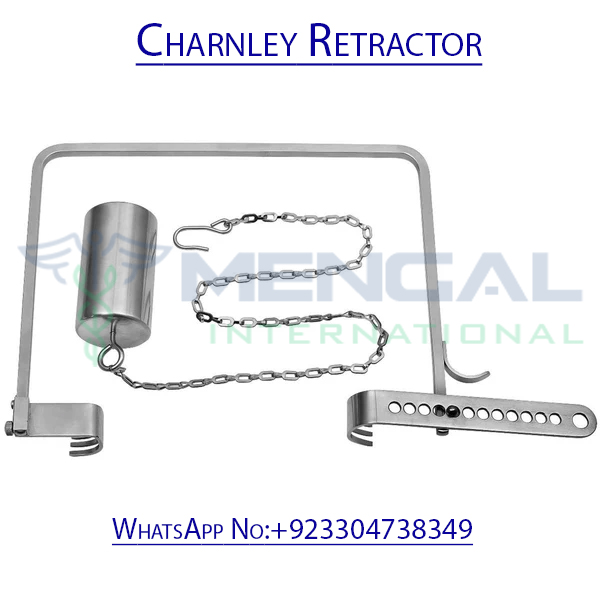
The retractor typically consists of several key parts:
* The Main Frame: This is the central, often U-shaped or rectangular, robust metal structure that provides the anchor for the retracting blades. It's designed to be strong enough to withstand significant tissue tension without deforming.
* Adjustable Clamps/Arms: These mechanisms slide along the main frame, allowing for variable width and angle adjustments to accommodate different patient anatomies and surgical approaches.
* Retractor Blades: These are the actual tissue-holding components. They come in various shapes and sizes to suit different anatomical structures and depths of retraction.
* Shapes: Straight, curved, angled, blunt, sharp (though initial retractors typically use blunt blades for broad tissue retraction).
* Sizes: Varying lengths and widths to reach different depths and retract differing amounts of tissue.
* Teeth/Serrations: Some blades may have gentle teeth or serrations to better grip superficial tissues without causing trauma.
Materials:
The Charnley Initial Retractor is manufactured from high-grade, surgical-quality stainless steel. This material choice is critical for several reasons:
* Biocompatibility: It is inert and does not react adversely with body tissues, preventing allergic reactions or rejection.
* Corrosion Resistance: It withstands repeated sterilization cycles (e.g., autoclaving) and exposure to bodily fluids without rusting or degrading.
* Strength and Durability: It must be strong enough to provide consistent retraction force without bending or breaking, ensuring long-term reliability in the operating room.
* Ease of Sterilization: Its smooth, non-porous surface facilitates thorough cleaning and sterilization, crucial for infection control.
Mechanism of Action:
The self-retaining mechanism operates on a simple yet effective principle of leverage and tension.
1. Placement: The surgeon carefully positions the main frame around the incision site.
2. Blade Attachment: Specific blades are selected and attached to the adjustable clamps on the frame.
3. Tissue Engagement: The blades are gently inserted beneath the soft tissues that need to be retracted.
4. Tensioning: The clamps are then adjusted, gradually spreading the blades apart. This creates controlled tension on the surrounding tissues, pulling them away from the central surgical field. The self-retaining feature means that once the desired tension is achieved, the clamps lock into place, holding the tissues steadily without continuous manual effort.
5. Biomechanics: The retractor distributes pressure over a broader area of tissue compared to manual retraction, potentially reducing localized trauma. Its stable hold allows for precise surgical maneuvers, which is vital for delicate procedures like acetabular reaming or femoral preparation during hip replacement.
3. Extensive Clinical Indications & Usage
The Charnley Initial Retractor is a workhorse in orthopedic surgery, primarily indicated for procedures requiring wide, stable, and prolonged exposure of deep anatomical structures.
Primary Clinical Applications:
- Total Hip Arthroplasty (THA): This is arguably the most common and significant application.
- Posterior Approach: The retractor is invaluable for retracting the gluteus maximus and other posterior soft tissues, providing an excellent view of the hip capsule, femoral neck, and acetabulum. This allows for safe dislocation of the femoral head, precise reaming of the acetabulum for cup placement, and meticulous preparation of the femoral canal.
- Lateral/Anterolateral Approaches: While less frequently used for initial retraction in some lateral approaches compared to posterior, it can still be adapted to retract muscles like the gluteus medius and minimus, optimizing exposure for acetabular preparation and femoral broaching.
- Complex Fracture Fixation around Major Joints: For fractures involving the acetabulum, proximal femur, or distal femur, the retractor can provide the necessary exposure to reduce fragments accurately and apply fixation hardware.
- Pelvic Trauma Surgery: In cases of severe pelvic fractures, precise exposure of bony landmarks and vascular structures is critical, where the Charnley can be instrumental.
- Other Major Joint Reconstructions: While less common than in THA, modified versions or principles of the Charnley retractor can be applied in certain complex knee or shoulder reconstructions where extensive, stable soft tissue retraction is needed.
Fitting and Usage Instructions (General Principles for Surgical Teams):
The precise application of the Charnley Initial Retractor is a skill honed through experience and meticulous attention to anatomical detail.
1. Incision and Initial Dissection: After the surgical incision is made and superficial layers are dissected, the surgeon identifies the planes for retraction.
2. Frame Placement: The main frame of the Charnley retractor is carefully positioned around the edges of the incision, ensuring it rests stably on bony prominences or robust soft tissue.
3. Blade Selection: The surgical team selects appropriate blades based on the depth of the surgical field, the type of tissue to be retracted, and the desired exposure. For instance, wider, blunter blades are often used for broad muscle retraction, while narrower blades might be used for specific capsular retraction.
4. Blade Insertion: Blades are gently inserted into the tissue planes, ensuring they are placed beneath the structures to be retracted without impinging on neurovascular bundles.
5. Progressive Tensioning: The adjustable clamps are then engaged, and the blades are slowly and incrementally spread apart. This allows for gradual tissue stretching, minimizing trauma. The surgeon continually assesses the tension and tissue viability.
6. Optimal Exposure: The goal is to achieve maximal, stable exposure of the target anatomical structures (e.g., acetabulum, femoral head) while minimizing pressure on surrounding vital structures.
7. Regular Assessment: Throughout the procedure, the surgical team periodically checks the retracted tissues for signs of excessive pressure, ischemia, or nerve impingement. Adjustments are made as needed.
8. Removal: Upon completion of the procedure, the tension is gradually released, and the blades are carefully removed to avoid sudden tissue recoil or damage.
4. Risks, Side Effects, or Contraindications
While the Charnley Initial Retractor is a cornerstone of safe and effective surgery, its use is not without potential risks if not handled with expert care. Understanding these is crucial for both the surgical team and patient education.
Potential Risks and Side Effects (Intraoperative and Postoperative):
- Nerve Damage: This is one of the most significant concerns. Excessive or prolonged pressure from the retractor blades on peripheral nerves (e.g., the sciatic nerve during posterior hip approaches) can lead to neuropraxia, paresthesia, or, in severe cases, permanent nerve damage. The surgeon must be acutely aware of nerve pathways and use appropriate padding and intermittent release of tension.
- Vascular Injury: While less common with blunt blades, improper placement or excessive force could theoretically compromise nearby blood vessels, leading to bleeding or ischemia.
- Soft Tissue Ischemia/Necrosis: Prolonged, high-pressure retraction can restrict blood flow to the retracted tissues, potentially leading to tissue damage, especially in patients with compromised vascularity. This underscores the need for careful and intermittent assessment of tissue viability.
- Muscle Damage: Over-stretching or crushing of muscle fibers can occur, contributing to postoperative pain, weakness, or delayed recovery.
- Bone Damage/Fracture: In patients with severe osteopenia or osteoporosis, aggressive retraction against bony prominences could theoretically lead to localized bone bruising or even fracture, though this is rare with proper technique.
- Instrument Malfunction: While rare due to robust design and regular maintenance, mechanical failure of the retractor (e.g., clamps slipping, blades bending) could occur, necessitating immediate replacement and potentially delaying the procedure.
Contraindications (Relative Considerations):
There are no absolute contraindications to the use of the Charnley Initial Retractor itself, as its application is highly dependent on surgical judgment and technique. However, certain patient factors and surgical scenarios warrant extra caution:
* Severe Osteoporosis: Patients with extremely brittle bones may be at higher risk for bone damage from retractor pressure. Meticulous technique and potentially alternative retraction methods are considered.
* Pre-existing Neurological Deficits: Patients with pre-existing nerve damage or neurological conditions may be more susceptible to iatrogenic nerve injury, requiring heightened vigilance.
* Extremely Obese Patients: While the retractor is designed for deep tissue retraction, in very obese patients, the sheer volume of tissue can make effective and safe retraction challenging, sometimes requiring specialized longer blades or alternative strategies.
* Anatomical Aberrations: Unusual anatomical variations might make standard retractor placement difficult or risky.
5. Expert Tips from Dr. Mohammed Hutaif
As an orthopedic specialist with extensive experience, Dr. Mohammed Hutaif emphasizes the critical role of the Charnley Initial Retractor in achieving superior surgical outcomes. His insights underscore the blend of technical proficiency and clinical judgment required for its optimal use:
- "Precision is Paramount, Patience is Key": "The Charnley retractor offers unparalleled precision in exposure, but it's not a tool to be rushed. Gradual, incremental retraction, allowing tissues time to stretch, is crucial. Never force the retraction; instead, allow the tissues to relax into position. This patience minimizes trauma and optimizes the surgical field."
- "Anatomical Awareness is Your Compass": "Before placing any blade, visualize the entire anatomical landscape – nerves, vessels, and bony landmarks. Always position blades in safe tissue planes, away from neurovascular structures. A thorough understanding of surgical anatomy is your best defense against complications."
- "Less Tension, More Often": "My philosophy is 'less tension, more often.' Rather than applying maximum tension once, I prefer to achieve adequate exposure with the minimum necessary tension, and then periodically check and potentially release tension for a few seconds if the procedure allows. This intermittent release helps maintain tissue perfusion and reduces the risk of ischemia or nerve compression."
- "Choose Your Blades Wisely": "The Charnley system offers a variety of blades. Selecting the right blade – considering its width, curve, and length – for the specific tissue and depth you're working with is crucial. A well-chosen blade distributes pressure effectively and optimizes exposure without undue stress."
- "The Charnley is an Extension of Your Hands, Not a Replacement": "While it provides hands-free retraction, the Charnley retractor requires constant monitoring. It's not a 'set it and forget it' tool. Continuously observe the retracted tissues for blanching, color changes, or any signs of undue pressure. Your vigilance directly translates to patient safety."
- "Maintain Your Instruments Meticulously": "A well-maintained instrument performs reliably. Ensure the retractor is regularly inspected for any signs of wear, damage, or stiffness in its mechanisms. Proper sterilization and care extend its lifespan and ensure its consistent function in critical moments."
- "Team Communication is Vital": "Effective use of the Charnley retractor is a team effort. The surgeon, first assistant, and scrub nurse must communicate clearly regarding blade placement, tension adjustments, and any concerns about tissue viability. This collaborative approach enhances safety and efficiency."
6. Massive FAQ Section
Q1: What is the main purpose of the Charnley Initial Retractor?
A1: The primary purpose of the Charnley Initial Retractor is to provide stable, hands-free, and wide exposure of the surgical site during complex orthopedic procedures, most notably total hip arthroplasty (hip replacement). By retracting soft tissues such as muscles and skin, it allows the surgeon an unobstructed view and working space to perform precise bone preparation and implant placement.
Q2: Who was Sir John Charnley, and why is this instrument named after him?
A2: Sir John Charnley (1911-1982) was a pioneering British orthopedic surgeon widely regarded as the "father of modern hip replacement." He developed many of the fundamental principles and techniques for total hip arthroplasty, including the low-friction arthroplasty concept. The Charnley Initial Retractor is named after him because it was an integral part of the surgical system he developed to achieve consistent and reproducible results in his revolutionary hip replacement surgeries.
Q3: What materials are Charnley retractors typically made from?
A3: Charnley retractors are typically manufactured from high-grade, surgical-quality stainless steel. This material is chosen for its excellent biocompatibility (it won't react with body tissues), corrosion resistance (withstanding repeated sterilization), exceptional strength, and durability, ensuring it can withstand the rigors of orthopedic surgery.
Q4: Is the Charnley Initial Retractor used in all joint surgeries?
A4: No, the Charnley Initial Retractor is not used in all joint surgeries. Its design is specifically optimized for procedures requiring deep, wide, and stable soft tissue retraction, particularly in total hip arthroplasty. While principles of its design might inspire other retractors, the "Charnley Initial" specifically refers to its application in major joint replacements, especially the hip.
Q5: How does the use of this retractor improve patient outcomes?
A5: The Charnley Initial Retractor improves patient outcomes by enabling surgeons to perform procedures with greater precision and efficiency. By providing a consistently clear and stable surgical field, it facilitates accurate bone cuts, meticulous implant positioning, and thorough removal of debris. This precision reduces the risk of complications, contributes to better long-term implant function, and can lead to faster recovery and reduced postoperative pain for the patient.
Q6: What are the potential risks associated with its use?
A6: While highly beneficial, potential risks include nerve damage (due to excessive or prolonged pressure on nerves like the sciatic nerve), vascular injury, soft tissue ischemia or necrosis from prolonged high-pressure retraction, and muscle damage. These risks are minimized through meticulous surgical technique, careful anatomical awareness, and intermittent assessment of the retracted tissues by the surgical team.
Q7: How is the Charnley Initial Retractor sterilized?
A7: Like all reusable surgical instruments, the Charnley Initial Retractor undergoes rigorous sterilization protocols. Typically, it is cleaned thoroughly to remove all organic matter, then sterilized using steam autoclaving (high-pressure saturated steam). This process ensures the complete elimination of all microorganisms, preventing surgical site infections.
Q8: Can patients feel the retractor during surgery?
A8: No, patients do not feel the retractor during surgery. All major orthopedic surgeries involving instruments like the Charnley Initial Retractor are performed under general anesthesia or regional anesthesia (e.g., spinal block), which ensures the patient is completely unconscious or numb to the surgical area.
Q9: Are there different types of Charnley retractors or variations?
A9: While the "Charnley Initial Retractor" refers to a specific design, there are variations in the types of blades that can be attached to the main frame. These blades come in different lengths, widths, and curvatures (e.g., straight, angled, curved, blunt, sharp) to accommodate various anatomical requirements and depths of retraction during a procedure.
Q10: How long has this instrument been in clinical use?
A10: The Charnley Initial Retractor, or variations based on its original design, has been in clinical use for many decades, dating back to the pioneering work of Sir John Charnley in the mid-20th century. Its enduring design and effectiveness have made it a staple in orthopedic operating rooms worldwide for over half a century.
Q11: What makes it "self-retaining"?
A11: The "self-retaining" feature means that once the blades are positioned and the desired tension is achieved, the retractor's clamps or locking mechanisms hold the blades firmly in place. This eliminates the need for a surgical assistant to manually hold tissues apart throughout the procedure, freeing up their hands for other tasks and providing a consistent, stable view for the surgeon.
Q12: Is the Charnley Initial Retractor reusable or disposable?
A12: The Charnley Initial Retractor is a robust, reusable surgical instrument. Made from high-grade stainless steel, it is designed to withstand countless sterilization cycles and years of use, provided it is properly maintained and inspected. This makes it a cost-effective and environmentally conscious choice for surgical facilities.