


The Pinnacle of Hip Arthroplasty: A Comprehensive Guide to Ceramic Femoral Heads (36mm, 32mm, 28mm)
1. Comprehensive Introduction & Overview
Total Hip Arthroplasty (THA), commonly known as total hip replacement, stands as one of the most successful surgical interventions in modern medicine, significantly improving the quality of life for millions suffering from debilitating hip conditions. At the heart of this intricate procedure lies the prosthetic implant, a critical component of which is the femoral head.
Ceramic femoral heads represent a significant advancement in orthopedic implant technology, offering superior wear resistance, biocompatibility, and long-term durability compared to earlier generations of implants. These precision-engineered components are designed to articulate smoothly within an acetabular liner (made of polyethylene or ceramic) to restore pain-free motion and stability to the hip joint.
This comprehensive guide delves into the world of ceramic femoral heads, specifically focusing on the widely used sizes of 36mm, 32mm, and 28mm. We will explore their sophisticated design, advanced materials, detailed clinical applications, critical biomechanical properties, and the profound impact they have on patient outcomes. As expert Medical SEO Copywriters and Orthopedic Specialists, our aim is to provide an authoritative resource for surgeons, medical professionals, and informed patients alike.
2. Deep-dive into Technical Specifications & Mechanisms
Design & Materials
The success of ceramic femoral heads is fundamentally rooted in their meticulous design and the advanced materials from which they are crafted.
Material Composition
Modern ceramic femoral heads are primarily manufactured from highly advanced ceramic composites, which offer an unparalleled combination of hardness, smoothness, and inertness.
- Alumina (Al2O3) Ceramics: Historically, alumina was one of the first ceramics used. It is extremely hard and resistant to scratching. First-generation alumina ceramics had limitations in fracture toughness, but advancements have led to more robust formulations.
- Zirconia (ZrO2) Ceramics: Zirconia offers higher fracture toughness than alumina, making it more resistant to catastrophic failure. However, zirconia can undergo a low-temperature degradation process (aging) that can reduce its mechanical properties over time, an issue largely mitigated by modern processing techniques.
- Zirconia-Toughened Alumina (ZTA) / Mixed-Matrix Ceramics (e.g., BIOLOX® delta): These are the current gold standard. BIOLOX® delta, for instance, is a composite material made of approximately 75% alumina, 25% zirconia, and trace amounts of strontium oxide and chromium oxide. This blend leverages the hardness of alumina with the fracture toughness and transformation toughening mechanism of zirconia, resulting in a material with:
- Exceptional Hardness: Minimizes wear against articulating surfaces.
- High Fracture Toughness: Significantly reduces the risk of catastrophic fracture compared to earlier ceramics.
- Excellent Biocompatibility: Non-toxic, non-allergenic, and highly inert within the biological environment, preventing adverse tissue reactions or ion release.
- Superb Surface Finish: Achieved through advanced polishing techniques, resulting in an incredibly smooth surface (Ra < 0.005 µm) that minimizes friction and wear.
Manufacturing Process
The production of ceramic femoral heads involves a highly controlled and sophisticated process:
- Powder Preparation: High-purity ceramic powders are precisely mixed.
- Forming: The powder is compacted into a 'green body' using techniques like isostatic pressing.
- Sintering: The green body is heated to extremely high temperatures (e.g., 1600-1700°C) in a controlled atmosphere. This fuses the ceramic particles, increasing density and strength.
- Machining & Polishing: The sintered ceramic is precision-machined to its final spherical geometry and then meticulously polished to an ultra-smooth finish, critical for optimal articulation and minimal wear.
- Quality Control: Each head undergoes rigorous inspection, including dimensional checks, surface roughness measurements, and non-destructive testing (e.g., dye penetrant, eddy current) to detect any micro-cracks or flaws.
Head Geometry
The femoral head is a perfectly spherical component designed to articulate within the acetabular cup. It features a precisely machined conical taper on its internal aspect, designed to mate securely with the corresponding taper on the femoral stem. This taper interface (e.g., 12/14 taper) ensures a strong, stable, and crevice-free connection.
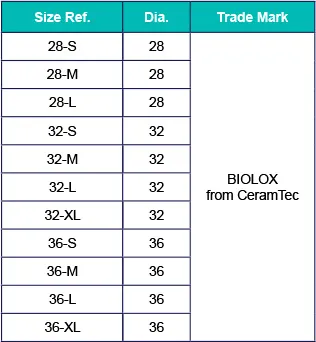
Sizes (36mm, 32mm, 28mm)
The selection of femoral head size is a critical surgical decision, balancing factors like joint stability, range of motion, and wear characteristics.
- 28mm Ceramic Femoral Head:
- Characteristics: Historically common, offers good wear performance, especially against ceramic liners.
- Considerations: Smaller head size can lead to a slightly higher risk of dislocation due to a shorter jump distance and potentially reduced impingement-free range of motion compared to larger heads.
- 32mm Ceramic Femoral Head:
- Characteristics: A popular choice, often considered a good balance between stability and wear. Provides improved jump distance and range of motion over 28mm.
- Considerations: Widely used across various patient demographics.
- 36mm Ceramic Femoral Head:
- Characteristics: Represents a trend towards larger head sizes. Offers significantly increased jump distance, leading to enhanced joint stability and a reduced risk of dislocation. Also permits a greater range of motion before impingement.
- Considerations: While larger heads historically had concerns about increased volumetric wear with polyethylene liners, this concern is largely mitigated when articulating against ceramic liners, which exhibit extremely low wear rates regardless of head size.
Biomechanics
The biomechanical advantages of ceramic femoral heads are paramount to their clinical success.
- Friction & Wear: Ceramic-on-ceramic (CoC) bearings exhibit the lowest coefficient of friction and the lowest wear rates among all bearing surfaces currently available for THA. This ultra-low wear is crucial for the long-term survival of the implant.
- Mechanism: The highly polished, hydrophilic ceramic surfaces attract a layer of synovial fluid, creating a fluid-film lubrication that minimizes direct surface contact and friction.
- Impact: Minimal wear debris generation significantly reduces the risk of osteolysis (bone loss due to inflammatory reaction to debris), a common cause of implant loosening and revision surgery with older bearing surfaces.
- Stress Distribution: The high modulus of elasticity and compressive strength of ceramics allow them to effectively handle the significant loads experienced by the hip joint during daily activities. The spherical design ensures even distribution of contact stresses.
- Range of Motion (ROM) & Stability: Larger femoral heads (e.g., 36mm) increase the "head-to-neck ratio," which describes the size of the head relative to the neck of the femoral component. A larger ratio means:
- Increased Jump Distance: The distance the head must travel out of the socket before dislocation occurs is greater, enhancing stability.
- Reduced Impingement: The larger head can articulate through a greater arc before the neck of the femoral stem contacts the rim of the acetabular cup, allowing for a wider, impingement-free range of motion.
- Biocompatibility: The inert nature of modern ceramics ensures minimal biological reaction. They do not release metallic ions, eliminating concerns about metal hypersensitivity or metallosis, which can be issues with metal-on-metal or metal-on-polyethylene bearings.
3. Extensive Clinical Indications & Usage
Ceramic femoral heads are a preferred choice for a broad spectrum of patients undergoing total hip arthroplasty, particularly those seeking long-term durability and optimal function.
Indications for Use
The primary indications for THA with ceramic femoral heads include:
- Osteoarthritis (OA): The most common reason, involving degenerative joint disease.
- Rheumatoid Arthritis (RA): An inflammatory autoimmune disease causing joint destruction.
- Avascular Necrosis (AVN): Death of bone tissue due to interruption of blood supply.
- Post-traumatic Arthritis: Arthritis developing after a hip injury or fracture.
- Developmental Dysplasia of the Hip (DDH): Congenital abnormality leading to hip instability.
- Ankylosing Spondylitis: A chronic inflammatory disease primarily affecting the spine and large joints.
- Failed Previous Hip Surgery: In some revision cases, ceramic bearings can be utilized, though careful consideration of existing implants and bone stock is necessary.
- Younger, Active Patients: Due to their superior wear characteristics and expected longevity, ceramics are highly beneficial for patients with a longer life expectancy or higher activity levels.
- Patients with Metal Allergies: Ceramic femoral heads offer an excellent solution for individuals with known sensitivities to nickel, cobalt, or chromium.
Detailed Surgical Applications (Total Hip Arthroplasty - THA)
The integration of ceramic femoral heads into THA follows a standardized, yet meticulously executed, surgical protocol.
Pre-operative Planning
- Patient Selection: A thorough evaluation of the patient's medical history, physical condition, and activity level.
- Radiographic Templating: X-rays are used with specialized templates to pre-operatively determine the optimal implant sizes (femoral stem, acetabular cup, and femoral head) to restore leg length, offset, and hip biomechanics. This helps in selecting the appropriate head diameter (28mm, 32mm, 36mm) to achieve desired stability and range of motion.
- Patient Education: Discussing the benefits and potential risks of ceramic bearings with the patient.
Intra-operative Procedure (Key Steps Related to Femoral Head)
- Surgical Approach: The surgeon selects an appropriate approach (e.g., posterior, anterolateral, direct anterior) to access the hip joint.
- Femoral Preparation: The femoral head is resected, and the femoral canal is reamed and broached to precisely fit the chosen femoral stem. The stem is then impacted into place.
- Acetabular Preparation: The acetabulum is reamed to a hemispherical shape, and the acetabular cup (and liner, if applicable) is implanted. For ceramic-on-ceramic bearings, a ceramic liner is used.
- Trial Reduction: A trial femoral head (of the chosen size, e.g., 32mm or 36mm) and trial liner are placed, and the hip is reduced. The surgeon then assesses joint stability, range of motion, leg length, and offset across a full range of motion. This is a critical step to confirm the final head size and ensure proper biomechanics.
- Final Implant Assembly:
- The sterile ceramic femoral head is carefully removed from its packaging.
- The taper on the femoral stem is meticulously cleaned and dried to ensure a perfect, debris-free interface.
- The ceramic femoral head is placed onto the stem taper.
- Impaction: The head is gently but firmly impacted onto the taper using a specialized impaction tool. This creates a cold weld, securing the head to the stem. Excessive force or repeated impaction should be avoided.
- The hip joint is then carefully reduced.
- Final Assessment: The surgeon re-evaluates stability, leg length, and range of motion to ensure optimal implant positioning and function.
Fitting/Usage Instructions (Surgeon's Perspective)
- Handle with Care: Ceramic heads are extremely hard but can be susceptible to brittle fracture if dropped or subjected to localized impact. Always handle with sterile gloves and avoid contact with non-sterile surfaces.
- Taper Cleaning: Before assembly, meticulously clean and dry both the internal taper of the ceramic head and the external taper of the femoral stem. Any blood, bone, tissue, or saline solution can compromise the taper lock, potentially leading to fretting corrosion or head disassociation.
- Proper Impaction: Use the manufacturer-recommended impaction tool. Apply a firm, axial force to seat the head securely. Avoid angular forces or "wobbling" the head during impaction. Listen for a distinct, solid sound indicating proper seating. Do not over-impact.
- Avoid Contamination: Ensure no debris, even microscopic, gets between the taper surfaces.
- Trial First: Always use trial components to confirm sizing and stability before committing to the final ceramic implant.
Patient Outcome Improvements
The adoption of ceramic femoral heads has profoundly improved patient outcomes in THA.
- Exceptional Longevity: The ultra-low wear rates of ceramic bearings translate to significantly extended implant survival, particularly crucial for younger, more active patients. This reduces the likelihood of needing revision surgery due to wear-related issues.
- Reduced Revision Rates: Lower incidence of osteolysis and aseptic loosening directly attributable to minimal wear debris.
- Superior Pain Relief: As with all successful THAs, ceramic bearings effectively eliminate pain caused by arthritis or injury.
- Improved Function & Mobility: The low friction and potential for larger head sizes allow for a greater, smoother range of motion, enabling patients to return to a wider array of activities.
- Reduced Risk of Osteolysis: The primary advantage, as ceramic debris is biologically inert and produced in minimal quantities, preventing the inflammatory cascade that leads to bone resorption.
- Elimination of Metal Allergy Concerns: Provides a safe and effective option for patients with known sensitivities to metallic implant components.
- Reduced Squeaking (Modern Ceramics): While historically a concern, advancements in ceramic materials and manufacturing have significantly reduced the incidence of audible squeaking, making it a rare occurrence for most patients.
4. Risks, Side Effects, or Contraindications
While ceramic femoral heads offer significant advantages, it is crucial to understand the potential risks, side effects, and contraindications associated with their use.
Potential Risks & Side Effects
- Ceramic Fracture: Although extremely rare with modern, advanced ceramic composites (like BIOLOX® delta), catastrophic fracture of a ceramic femoral head or liner is a known, albeit infrequent, complication. This can be caused by:
- Manufacturing Defects: Extremely rare due to stringent quality control.
- Intraoperative Trauma: Improper impaction, dropping the implant, or direct impact during surgery.
- Postoperative Trauma: High-energy trauma to the hip.
- Component Impingement: Repeated micro-impingement between the femoral neck and acetabular rim can generate stress leading to fracture.
- Suboptimal Taper Connection: Fretting corrosion or inadequate seating can weaken the head.
- Consequences: Fracture necessitates immediate revision surgery, which can be complex due to abrasive ceramic debris within the joint.
- Squeaking/Noise: A low incidence of audible squeaking or clicking can occur with ceramic-on-ceramic bearings. This phenomenon is often benign and not associated with implant failure, but it can be bothersome for some patients. Factors contributing to squeaking can include:
- Patient Anatomy: Certain gait patterns or soft tissue impingement.
- Implant Position: Extreme angles.
- Lubrication Issues: Transient lack of fluid film.
- Aseptic Loosening: Like any joint replacement component, the femoral stem or acetabular cup can loosen over time without infection. This is generally related to biological fixation, bone quality, or surgical technique, not directly the ceramic head material itself.
- Dislocation: While larger ceramic heads reduce this risk, dislocation can still occur due to patient activity, poor surgical technique, or implant malposition.
- Heterotopic Ossification (HO): The formation of new bone in soft tissues around the hip joint, which can restrict motion.
- Infection: A risk with any surgical procedure.
- Ceramic Debris: In the rare event of a ceramic fracture, the highly abrasive ceramic debris can cause significant damage to the surrounding soft tissues and bone, making revision surgery challenging.
Contraindications
- Active Infection: Absolute contraindication. Any active infection in the body, particularly around the hip, must be eradicated before THA.
- Skeletal Immaturity: In patients whose epiphyses have not yet fused, growth plates could be damaged.
- Significant Bone Loss: Insufficient bone stock in the femur or acetabulum to achieve stable fixation of the prosthetic components.
- Severe Muscular Atrophy or Neuromuscular Conditions: Patients unable to cooperate with postoperative rehabilitation may not achieve optimal outcomes.
- Known Hypersensitivity to Implant Materials: While rare for ceramics, this should always be considered.
- Previous Ceramic Fracture: A history of ceramic fracture in a prior joint replacement is a relative contraindication, requiring careful consideration and discussion with the patient due to the potential for re-fracture.
- Conditions Precluding Surgery: Any medical condition that makes the patient an unacceptably high surgical risk.
5. Maintenance/Sterilization Protocols
For medical facilities and surgical teams, adherence to strict maintenance and sterilization protocols is paramount to ensuring patient safety and optimal implant performance.
Handling & Storage
- Original Packaging: Ceramic femoral heads are typically supplied sterile and individually packaged. They must remain in their original, unopened, undamaged sterile packaging until immediately prior to implantation.
- Storage Environment: Store implants in a dry, clean, temperature-controlled environment, away from direct sunlight and sources of vibration or impact.
- Avoid Impact: Never drop or subject packaged or unpackaged ceramic heads to impact. Even seemingly minor impacts can create micro-cracks that compromise the integrity of the implant.
Sterilization
- Pre-Sterilized Implants: The vast majority of ceramic femoral heads are supplied by the manufacturer as sterile, single-use devices.
- Do NOT Re-sterilize: Single-use implants MUST NOT be re-sterilized or re-used. Re-sterilization can compromise the material properties, sterility, and structural integrity of the ceramic.
- Non-Sterile Implants (if applicable): In rare cases where a ceramic head might be supplied non-sterile (e.g., for specific research or custom applications, though highly unusual for standard implants), follow the manufacturer's validated sterilization instructions precisely. This typically involves steam sterilization (autoclaving) at specific temperatures, pressures, and durations. Always verify the validated method from the manufacturer's IFU (Instructions For Use).
Inspection
- Pre-Use Inspection: Before opening the sterile package, inspect the packaging for any signs of damage, punctures, or breaches that could compromise sterility.
- Visual Inspection: Once the package is opened in the sterile field, visually inspect the ceramic femoral head under good lighting for any flaws, cracks, chips, scratches, or surface imperfections. Even a microscopic flaw can be a stress riser and lead to catastrophic failure. If any defect is observed, the implant must be discarded and replaced.
- Confirm Size: Verify that the size (e.g., 36mm, 32mm, 28mm) and taper type match the surgical plan and the corresponding femoral stem.
Traceability
- Documentation: Maintain meticulous records of the implant's unique device identifier (UDI), lot number, serial number, and expiration date in the patient's medical record. This is crucial for product traceability in the event of a recall or adverse event reporting.
- Patient Sticker: Affix the provided patient sticker (containing implant details) to the patient's chart as per hospital protocol.
6. Frequently Asked Questions (FAQ)
Q1: What are ceramic femoral heads made of?
A1: Modern ceramic femoral heads are typically made from advanced ceramic composites, most commonly Zirconia-toughened alumina (ZTA), such as BIOLOX® delta. This material combines the extreme hardness of alumina with the enhanced fracture toughness of zirconia, resulting in a highly durable, wear-resistant, and biocompatible implant.
Q2: Why choose ceramic over metal or plastic (polyethylene) heads?
A2: Ceramic femoral heads offer superior advantages, primarily ultra-low wear rates and exceptional biocompatibility. Compared to metal-on-polyethylene, ceramic-on-ceramic bearings produce significantly less wear debris, reducing the risk of osteolysis and aseptic loosening. They also eliminate concerns about metal ion release and metal allergies, which can occur with metal implants.
Q3: What are the advantages of larger ceramic femoral heads (e.g., 36mm)?
A3: Larger ceramic femoral heads (like 36mm) significantly increase the "jump distance," which is the distance the head must travel to dislocate from the socket. This enhances hip joint stability and reduces the risk of dislocation. They also allow for a greater range of motion before impingement occurs between the femoral neck and the acetabular cup.
Q4: Can ceramic femoral heads break?
A4: While extremely rare with modern ceramic materials and manufacturing processes, catastrophic fracture of a ceramic femoral head or liner is a known, though infrequent, complication. Advances in ZTA composites have dramatically improved their fracture toughness, making them much more resistant to failure than earlier ceramic generations.
Q5: Is squeaking normal with ceramic implants?
A5: A low incidence of audible squeaking or clicking can occur with ceramic-on-ceramic bearings. While often benign and not indicative of implant failure, it can be bothersome for some patients. The exact cause is not fully understood but may relate to specific patient anatomy, implant positioning, or transient lubrication issues. Modern ceramics have significantly reduced the prevalence of this phenomenon.
Q6: Are ceramic heads safe for patients with metal allergies?
A6: Yes, ceramic femoral heads are an excellent choice for patients with known sensitivities or allergies to metals like nickel, cobalt, or chromium. Ceramics are biologically inert and do not release metal ions, thereby eliminating the risk of allergic reactions or metallosis associated with metallic implants.
Q7: How long do ceramic femoral heads last?
A7: Ceramic femoral heads, especially when articulating against a ceramic liner (ceramic-on-ceramic), are known for their exceptional longevity. Due to their ultra-low wear rates and minimal debris generation, they are designed to last for decades, often exceeding 20-30 years in many patients, making them a preferred choice for younger and more active individuals.
Q8: What is the typical recovery time after a hip replacement with a ceramic head?
A8: The recovery time for a total hip replacement with a ceramic head is similar to other THA procedures, typically involving several weeks to months. Most patients can bear weight immediately or soon after surgery, with full recovery of strength and mobility often taking 3 to 6 months. Physical therapy is crucial for optimal outcomes.
Q9: Can ceramic implants be used in revision surgery?
A9: Yes, ceramic components can be used in revision total hip arthroplasty, but the decision requires careful consideration. If there is significant ceramic debris from a previous ceramic fracture, it must be meticulously removed, as remaining abrasive particles can damage new implants. The existing components and bone quality must also be suitable for ceramic bearing surfaces.
Q10: What is the difference between 28mm, 32mm, and 36mm ceramic heads?
A10: These numbers refer to the diameter of the femoral head.
* 28mm: Smaller, traditionally used, good wear, but potentially lower stability.
* 32mm: A common intermediate size, balancing stability and range of motion.
* 36mm: Larger, offering significantly increased stability and greater range of motion, often preferred for active patients to reduce dislocation risk. The choice depends on individual patient anatomy and surgical goals.
Q11: Are there any activities I should avoid with a ceramic hip replacement?
A11: While modern hip replacements allow for a wide range of activities, high-impact sports (like running, jumping, contact sports) are generally discouraged to protect the implant from excessive stress and potential wear or loosening over many years. Low-impact activities such as walking, swimming, cycling, and golf are highly recommended.
Q12: How are these heads sterilized for surgery?
A12: Ceramic femoral heads are typically supplied by the manufacturer as sterile, single-use devices. They undergo a validated sterilization process (e.g., gamma irradiation or electron beam sterilization) and are packaged in sterile barriers. Surgical teams must ensure the sterile packaging is intact before opening it in the operating room. Re-sterilization of single-use implants is strictly prohibited.