The Definitive Guide to Cannulated Cancellous Screws: 4.0mm, 6.5mm, and 7.3mm
Comprehensive Introduction & Overview
In the dynamic field of orthopedic surgery, the precision and efficacy of fixation devices are paramount to achieving optimal patient outcomes. Among the most versatile and widely utilized implants are Cannulated Cancellous Screws. These specialized screws are engineered to provide stable fixation in cancellous (spongy) bone, which is characterized by its high porosity and excellent capacity for osteointegration. The cannulated design represents a significant advancement, allowing for minimally invasive, highly accurate screw placement over a guide wire, thereby enhancing surgical efficiency and reducing operative trauma.
This comprehensive guide will delve into the intricacies of Cannulated Cancellous Screws, specifically focusing on the most common diameters: 4.0mm, 6.5mm, and 7.3mm. Each size is meticulously designed for distinct clinical applications, ranging from delicate hand and foot fractures to robust fixation in the hip and knee. We will explore their advanced design and material science, detailed surgical applications, biomechanical principles, stringent maintenance and sterilization protocols, and ultimately, their profound impact on improving patient recovery and long-term functional stability. This resource aims to serve as an authoritative reference for orthopedic surgeons, residents, and medical professionals seeking to deepen their understanding of these critical orthopedic instruments.
Deep-Dive into Technical Specifications & Mechanisms
The effectiveness of cannulated cancellous screws lies in their sophisticated engineering and the biomechanical principles they leverage. Understanding these technical aspects is crucial for appropriate selection and application.
Design Features
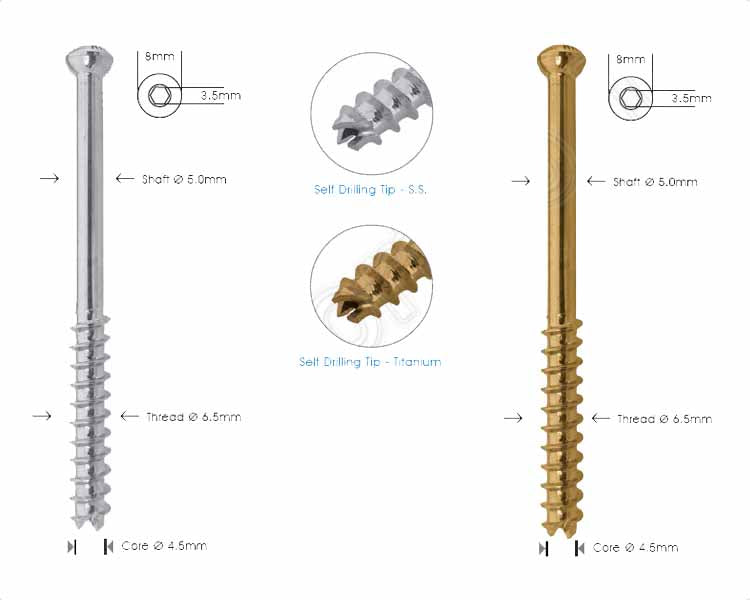
Cannulated cancellous screws are a marvel of orthopedic engineering, incorporating several key features that differentiate them from conventional solid screws:
- Cannulation: This is the defining feature. A hollow central lumen runs through the entire length of the screw, allowing it to be threaded over a pre-placed guide wire.
- Benefit: Enables precise placement, reduces the need for large incisions, minimizes soft tissue disruption, and facilitates accurate reduction of bone fragments under fluoroscopic guidance.
- Thread Design: Optimized for cancellous bone, which is softer and less dense than cortical bone.
- Deep, Wide Threads: Provide maximum purchase in spongy bone, distributing load over a larger surface area.
- Self-Tapping Flutes: Many designs incorporate self-tapping tips, eliminating the need for pre-drilling the screw hole, thereby simplifying the surgical procedure and reducing surgical time.
- Partial vs. Fully Threaded:
- Partially Threaded Screws: Crucial for achieving interfragmentary compression (lag screw principle). The unthreaded portion allows the screw head to pull the bone fragment closer to the main bone, compressing the fracture site.
- Fully Threaded Screws: Primarily used for neutralization or holding fragments in a reduced position without compression, or when compression is achieved by other means. They are also used when the screw crosses a joint line, preventing compression across the joint.
- Head Design:
- Low Profile: Minimizes soft tissue irritation and prominence, which can be a common complaint post-surgery.
- Driver Interface: Typically a hexagonal or star-shaped recess, ensuring secure engagement with the screwdriver and preventing stripping during insertion.
- Tip Design: Often features a blunt, rounded, or tapered tip to facilitate smooth insertion over the guide wire and prevent damage to surrounding tissues.
Materials
The choice of material for orthopedic implants is critical, balancing strength, biocompatibility, and resistance to corrosion.
- Titanium Alloy (Ti-6Al-4V): The gold standard for many orthopedic implants.
- Biocompatibility: Excellent tissue acceptance, minimizing adverse reactions.
- Strength-to-Weight Ratio: High strength, yet relatively light.
- Corrosion Resistance: Highly resistant to corrosion in the physiological environment.
- MRI Compatibility: Generally considered safe for MRI, although some local artifacting may occur.
- Stainless Steel (316L): Another common material, particularly for cost-effective solutions.
- Strength: Good mechanical strength.
- Corrosion Resistance: Adequate, but generally less resistant than titanium in the long term.
- Biocompatibility: Well-established, but some patients may have nickel sensitivity.
- MRI Compatibility: Can cause more significant artifacting compared to titanium.
Diameters and Their Specificity
The availability of different diameters is fundamental to addressing the diverse anatomical and fracture patterns encountered in orthopedics.
- 4.0mm Cannulated Cancellous Screw:
- Primary Use: Smaller bone fragments, areas with limited bone stock, or pediatric applications.
- Characteristics: Finer threads, smaller core diameter.
- Applications: Hand (scaphoid, metacarpals, phalanges), foot (metatarsals, phalanges), distal radius, radial head, pediatric fractures.
- 6.5mm Cannulated Cancellous Screw:
- Primary Use: Medium to large bone fragments, areas requiring moderate to strong fixation.
- Characteristics: Robust threads, larger core diameter for increased strength.
- Applications: Tibial plateau, distal femur, humeral head, ankle fractures (medial/lateral malleolus, pilon), calcaneus, talus.
- 7.3mm Cannulated Cancellous Screw:
- Primary Use: Large bone fragments, areas requiring maximum fixation strength and compression, especially in large joints.
- Characteristics: Heaviest threads, largest core diameter, providing superior purchase and resistance to pullout.
- Applications: Femoral neck fractures, intertrochanteric fractures (often in conjunction with plates), sacral fractures, acetabular fractures, SI joint fusion, large fragments of the tibial plateau or distal femur.
Biomechanics and Mechanism of Action
The biomechanical principles behind cannulated cancellous screws are critical for achieving stable fixation:
- Lag Screw Principle (Interfragmentary Compression): This is the most common application of partially threaded cancellous screws.
- A guide wire is placed across the fracture.
- A glide hole (oversized drill hole) is created in the near cortex/fragment, allowing the unthreaded portion of the screw to pass freely.
- A thread hole (undersized drill hole) is created in the far cortex/fragment.
- As the partially threaded screw is inserted, the threads engage only the far fragment. As the screw head contacts the near fragment, it pulls the two fragments together, generating powerful interfragmentary compression. This compression enhances stability, promotes healing by reducing micromotion, and can convert tensile forces into compressive forces across the fracture.
- Neutralization: Fully threaded screws, or partially threaded screws used without a glide hole, can act as neutralization screws, holding fragments in alignment after reduction, preventing shear, bending, or torsional forces from displacing the fracture.
- Load Sharing: The screw, while providing fixation, also allows the bone to bear some of the physiological loads, which is crucial for stimulating bone healing and preventing stress shielding.
- Primary vs. Secondary Stability:
- Primary Stability: Achieved immediately post-surgery through rigid fixation, often via compression.
- Secondary Stability: Achieved over time as bone healing progresses and the screw integrates with the surrounding bone (osteointegration).
Extensive Clinical Indications & Usage
Cannulated cancellous screws are indispensable tools in orthopedic trauma and reconstructive surgery. Their versatility allows for application across a wide spectrum of anatomical sites and fracture patterns.
General Principles of Usage
Regardless of the specific application, several core principles guide the use of cannulated cancellous screws:
- Aseptic Technique: Strict adherence to sterile procedures to prevent surgical site infection.
- Precise Reduction: Accurate anatomical reduction of bone fragments is paramount for optimal healing and functional outcome.
- Fluoroscopic Guidance: Intraoperative imaging (C-arm fluoroscopy) is essential for confirming guide wire placement, screw trajectory, and final screw position, especially with cannulated systems.
- Appropriate Screw Length and Diameter Selection: Tailoring the screw to the specific fracture pattern, bone quality, and anatomical location is critical.
- Bone Quality Assessment: The quality of cancellous bone (e.g., in osteoporotic patients) significantly impacts screw purchase and holding power. Adjunctive fixation or alternative strategies may be necessary in poor bone.
Specific Clinical Applications by Diameter
4.0mm Cannulated Cancellous Screws
These smaller screws are ideal for delicate bones and smaller fragments where precise, controlled fixation is required.
- Hand & Wrist:
- Scaphoid Fractures: A primary indication, offering excellent compression and stability for this notoriously difficult-to-heal bone.
- Metacarpal and Phalangeal Fractures: Especially intra-articular fractures requiring precise reduction.
- Distal Radius Fractures: Particularly for fixation of small fragments or volar rim fractures.
- Foot & Ankle:
- Metatarsal and Phalangeal Fractures: Similar to hand fractures, providing stable fixation in small bones.
- Malleolar Fractures: For fixation of small, displaced fragments or in conjunction with larger screws/plates.
- Calcaneal Avulsion Fractures: Fixation of small posterior avulsion fragments.
- Elbow:
- Radial Head Fractures: For specific fracture patterns amenable to screw fixation.
- Pediatric Orthopedics:
- Fixation of physeal-sparing fractures in various locations, where minimal disruption to growth plates is crucial.
6.5mm Cannulated Cancellous Screws
These intermediate-sized screws provide robust fixation for larger bone fragments and areas of moderate to good cancellous bone stock.
- Knee:
- Tibial Plateau Fractures: Especially Schatzker Type I, II, III fractures, providing strong subchondral support and interfragmentary compression.
- Distal Femoral Fractures: Supracondylar and intercondylar fractures, often used in conjunction with plates.
- Ankle:
- Bimalleolar and Trimalleolar Fractures: Fixation of medial malleolus, posterior malleolus, and sometimes lateral malleolus.
- Pilon Fractures: For fixation of specific articular fragments.
- Hip & Pelvis:
- Femoral Head Fractures: For specific fracture patterns.
- Acetabular Fractures: Fixation of certain wall or column fragments.
- Shoulder & Humerus:
- Humeral Head Fractures: For specific patterns, especially those involving the greater or lesser tuberosity.
- Distal Humerus Fractures: For articular fragments.
- Calcaneus:
- Intra-articular calcaneal fractures, providing stable fixation of posterior facet fragments.
7.3mm Cannulated Cancellous Screws
These largest screws are reserved for areas requiring maximal strength, especially in load-bearing joints and large bone segments.
- Hip:
- Femoral Neck Fractures: A cornerstone for Garden Type I, II, and III fractures, providing strong interfragmentary compression and rotational stability. Often used in a triangular configuration (inverted triangle).
- Intertrochanteric Fractures: While often managed with intramedullary nails or dynamic hip screws, 7.3mm screws may be used for specific fragment fixation or as part of a supplementary construct.
- Knee:
- Tibial Plateau Fractures: For larger fragments, particularly in Type IV-VI fractures, providing robust support.
- Distal Femoral Fractures: For large condylar fragments, often with plate constructs.
- Pelvis & Sacrum:
- Sacral Fractures: For stabilization of sacral ala fractures or in sacroiliac joint disruption.
- Acetabular Fractures: For large articular fragments or columns, providing substantial compression.
- Spine:
- Sacroiliac Joint Fusion: For stabilization in cases of instability or degeneration.
Fitting/Usage Instructions (General Surgical Workflow)
- Patient Positioning and Anesthesia: Appropriate positioning to allow access and fluoroscopy.
- Incision and Exposure: Minimally invasive approach guided by fluoroscopy.
- Fracture Reduction: Manual or instrumented reduction of bone fragments under fluoroscopic visualization.
- Guide Wire Placement:
- A small incision is made.
- A sharp-tipped guide wire is inserted percutaneously or through a small open approach, carefully directed across the fracture site to achieve optimal trajectory and depth.
- Fluoroscopy is used to confirm accurate placement in multiple planes.
- Measurement: A depth gauge is used over the guide wire to determine the appropriate screw length.
- Cannulated Drilling (Optional/Specific Designs):
- Some systems require a cannulated drill bit to create a pilot hole over the guide wire, especially in denser cancellous bone or subchondral bone.
- For lag screw technique, a larger cannulated drill bit may be used to create the glide hole in the near cortex.
- Countersinking (Optional): A cannulated countersink may be used to recess the screw head below the bone surface, preventing soft tissue irritation.
- Screw Insertion:
- The selected cannulated screw is loaded onto the cannulated screwdriver.
- The screwdriver and screw are carefully advanced over the guide wire.
- The screw is gently rotated and advanced until it engages the far cortex (for partially threaded screws) or achieves desired purchase.
- Fluoroscopy is used to confirm final screw position and compression.
- Guide Wire Removal: Once the screw is fully seated and fixation is confirmed, the guide wire is carefully removed.
- Wound Closure: Standard sterile closure.
Maintenance & Sterilization Protocols (for Implants)
It is crucial to understand that Cannulated Cancellous Screws are single-use, sterile implants. They are not designed for maintenance or resterilization by the hospital. The protocols below pertain to their handling and storage before use.
- Sterilization by Manufacturer: These screws are sterilized by the manufacturer (typically via gamma irradiation or ethylene oxide) and supplied in sterile, individually sealed packages.
- Packaging Integrity: Before use, the sterile packaging must be inspected for any signs of damage, tears, or compromise. A compromised package means the implant is no longer sterile and must be discarded.
- Storage: Implants must be stored in a clean, dry environment, away from extreme temperatures and direct sunlight, as per the manufacturer's instructions.
- Expiration Date: Always check the expiration date on the package. Expired implants must not be used.
- Traceability: Each implant package typically includes unique identifiers (e.g., lot number, serial number) for traceability, which is critical for patient safety and recall procedures.
- Handling in OR: Once opened in the sterile field, the implant should be handled with sterile instruments only. Any implant dropped or contaminated must be discarded.
- Disposal: Unused or contaminated implants, as well as packaging materials, must be disposed of according to hospital protocols for medical waste.
Biomechanics & Patient Outcome Improvements
Biomechanics in Detail
The biomechanical efficacy of cannulated cancellous screws contributes directly to superior patient outcomes.
- Enhanced Stability: The deep threads in cancellous bone, combined with the lag screw effect (interfragmentary compression), provide high primary stability, resisting shear, bending, and torsional forces. This rigidity is critical in the early post-operative period.
- Reduced Micromotion: Stable fixation minimizes micromotion at the fracture site. Excessive micromotion can impede callus formation and lead to delayed union or non-union. By reducing this, screws promote optimal conditions for bone healing.
- Load Sharing vs. Load Bearing: While providing strong fixation, cancellous screws allow for a degree of load sharing with the bone, which is physiologically beneficial. Pure load-bearing implants (like some plates) can lead to stress shielding, where the bone becomes less dense due to reduced stress, potentially hindering long-term strength.
- Anatomical Reduction Maintenance: The precision afforded by cannulation ensures that the anatomical reduction achieved by the surgeon is maintained throughout the healing process, crucial for restoring joint congruence and preventing post-traumatic arthritis.
Patient Outcome Improvements
The adoption of cannulated cancellous screws has significantly elevated the standard of care in orthopedic surgery, leading to tangible benefits for patients:
- Faster Rehabilitation and Mobilization: Stable fixation allows for earlier weight-bearing and initiation of physical therapy, accelerating the return to daily activities and reducing the risk of complications associated with prolonged immobilization (e.g., muscle atrophy, joint stiffness, deep vein thrombosis).
- Reduced Pain: Stable fracture fixation minimizes painful micromotion and irritation, contributing to better pain management post-operatively.
- Minimally Invasive Surgery: The cannulated design often facilitates smaller incisions, leading to:
- Less soft tissue dissection and trauma.
- Reduced blood loss.
- Lower risk of infection.
- Smaller scars and improved cosmetic outcomes.
- Lower Incidence of Non-Union/Malunion: By providing optimal biomechanical conditions for healing (stable fixation, compression, anatomical reduction), these screws significantly reduce the rates of fractures failing to heal or healing in a deformed position.
- Improved Functional Recovery: The combination of anatomical reduction, stable fixation, and early mobilization leads to better restoration of pre-injury function, range of motion, and overall quality of life.
- Reduced Need for Revision Surgery: Robust primary fixation and improved healing rates decrease the likelihood of needing subsequent surgeries due to implant failure or complications.
Risks, Side Effects, or Contraindications
While highly effective, the use of cannulated cancellous screws is not without potential risks, side effects, or contraindications. A thorough understanding of these factors is essential for informed surgical decision-making and patient counseling.
Potential Risks and Side Effects
- Infection: As with any surgical procedure involving implants, there is a risk of superficial or deep surgical site infection, which may necessitate antibiotic treatment or implant removal.
- Nerve or Vascular Damage: During guide wire insertion or screw placement, especially in anatomically complex areas, there is a risk of iatrogenic injury to nerves or blood vessels.
- Screw Breakage or Loosening: Despite robust design, screws can break under excessive load or loosen over time, particularly in patients with poor bone quality or non-compliance with weight-bearing restrictions.
- Non-Union or Malunion: While these screws aim to prevent these complications, they can still occur if biological healing factors are compromised, or if fixation is insufficient.
- Implant Prominence/Irritation: Even low-profile screw heads can sometimes cause irritation to overlying soft tissues, necessitating subsequent removal.
- Loss of Reduction: Early weight-bearing or trauma can lead to displacement of the fracture fragments despite adequate screw fixation.
- Allergic Reaction: Though rare, patients can have an allergic reaction to the implant material (e.g., nickel in stainless steel).
- Guide Wire Complications: Breakage or migration of the guide wire can occur, requiring retrieval.
- Thermal Necrosis: Over-drilling or rapid screw insertion without adequate cooling can cause localized bone necrosis.
- Post-traumatic Arthritis: Especially in intra-articular fractures, even with perfect fixation, damage to articular cartilage can predispose to arthritis.
Contraindications
- Active Infection: The presence of an active infection at the surgical site is an absolute contraindication, as it significantly increases the risk of implant-related infection and osteomyelitis.
- Severe Osteoporosis / Insufficient Bone Quality: In cases of extremely poor bone quality, the screws may not achieve adequate purchase, leading to early loosening or pullout. Alternative fixation methods (e.g., cemented screws, augmentation with bone cement, or different plate constructs) may be necessary.
- Allergy to Implant Material: While rare, a documented allergy to titanium or stainless steel components would contraindicate the use of screws made from that material.
- Patient Non-Compliance: Patients who are unwilling or unable to adhere to post-operative weight-bearing restrictions or rehabilitation protocols may be poor candidates for fixation with cancellous screws, especially in load-bearing areas.
- Fracture Morphology Not Amenable to Screw Fixation: Certain highly comminuted fractures or those with significant bone loss may not be suitable for screw-only fixation and may require plate-and-screw constructs or alternative methods.
- Severe Comorbidities: Patients with severe medical comorbidities that preclude surgery or anesthesia may not be candidates.
Massive FAQ Section
Q1: What is a cannulated cancellous screw?
A1: A cannulated cancellous screw is a specialized orthopedic implant designed for fixing bone fractures, particularly in the softer, spongy cancellous bone. Its distinguishing feature is a hollow central channel (cannula) that allows it to be precisely inserted over a pre-placed guide wire, enhancing accuracy and minimizing surgical invasiveness.
Q2: Why are there different sizes like 4.0mm, 6.5mm, and 7.3mm?
A2: The different diameters (4.0mm, 6.5mm, 7.3mm) are crucial for matching the screw to the specific bone size, fracture pattern, and desired fixation strength.
* 4.0mm: Used for smaller bones (hand, foot) and delicate fragments.
* 6.5mm: Ideal for medium-sized bones and larger fragments (ankle, knee, elbow).
* 7.3mm: Provides maximum strength for large bones and major load-bearing areas (hip, pelvis, large knee fragments).
Q3: What material are these screws typically made from?
A3: Cannulated cancellous screws are predominantly made from biocompatible materials such as titanium alloy (Ti-6Al-4V) or 316L stainless steel. These materials offer excellent strength, corrosion resistance, and are well-tolerated by the human body.
Q4: How does cannulation improve surgical outcomes?
A4: Cannulation significantly improves surgical outcomes by:
1. Precision: Allows for highly accurate screw placement over a guide wire, confirmed with fluoroscopy.
2. Minimally Invasive: Reduces the need for large incisions and extensive soft tissue dissection.
3. Efficiency: Streamlines the surgical process, potentially reducing operative time.
4. Reduced Trauma: Less disruption to surrounding tissues, leading to potentially faster healing and less post-operative pain.
Q5: Are these screws removed after the bone has healed?
A5: Not always. Whether screws are removed depends on several factors:
* Patient Symptoms: If the implant causes pain, irritation, or functional issues.
* Location: Screws near joints or under thin skin are more likely to be symptomatic.
* Patient Preference: Some patients prefer removal.
* Surgeon's Discretion: Based on the specific case.
In many cases, if the screws are not causing problems, they can remain in place indefinitely.
Q6: What are the main benefits of using these screws for patients?
A6: Patients benefit from:
* Stable Fixation: Promotes optimal bone healing and reduces the risk of non-union.
* Faster Recovery: Allows for earlier mobilization and rehabilitation.
* Reduced Pain: Stable fractures cause less pain.
* Minimally Invasive: Smaller scars, less blood loss, and potentially lower infection rates.
* Improved Functional Outcomes: Better restoration of pre-injury function and range of motion.
Q7: Can these screws be used in all types of bones?
A7: Cannulated cancellous screws are specifically designed for cancellous (spongy) bone, which is found at the ends of long bones and in flat bones (e.g., hip, spine). While they can cross cortical bone, their primary purchase is in cancellous bone. They are generally not used as primary fixation in purely cortical bone, which requires different screw designs.
Q8: What is the difference between a fully threaded and partially threaded cancellous screw?
A8:
* Partially Threaded Screws: Have threads only on the distal portion. They are used to create compression across a fracture site (lag screw technique) by pulling bone fragments together.
* Fully Threaded Screws: Have threads along their entire length. They are used for neutralization or holding fragments in position without compression, or when the screw needs to bridge a joint space without compressing it.
Q9: How long does it take to recover after surgery with these screws?
A9: Recovery time varies significantly depending on the fracture's location and severity, the patient's overall health, and adherence to rehabilitation protocols. Generally, bone healing takes 6-12 weeks, but full functional recovery and return to strenuous activities can take 3-12 months or longer. Your surgeon and physical therapist will provide a personalized recovery plan.
Q10: How do surgeons ensure precise placement of these screws?
A10: Surgeons ensure precise placement primarily through:
* Guide Wire: The cannulated design allows the screw to follow a precisely positioned guide wire.
* Fluoroscopy (C-arm): Real-time X-ray imaging during surgery provides continuous visualization of the guide wire and screw placement in multiple planes.
* Anatomical Knowledge: Extensive understanding of bone anatomy and fracture patterns.
* Specialized Instruments: Use of depth gauges, drills, and drivers specifically designed for these screws.
Q11: What are the potential complications of using cannulated cancellous screws?
A11: While generally safe, potential complications include infection, nerve or blood vessel damage, screw loosening or breakage, non-union or malunion, implant irritation requiring removal, and guide wire complications. Your surgeon will discuss these risks with you.
Q12: Are these screws safe for MRI scans?
A12: Most modern cannulated cancellous screws made from titanium alloy are generally considered safe for MRI scans. However, they may cause some local image artifacting (distortion) in the immediate vicinity of the implant. Stainless steel screws may cause more significant artifacting. Always inform your radiologist and MRI technician about any metallic implants you have.