Chronic Mallet Finger Secondary Repair: Advanced Surgical Techniques
Key Takeaway
Chronic mallet finger deformities present a complex reconstructive challenge due to tendon attenuation and secondary joint contractures. Secondary repair techniques, such as Fowler’s central slip release and spiral oblique retinacular ligament (SORL) reconstruction, aim to restore the extensor mechanism's biomechanical balance. This guide details the indications, surgical steps, and postoperative protocols necessary to achieve optimal functional outcomes in delayed mallet finger presentations.
INTRODUCTION TO CHRONIC MALLET FINGER DEFORMITIES
The management of a chronic mallet finger—typically defined as a terminal extensor tendon disruption presenting more than four weeks post-injury—poses a significant reconstructive challenge to the orthopedic hand surgeon. Unlike acute injuries, which often respond favorably to strict immobilization, chronic lesions are characterized by tendon attenuation, scar tissue interposition, and secondary biomechanical imbalances across the digital joints.
When the terminal extensor tendon is lengthened or ruptured, the extensor mechanism's proximal pull is concentrated entirely on the central slip at the proximal interphalangeal (PIP) joint. Over time, this unopposed proximal migration leads to PIP joint hyperextension and secondary distal interphalangeal (DIP) joint flexion, culminating in a classic swan neck deformity.
Secondary repair techniques are indicated when conservative management fails, passive motion remains satisfactory, and arthritic changes in the distal joint are minimal to moderate. This masterclass details two primary reconstructive avenues: Fowler’s central slip release and the reconstruction of the oblique retinacular ligament (including lateral band transfer techniques).
BIOMECHANICS AND PATHOANATOMY
To successfully execute a secondary repair, the surgeon must possess an intimate understanding of the digital extensor mechanism. The extensor digitorum communis (EDC) trifurcates over the proximal phalanx. The central slip inserts into the base of the middle phalanx, extending the PIP joint. The lateral slips join with the intrinsic tendons (lumbricals and interossei) to form the conjoined lateral bands, which merge distally to form the terminal tendon inserting into the base of the distal phalanx.
In a chronic mallet finger:
1. Terminal Tendon Attenuation: The avulsed or lacerated terminal tendon heals with an elongated scar, resulting in an extensor lag at the DIP joint.
2. Central Slip Overload: The proximal retraction of the extensor mechanism concentrates force on the central slip.
3. Volar Plate Laxity: Chronic PIP hyperextension stretches the volar plate, leading to a reducible or fixed swan neck deformity.
💡 Clinical Pearl: The Tenodesis Test
Before committing to a surgical reconstruction, meticulously assess passive joint mobility. If the DIP joint cannot be passively extended to neutral, a joint contracture exists, and a simple tendon reconstruction will fail. In such cases, a preliminary or concurrent joint release (or arthrodesis) must be considered.
SURGICAL TECHNIQUE 1: FOWLER’S CENTRAL SLIP RELEASE
The Fowler procedure is an elegant, biomechanically sound operation designed to correct the imbalance of a chronic mallet finger. By releasing the central slip from its insertion on the middle phalanx, the entire extensor mechanism is allowed to displace proximally. This proximal shift increases tension on the distal end, effectively tightening the attenuated terminal tendon scar and restoring DIP joint extension.
Indications
- Chronic mallet finger with an extensor lag greater than 30 degrees.
- Flexible PIP and DIP joints (full passive range of motion).
- Absence of severe osteoarthritis in the DIP joint.
Patient Positioning and Anesthesia
The procedure is typically performed under regional anesthesia (e.g., axillary block) or Wide Awake Local Anesthesia No Tourniquet (WALANT). The WALANT technique is highly advantageous here, as it allows the surgeon to assess active tensioning and the correction of the extensor lag intraoperatively. The patient is positioned supine with the operative arm extended on a radiolucent hand table.
Step-by-Step Surgical Approach
1. Incision and Exposure
* Make a midlateral finger incision extending from just distal to the PIP joint to a point level with the middle of the proximal phalanx.
* Carefully dissect through the subcutaneous tissues, taking care to protect the neurovascular bundles located volar to the incision line (Cleland’s and Grayson’s ligaments may need to be partially divided).
* Open the deep tissues until the lateral edge of the lateral band of the extensor hood is clearly identified.
2. Elevation of the Extensor Mechanism
* Elevate the edge of the lateral band using a small skin hook.
* With the finger held in extension, continue elevating the extensor expansion dorsally until the deep surface of the central slip is exposed at its insertion into the base of the middle phalanx at the PIP joint.
* Elevate the entire extensor hood from the dorsal aspect of the proximal phalanx to ensure free proximal excursion.
3. Release of the Central Slip
* Using the precise point of a No. 11 Bard-Parker knife blade, begin on the deep surface of the central slip.
* Carefully free the insertion of the central slip from the proximal dorsal edge of the middle phalanx.
🚨 Surgical Warning: Joint Capsule Integrity
When releasing the central slip, exercise extreme caution to avoid breaching the underlying PIP joint capsule. A capsular tear can lead to postoperative adhesions, severe stiffness, or iatrogenic joint instability.
4. Biomechanical Tensioning
* Releasing the central slip allows the entire extensor mechanism to displace proximally.
* Observe the distal joint; the tension increases on the distal end and is transmitted to the avulsed terminal tendon. Because the tendon has become too long after healing to the distal phalanx by scar, this proximal shift restores the necessary tension to extend the DIP joint.
* If performed under WALANT, ask the patient to actively extend the digit to confirm the correction of the mallet lag and the absence of PIP hyperextension.
5. Closure
* Deflate the tourniquet (if used) and achieve meticulous hemostasis.
* Close the wound with interrupted 5-0 nylon sutures.
* Apply a sterile, non-adherent compressive dressing.
SURGICAL TECHNIQUE 2: TENDON TRANSFER AND GRAFTING (SORL RECONSTRUCTION)
When a chronic mallet finger is accompanied by a severe, hyperextension locking deformity at the PIP joint (swan neck deformity), a Fowler release alone may be insufficient. In these scenarios, reconstructing the oblique retinacular ligament (ORL) or performing a lateral band transfer is required to simultaneously tether the PIP joint in slight flexion and extend the DIP joint.
The Spiral Oblique Retinacular Ligament (SORL) Reconstruction
Successful treatment of posttraumatic mallet deformities has been widely reported using the SORL technique. This procedure utilizes a free tendon graft (commonly the palmaris longus) to recreate the tenodesis effect of the native ORL.
Graft Routing and Fixation:
1. Distal Attachment: The graft is secured to the dorsal base of the distal phalanx.
2. Routing: It is passed proximally along the anatomical path of the ORL.
3. Spiraling: The graft spirals volar to the flexor tendon sheath, passing carefully between the neurovascular bundle and the flexor sheath.
4. Proximal Fixation: It crosses to the opposite side of the proximal phalanx, volar to the PIP joint axis of rotation, and is secured to the base of the proximal phalanx through a drill hole using a pull-out technique or a modern suture anchor.
By passing volar to the PIP joint and dorsal to the DIP joint, tension on the graft simultaneously flexes the PIP and extends the DIP, directly counteracting the swan neck deformity.
Lateral Band Transfer Technique
An alternative to a free graft is the transfer of a single lateral band of the extensor mechanism. This technique corrects recurrent hyperextension and locking of the PIP joint while addressing the old mallet deformity, provided passive motion is satisfactory and arthritic changes are no worse than moderate.
Step 1: Exposure and Identification
Expose the extensor hood and the flexor tendon sheath through a curved dorsal or midlateral incision. Identify the lateral bands.
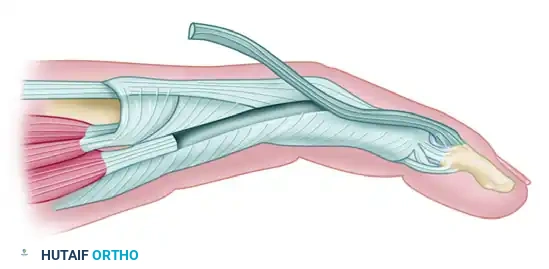
Figure A: Lateral view of the intact extensor hood and the underlying flexor tendon sheath prior to lateral band detachment.
Step 2: Proximal Detachment
Isolate one of the lateral bands (typically the ulnar lateral band to preserve radial-sided pinch biomechanics). Detach it proximally at the level of the proximal phalanx, leaving its distal insertion at the terminal tendon intact.
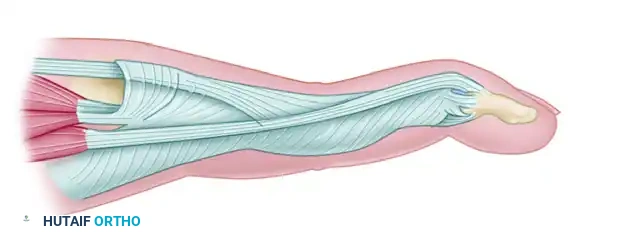
Figure B: One lateral band of the extensor hood has been detached proximally, preparing it for volar transposition.
Step 3: Creation of the Pulley and Suturing
Create a small, robust pulley in the flexor tendon sheath directly opposite the PIP joint. Thread the detached proximal end of the lateral band through this pulley. Suture the band back onto the extensor hood under carefully calibrated tension.
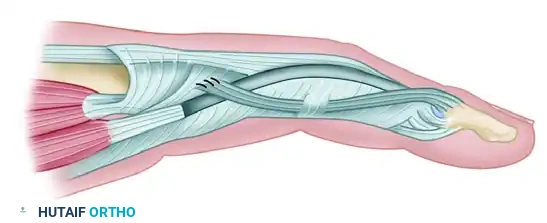
Figure C: The detached band has been threaded through the small pulley made in the flexor tendon sheath opposite the proximal interphalangeal joint and has been sutured to the hood.
💡 Clinical Pearl: Tensioning the Transfer
The transferred lateral band must be sutured under enough tension to create a slight flexion contracture of the PIP joint (approximately 10 to 15 degrees). This deliberate tethering prevents the PIP joint from snapping back into hyperextension locking, effectively curing the swan neck biomechanics.
POSTOPERATIVE CARE AND REHABILITATION PROTOCOL
The success of any secondary mallet finger repair is heavily dependent on strict adherence to a phased postoperative rehabilitation protocol. The reconstructed tissues require prolonged protection to heal at the correct length without stretching out.
Phase I: Maximum Protection (Weeks 0 to 3)
- Immobilization: Immediately postoperatively, the finger is protected with a custom thermoplastic splint.
- Positioning: The PIP joint is immobilized in no more than 30 degrees of flexion, and the DIP joint is held in strict, absolute extension.
- Rationale: Prevention of acute flexion of the PIP joint is critical; excessive flexion will tear the healing joint capsule and the newly released central slip, leading to catastrophic failure of the Fowler procedure.
- Wound Care: Sutures are removed at 10 to 14 days postoperatively. Pin site care (if a transarticular K-wire was used for temporary DIP fixation) is performed daily.
Phase II: Controlled Mobilization (Weeks 3 to 7)
- Splint Modification: At exactly 3 weeks, the initial splint is removed.
- DIP Isolation: A new, small metal or thermoplastic splint is applied exclusively to immobilize the DIP joint. The DIP joint must be held in continuous extension for 4 additional weeks.
- PIP/MCP Motion: With the DIP joint securely splinted, the patient is cleared to begin full active and passive range of motion of the PIP and metacarpophalangeal (MCP) joints. This differential gliding prevents extensor mechanism adhesions while protecting the terminal tendon healing zone.
Phase III: Weaning and Strengthening (Weeks 7 and Beyond)
- Splint Weaning: At 7 weeks postoperatively, the DIP splint is gradually weaned. It is initially removed during the day for light activities but must be worn at night for an additional 2 to 4 weeks to prevent nocturnal stretching of the repair.
- Therapy: Gentle active flexion of the DIP joint is initiated. Passive forced flexion is strictly contraindicated.
- Monitoring: The patient is monitored closely for any recurrence of the extensor lag. If a lag of more than 10 degrees develops, daytime splinting is immediately reinstituted.
COMPLICATIONS AND PITFALLS
Even in experienced hands, secondary repair of chronic mallet fingers carries a high complication profile. Surgeons must be prepared to manage the following:
- Recurrent Extensor Lag: The most common complication. Often due to inadequate tensioning during surgery, premature splint removal, or patient non-compliance. Management requires reinstitution of strict extension splinting.
- PIP Joint Stiffness: Over-tensioning of a SORL graft or excessive scar formation after a Fowler release can lead to a fixed PIP flexion contracture. Meticulous surgical technique and early PIP mobilization (while protecting the DIP) are preventative.
- Skin Necrosis: The dorsal skin over the DIP joint is exceptionally thin. Aggressive dissection or overly tight closure can lead to ischemia and necrosis, potentially exposing the tendon repair.
- Swan Neck Recurrence: If the volar plate laxity is not adequately addressed, or if the lateral band transfer stretches out, the hyperextension locking may recur.
CONCLUSION
The secondary repair of a chronic mallet finger demands a profound understanding of digital biomechanics. Whether employing the Fowler central slip release to shift the extensor mechanism proximally, or utilizing a lateral band transfer/SORL reconstruction to correct a concurrent swan neck deformity, precise surgical execution is paramount. By combining meticulous intraoperative tensioning with a rigid, phased postoperative rehabilitation protocol, the orthopedic surgeon can successfully restore functional biomechanical equilibrium to the chronically injured digit.
You Might Also Like