Anesthesia in Hand and Upper Extremity Surgery: A Masterclass
Key Takeaway
The judicious selection of anesthetic technique is a cornerstone of successful hand and upper extremity surgery. This comprehensive guide details the indications, pharmacology, and step-by-step administration of regional and general anesthesia. Designed for orthopedic surgeons, it emphasizes patient positioning, precise nerve block execution, and postoperative protocols to optimize surgical outcomes, ensure patient comfort, and facilitate early mobilization in complex upper limb reconstructions.
Introduction: The Critical Role of Anesthesia in Hand and Upper Extremity Surgery
The judicious selection and flawless execution of anesthetic techniques form the bedrock of successful hand and upper extremity surgery. Anesthesia in this highly specialized field extends far beyond mere pain control; it directly dictates surgical precision, intraoperative physiological stability, and the trajectory of postoperative rehabilitation. For the advanced orthopedic resident, fellow, or practicing consultant, a profound, nuanced understanding of available anesthetic modalities, their pharmacokinetic profiles, indications, contraindications, and potential complications is indispensable.
The primary objectives of anesthesia in upper extremity surgery are multifaceted and demanding:
* Absolute Analgesia: Ensuring the patient experiences zero nociceptive stimulus during intricate, often prolonged procedures.
* Surgical Field Immobility: Achieving a completely motionless operative field, which is an absolute prerequisite for microsurgical anastomoses, nerve repairs, and precise anatomical dissection.
* Patient Comfort and Dynamic Cooperation: Minimizing anxiety while, in specific techniques, allowing for intraoperative active movement to assess tendon glide, joint stability, or fracture reduction.
* Optimized Hemostasis: Utilizing regional techniques that induce sympathectomy, thereby improving peripheral perfusion while simultaneously allowing for prolonged, comfortable tourniquet times.
* Enhanced Recovery After Surgery (ERAS): Leveraging regional blocks to provide extended postoperative analgesia, drastically reducing reliance on systemic opioids and facilitating immediate postoperative mobilization.
The choice of anesthesia is a highly collaborative, multidisciplinary decision involving the orthopedic surgeon, the anesthesiologist, and the patient. It must be seamlessly integrated into the preoperative planning phase.
General Principles of Surgical Setup and Positioning
Regardless of the chosen anesthetic modality, meticulous patient positioning and surgical setup are paramount. The upper extremity must be positioned to allow 360-degree access to the surgical site while maintaining the patient's physiological stability, airway patency, and cervical spine neutrality.
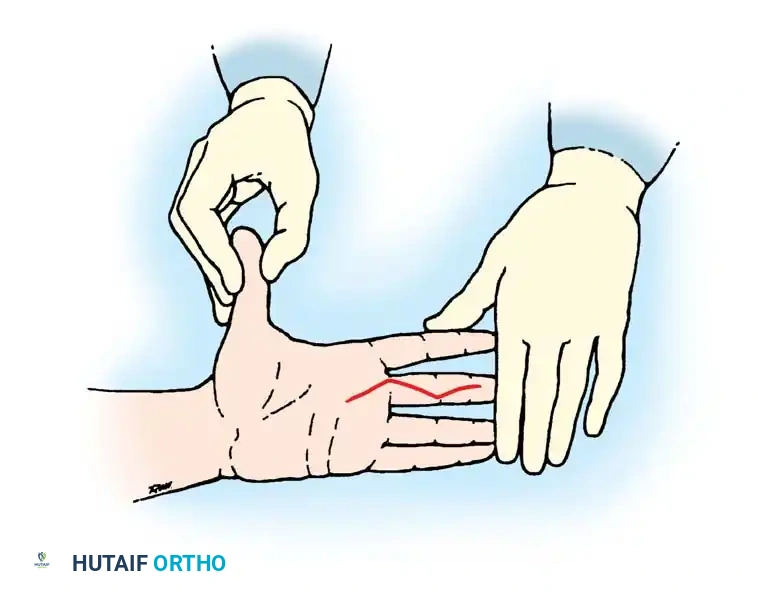
Clinical Pearl: For the vast majority of hand and wrist procedures, the patient is positioned supine with the operative arm abducted on a radiolucent hand table. Crucially, shoulder abduction must never exceed 90 degrees to prevent traction injuries to the brachial plexus. The assistant's role in stabilizing the hand is critical for maintaining a consistent surgical field, especially during intricate maneuvers like incision planning and flap elevation.
Fig. 61-3 Ideal position for the assistant to stabilize the patient’s hand as the surgeon makes a precise zigzag (Bruner) incision. Note the counter-tension applied to optimize skin turgor.
Basic surgical instrumentation for hand surgery is highly specialized, emphasizing fine motor control, magnification compatibility, and atraumatic tissue handling. The instruments must reflect the delicate nature of the anatomy.

Fig. 61-4 Basic instruments for any surgical procedure on the hand. An octagonal-shaped knife handle is preferable to a flat handle because the scalpel is most commonly held via a precision pinch in hand surgery. Instruments include the knife handle, small rat-tooth forceps, dissecting scissors, small hemostats, ruler, marking pencil, double-hook Lovejoy retractors, and a probe.
Local Anesthetic Agents: Pharmacology and Clinical Application
Local anesthetic agents achieve their effect by reversibly binding to the intracellular portion of voltage-gated sodium channels in nerve membranes. This blockade inhibits sodium influx, thereby preventing the depolarization necessary for the propagation of action potentials. The ideal agent possesses a rapid onset, predictable duration, minimal local tissue toxicity, and a high threshold for systemic toxicity.
Key Local Anesthetic Agents in Orthopedics
- Lidocaine (Xylocaine):
- Pharmacokinetics: An amide-type anesthetic with rapid onset (within 2-5 minutes) and intermediate duration of action (1-2 hours).
- Dosage: The recommended safe maximum dosage is 4.5 mg/kg (without epinephrine) up to 300 mg, or 7 mg/kg (with epinephrine) up to 500 mg in a healthy adult.
- Clinical Use: The workhorse for local infiltration, short-duration peripheral nerve blocks, and Intravenous Regional Anesthesia (IVRA).
- Mepivacaine (Carbocaine):
- Pharmacokinetics: Similar to lidocaine but with a slightly longer duration of action (1.5-3 hours) and less vasodilation, making it effective even without epinephrine.
- Dosage: Maximum dosage is 5 mg/kg (up to 400 mg).
- Clinical Use: Highly effective for peripheral nerve blocks where an intermediate duration is desired, particularly in patients where epinephrine is contraindicated.
- Bupivacaine (Marcaine):
- Pharmacokinetics: Highly lipid-soluble and protein-bound, resulting in a slower onset (10-20 minutes) but a significantly prolonged duration of action (up to 8-12 hours). It carries a higher risk of cardiotoxicity compared to lidocaine.
- Dosage: Maximum dosage is 2.5 mg/kg, not exceeding 175 mg (without epinephrine) or 225 mg (with epinephrine).
- Clinical Use: The agent of choice for major reconstructive procedures, replantations, and continuous catheter brachial plexus blocks where prolonged postoperative analgesia is critical.
- Ropivacaine (Naropin):
- Pharmacokinetics: A long-acting amide similar to bupivacaine but formulated as a pure S-enantiomer, which significantly reduces its cardiotoxic and neurotoxic profile.
- Clinical Use: Increasingly replacing bupivacaine for high-volume regional blocks due to its superior safety margin.
Surgical Warning: The traditional dogma dictating that epinephrine is absolutely contraindicated in digital blocks ("no epinephrine in fingers, toes, penis, or nose") has been heavily challenged by modern evidence. The advent of WALANT (Wide Awake Local Anesthesia No Tourniquet) has proven that 1% lidocaine with 1:100,000 epinephrine is safe for digital infiltration, provided the surgeon has phentolamine (an alpha-blocker) readily available for rescue reversal of vasospasm. However, in patients with severe peripheral vascular disease or scleroderma, traditional caution remains prudent.
Factors Influencing the Choice of Anesthesia
The selection of an anesthetic technique is a nuanced, multifactorial decision that balances patient safety, surgical requirements, and institutional logistics.
Patient-Specific Factors
- Age and Cognitive Status: Pediatric patients and adults with severe cognitive impairments typically require general anesthesia to ensure immobility.
- Cardiopulmonary Comorbidities: Patients with severe ischemic heart disease, congestive heart failure, or chronic obstructive pulmonary disease (COPD) benefit immensely from regional anesthesia, which avoids the myocardial depression and airway manipulation inherent to general anesthesia.
- Anticoagulation Status: The American Society of Regional Anesthesia and Pain Medicine (ASRA) guidelines must be strictly followed. Deep blocks (e.g., infraclavicular) carry a higher risk of non-compressible hematoma in anticoagulated patients compared to superficial blocks (e.g., axillary).
- Anatomical Challenges: Severe cervical spine arthritis, morbid obesity, or local infection at the injection site may preclude certain regional approaches.
Surgical Factors
- Procedure Duration: Brief procedures (e.g., trigger finger release) are ideal for local infiltration or WALANT. Prolonged microsurgery (e.g., free tissue transfer) necessitates long-acting regional blocks or general anesthesia.
- Intraoperative Assessment: Procedures such as tenolysis, tendon transfers, and complex capsulotomies are vastly improved when the patient is awake and can actively move their digits, allowing the surgeon to assess tension and glide in real-time.
General Anesthesia in Upper Extremity Surgery
General anesthesia induces a reversible state of unconsciousness, amnesia, analgesia, and muscle relaxation. While regional anesthesia is often preferred, general anesthesia remains indispensable in specific scenarios.
Indications
- Massive polytrauma or bilateral upper extremity injuries.
- Procedures requiring concomitant harvesting of distant autografts (e.g., fibula free flap, iliac crest bone graft).
- Absolute contraindications to regional anesthesia (e.g., patient refusal, severe coagulopathy, local infection).
- Surgeries exceeding the safe duration of tourniquet inflation or the temporal limits of regional blocks.
Disadvantages and Risks
- Systemic physiological stress, including fluctuations in blood pressure and cardiac output.
- Postoperative Nausea and Vomiting (PONV), which can be particularly detrimental if the patient requires immediate oral intake of vasodilators post-replantation.
- Absence of the sympathectomy-induced vasodilation provided by regional blocks, which is highly beneficial for flap survival.
Regional Anesthesia: The Gold Standard
Regional anesthesia involves the targeted blockade of nerve plexuses or peripheral nerves. It is widely considered the gold standard for upper extremity surgery due to its profound benefits.
Advantages of Regional Anesthesia
- Hemodynamic Stability: Avoids the profound vasodilation and cardiac depression associated with volatile anesthetics.
- Sympathectomy: Blocks vasoconstrictive sympathetic fibers, resulting in maximal vasodilation. This is critical for optimizing perfusion in replantations and microvascular free flaps.
- Superior Pain Control: Drastically reduces postoperative opioid consumption, mitigating opioid-related side effects such as respiratory depression, ileus, and PONV.
- Preemptive Analgesia: Blocking nociceptive pathways before the surgical incision prevents central sensitization and reduces the incidence of chronic regional pain syndrome (CRPS).
1. Brachial Plexus Blocks
Brachial plexus blocks provide comprehensive anesthesia to the upper extremity. The choice of approach depends on the surgical site.
a. Interscalene Block
- Target: Roots and trunks (C5-C7) between the anterior and middle scalene muscles.
- Indications: Ideal for shoulder, clavicle, and proximal humerus surgery.
- Pitfalls: Frequently spares the ulnar nerve (C8-T1). It carries a near 100% incidence of ipsilateral phrenic nerve blockade (hemidiaphragmatic paresis), making it contraindicated in patients with severe contralateral pulmonary disease.
b. Supraclavicular Block
- Target: Trunks and divisions of the plexus as they cross the first rib.
- Indications: Often termed the "spinal anesthesia of the upper extremity," it provides dense, rapid-onset anesthesia for the mid-humerus down to the hand.
- Pitfalls: Historically associated with a risk of pneumothorax. However, the modern use of high-frequency ultrasound guidance has reduced this risk to near zero.
c. Infraclavicular Block
- Target: Cords of the brachial plexus surrounding the axillary artery, deep to the pectoralis minor.
- Indications: Excellent for elbow, forearm, and hand surgery. Highly reliable for blocking the musculocutaneous and axillary nerves.
- Pitfalls: Deeper block, making ultrasound visualization more challenging in obese patients.
d. Axillary Block
- Target: Terminal branches (median, ulnar, radial) within the axillary sheath.
- Indications: The safest and most common block for forearm, wrist, and hand surgery.
- Pitfalls: The musculocutaneous nerve exits the sheath proximally; therefore, it must be blocked separately within the coracobrachialis muscle to ensure anesthesia of the lateral forearm.
2. Peripheral Nerve Blocks at the Wrist
For localized procedures of the hand and digits, blocking the terminal nerves at the wrist provides excellent anesthesia without paralyzing the extrinsic forearm musculature.
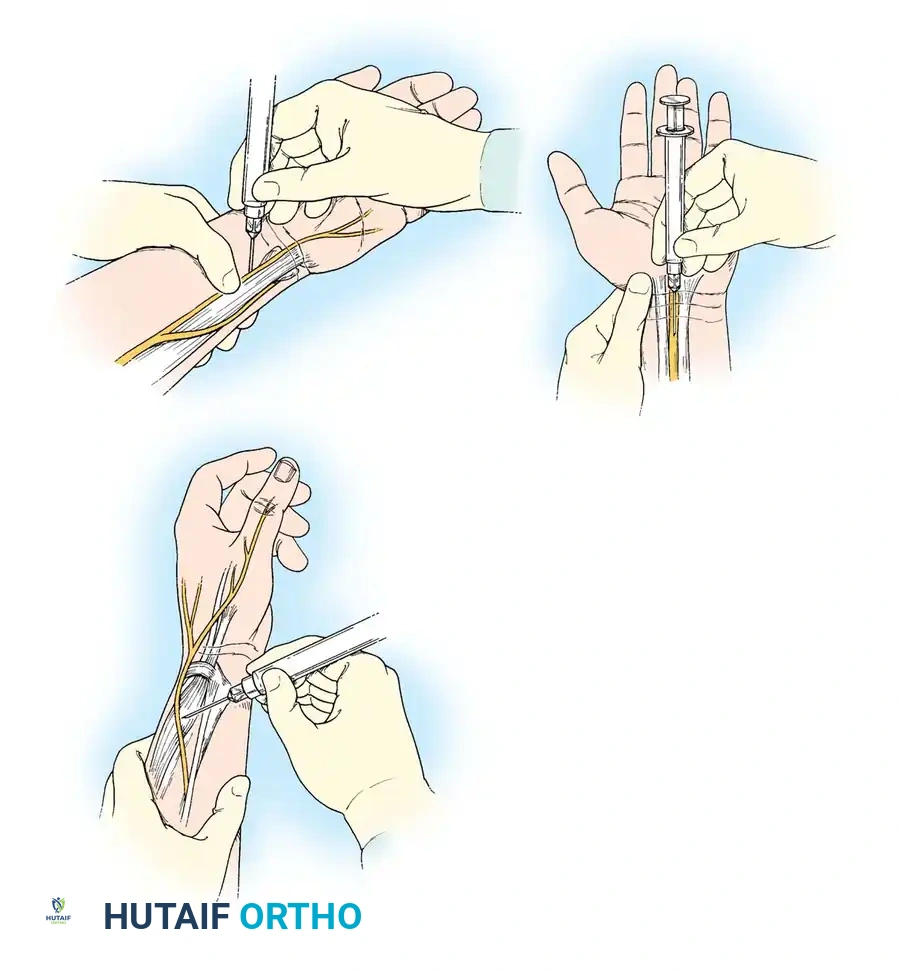
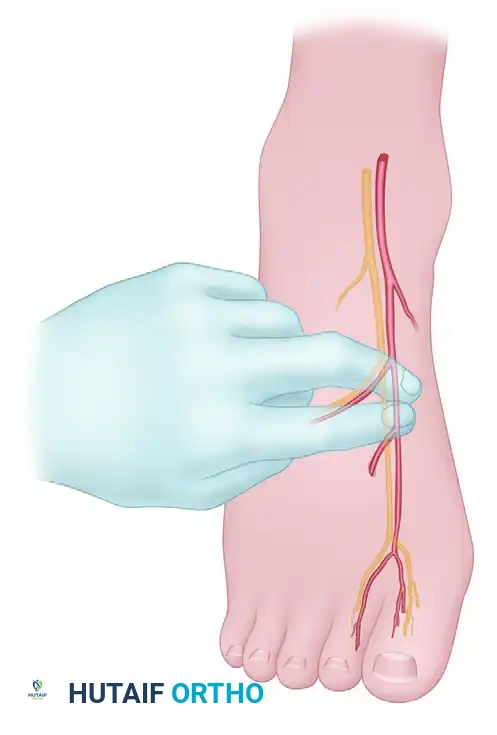
Fig. 61-5 Peripheral nerve blocks at the wrist. Top Left: Median nerve block injected between the flexor carpi radialis (FCR) and palmaris longus (PL) tendons. Top Right: Ulnar nerve block injected deep to the flexor carpi ulnaris (FCU), taking care to aspirate and avoid the ulnar artery. Bottom Left: Radial sensory nerve block injected subcutaneously over the anatomical snuffbox and radial styloid.
- Median Nerve Block: Administered at the proximal wrist crease between the palmaris longus and flexor carpi radialis tendons. Care must be taken to avoid intraneural injection, which can cause severe, permanent neuropathy.
- Ulnar Nerve Block: Administered just proximal to the pisiform, deep to the flexor carpi ulnaris tendon. The ulnar artery lies immediately radial to the nerve; meticulous aspiration is mandatory to prevent intravascular injection.
- Radial Nerve Block: A subcutaneous field block extending from the radial styloid dorsally across the anatomical snuffbox to anesthetize the superficial sensory branches.
3. Intravenous Regional Anesthesia (IVRA) / Bier Block
IVRA is an elegant, highly effective technique for procedures lasting less than 60 to 90 minutes on the distal upper extremity, such as carpal tunnel release, closed reduction of distal radius fractures, or hardware removal.
Mechanism and Technique
IVRA relies on the intravenous administration of local anesthetic into an exsanguinated, tourniquet-isolated limb. The anesthetic diffuses retrogradely through the venous system into the vasa nervorum and peripheral nerve endings.
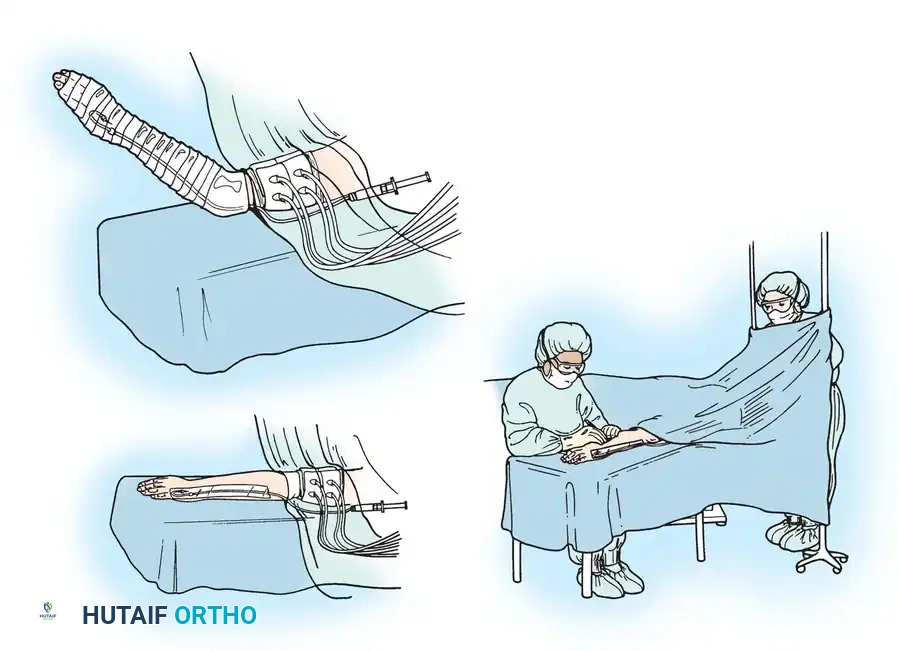
Fig. 61-6 Setup for Intravenous Regional Anesthesia (Bier Block). Top Left: The limb is elevated and tightly wrapped with an Esmarch bandage to exsanguinate the venous system. Bottom Left: A double pneumatic tourniquet is applied to the proximal arm. Right: The surgeon operates under a bloodless, anesthetized field. Note the intravenous cannula secured in the dorsum of the hand prior to exsanguination.
Step-by-Step Protocol:
1. Preparation: Insert a small-gauge IV cannula into a distal vein of the operative limb. Apply a double pneumatic tourniquet to the proximal arm.
2. Exsanguination: Elevate the arm and tightly wrap it with an Esmarch bandage from distal to proximal.
3. Isolation: Inflate the proximal cuff of the double tourniquet to 250 mm Hg (or 100 mm Hg above systolic pressure). Remove the Esmarch bandage. Confirm absence of radial pulse.
4. Injection: Slowly inject 40-50 mL of 0.5% Lidocaine (without epinephrine) through the distal IV cannula. Anesthesia onset is typically within 5 minutes.
5. Tourniquet Management: If the patient develops tourniquet pain (usually after 30-45 minutes), inflate the distal cuff (which now lies over anesthetized tissue), and subsequently deflate the proximal cuff.
6. Deflation Protocol: CRITICAL SAFETY STEP. The tourniquet must never be deflated before 20 minutes have elapsed from the time of injection, even if the surgery finishes early. Premature deflation releases a massive bolus of local anesthetic into the systemic circulation, risking Local Anesthetic Systemic Toxicity (LAST). Deflation should be performed cyclically (deflate for 10 seconds, reinflate for 1 minute) to allow gradual systemic buffering.
Postoperative Protocols and Complication Management
The transition from the operating room to the recovery phase requires vigilant management, particularly regarding the resolution of regional blocks.
- Rebound Pain: As a long-acting regional block (e.g., bupivacaine) wears off, patients can experience a sudden, severe onset of nociception known as "rebound pain." This must be preempted with a multimodal oral analgesic regimen (acetaminophen, NSAIDs, and a short course of oral opioids) initiated before the block fully resolves.
- Local Anesthetic Systemic Toxicity (LAST): A life-threatening complication resulting from intravascular injection or rapid systemic absorption. Early signs include perioral numbness, tinnitus, and metallic taste, rapidly progressing to seizures, arrhythmias, and cardiovascular collapse. Treatment: Immediate airway management, seizure suppression (benzodiazepines), and the rapid administration of 20% Intravenous Lipid Emulsion (Intralipid) to act as a "lipid sink," drawing the anesthetic away from cardiac and cerebral tissues.
- Neurologic Assessment: Any persistent paresthesia or motor deficit lasting beyond the expected duration of the local anesthetic must be urgently evaluated to rule out compressive hematoma or direct intraneural injury.
By mastering these anesthetic principles, the orthopedic surgeon ensures not only the technical success of the procedure but also the paramount safety and comfort of the patient.
You Might Also Like