Mastering the Chevron Osteotomy of the Fifth Metatarsal and Management of Freiberg Infraction
Key Takeaway
The chevron osteotomy of the fifth metatarsal is a highly effective, joint-sparing procedure for correcting symptomatic bunionette deformities. By translating the metatarsal head medially, it reduces the intermetatarsal angle and relieves lateral prominence pain. This guide details the step-by-step surgical technique, including capsular exposure, precise biplanar osteotomy execution, Kirschner wire fixation, and postoperative protocols, alongside the surgical management of Freiberg infraction via metatarsal head resection.
INTRODUCTION TO FOREFOOT PATHOLOGY: THE BUNIONETTE DEFORMITY
The bunionette, commonly referred to as a "Tailor’s bunion," is a painful lateral prominence of the fifth metatarsal head. Historically associated with the cross-legged sitting posture of tailors, the modern etiology is largely attributed to constricting footwear combined with intrinsic biomechanical abnormalities of the forefoot.
Pathoanatomically, bunionette deformities are classified into three distinct types based on radiographic evaluation:
* Type I: Enlargement or hypertrophy of the lateral aspect of the fifth metatarsal head.
* Type II: Lateral bowing of the distal fifth metatarsal shaft.
* Type III: An increased fourth-to-fifth intermetatarsal angle (IMA), typically exceeding the normal physiological limit of 8 degrees.
The Chevron Osteotomy of the Fifth Metatarsal is a highly versatile, joint-sparing, distal intra-articular procedure. It is primarily indicated for Type I and mild-to-moderate Type III deformities. By creating a V-shaped biplanar cut in the distal metaphysis, the surgeon can translate the capital fragment medially, effectively reducing the lateral prominence and narrowing the forefoot width. Furthermore, the osteotomy allows for dorsal angulation of the metatarsal head, which is highly beneficial in patients presenting with a concomitant intractable plantar keratosis (IPK) beneath the fifth metatarsal head.
Clinical Pearl: The fifth metatarsal chevron osteotomy is biomechanically less stable than its first metatarsal counterpart. The fifth ray lacks the robust soft-tissue envelope and broad cancellous bone surface area of the first ray. Consequently, meticulous surgical technique, precise osteotomy angles, and rigid internal fixation are paramount to prevent unexpected displacement, malunion, or nonunion.
PREOPERATIVE EVALUATION AND BIOMECHANICS
Clinical Assessment
Patients typically present with localized pain, erythema, and hyperkeratotic skin changes over the lateral eminence of the fifth metatarsophalangeal (MTP) joint. Pain is exacerbated by narrow-toe-box footwear and prolonged weight-bearing. A thorough physical examination must assess:
* The reducible nature of the deformity.
* The presence of a plantar callosity (indicating structural plantarflexion of the fifth ray).
* Range of motion of the fifth MTP joint to rule out arthritic changes.
* Neurovascular status, particularly the sural nerve distribution.
Radiographic Planning
Standard weight-bearing anteroposterior (AP), lateral, and oblique radiographs of the foot are mandatory.
* 4-5 Intermetatarsal Angle (IMA): Normal is < 8 degrees. An angle > 10 degrees often necessitates surgical correction.
* Lateral Bowing Angle: Evaluated to differentiate between Type II and Type III deformities.
* Fifth MTP Joint Congruency: Subluxation or joint space narrowing may dictate a different surgical approach, such as arthroplasty or resection.
SURGICAL TECHNIQUE: CHEVRON OSTEOTOMY OF THE FIFTH METATARSAL
1. Patient Positioning and Anesthesia
The procedure is typically performed under regional anesthesia (ankle block or popliteal block) with intravenous sedation. The patient is placed in the supine position. A calf or thigh tourniquet is applied to ensure a bloodless surgical field, which is critical for identifying the delicate capsular structures and avoiding thermal necrosis during the osteotomy.
2. Incision and Soft Tissue Dissection
Begin the incision laterally in the midline, approximately 1 cm distal to the fifth metatarsophalangeal joint. Extend the incision proximally in line with the longitudinal axis of the metatarsal shaft for 3 to 4 cm.
![]()
Carefully dissect through the subcutaneous tissues, taking great care to identify and retract the dorsal and plantar branches of the sural nerve.
3. Capsulotomy and Joint Exposure
Enter the metatarsophalangeal joint through a midlateral or an inverted L-shaped capsulotomy. This approach transects the abductor digiti minimi insertion and exposes the entire lateral aspect of the fifth metatarsal head.
![]()
- Sublux the fifth toe medially to improve visualization of the articular surface.
- Expose the distal 2 cm of the metatarsal shaft dorsally, laterally, and sufficiently plantarward to clearly visualize the exit point of the proposed plantar limb of the osteotomy.
Surgical Warning: Leave the soft tissue intact medially. The vascular supply to the fifth metatarsal head enters via the medial capsular attachments. Stripping the medial soft tissues drastically increases the risk of avascular necrosis (AVN) of the capital fragment. Use sharp dissection for exposure so that aggressive periosteal elevation does not become necessary.
4. Exostectomy (Lateral Eminence Resection)
Using a microsagittal saw, remove the lateral 1 to 2 mm of the lateral eminence.
![]()
Do not resect the eminence completely flush with the metatarsal shaft. Over-resection narrows the metatarsal head excessively, leaving insufficient bone stock for the subsequent chevron osteotomy and compromising the stability of the capital fragment.
5. Execution of the Chevron Osteotomy
Precision is the hallmark of this step. The area for the double-limb osteotomy is highly constrained.
* Apex Placement: Make a centering hole with a 0.045-inch Kirschner wire exactly 5 mm proximal to the articular cartilage of the metatarsal head. This hole must be equidistant from the dorsal and plantar cortices. This serves as the apex of the V-osteotomy.
* Dorsal Limb: Using a 4-mm blade on a power saw, start the dorsal limb of the osteotomy angled 30 to 40 degrees from the midlateral longitudinal axis of the fifth metatarsal. Proceed cautiously with minimal pushing of the saw to prevent the blade from "walking" into the capital fragment distally.
![]()
- Plantar Limb: The plantar limb is cut next, again at about 30 to 40 degrees to the midline, creating an apex angle of 60 to 80 degrees. Exposure of the distal shaft dorsally, laterally, and plantarward affords the surgeon maximum control over these cuts. As in the first metatarsal chevron osteotomy, the saw blade must be held strictly at right angles (perpendicular) to the metatarsal shaft to prevent unintended dorsal or plantar elevation during translation.
6. Translation of the Capital Fragment
Once the osteotomy is complete, manually translate the fifth metatarsal head medially by 2 to 4 mm, depending on the native diameter of the metatarsal.
![]()
Clinical Pearl: If the patient presented with a symptomatic plantar callosity (intractable plantar keratosis), tilt the metatarsal head dorsally by 2 to 3 mm during translation. This offloads the plantar aspect of the metatarsal head, directly addressing the mechanical etiology of the callus.
7. Internal Fixation
Because this osteotomy is inherently less stable than its first metatarsal equivalent, it can tilt unexpectedly medially, plantarward, or dorsally.
* Appose the osteotomy surfaces as congruently as possible, ensuring the head remains in line with the shaft.
* Utilize one or two 0.045-inch Kirschner wires for rigid stability.
* Start the wires proximally, just dorsal and plantar to the midline of the shaft, and drive them obliquely across the osteotomy site into the metatarsal head.
![]()
- After fixation, use a small rongeur or a rasp to smooth the lateral overhang of the proximal metatarsal shaft. Take extreme care not to remove the cortex adjacent to the Kirschner wires, which could compromise their purchase and lead to fixation failure.
8. Capsular Closure and Soft Tissue Balancing
The capsular closure is a critical, non-negotiable step to prevent postoperative medial subluxation of the fifth toe.
* Hold the toe congruously on the metatarsal head.
* Using a 3-0 absorbable suture (e.g., Vicryl), meticulously repair the lateral capsule.
* During this repair, bring the tendon of the abductor digiti minimi dorsally into the midline.
![]()
After completing the capsular repair, the toe should remain in perfect anatomical position without any extraneous manual support. Apply a sterile, compressive dressing designed to hold the toe in proper alignment and relieve tension on the capsular repair.
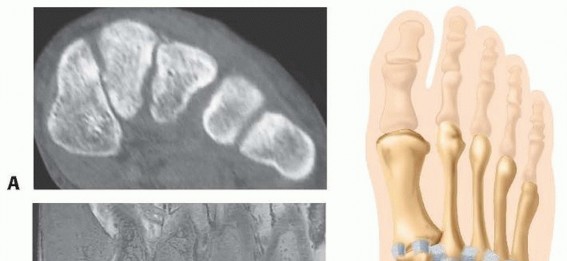
FREIBERG INFRACTION: PATHOPHYSIOLOGY AND SURGICAL MANAGEMENT
While addressing forefoot pathology, the orthopedic surgeon must be adept at diagnosing and treating osteochondroses of the metatarsal heads. Freiberg infraction is a classic example of this category of disease, characterized by osteonecrosis of the subchondral cancellous bone followed by a complex, often painful, reparative process.
Etiology and Biomechanics
A misshapen metatarsal head is frequently an incidental radiographic finding. However, careful clinical questioning often reveals a distinct period during adolescence when the patient experienced localized forefoot pain.
Because the second toe is frequently the longest digit and the second ray is the least mobile segment of the forefoot, excessive pressure on the metatarsal head during the terminal stance phase of weight-bearing can cause repetitive microfractures. This mechanical overload leads to:
1. Loss of blood supply to the subchondral bone.
2. Collapse of the cancellous bone architecture.
3. Severe cartilage deformation and flattening of the metatarsal head.
Synovitis invariably accompanies this necrotic process. If the synovitis is prolonged and severe, it results in a marked limitation of motion, particularly in MTP joint extension. With the loss of extension, weight-bearing forces cause abnormal stress to be applied directly to the metatarsal shaft, which subsequently becomes widened due to reactive bicortical thickening. In addition to irregular ossification of the primary ossification center and shaft widening, osteochondral fragmentation (loose bodies) frequently occurs around the joint space.
Clinical Presentation
Symptoms include:
* Deep, aching pain around the involved metatarsophalangeal joint, primarily exacerbated by weight-bearing.
* Point tenderness directly over the dorsal aspect of the metatarsal head.
* Limitation of motion, with a rigid block to dorsiflexion.
* Periarticular swelling secondary to chronic synovitis.
Conservative Management
Most patients with early-stage Freiberg infraction can be managed non-operatively. Treatment modalities include:
* Modification of high-impact activities.
* Custom semirigid orthoses with metatarsal pads to offload the affected head.
* Footwear modifications utilizing metatarsal bars or rigid rocker-bottom soles.
* In refractory acute cases, a short-leg walking cast with a toe extension may be required to completely rest the painful foot. Occasionally, crutches are necessary for strict non-weight-bearing.
Surgical Management: Metatarsal Head Resection
If conservative management fails and the joint is destroyed (Smillie Stage IV or V), surgical intervention is warranted. While joint-sparing dorsal closing-wedge osteotomies are preferred in early stages, advanced collapse requires resection arthroplasty.
The Giannestras Procedure (Resection of the Metatarsal Head):
In cases of severe, end-stage Freiberg infraction affecting the lesser metatarsals (including the fifth), resection of the metatarsal head provides reliable pain relief.
![]()
The metatarsal head is removed via an oblique osteotomy directed from dorsal-distal to plantar-proximal, well proximal to the head-neck junction. This oblique cut ensures that no sharp plantar bony prominence remains to cause a secondary transfer lesion or intractable plantar keratosis. The remaining capsule is often interposed into the void to act as a biologic spacer.
POSTOPERATIVE CARE AND REHABILITATION PROTOCOL
The success of both the fifth metatarsal chevron osteotomy and forefoot resection arthroplasties relies heavily on strict adherence to postoperative protocols.
Phase I: Acute Healing (Days 0 - 14)
* Activity is strictly reduced for the first 72 hours, and the foot is continuously elevated above heart level to minimize edema and throbbing pain.
* A rigid postoperative shoe is worn at all times.
* Weight-bearing to tolerance on the heel and lateral border of the foot is allowed, but forefoot loading is discouraged.
* 1-Week Post-Op: The initial surgical dressing is changed. It must be carefully reapplied to maintain the proper alignment of the toe and relieve any tension on the delicate lateral capsular repair.
* 2-Weeks Post-Op: Sutures are removed. A web spacer made of gauze or foam rubber, secured with narrow tape, is utilized to maintain the proper position of the toe and prevent medial drift.
Phase II: Intermediate Rehabilitation (Weeks 4 - 8)
* At 4 weeks, if clinical healing is progressing, the patient may transition to a wide toe box, firm-soled athletic shoe.
* A short-leg walking cast extending distal to the toes is occasionally utilized for 1 month if the patient is non-compliant or must be more active than a standard postoperative shoe would safely allow.
* 6 to 8 Weeks Post-Op: Radiographs are obtained to confirm bony union of the osteotomy. Once clinical and radiographic healing is confirmed, the Kirschner wires are removed in the office setting under local anesthesia.
Phase III: Long-Term Follow-Up
* Patients are advised that mild swelling may persist for up to 4 to 6 months.
* Physical therapy may be initiated to restore MTP joint range of motion and strengthen the intrinsic foot musculature.
COMPLICATIONS AND PITFALLS
While highly successful, the chevron osteotomy of the fifth metatarsal carries specific risks:
1. Avascular Necrosis (AVN): The most devastating complication. Prevented by strictly avoiding medial soft tissue stripping.
2. Malunion / Nonunion: Often due to premature weight-bearing, inadequate K-wire fixation, or thermal necrosis from the saw blade.
3. Transfer Metatarsalgia: Caused by unintended dorsal elevation of the capital fragment during the osteotomy. The saw blade must remain perfectly perpendicular to the shaft.
4. Recurrence: Under-correction of the IMA or failure to adequately repair the lateral capsule and reposition the abductor digiti minimi can lead to recurrent deformity.
By mastering the precise geometric cuts of the chevron osteotomy, respecting the delicate vascular anatomy of the forefoot, and executing meticulous soft-tissue balancing, the orthopedic surgeon can achieve excellent, reproducible outcomes in the management of bunionette deformities and associated forefoot pathologies.
You Might Also Like