Mastering Complex Arthroplasty: Paley Principles for Deformity Correction
Key Takeaway
Complex arthroplasty in severe malalignment requires applying Paley principles like Mechanical Axis Deviation, Joint Orientation Angles, and CORA. This ensures optimal biomechanics, prevents component malposition, and avoids the 'Arthroplasty Trap,' leading to successful, long-lasting outcomes in challenging reconstructive cases.
Intersection of Arthroplasty and Deformity Correction
Standard Total Knee Arthroplasty and Total Hip Arthroplasty are widely celebrated as some of the most successful surgical procedures in modern medicine for end-stage osteoarthritis. However, the paradigm shifts dramatically when degenerative joint disease is coupled with severe extraarticular or intraarticular malalignment. In these complex clinical scenarios, the difficulty of the reconstruction increases exponentially, testing the limits of both the surgeon's skill and the implant's biomechanical design.
Orthopedic surgeons can no longer rely on standard intramedullary or extramedullary alignment guides in the face of profound deformity. Post-traumatic malunions, congenital bowing, metabolic bone diseases, and prior failed osteotomies create distorted anatomy that will inevitably lead to component malposition if traditional techniques are utilized. This malposition results in severe ligamentous instability, altered kinematics, accelerated polyethylene wear, and ultimately, catastrophic biomechanical failure of the arthroplasty.
To achieve a successful, long-lasting outcome in these complex scenarios, the orthopedic surgeon must fundamentally transition from a traditional joint replacement mindset to a highly analytical deformity correction mindset. This evolution requires a profound, working understanding of Dr. Dror Paley’s principles of deformity correction. Mastering the concepts of the mechanical axis, joint orientation angles, and the Center of Rotation of Angulation is non-negotiable for the modern reconstructive surgeon.
This comprehensive guide explores the nuanced biomechanics, meticulous preoperative planning, and precise surgical execution required when performing arthroplasty in the presence of severe malalignment. By integrating Paley principles into daily arthroplasty practice, surgeons can confidently navigate distorted anatomy and restore optimal biomechanics.
Fundamentals of Paley Deformity Principles in Arthroplasty
Before a scalpel touches skin or a saw blade makes a single bone cut, the surgeon must definitively map the level, magnitude, and plane of the deformity. The ultimate goal of any lower extremity arthroplasty is to restore the Mechanical Axis Deviation to neutral while maintaining joint lines that are perfectly parallel to the ground during the stance phase of gait.
Calculating Mechanical Axis Deviation
The Mechanical Axis Deviation is the foundational metric in deformity correction. It is determined by drawing a line from the center of the femoral head to the center of the tibial plafond on a full-length, weight-bearing anteroposterior radiograph. In a normally aligned lower extremity, this mechanical axis line should pass slightly medial to the exact center of the knee joint, typically bisecting the medial tibial spine.
When the mechanical axis passes medial to the center of the knee, the limb is in varus, creating a medial Mechanical Axis Deviation. When the axis passes lateral to the center of the knee, the limb is in valgus, creating a lateral Mechanical Axis Deviation. Quantifying the exact millimeter deviation from the joint center is the first step in understanding the magnitude of the corrective forces required during arthroplasty.
Defining Normal Joint Orientation Angles
Restoring the Mechanical Axis Deviation requires restoring normal joint orientation angles. These angles define the relationship between the mechanical or anatomic axes of the long bones and their respective articular surfaces. In a neutral mechanical alignment philosophy, the goal is to cut the distal femur and proximal tibia orthogonal to their mechanical axes.
| Joint Orientation Angle | Abbreviation | Normal Value Range | Clinical Significance in Arthroplasty |
|---|---|---|---|
| Mechanical Lateral Distal Femoral Angle | mLDFA | 85 to 90 degrees (Avg 87) | Dictates the distal femoral bone cut in the coronal plane. |
| Mechanical Medial Proximal Tibial Angle | mMPTA | 85 to 90 degrees (Avg 87) | Dictates the proximal tibial bone cut in the coronal plane. |
| Joint Line Convergence Angle | JLCA | 0 to 2 degrees | Indicates intraarticular deformity due to cartilage loss or ligament laxity. |
| Anatomic Lateral Distal Femoral Angle | aLDFA | 79 to 83 degrees (Avg 81) | Used when referencing the intramedullary axis of the femur. |
| Posterior Proximal Tibial Angle | PPTA | 77 to 84 degrees (Avg 81) | Dictates the sagittal slope of the proximal tibial cut. |
Understanding the distinction between mechanical and anatomic axes is paramount. The mechanical axis of the femur connects the center of the femoral head to the center of the knee, while the anatomic axis runs down the center of the medullary canal. The angle between these two axes is typically 5 to 7 degrees, which dictates the standard valgus cut angle set on distal femoral intramedullary guides. However, in deformed femurs, this angle can vary wildly, rendering standard intramedullary guides useless and dangerous.
Center of Rotation of Angulation and Its Clinical Significance
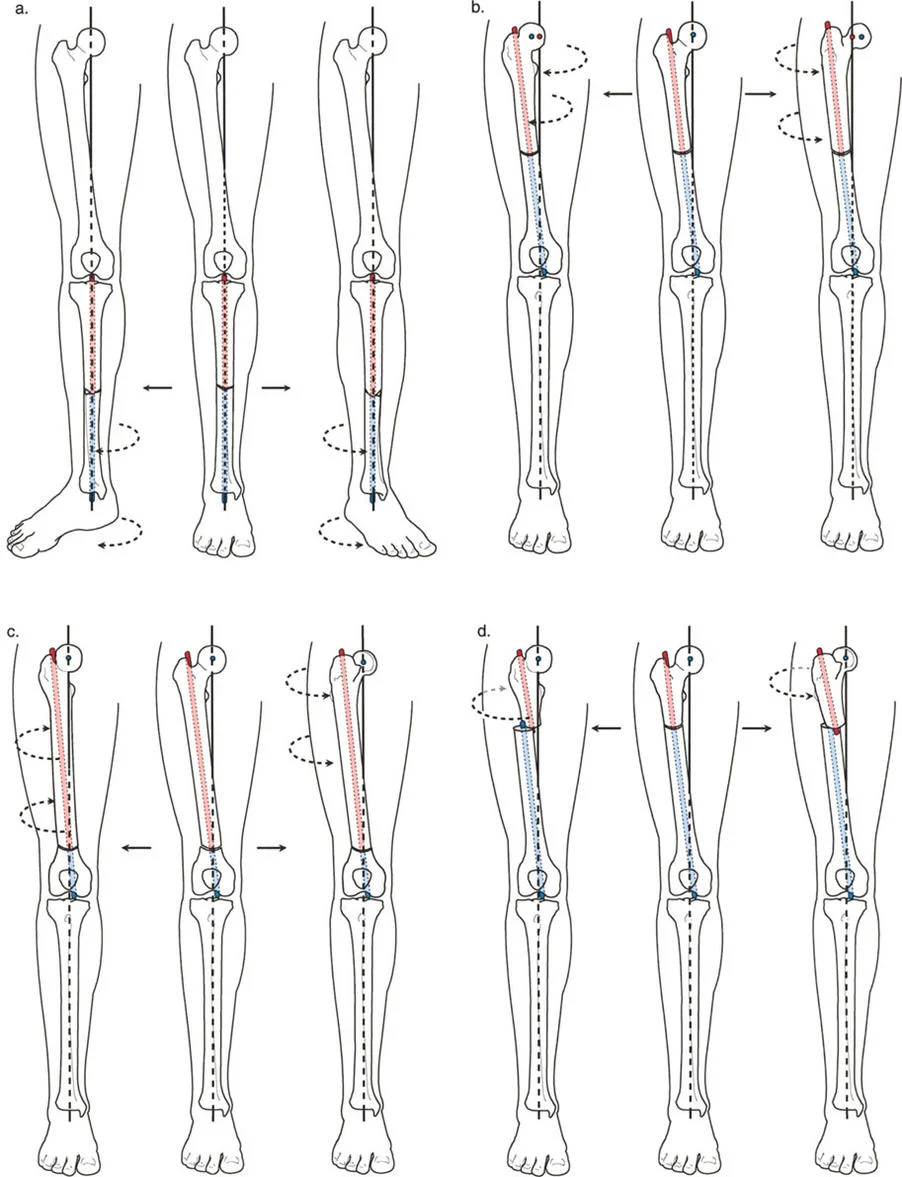
The Center of Rotation of Angulation is the cornerstone of Dr. Paley's deformity analysis. It is defined as the intersection point of the proximal and distal mid-diaphyseal anatomical axes of a deformed bone. Identifying the exact location of the Center of Rotation of Angulation dictates whether a deformity can be corrected simultaneously with standard arthroplasty bone cuts or if it mandates a separate extraarticular osteotomy.
When evaluating a deformed limb, the surgeon must draw the mechanical axis line of the proximal segment and the mechanical axis line of the distal segment. Where these two lines intersect is the Center of Rotation of Angulation. The magnitude of the angle formed at this intersection is the true magnitude of the bony deformity.
Applying Paley Osteotomy Rules to Joint Replacement
When determining how to address the identified Center of Rotation of Angulation during a joint replacement, the surgeon must rigorously apply Paley’s Osteotomy Rules. Understanding these rules dictates the entire surgical approach, implant selection, and need for modularity.
Osteotomy Rule 1 Intraarticular Correction
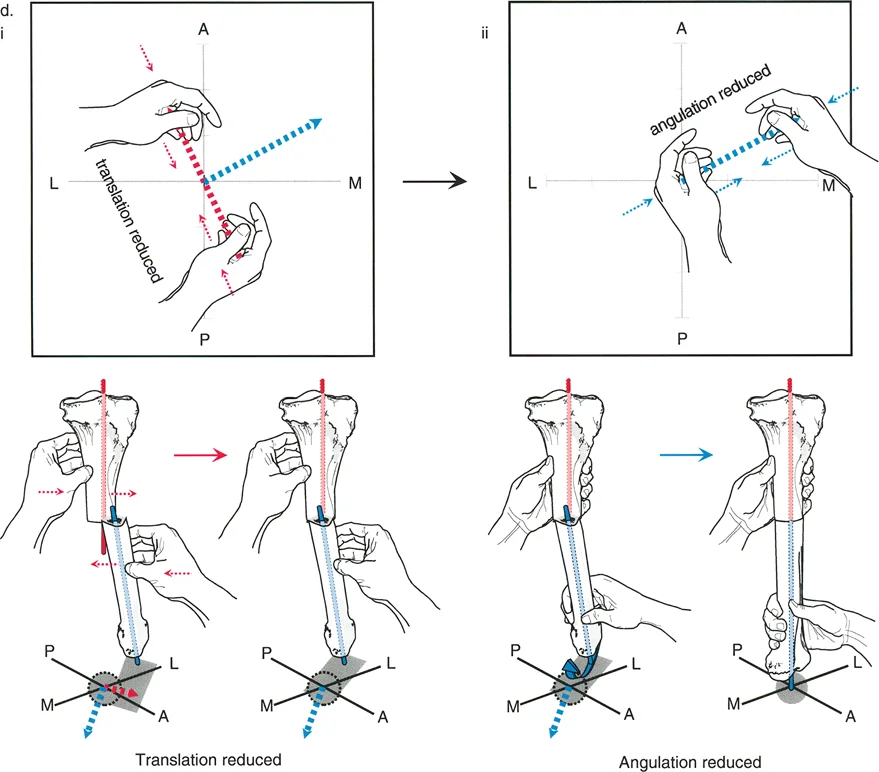
Paley's Osteotomy Rule 1 states that when the osteotomy or bone resection passes directly through the Center of Rotation of Angulation, pure angulation corrects the deformity without any translation. This is the ideal, straightforward scenario in total joint arthroplasty.
If the Center of Rotation of Angulation is located intraarticularly, which is typical for deformities secondary to severe asymmetric articular wear, cartilage loss, and condylar collapse, standard arthroplasty cuts follow Rule 1. The surgeon simply makes the distal femoral and proximal tibial cuts orthogonal to the mechanical axes. Because the cuts pass through the apex of the deformity, the bone resections naturally realign the limb perfectly without creating any secondary translational deformities.
Osteotomy Rule 2 Utilizing Offset Stems
Paley's Osteotomy Rule 2 states that when the osteotomy is performed outside the Center of Rotation of Angulation, the bone ends must be translated to realign the mechanical axis perfectly.
In the context of arthroplasty, the bone cuts are fixed at the joint line. If the patient has a metaphyseal or diaphyseal deformity, the Center of Rotation of Angulation is located far from the joint line cuts. If the surgeon simply angulates the cut to match the mechanical axis, a translation deformity will occur at the joint line.
To manage this, surgeons frequently utilize offset stems. Offset stems allow the surgeon to translate the diaphyseal intramedullary fixation relative to the intraarticular joint line components. By dialing in the correct amount of offset, the surgeon effectively respects Rule 2, realigning the mechanical axis perfectly without requiring a separate, morbid extraarticular bone cut.
Osteotomy Rule 3 The Arthroplasty Trap
Paley's Osteotomy Rule 3 states that when an osteotomy is performed outside the Center of Rotation of Angulation without translation, a secondary translation deformity is inevitably created, often termed a zig-zag deformity. In joint replacement, violating this rule leads to what is known as the Arthroplasty Trap.
One of the most common and devastating errors in complex arthroplasty is falling into this trap. Imagine a patient with a severe extraarticular diaphyseal deformity, such as a healed midshaft femur fracture with a 20-degree varus bow. The Center of Rotation of Angulation is located in the midshaft. If the surgeon attempts to correct the overall limb alignment purely by making asymmetric, intraarticular bone cuts during a knee replacement, they are directly violating Rule 3.
To make the limb straight using only joint line cuts, the surgeon would have to resect massive amounts of bone from one condyle while leaving the other almost untouched. This leads to three catastrophic consequences:
1. Excessive, asymmetric bone over-resection compromises the metaphyseal bone stock, often requiring massive augments or cones just to support the primary implant.
2. Severe joint line obliquity is created. The joint line is no longer parallel to the ground, altering the kinematics of the knee and causing massive shear stresses on the polyethylene bearing, leading to early aseptic loosening.
3. Profound collateral ligament imbalance occurs. The epicondylar origins of the ligaments are completely distorted relative to the new joint line, creating a flexion-extension gap mismatch that often cannot be corrected even with highly constrained hinged prostheses.
Preoperative Templating for Complex Arthroplasty
Avoiding the Arthroplasty Trap requires meticulous preoperative templating. The surgeon must determine whether standard intraoperative correction will suffice, if offset stems can manage the required translation, or if the extraarticular deformity is so severe that a simultaneous or staged extraarticular osteotomy is required.
Step by Step Preoperative Planning Protocol
- Obtain Optimal Imaging Secure full-length, weight-bearing anteroposterior radiographs of both lower extremities, standing lateral radiographs, and dedicated joint views.
- Assess Intraarticular Deformity Measure the Joint Line Convergence Angle to determine how much of the deformity is purely due to cartilage loss and ligamentous laxity. This portion of the deformity will correct passively with standard soft tissue releases and component insertion.
- Map the Mechanical Axes Draw the mechanical axis of the femur and the tibia.
- Locate the CORA Identify the intersection of the proximal and distal anatomical axes for any deformed bone segment.
- Simulate Bone Cuts Draw the planned distal femoral and proximal tibial resections at 90 degrees to their respective mechanical axes.
- Evaluate the Residual Defect If the simulated cuts result in asymmetric bone resection exceeding 10 to 15 millimeters, or if the collateral ligament origins are significantly compromised, an extraarticular correction strategy must be formulated.
- Template Implants Overlay templating software to determine if modular offset stems can bridge the translation gap, or if diaphyseal engaging stems are required for stability.
Managing Extraarticular Deformity During Total Knee Arthroplasty
When the Center of Rotation of Angulation is extraarticular, the surgeon must decide between an intraarticular compensatory cut, the use of offset stems, or a formal extraarticular osteotomy. The decision is largely based on the distance of the deformity from the joint line and the magnitude of the angulation.
Femoral Extraarticular Deformity Considerations
Deformities in the femur are common following trauma. Generally, intraarticular compensatory cuts can be tolerated for femoral deformities up to 10 degrees in the coronal plane and 20 degrees in the sagittal plane, provided the deformity is located in the mid-to-proximal diaphysis.
Because the femur is further from the joint line, a small angulation creates a larger translation at the knee. If the surgeon attempts to correct a 15-degree distal metaphyseal varus deformity intraarticularly, the medial collateral ligament origin will be severely elevated relative to the joint line, creating an unmanageable asymmetric gap. In these cases, a simultaneous distal femoral closing wedge or opening wedge osteotomy, stabilized by a long-stemmed revision femoral component, is the treatment of choice.
Tibial Extraarticular Deformity Considerations
The tibia is less forgiving than the femur regarding compensatory intraarticular cuts. Coronal plane deformities greater than 10 degrees or sagittal plane deformities greater than 15 degrees typically require a formal extraarticular osteotomy.
If a severe tibial recurvatum deformity is corrected by simply altering the slope of the proximal tibial bone cut, the surgeon risks cutting anteriorly into the tibial tubercle, compromising the extensor mechanism insertion. Furthermore, severe varus or valgus bowing of the tibia will cause a standard straight intramedullary stem to impinge on the diaphyseal cortex, forcing the tibial tray into malalignment.
Indications for Simultaneous Osteotomy and Arthroplasty
Performing a simultaneous extraarticular osteotomy and total knee arthroplasty is technically demanding but offers the advantage of a single surgical intervention. The primary indications include:
* Deformities exceeding the threshold for intraarticular compensation (greater than 10-15 degrees coronal, 15-20 degrees sagittal).
* Deformities located close to the joint line where compensatory cuts would obliterate collateral ligament attachments.
* Cases where the intramedullary canal is obliterated or severely bowed, preventing the passage of a standard or revision stem without osteotomy.
During this procedure, the osteotomy is typically performed first to restore the mechanical axis of the bone. The bone ends are provisionally stabilized, and then standard arthroplasty cuts are executed. A long diaphyseal-engaging stem is then used to bypass the osteotomy site, acting as an intramedullary nail to stabilize the fracture while simultaneously anchoring the joint component.
Managing Extraarticular Deformity During Total Hip Arthroplasty
While knee arthroplasty relies heavily on coronal and sagittal alignment, total hip arthroplasty in the setting of severe deformity focuses on restoring the center of rotation of the hip, managing limb length discrepancy, and ensuring adequate femoral offset.
Proximal Femoral Deformity and Stem Selection
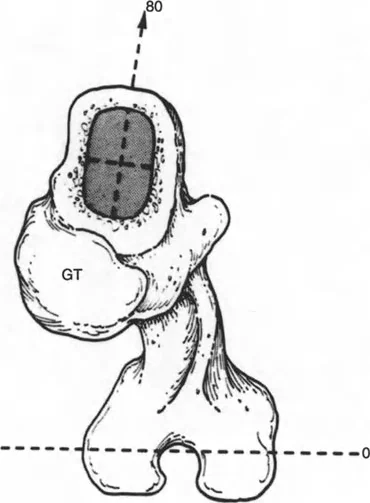
Proximal femoral deformities are frequently encountered in patients with prior slipped capital femoral epiphysis, Legg-Calve-Perthes disease, or previous intertrochanteric fractures. The Center of Rotation of Angulation is often located in the metaphysis or proximal diaphysis.
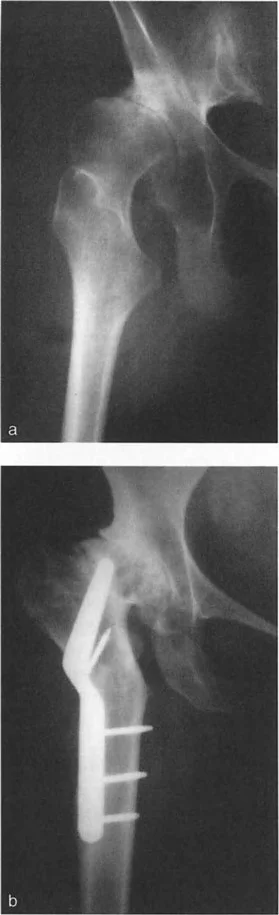
If the deformity prevents the passage of a standard straight femoral stem, the surgeon must apply Paley's principles. A templated osteotomy at the level of the Center of Rotation of Angulation allows the surgeon to realign the diaphysis with the metaphysis. In cases of severe developmental dysplasia of the hip with high dislocation, the femur is functionally shortened. A subtrochanteric shortening osteotomy is often required to bring the femoral head down to the true acetabulum without causing catastrophic sciatic nerve palsy from over-lengthening.
Modular stems are invaluable in these scenarios. A modular fluted tapered stem allows the surgeon to gain diaphyseal fixation independent of the proximal metaphyseal anatomy. The proximal body can then be dialed into the correct version and offset, effectively managing the translation and rotation created by the extraarticular deformity.
Acetabular Dysplasia and Center of Rotation
On the acetabular side, severe dysplasia results in a superior and lateral migration of the hip center of rotation. Restoring the anatomic center of rotation is critical for optimizing abductor biomechanics and maximizing implant longevity.
Leaving the cup in a high hip center position increases joint reactive forces and leads to early loosening. To restore the center of rotation to its anatomic location, the surgeon may need to utilize structural bone grafts from the resected femoral head, porous metal augments, or custom triflange components to bridge the gap between the true acetabulum and the dysplastic superior rim.
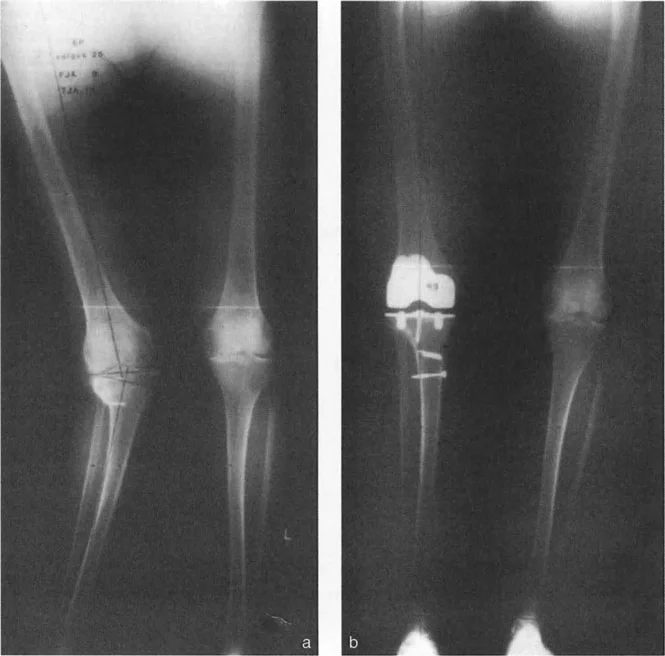
Total Knee Arthroplasty Following Failed High Tibial Osteotomy
High Tibial Osteotomy remains a valuable, joint-preserving procedure for younger, active patients suffering from medial compartment osteoarthritis with varus malalignment. However, as the natural history of the disease progresses, these patients eventually require conversion to a total knee arthroplasty. This conversion is notoriously one of the most challenging procedures in reconstructive surgery.
Biomechanical Alterations Post HTO
A previous High Tibial Osteotomy fundamentally alters the anatomy of the proximal tibia, creating a multi-planar extraarticular deformity.
First, the osteotomy creates a coronal plane offset, often referred to as a dog-leg deformity. The proximal tibial metaphysis is translated relative to the diaphysis. If the surgeon uses a standard long intramedullary tibial guide, the guide rod will hit the lateral cortex of the diaphysis, forcing the cutting block into varus.
Second, opening wedge osteotomies typically increase the posterior tibial slope, while closing wedge osteotomies decrease the slope. The surgeon must carefully assess the sagittal plane to avoid excessive resection of the posterior tibial plateau, which would compromise the flexion gap and lead to posterior instability.
Third, the patella is frequently altered. Closing wedge osteotomies, and particularly opening wedge osteotomies that involve patellar tendon scarring, often result in patella infera or patella baja. The patella sits abnormally low, making eversion of the extensor mechanism exceptionally difficult and increasing the risk of catastrophic patellar tendon avulsion during the exposure.
Surgical Technique for Post HTO Arthroplasty
Executing a total knee arthroplasty after a failed High Tibial Osteotomy requires a meticulous, step-wise approach:
- Hardware Removal Retained plates and screws must be removed. This can be done as a staged procedure if infection is suspected, or simultaneously. If done simultaneously, the surgeon must bypass the empty screw holes with a longer tibial stem to prevent postoperative stress fractures.
- Extensor Mechanism Management Due to patella baja, a standard medial parapatellar arthrotomy may not provide adequate exposure. The surgeon should be prepared to perform a quadriceps snip or a tibial tubercle osteotomy to safely lateralize the extensor mechanism without avulsing the patellar tendon.
- Managing the Dog-Leg Deformity To address the translational deformity created by the previous osteotomy, offset tibial stems are frequently required. The offset allows the surgeon to center the tibial tray on the metaphysis while the stem engages the offset diaphysis, perfectly executing Paley's Osteotomy Rule 2.
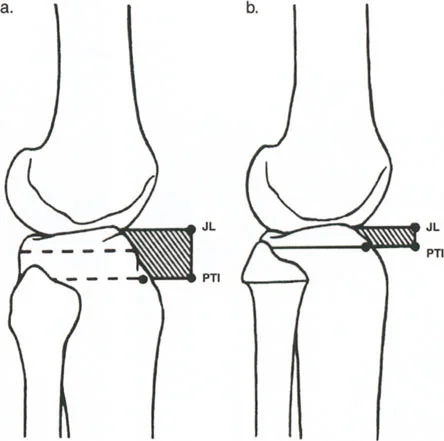
- Restoring Joint Line Height Because the proximal tibia has been altered, standard referencing off the remaining cartilage is inaccurate. The surgeon must rely on the fibular head or the epicondyles to accurately restore the joint line height and prevent mid-flexion instability.
Ligamentous Balancing in the Deformed Limb
Addressing the bony deformity is only half the battle; the soft tissue envelope must be meticulously balanced to achieve a stable, functional arthroplasty. Severe chronic malalignment leads to contracture of the soft tissues on the concave side of the deformity and stretching of the soft tissues on the convex side.
Gap Kinematics and Deformity Correction
In a severe varus knee, the medial collateral ligament and medial capsule are contracted, while the lateral collateral ligament is attenuated. Once the bone cuts are made orthogonal to the mechanical axis, the surgeon will be left with a tight medial gap and a loose lateral gap.
Standard sequential soft tissue releases are required. For varus deformities, this involves releasing the deep medial collateral ligament, the posteromedial capsule, and the semimembranosus insertion. For valgus deformities, the release sequence targets the lateral capsule, the iliotibial band, the popliteus tendon, and the lateral collateral ligament.
However, if the surgeon has fallen into the Arthroplasty Trap and attempted to correct a severe extraarticular deformity with intraarticular cuts, the epicondylar origins of these ligaments will be so displaced that no amount of soft tissue release will balance the gaps. The gaps will be asymmetric in both flexion and extension, mandating the use of highly constrained implants.
Implant Constraint Selection Criteria
The goal of any arthroplasty is to use the least amount of constraint necessary to achieve stability. However, in the setting of severe deformity correction, higher levels of constraint are frequently required.
- Cruciate Retaining or Posterior Stabilized Appropriate for mild to moderate intraarticular deformities where the collateral ligaments are intact and can be balanced with standard releases.
- Constrained Condylar Knee Required when the collateral ligaments are attenuated or when mild epicondylar mismatch exists following the correction of a moderate extraarticular deformity. The tall tibial post provides coronal plane stability.
- Rotating Hinge Indicated for severe extraarticular deformities corrected simultaneously, profound collateral ligament deficiency, or cases where massive bone resection has obliterated the ligamentous origins entirely.
Summary of High Yield Clinical Pearls
- Respect the CORA Always locate the Center of Rotation of Angulation. If it is extraarticular, determine if offset stems or a formal osteotomy is required to prevent the Arthroplasty Trap.
- Beware the Arthroplasty Trap Never attempt to correct a severe diaphyseal deformity purely with asymmetric intraarticular bone cuts. This will destroy the bone stock, skew the joint line, and make ligamentous balancing impossible.
- Utilize Offset Stems Offset stems are the ultimate tool for executing Paley's Osteotomy Rule 2 in joint replacement, allowing diaphyseal fixation while managing translational mismatch at the metaphysis.
- Anticipate Patella Baja Post-HTO When converting a high tibial osteotomy to a total knee, anticipate severe exposure difficulties. Have a low threshold to perform a quadriceps snip to protect the patellar tendon.
- Template Meticulously Standard intramedullary guides are useless in deformed bones. Preoperative digital templating with full-length standing radiographs is mandatory to plan the level of bone resection and the required implant modularity.
- Prepare for Modularity and Constraint Always have revision systems, offset stems, metaphyseal cones, and hinged implants available when tackling arthroplasty in the severely malaligned limb.
!!! info "Academic Resource & Medical Review"
This academic resource was prepared and medically reviewed by Prof. Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon. It is formulated specifically for medical students, orthopedic residents, and surgeons preparing for high-stakes board examinations (AAOS, FRCS Tr & Orth, Arab Board).
!!! warning "Disclaimer"
The surgical techniques, classifications, and clinical guidelines presented herein are for educational and academic review purposes only. They are not intended to replace institutional protocols or independent clinical judgment.
You Might Also Like